
Abstract

Laryngeal tuberculosis (TB), caused by Mycobacterium tuberculosis, is a rare form of extrapulmonary TB. Currently, with the advance of effective anti-TB drugs and the natural decline of TB in the developed countries, its incidence is estimated to be less than 1% of all TB cases, though it may be more commonly seen in immunocompromised patients. 1
An 84-year-old male patient denied any systemic diseases or medications. He visited our gastroenterology department on account of dysphagia, odynophagia, and throat lumping sensation for 5 months, during which period a body weight loss of 10 kg was also noted. Panendoscopy was done and an ulcerative lesion of epiglottis was noted (Figure 1). The gastrointestinal tract was without abnormal findings. The patient was referred to our otorhinolaryngology department, under the impression of epiglottis tumor, for further evaluation. The patient was then admitted. Chest X-ray revealed mixed pattern opacity over bilateral lung fields (Figure 2) and mycobacterium tuberculosis or nontuberculous mycobacterium infection was suspected. Due to the patient’s old age and abnormal chest X-ray (CXR) finding, office-based flexible laryngoscopy was arranged for tissue biopsy. At the same time, head and neck computed tomography scan showed epiglottis tumor with aryepiglottic folds extension. Despite negative finding of sputum acid-fast stain, the histopathological findings revealed several granulomas with Langhans giant cells and identified several acid-fast bacilli (Figure 3). The patient then received antituberculous agents AKuriT-4 (Rifampin + Isoniazid + Ethambutol + Pyrazinamide). A repeated laryngoscopy performed 1 month after commencement of treatment revealed almost complete regression of the lesion.
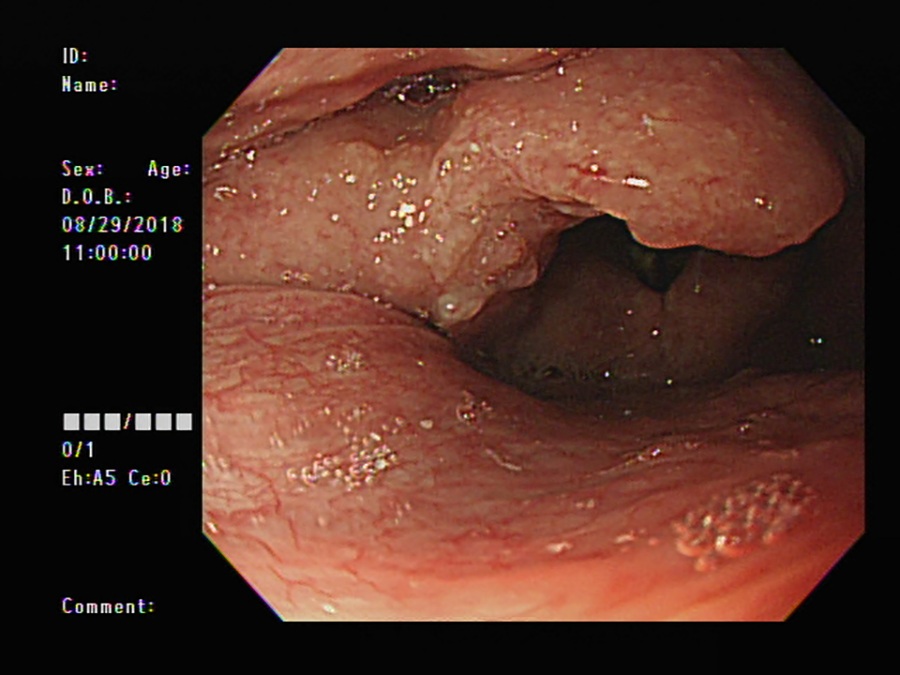
Panendoscopy reveals an ulcerative lesion of epiglottis; the gastrointestinal tract is without abnormal findings.

Chest X-ray reveals mixed pattern opacity over bilateral lung fields.
