
Abstract
Cognitive Behavior Therapy (CBT) for bulimia nervosa (BN) requires patient skill utilization (use of treatment skills) and skill acquisition (successful skill use) for symptom improvement. Treatment outcomes are unsatisfactory, possibly due to poor skill acquisition and utilization by post-treatment. Just-in-time adaptive interventions (JITAIs), momentary interventions delivered at opportunities for skill practice, may improve skill acquisition and utilization. Participants (N = 56 individuals with bulimia-spectrum eating disorders) completed electronic self-monitoring in CBT+ and received JITAIs or no JITAIs alongside 16 sessions of CBT. Feasibility, acceptability, target engagement, and treatment outcomes were evaluated. JITAIs demonstrated feasibility and acceptability. Treatment outcomes and target engagement did not differ between conditions. The lack of group differences in target engagement and treatment outcomes may be explained by skill use self-monitoring promoting skill utilization and acquisition or low statistical power. Our findings suggest that JITAIs are feasible and acceptable during CBT for BN and warrant additional study.
Keywords
Introduction
Bulimia nervosa (BN) is an eating disorder (ED) characterized by recurrent binge eating (consuming a large amount of food accompanied by a sense of loss of control) and compensatory behaviors (e.g., vomiting, laxatives or diuretics misuse, and driven exercise), motivated by extensive concern for body weight (American Psychiatric Association, 2013). Cognitive Behavioral Therapy (CBT) including the enhanced, transdiagnostic version, CBT-E, is the most evidence-based treatment for BN (Fairburn et al., 2009; Hay et al., 2009; National Institute for Clinical Excellence, 2011; Shapiro et al., 2007). CBT for BN is skills-focused, dedicating the majority of treatment content to teaching therapeutic skills focused on (1) reducing dietary restraint (i.e., conscious attempts to cut down the amount or types of food eaten to influence shape or weight) and (2) increasing adaptive responses to cues (i.e., increasing awareness of cues for binge eating and encouraging more effective behavioral responses; see Table 1; Fairburn, 2008).
Key CBT Skills for Bulimia-Spectrum Eating Disorders.
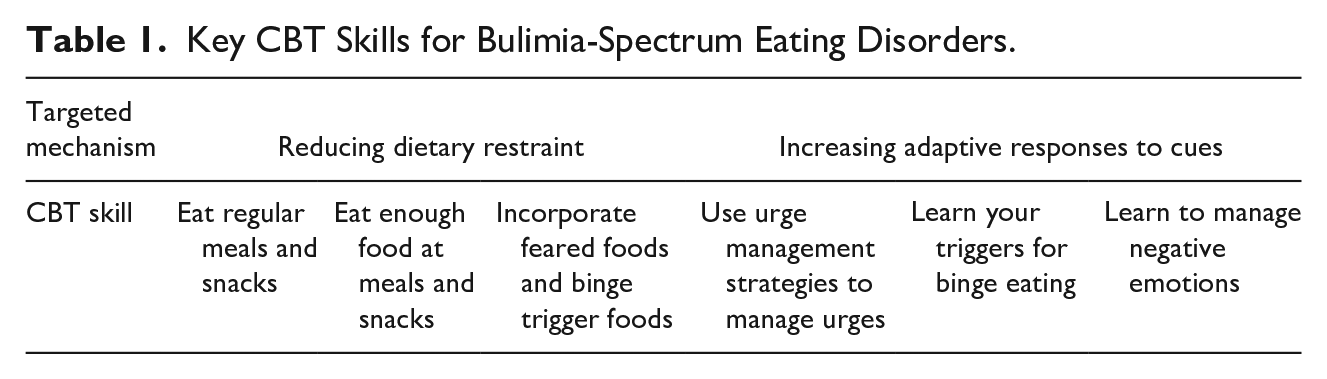
While CBT can be effective, nearly 70% of individuals with BN fail to achieve remission after a full course of CBT (Linardon & Wade, 2018). A key factor that may explain poor treatment response is suboptimal rates of skill utilization (Zendegui et al., 2014). Ample research has shown that poor utilization of skills designed to reduce dietary restraint consistently predicts worse outcomes in treatment, and studies of mechanisms within CBT for BN substantiate the role of reduced dietary restraint in driving clinical outcomes (Steel et al., 2000; Thiels et al., 2001; Towell et al., 2001; Troop et al., 1996; Westra et al., 2007; Wilson et al., 2002). Although less well-studied, failure to adaptively respond to cues for binge eating (particularly failure to regulate negative affect) is strongly associated with BN symptoms (Fischer et al., 2013; Lavender et al., 2015). Emerging literature has also shown that reduced ability to manage negative affect during CBT for BN is a strong predictor of poor outcomes (Peterson et al., 2017; Wilson et al., 2002). Thus, failure to sufficiently improve skills utilization may substantially contribute to poor treatment outcomes.
