
Abstract
Objective
The role of hearing loss (HL) in surgical outcomes is not well studied and could greatly impact the lives of patients in the post-operative setting.
Study Design
This is a retrospective cohort study of adults who underwent subspecialty surgeries in Otolaryngology. Patients were recruited from 58 health care organizations in the TriNetX Research Network.
Methods
Analysis was performed on data from January 2004 to January 2024. Patients with a history of subspecialty otolaryngologic surgical procedures with HL. Cohorts were matched for demographics, comorbidities, and hearing aid use. Post-surgical complications within 30 days of procedure were compared between patients with HL and those without.
Results
Rates of post-op surgical site infection (SSI) were higher in patients who had HL after Head and Neck (HN) procedures compared to those who did not (AR 2.03%, OR 1.22, [1.01 – 1.48], P < 0.01). Emergency Department (ED) visits after surgery were higher in the HL cohort for HN (AR 8.12%, OR 1.31, [1.20 – 1.49], P < 0.01), and Facial Plastic and Reconstructive Surgery (FPRS) (AR 4.58%, OR 1.13, [1.05 – 1.22], P < 0.01). Rates of wound disruption was higher in patients who had HL after HN procedures compared to those who did not (AR 1.34%, OR 1.27, [1.01 – 1.61], P < 0.05). In otology, HL patients had lower rates of cellulitis and abscess, and wound disruption (P < 0.05), along with lower rates of ED visits and readmission (P < 0.01.
Conclusion
Patients with HL had a higher risk of ED visits with HN, and FPRS procedures. The rate of SSI and dehiscence was higher in the HL cohort for HN.
Level of evidence
Level III (retrospective cohort study).
Introduction
Hearing loss (HL) is prevalent in the elderly population. Presbycusis, otherwise known as age-related sensorineural hearing loss (SNHL), is one of the most common age-related conditions affecting older adults and is only second to cardiovascular and arthritic diseases. 1 In the United States alone, HL affects about 27% of adults ages 60 to 69, 55% of those ages 70 to 79, and 79% of those ages 80 and older, with the prevalence of HL increasing every decade of life. 2
With presbycusis being so prevalent, hearing aids are used as a common intervention for age-related SNHL. However, while many patients receive hearing aids for their HL, a survey study comprising over 20,000 responses showed that 77% of patients had “a lot of trouble” using their hearing aids, and 50% of patients had “moderate trouble” while using their hearing aids. 3 Studies have gone on to demonstrate that patients with HL have higher Emergency Department (ED) visits, hospital readmission, and mortality for multiple medical disorders and general surgery procedures.3-5 This accounts for increased medical costs for patients and the healthcare systems, which thereby increases the care burden placed on hospitals that care for those with HL.
While there is a large HL population with specific care needs, there is little research that has been done on surgical outcomes in patients who have HL. One recent study published the association of hearing loss with post-surgical outcomes for major surgeries across multiple specialties. 6 However, otolaryngology surgical procedures constitute a wide array of diversity, with both minor and major procedures across multiple subspecialties. As a specialty that is responsible and prides itself in caring for patients with hearing loss, it is vital to inform ourselves of how we are caring for patients who have hearing loss so we can adapt to their care needs.
This study specifically evaluates the role of hearing loss, including presbycusis, unilateral SNHL, and bilateral SNHL, in the surgical outcomes of complex and simple otolaryngologic procedures. The span of specialties includes facial plastic and reconstructive surgery (FPRS), head and neck surgery (HN), otology, laryngology, and rhinology with a focus on sinus. As such, we sought to utilize the TriNetX database for a retrospective cohort study to evaluate the postsurgical outcomes of patients with HL.
Methods
Study Design
Data were collected from the TriNetX Research Network, which provided access to electronic medical records from approximately 96 million individuals over the age of 18 from 80 health care organizations. TriNetX is compliant with the Health Insurance Portability and Accountability Act, only contains deidentified data, and was exempted by the Penn State Institutional Review Board from the need for informed consent (STUDY00018629) in accordance with 45 CFR §46.
Data Collection
This database was queried to identify patients over the age of 18 years old, with a diagnosis of presbycusis, conductive HL, unilateral SNHL, or bilateral SNHL who underwent various Otolaryngology procedures from January 1, 2004, to January 1, 2024, using diagnosis (International Classification of Diseases‐10) and procedure codes (Current Procedural Terminology) outlined in Supplemental S1, available online. The cohorts were divided into those who had HL and those who did not have HL any time prior to when they had surgery. Severity of HL was not included due to its absence in coding in the TriNetX database. Cohorts were then further divided based on what subspecialty the procedures would most likely be performed in, including HN, rhinology, FPRS, laryngology, and otology. Sleep medicine was excluded due to small cohort size. While these procedures were categorized by subspecialty, there was no way to confirm that these procedures were conducted by an otolaryngologist or surgeon in another specialty. To avoid cross-over between specialties, FPRS was focused on reconstructive and cosmetic procedures while HN was focused primarily on ablative cases. Rhinology primarily was focused on sinus surgeries due to cross-over between septoplasties and rhinoplasties performed by both FPRS and rhinology.
For rhinology with a focus on sinus surgery CPT codes 31240, 30115, 31276, 31237, and 31239 were used. Laryngology cohort used CPT codes 31541, 1014609, 1014610, 31591, 1005872, 31591, 31561, 1005932, 31545, 31630, and 31631. Otology cohort used CPT codes CPT 69421, 69620, 69631, 69660, 69420, 69661, 69930, 1010163, 1010175, 69610, 69643, 69633, 69641, 69644, 69632, 69645, 69646, 69667, 69637, 69635, 69670, 69662 and 69666 along with SNOMED 31932005. FPRS cohort used CPT codes 30420, 30410, 30400, 30460, 30435, 30430, 30462, 30450, 67900, 101404, 15823, 21453, 21462, 14060, 14061, 14040, 14041, 15630, 15829, 30520, 15120, 67902, 67912, 67917, 67950, and 64716. HN cohort used CPT codes 1009039, 60240, 60500, 60220, 60260, 38724, 38510, 42415, 21046, 21047, 31225, 31230, 31360, 31365, 30150, 30160, 41120, 41130, 41135, 41150, 41153, 41155, 41140, and 41145 along with SNOMED 39497007, and 80496005. Descriptions for all CPT codes used for cohort building are found in Supplemental 1.
Primary outcomes included surgical site infection (SSI), cellulitis and abscess, wound disruption, hospital readmission, ED visits, and death within the first 30 days following surgery. For complications experienced by 1 to 9 patients, TriNetX reports these values as 10 to protect patient confidentiality. Pediatric patients were excluded due to the potential confounding of communication being reliant on their at-home care providers. CPT and ICD-10 codes used for outcomes are listed in Supplemental 2.
Statistical Analysis
Data analysis was performed from January 2003 to January 2024. Statistical analyses were performed within the TriNetX platform, 7 which is based on R, JAVA, and Python, to compare the post-surgical outcomes in varying otolaryngology subspecialty procedures between the HL and non‐HL groups. To reduce confounding bias and maximize external validity, the cohorts were 1:1 propensity score‐matched for demographics (age, sex, race, and ethnicity) and comorbidities using nearest neighbor methods without replacement and a caliper of 0.1 times the standard deviation. The time window for matching characteristics was set for 30 days before surgery through the date of surgery. 8
Comorbidities included ischemic heart diseases (I20‐I25), heart failure (I50), overweight and obesity (E66), metabolic disorders (E70-E88), alcohol related disorders (F10), type 2 diabetes mellitus (E11), and other chronic obstructive pulmonary disease (J44). Patients were also matched for hearing aid use (Z97.4) to reduce confounding from hearing assisted devices. These comorbidities were matched as they may impact postsurgical outcomes and clinical outcomes of interest. TriNetX also utilizes matrices of covariates with rows in randomized order to obtain propensity scores through logistic regression to reduce record order bias. Baseline characteristics with a standardized mean difference between the cohorts lower than 0.1 were used and considered well-balanced. Odds ratio (OR), 95% confidence intervals (CIs), and associated P values were used to evaluate the association between HL and outcomes in the postsurgical setting. Statistical significance was defined as p < 0.05.
