
Abstract

A 62-year-old male presented to the Laryngology Clinic 3 months after Direct Microlaryngoscopy with CO2 laser excision of a left vocal fold lesion. Pathology revealed ulceration with granulation tissue and inflammation. His only complaint was continued intermittent discomfort in the right side of his throat with swallowing. On laryngoscopy, a recurrent left vocal process granuloma was present.
Recommendations included treatment for laryngopharyngeal reflux. The patient started omeprazole 40 mg PO 30 minutes prior to breakfast and Zantac 300 mg PO before bedtime for 3 months. Dietary and lifestyle modifications were also recommended.
An in-office steroid injection was performed into the lesion. The Boston Scientific Interject needle (Spencer, IN) was inserted through the channeled part of the laryngoscope to the left vocal process granuloma. 1.0 mL of triamcinolone 40 mg/1 mL concentration was injected in the granuloma. The plan was followed up in 1 month to reassess the granuloma and possible repeat injection.
Upon follow-up, strobovideolaryngoscopy showed the left vocal process granuloma that had decreased in size from previous visit. Triamcinolone plaque was present on the superior surface of the left true vocal fold (Figures 1 and 2). Bilateral true vocal fold movement was symmetrical with minimal decrease in mucosal wave of the left vocal fold compared to the right. Hyperfunction with lateral compression was present. Periodicity was regular. The patient reported a raspy voice since the previous injection. He opted for removal of the plaque in the operating room versus nonsurgical treatment.

Triamcinolone plaque in left vocal fold abduction.
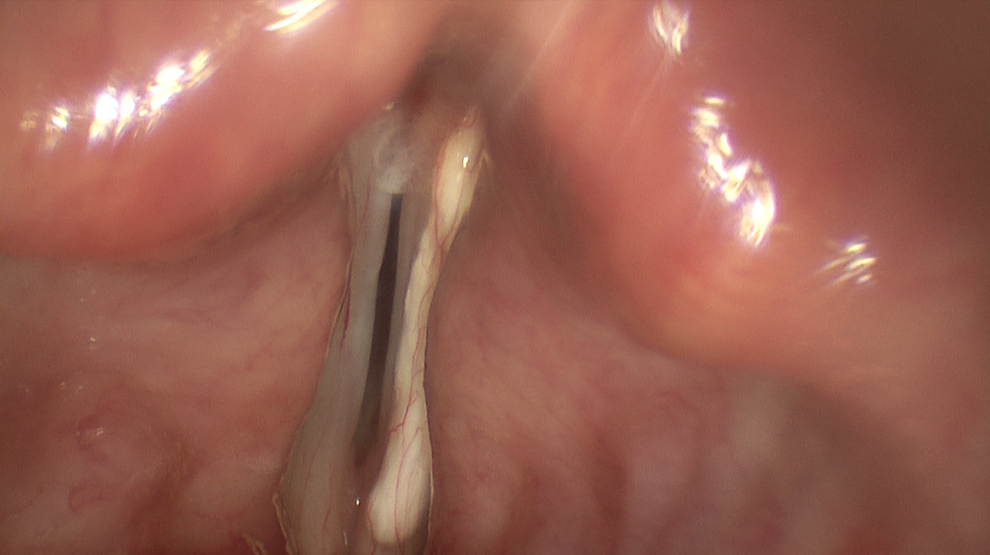
Triamcinolone plaque in left vocal fold adduction.
Vocal process granulomas are benign laryngeal lesions with controversial treatment and a tendency to recur. There are several treatment options with unpredictable results, high recurrence rates, and disappointing long-term outcome. The 3 most common treatment options are antireflux therapy, mostly proton pump inhibitors, voice therapy, and steroids. Surgical excision is usually reserved for refractory or recurrent cases. Botulinum toxin injection into the lateral cricoarytenoid muscle also has been effective. Intralesional steroids have been used to good effect with a 60% resolution rate following monthly injections. 1 Inhaled steroids, specifically triamcinolone, have been reported in the literature. 2 Dexamethasone solution is clear and does not leave any residual deposit. The triamcinolone plaque is believed to be the result of the chalky material present in the triamcinolone suspension itself. The steroid injected should not contain components that can form a precipitate. Moreover, liquids injected under pressure can travel easily beyond the intended area as occurred in this case. So, the use of an aqueous steroid for injection anywhere in the larynx is prudent.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.