Improvements in utilization of CBT skills for reducing dietary restraint and increasing adaptive responses to cues could improve treatment outcomes for BN. One approach to improving skills utilization during CBT for BN is to identify interventions that can help select opportunities for skill use during day-to-day life and provide targeted interventions to facilitate skill utilization during these moments. Just-in-time, adaptive interventions (JITAIs; Nahum-Shani et al., 2018) are particularly well suited to improve skills utilization outside the therapy office during CBT for BN. JITAIs are a smartphone intervention design that uses sophisticated algorithms to determine the timing and content of app delivered micro-interventions (Spruijt-Metz & Nilsen, 2014). A growing body of research has shown the promise of JITAIs as treatment augmentations for multiple mental health conditions (Wang & Miller, 2020).
JITAIs can facilitate skill utilization and acquisition via several pathways. First, JITAIs can improve awareness of when to use CBT skills by collecting, synthesizing, and sharing patterns of real-time data about triggers and behaviors (e.g., through self-monitoring data) with users. Second, JITAIs can facilitate skills practice by delivering interventions that coach users on how to use specific therapeutic skills at relevant times (Nahum-Shani et al., 2018). Third, JITAIs can synthesize data about skills utilization and deliver targeted interventions to enhance skills use during app-identified moments when the patient will benefit from feedback on skills utilization (Aldhaban, 2012; Oulasvirta et al., 2012; Wilansky et al., 2016). Emerging research has shown the promise of JITAIs in improving skills utilization (Levin et al., 2019; Reger et al., 2013, 2015; Wang & Miller, 2020), substantiating their high potential to improve treatment outcomes from CBT for BN.
Our team recently developed a JITAI system (CBT+) to deliver interventions to increase therapeutic skills utilization during CBT (Juarascio et al., 2021). Results from a small pilot feasibility and acceptability trial (n = 5) where all participants received 16 sessions of CBT and used the CBT+ app showed large improvements in CBT skills and clinically significant reductions in BN symptoms at post-treatment. However, this pilot trial only included five individuals and had no comparison condition. The current study is designed to assess the feasibility and acceptability of the CBT+ system when used in conjunction with CBT, evaluate the ability of the JITAIs within the CBT+ system to improve skill utilization, examine pre- to post-treatment changes in ED symptoms among individuals receiving JITAIs alongside CBT+, and provide a preliminary estimate of the independent efficacy of JITAIs within the CBT+ system to inform design of a future fully powered randomized controlled trial. Accordingly, 56 individuals with BN-spectrum EDs received 16-sessions of CBT-E focused version (Fairburn, 2008) and were randomized to either (1) use the CBT+ app for self-monitoring only (JITAIs-Off) or (2) use the CBT+ app for both self-monitoring and JITAIs (JITAIs-On). We hypothesized that (1) the CBT+ system would be feasible and acceptable, (2) individuals in JITAIs-On would show greater skill utilization compared to JITAIs-Off, and (3) individuals in JITAIs-On would show greater improvements in BN symptoms compared to JITAIs-Off.
Materials and Methods
Participants
Participants were 56 individuals with BN-spectrum EDs recruited from Philadelphia (pre-COVID-19 pandemic; n = 51) and nationally (during COVID-19; n = 5; 3 in JITAIs-On condition and 2 in JITAIs-Off condition) through flyers and radio and social media advertisements. Inclusion criteria were reporting ≥12 binge episodes and ≥12 compensatory behaviors in the last 3 months, age 18 to 70, BMI > 17.5, and willingness to use a smartphone application to track all eating episodes for 16 weeks. Exclusion criteria for the study were inability to speak, read, or write English, medical complications prohibiting safe outpatient treatment, comorbid diagnosis of psychotic disorder, bipolar disorder, substance use disorder, intellectual disability, or pervasive developmental disorder inhibiting engagement in study procedures, previous full course of CBT, current or planned pregnancy, and history of bariatric surgery.