Results
A total of 12018 patients with hearing loss who underwent HN procedures between 2004 and 2024 were found within the database. There were 12018 (4.2%) patients in the HL group and 273603 (95.8%) patients in the non-HL group. The mean age was 64.3 ± 12.9 and 55 ± 15.3 in the HL and non-HL group, respectively. The HL group included 5205 males (43.3%) and 9474 Caucasians (78.8%). After 1:1 propensity score matching for age, sex, race, ethnicity, and other relevant comorbidities, there were 12011 in each cohort.
A total of 5700 patients with hearing loss who underwent laryngological surgical procedures between 2004 and 2024 were found within the database. There were 5700 (6.2%) patients in the HL group and 74474 (93.8%) patients in the non-HL group. The mean age was 63.2 ± 12.3 and 58.2 ± 13.6 in the HL and non-HL group, respectively. The HL group included 3502 males (61.4%) and 4491 Caucasians (78.8%). After 1:1 propensity score matching for age, sex, race, ethnicity, and other relevant comorbidities, there were 5696 in each cohort.
A total of 31215 patients with hearing loss who underwent FPRS surgical procedures between 2004 and 2024 were found within the database. There were 31215 (7.0%) patients in the HL group and 348886 (93.0%) patients in the non-HL group. The mean age was 62 ± 16.1 and 53.3 ± 18.4 in the HL and non-HL group, respectively. The HL group included 16938 males (54.3%) and 25986 Caucasians (83.2%). After 1:1 propensity score matching for age, sex, race, ethnicity, and other relevant comorbidities, there were 31206 in each cohort.
A total of 88117 patients with hearing loss who underwent rhinology surgical procedures between 2004 and 2024 were found within the database. There were 15565 (13.5%) patients in the HL group and 564450 (86.5%) patients in the non-HL group. The mean age was 60.7 ± 14.8 and 49.1 ± 16.9 in the HL and non-HL group, respectively. The HL group included 40232 males (45.7%) and 66329 Caucasians (75.3%). After 1:1 propensity score matching for age, sex, race, ethnicity, and other relevant comorbidities, there were 88051 in each cohort.
A total of 73553 patients with hearing loss who underwent otology surgical procedures between 2004 and 2024 were found within the database. There were 73553 (82.1%) patients in the HL group and 16069 (17.9%) patients in the non-HL group. The mean age was 52.5 ± 17.5 and 48 ± 17.2 in the HL and non-HL group, respectively. The HL group included 34404 males (46.8%) and 55128 Caucasians (74.9%). After 1:1 propensity score matching for age, sex, race, ethnicity, and other relevant comorbidities, there were 1546 in each cohort.
Cohorts Demographics Before Propensity Score Matching
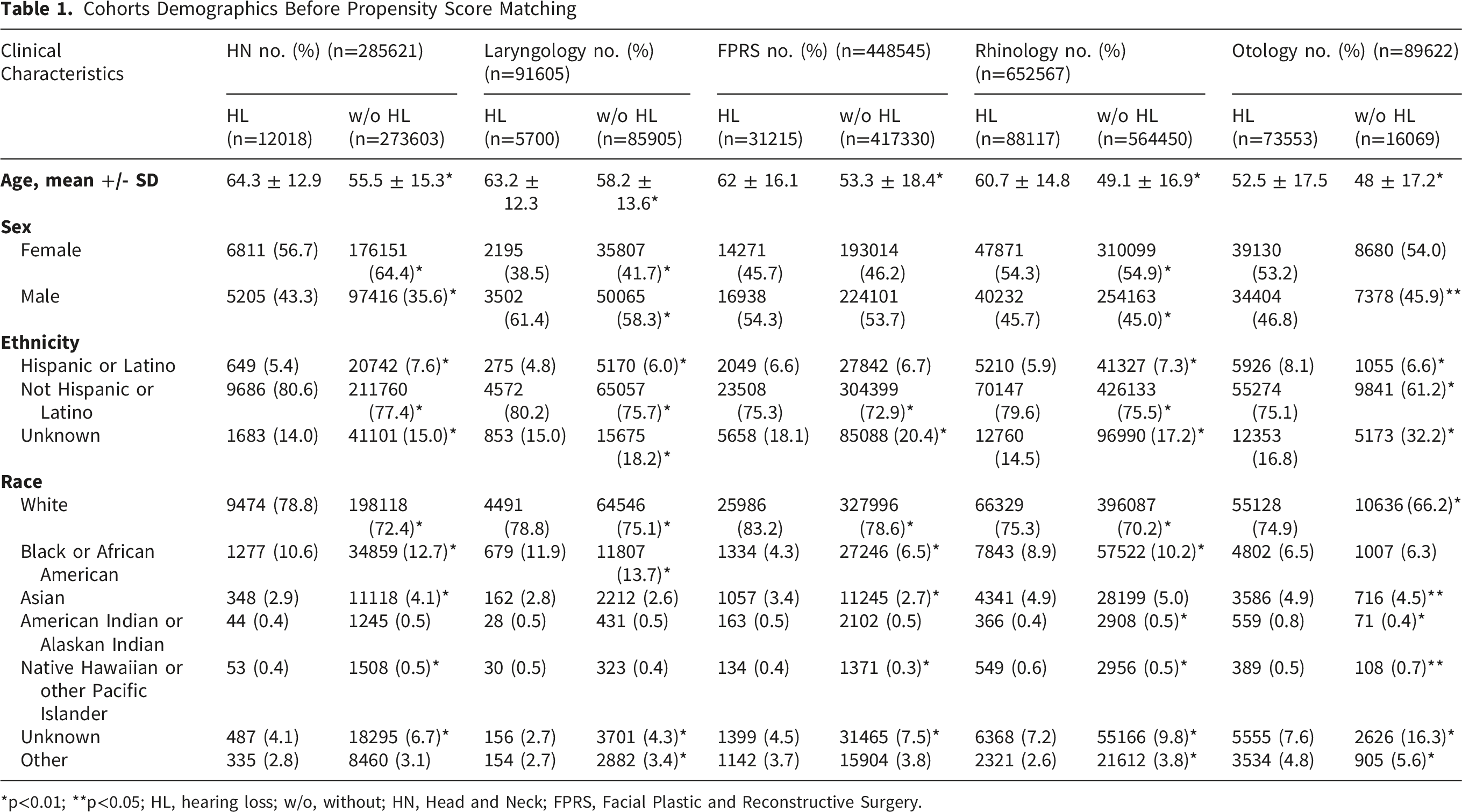
*p<0.01; **p<0.05; HL, hearing loss; w/o, without; HN, Head and Neck; FPRS, Facial Plastic and Reconstructive Surgery.