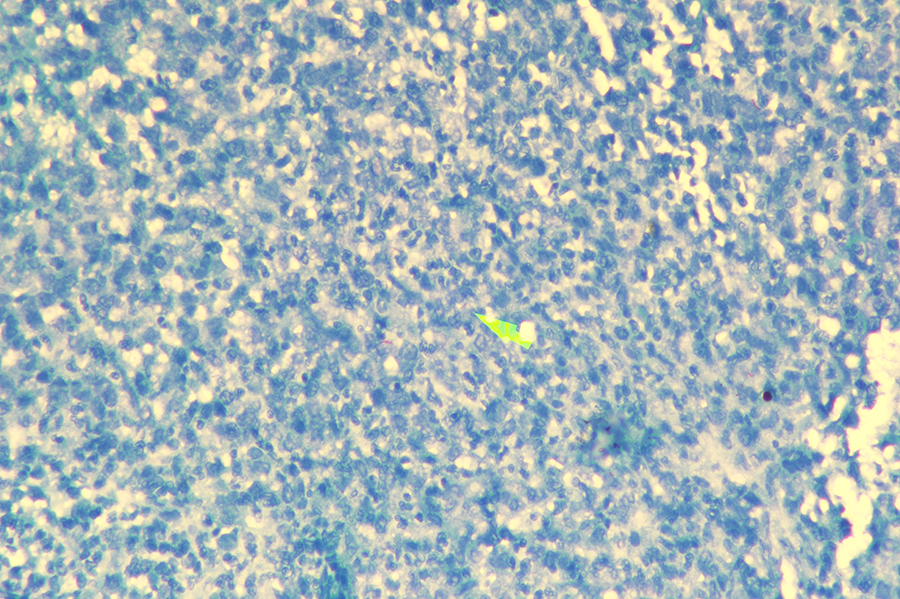
Histopathology under microscope reveals several granulomas with Langhans giant cells and also several acid-fast bacilli identified (arrow).
Laryngeal TB and malignancy share similar clinical presentations of local symptoms such as hoarseness, dysphagia, odynophagia, cough, stridor, hemoptysis, and, less predominantly, systemic complaints such as fever, night sweats, body weight loss, and cervical lymphadenopathy. Dysphonia was the most common symptom, followed by body weight loss, cough, dysphagia, and odynophagia. 2 Particularly, dysphonia and body weight loss may often raise the suspicion of malignancy. It was also hardly distinguishable even with laryngoscopy and image surveys.
Initial diagnosis as carcinoma is often made in laryngeal TB and is generally not considered until confirmed by preoperative CXR, biopsy pathology, or sputum acid-fast stain. Since TB has a potent infectivity, the US Centers for Disease Control and Prevention has emphasized the importance of acknowledging the changes in clinical characteristics, diagnostic points, early diagnosis, and timely treatment of the disease. 3 In this report, we presented a case of primary pulmonary TB with involvement of epiglottis, mimicking as laryngeal carcinoma initially.
According to Cleary and Batsakis, among laryngeal TB, vocal cords are the most commonly affected site (50%-70%), followed by false cords, epiglottis, aryepiglottic folds, arytenoids, posterior commissure, and subglottis. 4 Previous findings suggested that laryngeal TB was typically seen in those with long-time bedridden status, which might lead to accumulation of infective sputum bacilli at the posterior larynx. 3,5 Shin et al suggested that laryngeal TB may spread predominantly by blood and lymphatic fluid due to the finding that involvement of anterior larynx was more predominant than the arytenoids or posterior commissure. 5 Zhao et al reported a series of 61 cases showing similar findings that involvement of laryngeal TB in the anterior half of the larynx occurs trice as often as in the posterior half. 3 In our reported case, the patient was not bedridden and the involvement of epiglottis was previously considered rare. Taken these studies and our case report together, a change in laryngeal TB manifestation should be noted.
In conclusion, even though the prevalence of TB infection has decreased in recent decades, underrecognition and lack of clinical awareness likely contribute to underreporting. Otorhinolaryngologists should keep in mind the possibility of TB in the differential diagnosis of larynx tumors and the changing trend of clinical manifestations of laryngeal TB. Last but not least, laryngeal TB and carcinoma can coexist in the same time and laryngoscopy findings are often indistinguishable. Thus, biopsy should be taken from all suspicious lesions and at multiple sites. The most of all, we should never neglect the protective measures from being exposure to contagious diseases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.