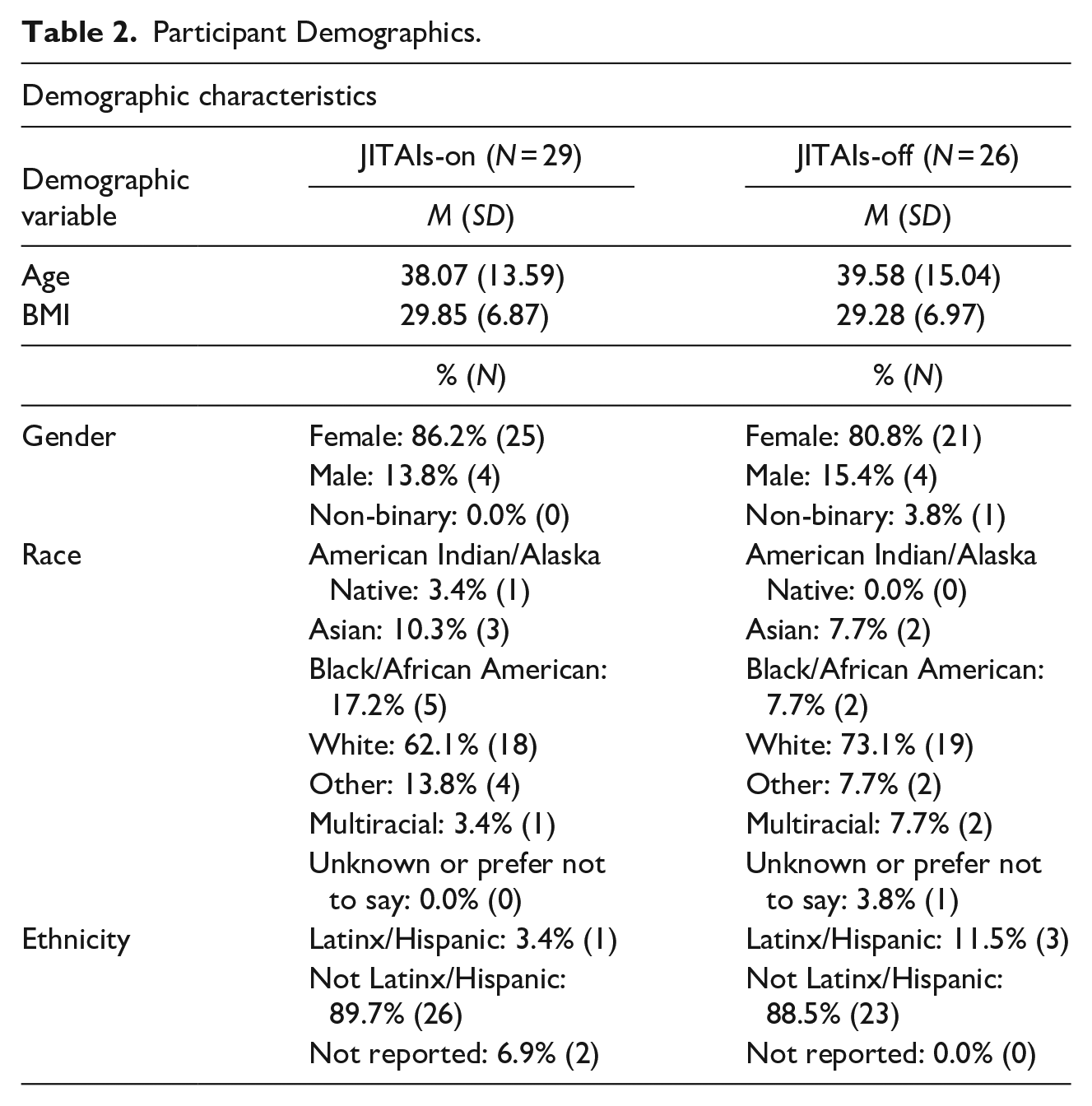
Participants were 83.9% female, 14.3% male, and 1.8% gender non-binary. Participants self-identified as 64.3% White, 8.9% Black, 7.1% Asian, and 19.6% multiracial or other. Four participants (7.1%) identified as Latinx/Hispanic. Participants had a mean age of 38.9 years (SD = 14.1) and mean BMI of 29.5 kg/m2 (SD = 6.8). Despite BMI inclusion criteria being set at >17.5 kg/m2, all participants had BMI >18.5 kg/m2. Participants primarily met behavioral criteria for DSM-5 BN (92.9%) with the rest of the sample (7.1%) meeting criteria for a BN-spectrum Other Specific Feeding and Eating Disorder (OSFED; e.g., BN with only subjectively-large binge episodes).