Cohorts Comorbidities Before Propensity Score Matching
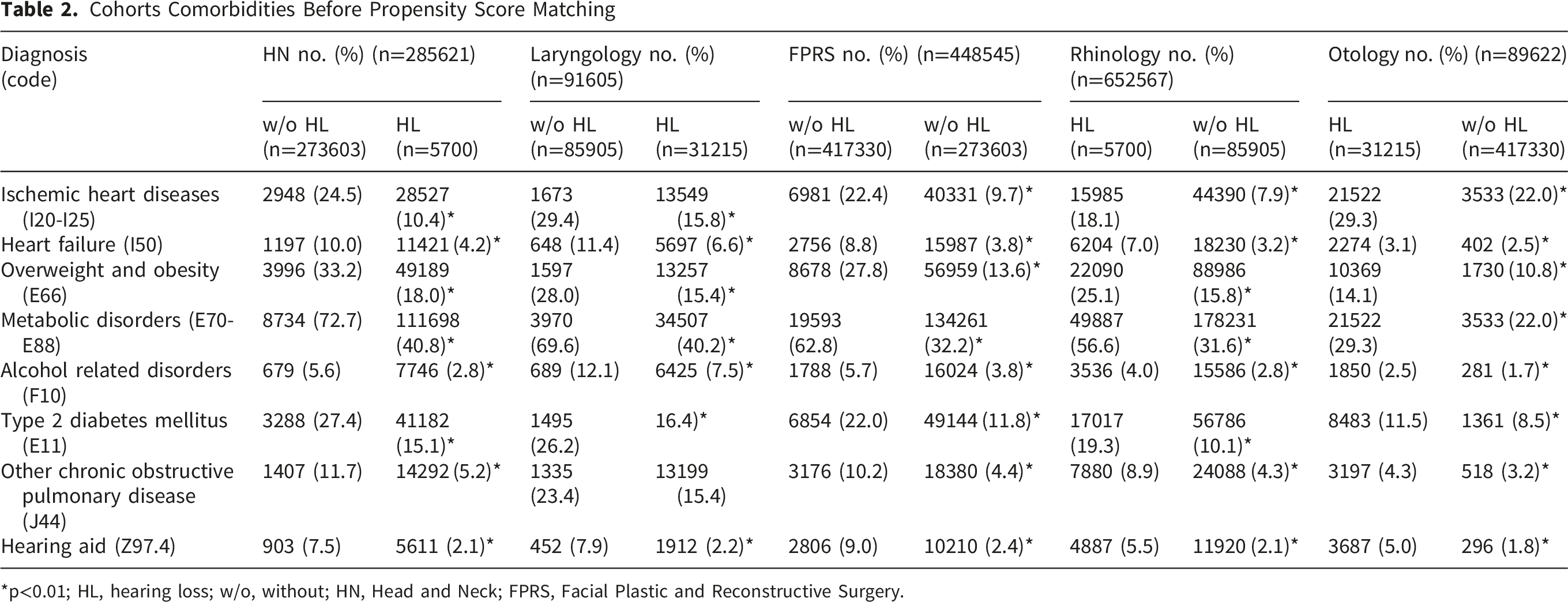
*p<0.01; HL, hearing loss; w/o, without; HN, Head and Neck; FPRS, Facial Plastic and Reconstructive Surgery.
Cohorts Demographics After Propensity Score Matching
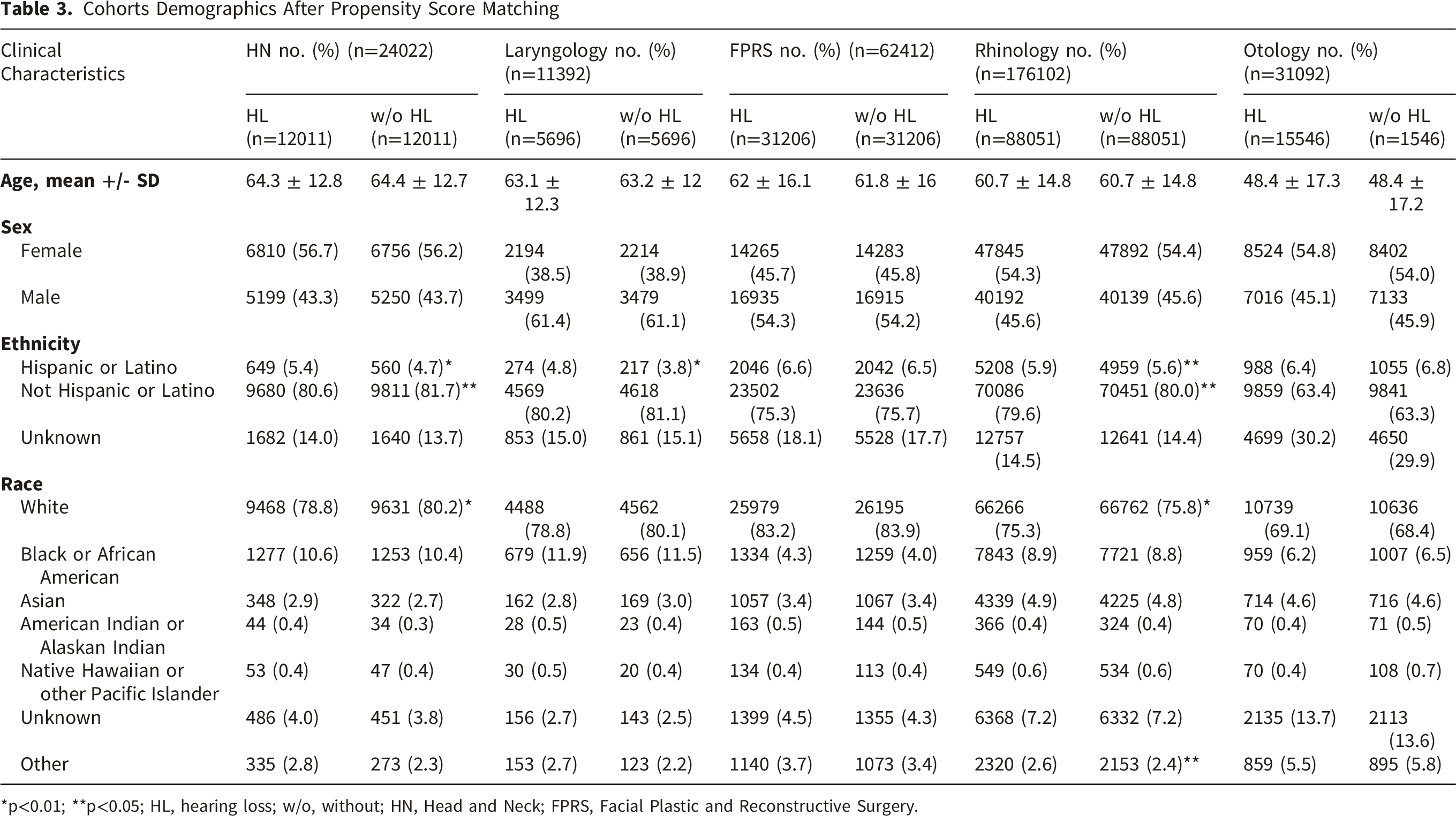
*p<0.01; **p<0.05; HL, hearing loss; w/o, without; HN, Head and Neck; FPRS, Facial Plastic and Reconstructive Surgery.
Cohorts Comorbidities After Propensity Score Matching
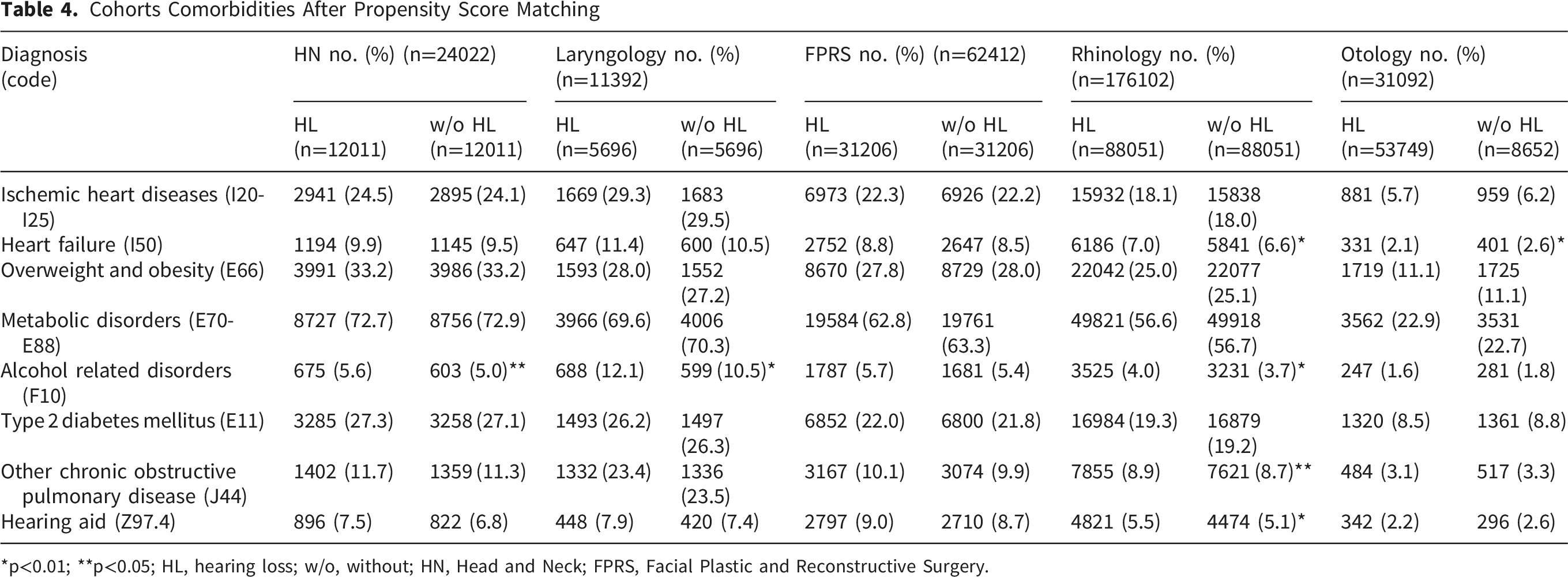
*p<0.01; **p<0.05; HL, hearing loss; w/o, without; HN, Head and Neck; FPRS, Facial Plastic and Reconstructive Surgery.
Outcome Analysis
After HN procedures, rates of SSI were higher among patients who had comorbid HL compared to those who did not. (AR 2.03%, OR 1.22, [1.01 – 1.48], P < 0.01). Emergency department visits were also higher after HN procedures (AR 8.12%, OR 1.31, [1.19 – 1.45], P < 0.01). After HN procedures, rates of wound disruption was higher in patients who had comorbid HL compared to those who did not (AR 1.34%, OR 1.27, [1.01 – 1.61], P < 0.05). Rates of hospital readmission were also higher in patients with HL (AR 19.58%, OR 1.11, [1.04 – 1.18], P < 0.01). There was also significantly lower mortality in patients with comorbid HL after HN procedures (AR 0.36%, OR 0.63, [0.43 – 0.92], P < 0.05). There was no significant difference in cellulitis and abscess formation in patients with HN procedures (Figure 1). Forest plot of head and neck odds ratios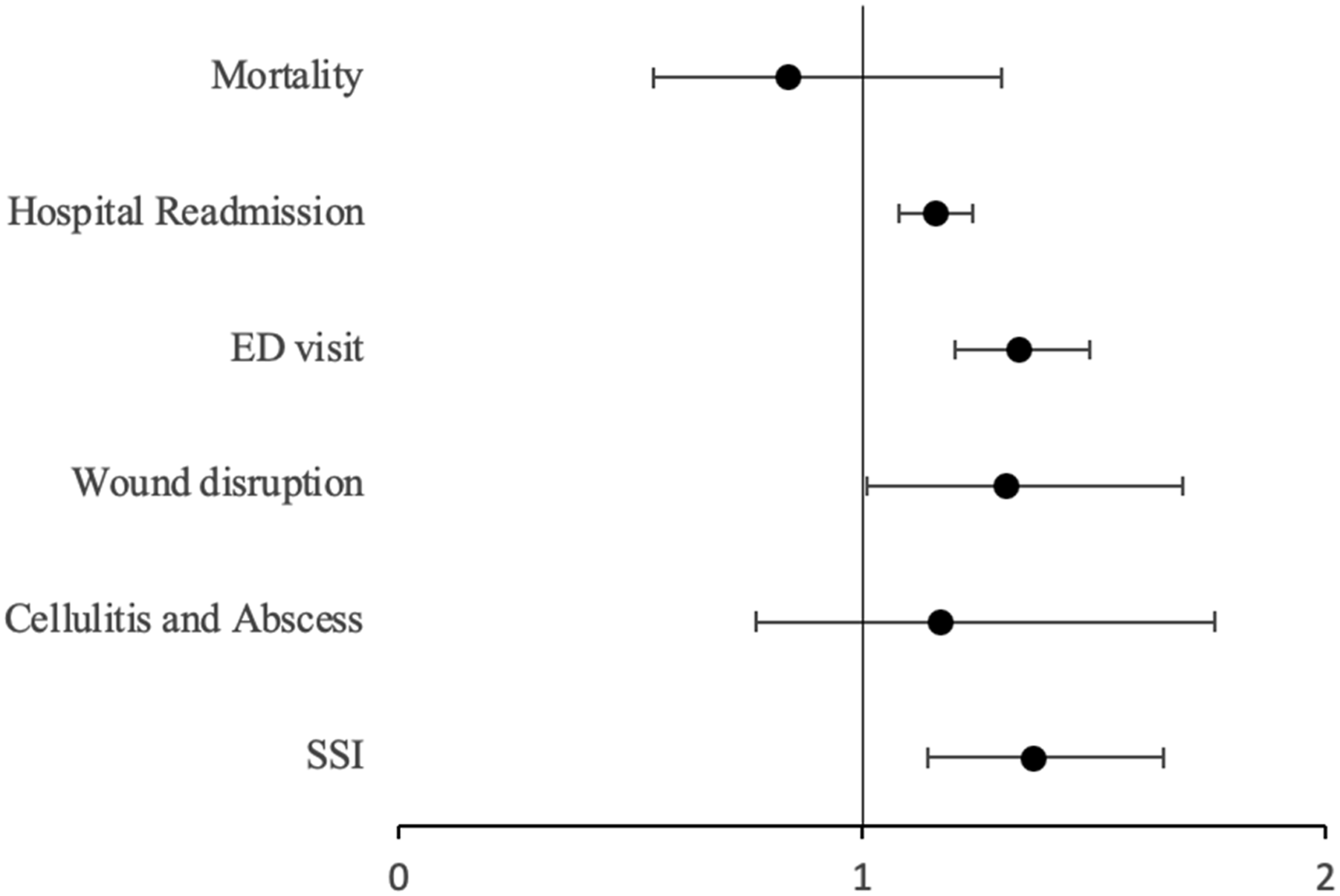