Procedures
Participants completed phone screening and a baseline assessment to confirm eligibility (see Figure 1 for flow diagram of participant retention). Eligible participants were randomly assigned to treatment conditions stratified by Eating Disorder Examination (EDE) global score, age, and gender. Enrolled participants completed mid-treatment, post-treatment, and 3-month follow-up assessments, which included completion of a semi-structured interview (EDE) to measure ED symptoms, self-report measures, and behavioral tasks. Participants also completed qualitative feedback interviews after the 4th, 8th, 12th, and 16th sessions. Informed consent was provided by all participants and study procedures were overseen by the University’s Institutional Review Board. Assessments and therapy sessions were initially conducted in-person, but during COVID-19 pandemic assessments and therapy sessions were completed virtually using the University’s HIPAA-compliant Zoom videoconferencing platform. The only change associated with virtual therapy and assessment procedures was the use of Zoom and a substantial number of participants in both conditions (8 in JITAIs-On and 12 in JITAIs-Off) completed at least some virtual therapy sessions. The CBT+ smartphone application and clinician portal were used the same way during in-person and virtual therapy sessions.
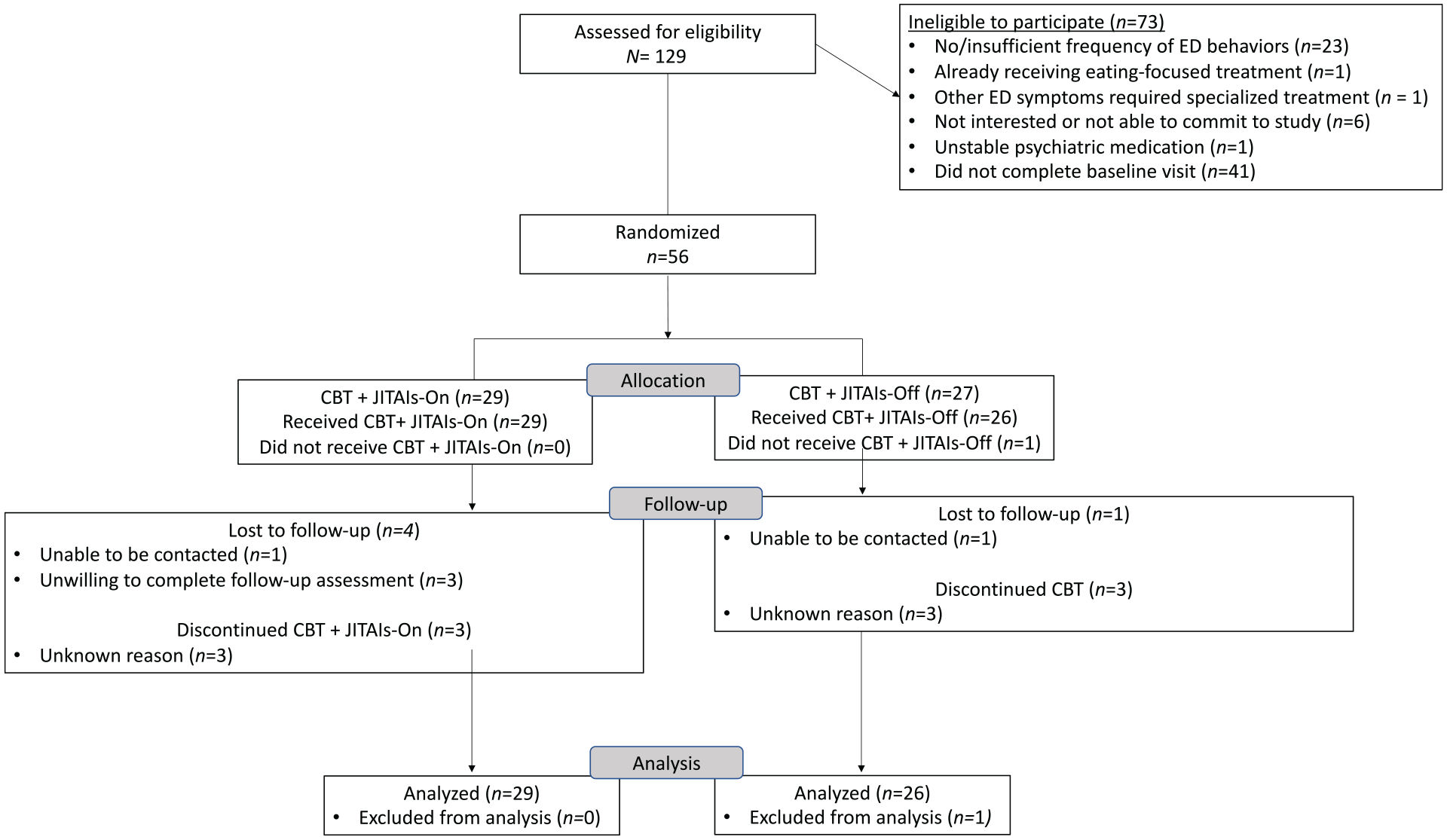
Flow diagram of participant retention.
Treatment
Participants received 16 weekly sessions of manualized, individual CBT-E focused version (CBT-E; Fairburn, 2008). Treatment was delivered by master’s and doctoral students, postdoctoral fellows, and licensed clinical psychologists who received weekly group supervision by a licensed clinical psychologist.
Adjunctive Smartphone Application
Participants used the CBT+ smartphone application to complete digital self-monitoring records throughout treatment (including self-monitoring of treatment skill usage to measure target engagement in both conditions). Self-monitoring included self-monitoring of eating behaviors (e.g., meal frequency and timing and food consumed), ED symptoms (e.g., binge eating, compensatory behaviors, and dietary restraint behaviors like restricting the amount or type of food consumed), and