After laryngological procedures, rates of hospital readmission were lower in patients with comorbid HL (AR 20.42%, OR 0.68, [0.62 – 0.74], P < 0.01). There was also significantly lower mortality in patients with comorbid HL after laryngological procedures (AR 1.0%, OR 0.53, [0.39 – 0.74], P < 0.01). There were no significant differences in post-surgical infection, ED visits, or wound disruption (Figure 2). Forest plot of laryngology odds ratios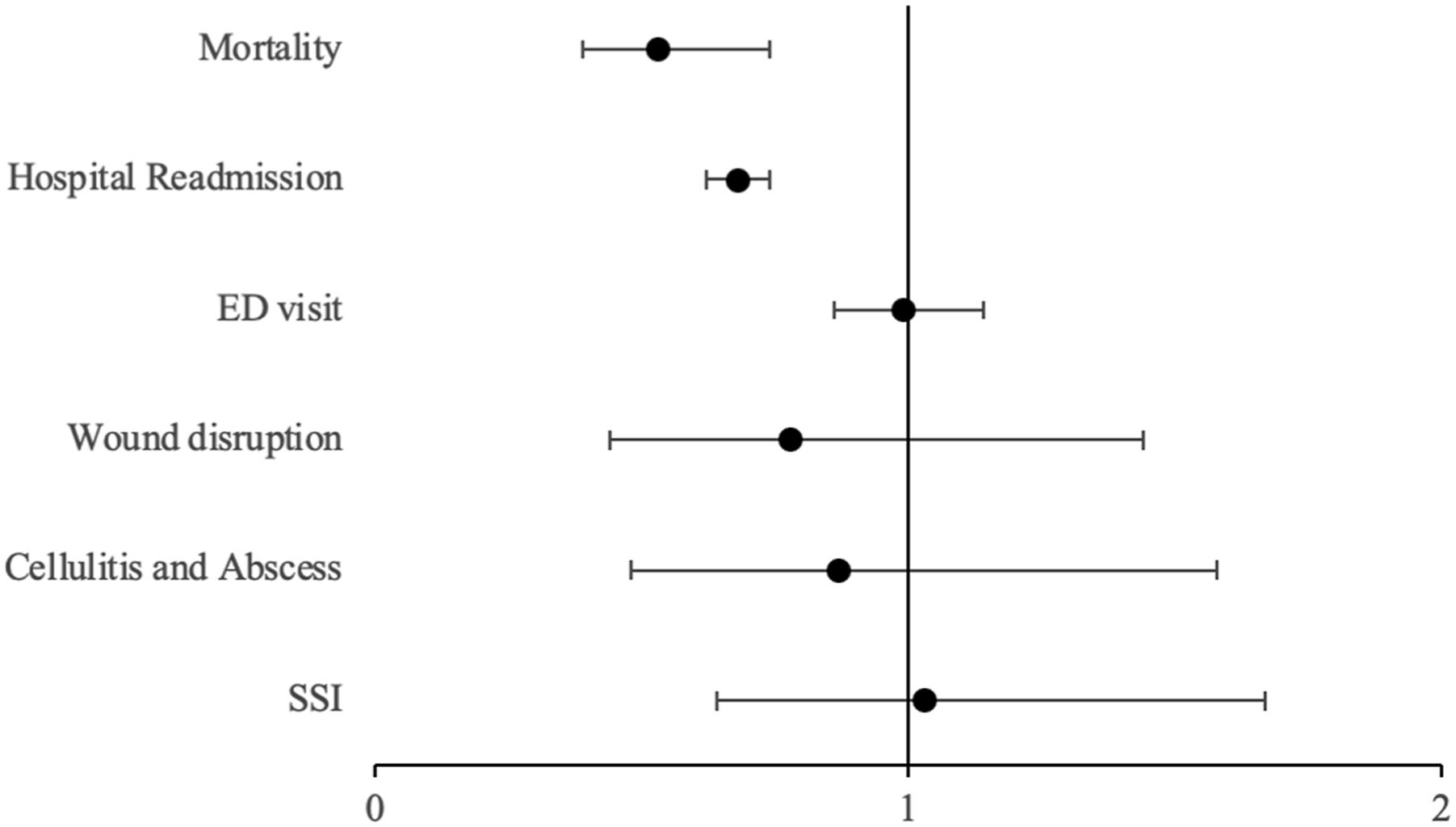
After FPRS procedures, rates of hospital readmission (AR 7.17%, OR 0.73, [0.69 – 0.77], P < 0.01), and mortality (AR 0.10%, OR 0.42, [0.27 – 0.65], P < 0.01) were lower in patients with comorbid HL. However, there were higher rates of ED visits in patients with comorbid HL (AR 4.58% OR 1.13, [1.05 – 1.22], P < 0.01). There was no significant difference in SSI, cellulitis and abscess, or wound disruption with FPRS procedures (Figure 3). Forest plot of facial plastic and reconstructive surgery odds ratios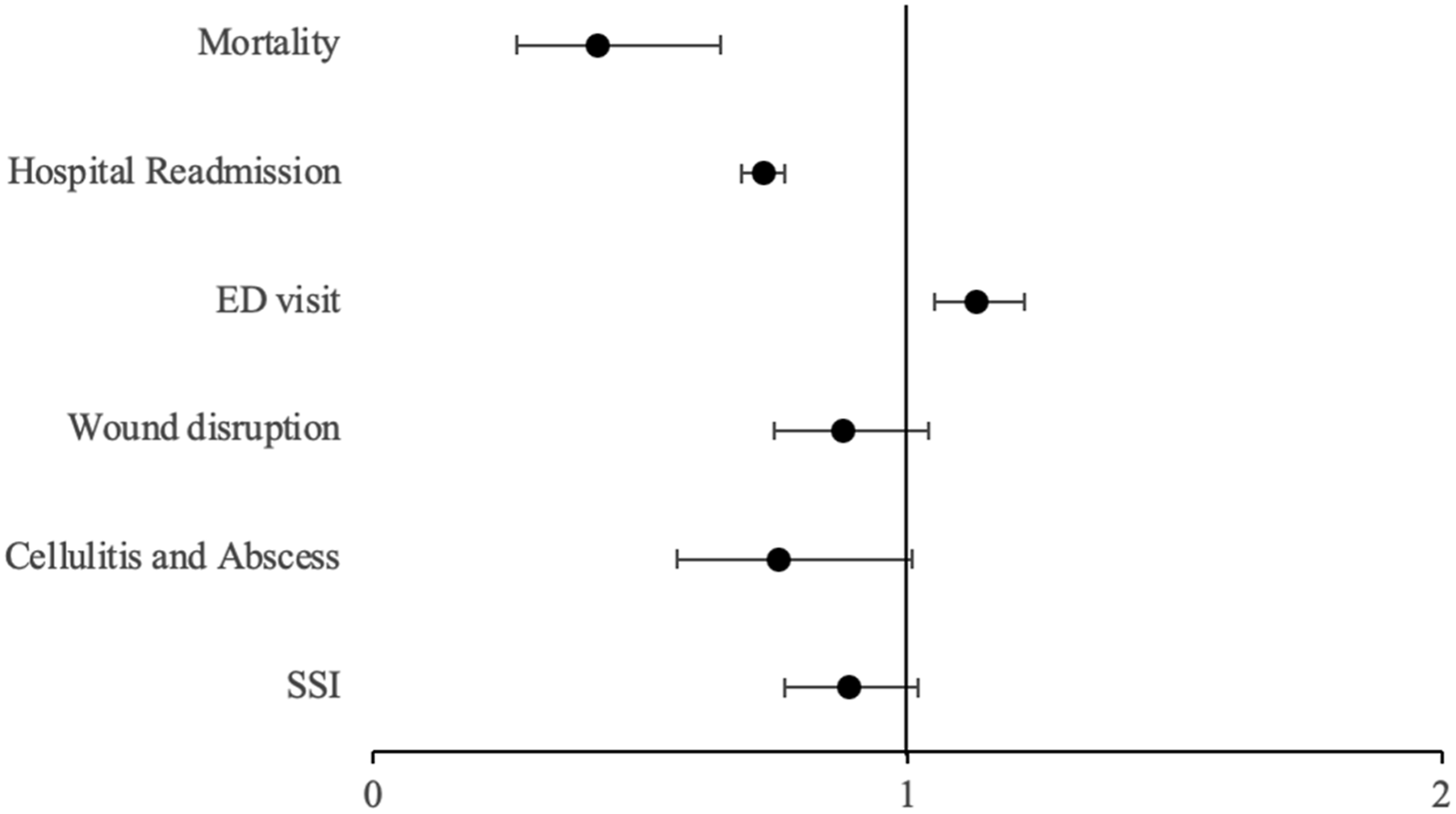
After rhinology surgical procedures, there were lower rates of SSI (AR 0.16%, OR 0.74, [0.59 – 0.92], P < 0.01), cellulitis and abscess (AR 0.13%, OR 0.52, [0.41 – 0.64], P < 0.01), wound disruption (AR 0.06%, OR 0.67, [0.47 – 0.96], P < 0.05), ED visits (AR 3.1%, OR 0.68, [0.66 – 0.71], P < 0.01), readmission (AR 6.15%, OR 0.88, [0.84 – 0.93], P < 0.01), and mortality (AR 0.11%, OR 0.30, [0.24 – 0.37], P < 0.01) in patients with comorbid HL (Figure 4). Forest plot of rhinology odds ratios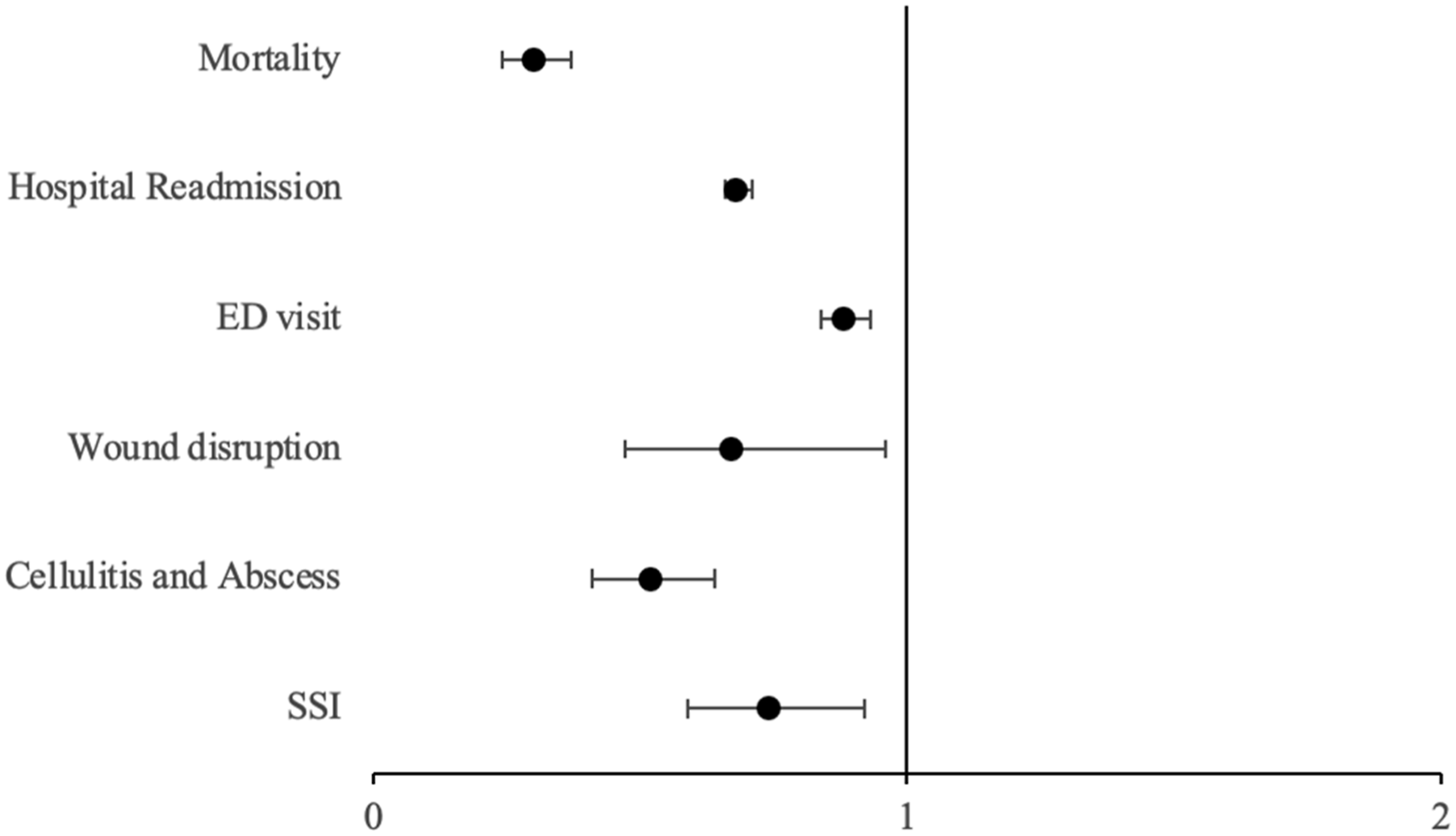