skills usage. Skills usage was monitored via several questions, including “What is the longest amount of time that’s elapsed between planned eating episodes since your last entry” (regular eating), “Have you used an urge management strategy?” (Urge management). “Have you used a mood management strategy?” (Management of negative emotions). Participants in the JITAIs-On condition received JITAIs (push notifications and in-app interventions) based on information inputted into the app in self-monitoring records. Push notifications included reminders to self-monitor in the app (which were sent anytime more than five waking hours elapsed without making an entry) and personalized notifications, the content and timing of which could be manually set by a clinician. In-app interventions were delivered following completion of a self-monitoring record that identified a skill use opportunity (e.g., a record in which a participant reported restrictive eating or urges to binge or use a compensatory behavior). These interventions included a brief description of the identified skill the patient should practice, rationale for practicing the skill, and specific instructions on how to try out the skill in real time (see Juarascio et al., 2021 for a full description of the CBT+ system and its development).
Measures
Eating pathology
The Eating Disorder Examination measured frequency of binge eating and compensatory behaviors and ED pathology (Fairburn et al., 2014). The EDE yields four subscale scores (Restraint, Eating Concern, Shape Concern, and Weight Concern) and a global score, with higher scores indicating more severe ED pathology.
Participant skill use
At each therapy session, participants self-reported their average skill use over the previous week using questions that were developed for this study (to allow for the measurement of CBT for BN-specific skill use). Skill use was rated on a 5-point scale, with the following anchors: 1 = No skill use, 2 = Skill use 1% to 25% of the time, 3 = Skill use 26% to 50% of the time, 4 = Skill use 51% to 75% of the time, and 5 = Skill use 76% to 100% of the time.
App usage
Measures of use of CBT+, including number of entries completed per day, were quantified from data collected by the smartphone application.
Acceptability
Participants rated statements about the acceptability of CBT+ based on the Technology Acceptance Model. Ratings were made on 7-point Likert scales with 1 = Strongly Disagree and 7 = Strongly Agree at the 16th session. See Table 2 for acceptability statements. Participants also completed acceptability interviews after sessions 4, 8, 12, and 16 in which they were asked open-ended questions about their experience of using the CBT+ app, such as “How would you describe your overall experience with the CBT+ app?”, “What do you like about CBT+?”, “What do you dislike about CBT+?”, and “Please describe any problems or bugs you have experienced when using the CBT+ app.” Participant responses were transcribed, and the data were reviewed by one study staff members for analysis. Themes that were common across multiple participants were extracted and quotes that exemplified these themes were selected for inclusion in this article.
Participant Demographics.
Statistical Analysis
Missing acceptability, target engagement, and treatment outcome data were imputed with five iterations using predictive mean matching and the R package “mice.” Descriptive statistics were calculated for all measures of acceptability, target engagement, and treatment outcomes. Independent samples t-tests compared treatment conditions on frequency of app use and acceptability ratings. Within-group general linear models were used to examine the pre- to post-treatment change in binge eating, compensatory behaviors, and EDE subscale and global scores. General linear models also examined the main effects of time, treatment condition, and the time by treatment condition interaction on target engagement and treatment outcome variables. Specifically, zero-inflated negative binomial models were fit for binge eating episodes and compensatory behaviors, zero-inflated gamma models were fit for EDE subscales scores, and a gaussian general linear model was fit for EDE global score. Attrition and remission rates were investigated by computing percentages and compared between groups using Pearson’s chi-square tests. Effect size estimates (Cohen’s d for independent samples t-tests and phi for chi-square tests) and 95% confidence intervals for estimates were reported given that the study was underpowered as a pilot study. All analyses were conducted in SPSS version 26.0 or R version 4.0.3. The p-values < .05 were considered statistically significant.
Results
Table 2 summarizes participant demographic characteristics. Pre- to post-treatment attrition was 10.7% across the entire sample. Attrition did not significantly differ between conditions at any time point (all p’s > .05; see Table 3). On average, participants made 3.01 entries per day across all treatment sessions (SD = 1.49) and number of entries did not significantly differ by condition. Compliance with self-monitoring in the app slightly declined after mid-treatment, with the sample reporting 3.31 entries per day on average between session 1 and 2 (SD = 1.46), 3.35 entries per day between sessions 8 and 9 (SD = 1.76), and 2.13 entries per day between sessions 15 and 16 (SD = 1.78). Both conditions rated the acceptability of the app similarly, although the JITAIs-On group rated “I find CBT+ easy to use” significantly higher than the JITAIs-Off group with medium effect size.
Feasibility and Acceptability of CBT+.

Table 4 depicts qualitative feedback on the acceptability of the full CBT+ system. Emergent themes regarding acceptability of the CBT+ system include the benefits of supportive accountability to a therapist, the usefulness of targeted, personalized feedback provided by the therapist via CBT+, JITAIs as reminders to use skills in real time, and tracking of skill use as a potent intervention even without JITAIs. In particular, participants reported that using the app allowed them to feel consistently accountable to their therapist via collecting accurate data on their eating patterns and allowing for in-the-moment communication to their therapist. Participants also described that having the ability to decide what interventions they would receive, and feeling that interventions were accurate and tailored to the factors maintaining their eating disorder contributed to the CBT+ app’s efficacy. Qualitative feedback also emphasized the helpfulness of both JITAIs and skills tracking (even in the absence of JITAIs) for reminding participants to practice therapeutic skills in real time. Overall, participants endorsed that thinking about skills, as prompted by skills monitoring and/or JITAIs, was helpful in facilitating skill acquisition and utilization between sessions.
Qualitative Participant Feedback on the CBT+ System.