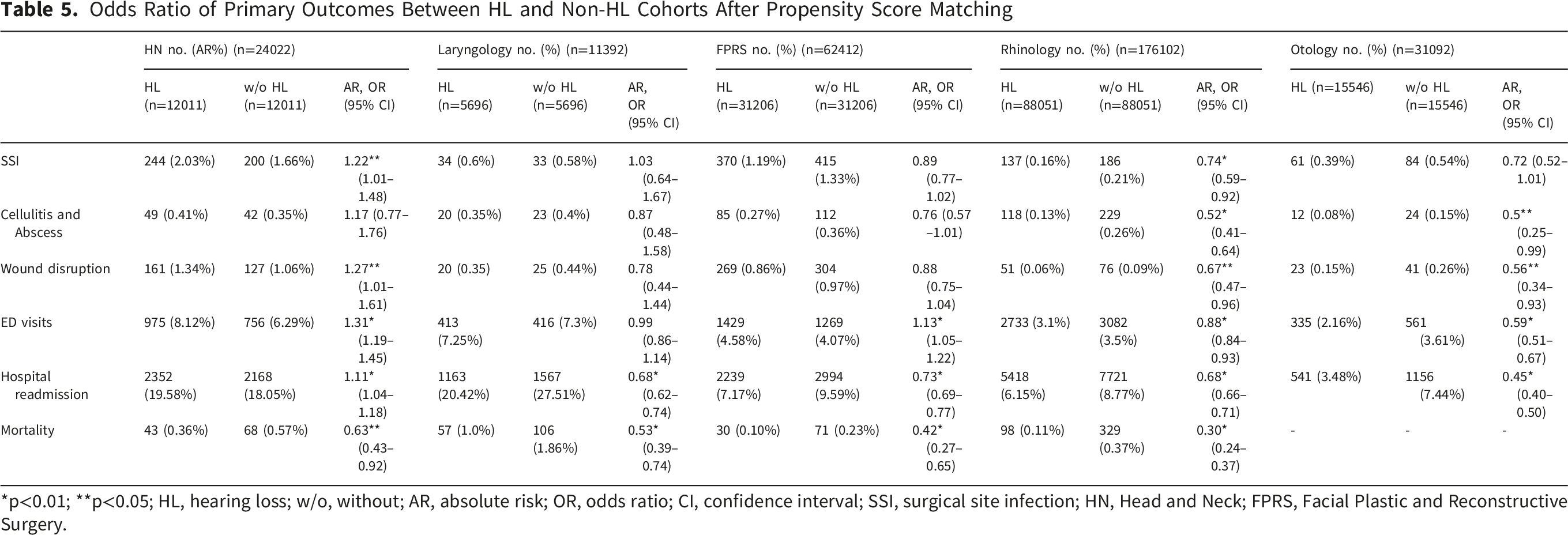
After otology procedures, there were lower rates of cellulitis and abscesses (AR 0.08%,OR 0.5, [0.25 – 0.99], P < 0.05), wound disruption (AR 0.15%, OR 0.56, [0.34 – 0.93], P < 0.05), hospital readmission (AR 3.48%, OR 0.45, [0.40 – 0.50], P < 0.01), and ED visits (AR 2.16%, OR 0.59, [0.51 – 0.67], p < 0.01) in patients with comorbid HL(Figure 5). Mortality rates were too low to calculate OR with TriNetX software (Table 5). Forest plot of otology odds ratios Odds Ratio of Primary Outcomes Between HL and Non-HL Cohorts After Propensity Score Matching *p<0.01; **p<0.05; HL, hearing loss; w/o, without; AR, absolute risk; OR, odds ratio; CI, confidence interval; SSI, surgical site infection; HN, Head and Neck; FPRS, Facial Plastic and Reconstructive Surgery.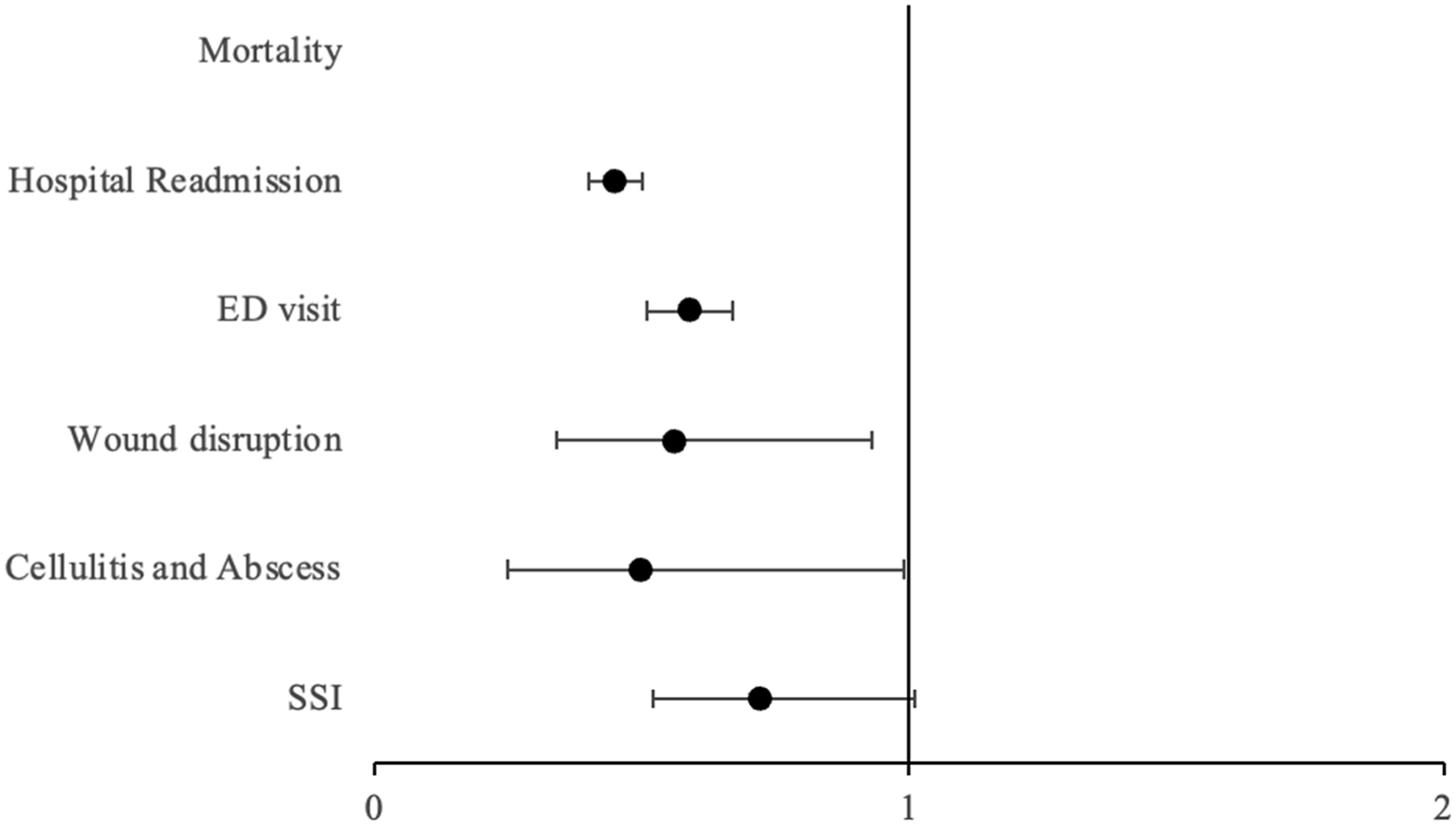
Discussion
Our study showed that patients with HL were, on average, more likely to experience post-operative SSI, wound disruption, hospital readmission, and subsequent emergency department encounters within 30 days following HN procedures. Patients with HL were more likely to have emergency department visits after FPRS procedures. In contrast, patients who have comorbid HL and underwent otology and rhinology surgical procedures had better outcomes compared to patients who do not have HL. Patients with HL undergoing laryngological procedures also had a decreased rate of hospital admission and mortality in the 30-day post-operative period.
What may contribute to higher rates of post-surgical complications is that HL may not always be accounted for in patient-provider communication, which could contribute to miscommunication and affect postoperative care. 9 One solution could be to include postoperative instructions with subtitles, which has been shown to improve patient-provider communication in a previous study. 10 Previous studies have also shown that patients with hearing loss may experience difficulty in patient-provider communication as well as lower health literacy, which could hinder provider and healthcare staff verbal instruction in the post-operative setting.8,11,12 This emphasizes the crucial importance of assessing patient understanding of postoperative care instructions to minimize complication rate and improve healthcare understanding. 13 While elderly patients have an increased risk of experiencing delirium post-operatively, this is further compounded in patients with co-morbid hearing loss.