Unexpectedly, target engagement results indicated that both conditions demonstrated greater skill use by session 16 compared to session 1 with no significant time by treatment condition interactions (see Table 5). Within the JITAIs-On condition, participants increased their use of skills for reducing dietary restraint from an average rating of 3.07 (corresponding to skill use 26%–50% of the time) at week 1 to 4.24 (corresponding to skill use 51%–75% of the time) at week 16 for regular eating, from 3.41(skill use 26%–50% of the time) at week 1 to 4.38 (skill use 51%–75% of the time) at week 16 for eating enough at meals and snacks, and from 2.45 (corresponding to skill use 1%–25% of the time) at week 1 to 3.79 (skill use 51%–75% of the time) at week 16 for incorporating feared foods. Regarding skills for increasing adaptive responses to cues, participants in the JITAIs-On condition increased their skill use from an average rating of 1.45 (corresponding to no skill use) at week 1 to 3.28 (skill use 26%–50% of the time) at week 16 for managing negative emotions, from 3.24 (skill use 26%–50% of the time) at week 1 to 4.55 (skill use 76%–100% of the time) at week 16 for awareness of binge triggers, and from 1.34 (no skill use) at week 1 to 3.86 (skill use 51%–75% of the time) at week 16 for urge management. There were significant, main effects of time on pre- to post-treatment binge eating episodes (both groups), compensatory behaviors (JITAIs-Off group), EDE subscale scores (both groups) and EDE global score (both groups; see Table 6). There were no significant main effects of treatment condition or significant time by treatment condition interaction effects on treatment outcomes (see Table 6). There was a notable pattern in change in binge eating frequency between post-treatment and follow-up, in which the JITAIs-Off group demonstrated a 76% increase on average whereas the JITAIs-On group demonstrated no change.
Target Engagement.

Treatment Outcomes.

Note. Treatment outcomes and remission are based on past-month ED behaviors. Total binge episodes include objectively- and subjectively-large binge episodes. Total compensatory behaviors include self-induced vomiting, laxative misuse, diuretic misuse, driven exercise, chewing and spitting, 24-hour fasting, 8 hour compensatory fasting, and other extreme weight control behaviors. Between group comparisons reflect the count regression model within the zero-inflated regression models (see Supplemental Table 1 for complete models).
Discussion
This study evaluated the first JITAI system designed to augment CBT for BN-spectrum EDs to improve therapeutic skills utilization. Consistent with hypotheses, the CBT+ system was found to be a feasible and acceptable augmentation to CBT for BN-spectrum EDs. Treatment retention was high in this study, with higher rates of retention in both conditions than those reported in other studies examining ecological momentary intervention systems including JITAI systems (Arean et al., 2016; Pramana et al., 2014; Pulantara, 2017; Reger et al., 2015). Participants showed good adherence to app use and data entry on the CBT+ app throughout active treatment. According to qualitative feedback, factors for high adherence included (1) finding monitoring using the CBT+ app directly relevant to CBT treatment and routine review and feedback by therapists regarding app-collected data during sessions, (2) the low-burden user interface of the CBT+ app that allowed participants to quickly complete data entry, and (3) considering CBT+ helpful in keeping participants accountable to their therapist and treatment goals. A slight decline in number of data entries occurred during the late-treatment phase (i.e., session 15–16), possibly due to some individuals deciding to “taper-off” self-monitoring (a standard recommendation in CBT to prepare for treatment termination), as tracking remained consistent throughout treatment until these final weeks. Another possible explanation for declining-entry trend is that participants became increasingly familiar with triggers and contexts associated with binge eating over time, and no longer perceived a need to self-monitor to gain awareness into these factors.
Participants in both conditions reported high acceptability of the CBT+ app, though participants in the JITAIs-On condition were significantly more likely to indicate that CBT+ was easy to use compared to JITAIs-Off. Qualitative results found that participants in the JITAIs-On condition reported that the micro-interventions were helpful in facilitating the use of therapeutic skills during moments when they experienced triggers for binge eating. Participants also perceived the micro-interventions designed by their therapist to be relevant, personalized to their needs, and helpful in providing support to address treatment-interfering behaviors (e.g., push notifications scheduled to remind participant to reduce alcohol use to prevent binge eating). Moreover, participants in the JITAIs-On condition perceived the micro-interventions as an extension of therapist support in the real-world. If replicated, these findings may suggest that JITAI systems are an acceptable augmentation to CBT among individuals with BN.
Qualitative acceptability data also suggest that the inclusion of skills-monitoring alone in CBT+ was surprisingly effective for encouraging skill utilization. The skills-monitoring component was included in both conditions to collect data on frequency of skill use. The positive results in both conditions combined with qualitative data noting the perceived utility of skills-monitoring suggest that the skills-monitoring component of CBT+ may have inadvertently replicated some possible benefits of the JITAIs-On condition such that our JITAIs-On and JITAIs-Off conditions were too similar to detect significant differences. Skills-monitoring may have functioned similarly to micro-interventions (e.g., increasing goal salience and providing reminders to use skills). In qualitative feedback interviews, participants in both conditions emphasized the utility of skills-monitoring in CBT+ for prompting reflection on skill use and treatment progress between sessions. Future research is needed to isolate the impacts of skills-monitoring and JITAIs to determine the additive value of each technological component.
Perhaps due to high overlap between conditions, the JITAIs-On condition did not produce higher rates of skill utilization than the JITAIs-Off condition. Frequent skills monitoring in the CBT+ app across conditions may have reminded all participants to practice therapeutic skills. It is also plausible that the review of skills use and encouragement for skills practice by study clinicians during treatment sessions may have produced all observed improvements in skills utilization in both conditions with no added benefit of CBT+. For example, on qualitative interviews, participants in both conditions reported feeling highly accountable to their clinicians for practicing skills (e.g., regular eating). Future research is needed to test whether technological augmentations to treatment like the CBT+ app can improve skill use compared to CBT without any technological augmentations.
Unexpectedly, participants in the JITAIs-On condition did not show greater significantly greater improvements in BN symptoms compared to those in the JITAIs-Off condition. Given the study’s low power to compare two active treatment conditions, it is important to consider patterns in results that may warrant future study. There was a notable pattern in post-treatment to follow-up change in frequency of binge eating, in which the JITAIs-Off group demonstrated a 76% average increase whereas the JITAIs-On group demonstrated no change, suggesting a possible role for JITAIs in relapse prevention. If replicated in a larger, fully powered clinical trial, these results may support the promise of integrating a JITAI system in CBT for BN for maintaining improvements in binge eating.
Strengths and Limitations
The current study faced several limitations. First, as is typical for ED studies, most participants were White women. Future research should attempt to replicate our findings in more diverse samples. Second, the measure of skill use that participants completed each week has not been validated. Problems with the measure performance may have contributed to the lack of group differences identified in the present study. Third, because both conditions in the present study included several common intervention components (e.g., digital self-monitoring, skills-monitoring, and data sharing with a treatment clinician) that may have contributed to improvements in skills use and BN pathology, our conditions may have been insufficiently distinct to identify differences between conditions in a small pilot trial. Future research should isolate these different technological intervention components that may impact skills utilization and clinical outcomes to identify unique contributions of digital health systems. Fourth, we did not have a condition where individuals received CBT without using any components of the CBT+ system, preventing us from making any conclusions about whether the CBT+ system improved skill utilization or clinical outcomes over CBT alone. Strengths of the study include the use of a rigorous comparison condition and use of a multi-modal assessment procedure including objective data from the CBT+ app, qualitative interviews and self-report measures of acceptability, and a clinical interview for assessing BN symptoms.
Conclusions
In sum, present study successfully deployed the first ever JITAI system as an augmentation to CBT for improving skills utilization and clinical outcomes in individuals with BN-spectrum disorders. Our findings suggest that JITAI systems are a feasible and acceptable augmentation to treatment and are worthy of additional study in fully powered clinical trials.
Supplemental Material
sj-docx-1-bmo-10.1177_01454455221109434 – Supplemental material for A Randomized Controlled Trial of CBT+: A Clinician-Controlled, Just-In-Time, Adjunctive Intervention for Bulimia-Spectrum Disorders
Supplemental material, sj-docx-1-bmo-10.1177_01454455221109434 for A Randomized Controlled Trial of CBT+: A Clinician-Controlled, Just-In-Time, Adjunctive Intervention for Bulimia-Spectrum Disorders by Adrienne S. Juarascio, Emily K. Presseller, Paakhi Srivastava, Stephanie M. Manasse and Evan M. Forman in Behavior Modification
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by a grant from the National Institute of Mental Health (R34MH116021) to Adrienne S. Juarascio.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.