HN procedures also carry a significant postoperative care burden with many open and extensive procedures, which may contribute to patients being unable to wear hearing aids in the postoperative period. 14 This could further worsen patient hearing deficits and lead to poorer outcomes in the post-operative recovery period. However, 30-day post-operative outcomes remained high in this cohort despite controlling for hearing aid use with propensity score matching. With all these factors, it becomes imperative to educate patients properly on their care and verify their understanding before undergoing extensive surgery such as HN resections.
While HN surgeries are inherently more morbid compared to minor outpatient surgical procedures that are included in our study, we do believe that these complications are multifactorial. Given the pervasive nature of how HL affects everyday life, we also suspected that HL may have affected other minor procedures, including myringotomy, tympanoplasty, and vocal cord medialization to name a few. We aimed to control for these variables through our propensity matching to reduce confounders and compare these patients. However, no significant associations were found. To further characterize the relationship of hearing loss and post-surgical outcomes, future studies could look at the association between out-patient follow up and qualitative scoring metrics. This would be better suited for single institutional reviews to allow for granular details since the TriNetX database does not store for this detailed information.
Concerning increased ED visitation, this could be due to the comorbidity of HL and overall communication barriers that are further complicated after receiving surgical care. A recent study by Wallace et al. showed that patients with hearing loss were 22% more likely to have an ED visit and were 27% more likely to need home health services. 14 Previous literature has shown that hearing loss is associated with greater morbidity, falls, and mobility deficits that could further require the need for emergency services.3-5,15 Two specialty subgroups also consisted of multiple nasal procedures such as septoplasty and endoscopic sinus surgery which are associated with increased risk of epistaxis. 16 This could have contributed to ED visitation rates for the FPRS cohort given the risk for immediate and delayed bleeding for these procedures.16-19
While our study shows significant findings in a few of our cohorts regarding increased risk of post-operative complications in patients with HL, it also demonstrated a decreased risk in other subspecialty procedures. Due to this being a large database study with large power, we recommend reviewing these results cautiously. These findings may reflect residual confounding or procedural heterogeneity that is not fully captured despite our propensity score matching and inclusion of a large array of procedures. To further characterize this relationship, institutional retrospective studies could be performed to allow for more granular details to be collected and statistically analyze these relationships more fully. An example of this is a previous study that showed an increased OR of 1.14 with every 10 dB of increased HL. 6 While this study showed this correlation, it was not specific to otolaryngology procedures.
As surgeons who also primarily treat hearing loss, otolaryngologists should be sensitive to the perioperative and postoperative needs of their patients with HL. They may also be the most equipped surgeons to address this disparity in perioperative and postoperative outcomes among their patients. Therefore, measures such as scheduling more time to counsel HL patients, having a third-party present during patient education, or providing written educational resources to patients with hearing loss may be of benefit. Perioperatively, it may also be of benefit to screen patients based on factors regarding increased noise exposure and take these factors into consideration for future risk models. Subpopulations at risk from chronic noise exposure at work come from a wide variety of vocations including construction, farmers, military personnel, and even musicians.20-23
Regarding caring for these at risk populations, the American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline on Age-Related Hearing Loss recommends techniques such as environmental manipulations, with examples of facing a person when speaking, rephrasing when the message is not understood, or moving away from noise. 24 It is also recommended to screen patients aged 50 years and older which may further aid with future pre-operative work-up, and to continue to re-evaluate patients who have HL every three years.
To our knowledge, our study is the first to show the post-surgical outcomes in patients with HL that are specific to subspecialty otolaryngologic procedures. This study is one of the largest retrospective studies utilizing a national database, which increases the generalizability of these results. However, it is not without limitations. TriNetX is a retrospective administrative database with inherent limitations to this type of data. The analysis is limited by the accuracy of data entry into the database. We minimized the risk of confounding variables by matching for multiple comorbidities that could impact surgical outcomes, along with propensity score matching. Even though we categorized these procedures under varying subspecialties of otolaryngology, TriNetX does not account for specialties that perform these procedures, so many of these surgeries could have been performed by other surgeons such as plastic surgeons, surgical oncologist, along with endocrine surgeons. While we attempted to include most procedures that are relevant to the subspecialties of otolaryngology, there is some crossover between subspecialties. We aimed to reduce this by not including procedures used for other cohorts, however, this is not truly representative of subspecialty practice. There is also no sensitivity testing in TriNetX to include procedures across multiple cohorts which further limits the generalizability to individual practice. Furthermore, some surgeries carry lower complication risks than others, such as reconstructive cases, compared to minor outpatient ear surgeries. However, we mitigated much of this through propensity matching, including hearing aid use, and suspected that hearing loss would increase post-operative risk in any procedure whether it is minor or major in nature.
Another limitation is that the communication of instruction of postoperative care also differs drastically from institution to institution, and this was not standardized and accounted for in this study, which included 58 healthcare networks in TriNetX. Our procedures that were compiled were also not exhaustive of the breadth and depth of each subspecialty of otolaryngology, which limits how large some of our cohorts were in this study. TriNetX also does not allow for statistical analysis for n < 10 to protect patient privacy, which resulted in no statistical correlations being made in one of our post-operative outcomes. TriNetX does not include grading of severity of hearing loss which is a known risk factor for increased postoperative risk in older adults. 9 Future studies could look at the role of HL in single institutions to account for specialty care and granular details through retrospective review. Prospective studies could also be conducted to target education for populations who have HL.
Conclusion
Based on our findings, patients with hearing loss undergoing HN surgical procedures have a higher rate of post-operative SSI, wound disruption, ED visits, and readmittance than those without HL. Patients with HL undergoing FPRS procedures also had a higher ED visitation rate. Future studies should aim to prospectively examine HN surgery outcomes in the HL population and implement changes in perioperative care to address the needs of the HL patient. Future studies could also determine how best to address this healthcare disparity and should include if the degree or severity of hearing loss correlates with increased morbidity.
Supplemental Material
Supplemental Material - Role of Hearing Loss in Otolaryngology Surgical Outcomes
Supplemental Material for Role of Hearing Loss in Otolaryngology Surgical Outcomes by Quentin C. Durfee, Hänel W. Eberly, David Goldrich, Mark Whitaker, Varun S. Patel in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material - Role of Hearing Loss in Otolaryngology Surgical Outcomes
Supplemental Material for Role of Hearing Loss in Otolaryngology Surgical Outcomes by Quentin C. Durfee, Hänel W. Eberly, David Goldrich, Mark Whitaker, Varun S. Patel in Ear, Nose & Throat Journal
Footnotes
Author Note
This article was presented at the AAO-HNSF 2024 Annual Meeting & OTO Experience, Miami, FL, September 28 – October 1, 2024.
Acknowledgements
We would like to acknowledge Caia Hypatia for their contributions to this study regarding project management.
Ethical Considerations
This study was conducted at The Pennsylvania State University College of Medicine and was deemed exempt by The Pennsylvania State University Institutional Review Board (IRB STUDY00018629).
Consent to Participate
There are no human participants in this article and informed consent is not required.
Author Contributions
Quentin C. Durfee, concept and design, acquisition, analysis, interpretation of data, and drafting of the manuscript; Hänel W. Eberly, concept and design, acquisition, analysis, interpretation of data, drafting of the manuscript, critical review of the manuscript for important intellectual content; David Goldrich, concept and design, acquisition, analysis, interpretation of data, drafting of the manuscript; critical review of the manuscript for important intellectual content, administrative, technical, or material support, supervision; Varun S. Patel, critical review of the manuscript for important intellectual content, obtained funding, administrative, technical, or material support, supervision, other – primary mentor and quality control.
Funding
The project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through Grant UL1 TR002014.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.