
Abstract
Teratomas are germ cell tumors typically originating in the gonads. Extragonadal occurrences, particularly in the parotid gland, are exceedingly rare. Due to their nonspecific clinical presentation, these tumors often pose a diagnostic challenge. We report a rare case of a mature cystic teratoma of the parotid gland in an 18-year-old female, who presented with a painless, slow-growing mass in the right postauricular region persisting for over a decade. Magnetic resonance imaging (MRI) demonstrated a lobulated mass with high signal intensity on T1- and T2-weighted sequences. The patient underwent a successful right superficial parotidectomy without postoperative complications. Histopathological analysis confirmed the diagnosis of mature cystic teratoma. This case underscores the necessity of including teratoma in the differential diagnosis of parotid gland neoplasms, especially when presenting as a long-standing, asymptomatic mass.
Introduction
Teratomas are germ cell tumors composed of tissues derived from one or more of the three germ layers, including epithelium, cartilage, neural tissue, fat, bone, and muscle. While they are typically found in the ovaries or testes, extragonadal teratomas account for approximately 15% of all cases, with only 3% to 5% occurring in the head and neck region.1-3 Parotid gland involvement is particularly uncommon. The first documented case of a parotid teratoma was reported by Shadid et al in 1975. 4 To date, only a few cases have been published. We present a case of a mature cystic teratoma of the parotid gland and provide a comprehensive review of the existing literature.
Case Report
An 18-year-old female with an unremarkable medical history presented with a right postauricular mass of over ten years’ duration. The mass had gradually increased in size but remained asymptomatic, with no associated pain, swelling, erythema, or discharge. Given the indolent and painless nature of the mass, the patient had not sought medical intervention, and no prior advanced imaging had been performed during the ten-year period.
Initially evaluated in the pediatric neurosurgery outpatient clinic, physical examination revealed a palpable mass measuring approximately 2.5 x 2.0 cm. Preoperative facial nerve function was normal, corresponding to a House-Brackmann Grade I. Magnetic resonance imaging (MRI) showed a lobulated mass in the posterior aspect of the right parotid gland, demonstrating high signal intensity on T1-weighted (T1WI), T2-weighted (T2WI), and T2FLAIR sequences with fat suppression signal. (Figure 1A and B) The mass measured approximately 2.8 x 2.2 x 3.0 cm. Preoperative magnetic resonance image of the patient (A) The coronal view shows a lobulated cystic mass (white arrow) in right parotid gland. (B) The tumor shows a significant signal dropout on fat-suppressed sequences (white arrow)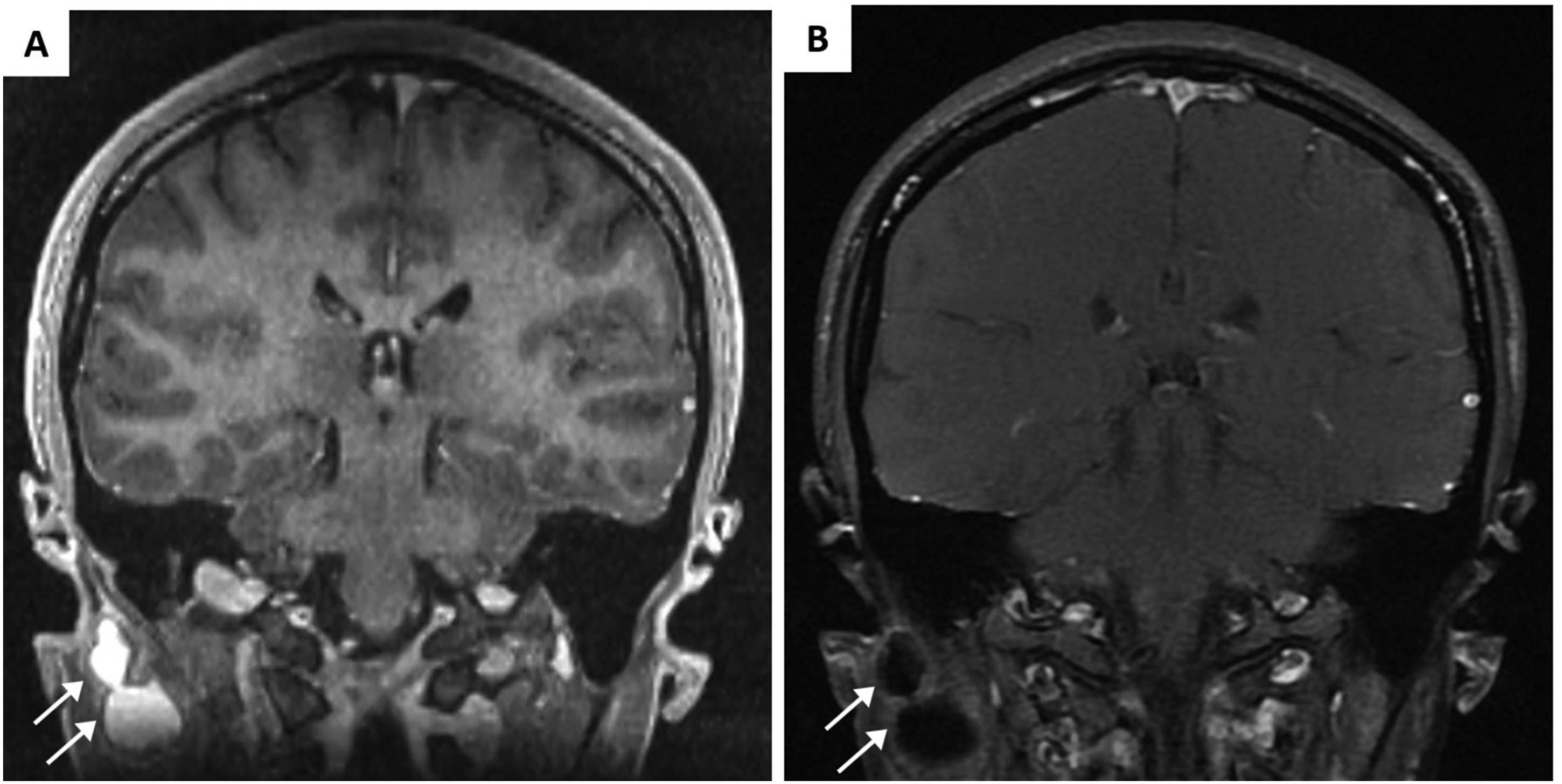
The patient was referred to our otolaryngology department and underwent a right superficial parotidectomy. Intraoperatively, the tumor presented as a well-encapsulated, whitish, cystic mass. It demonstrated no signs of local tissue invasion, encasement, or compression of the facial nerve. To ensure optimal safety, a continuous intraoperative nerve monitoring system was utilized. Due to the intact capsule and the lack of adherence to surrounding structures, the surgical dissection proceeded smoothly. The procedure was uneventful, with no postoperative complications. Postoperative facial nerve evaluation remained normal without any weakness. Pathological examination of the excised tumor revealed a cyst lined with squamous epithelium, containing epidermal tissue, skin adnexa, and cartilage nodules. (Figure 2A–C) The final diagnosis was confirmed as a mature cystic teratoma of the parotid gland. Histopathological findings of the tumor. (A) 10X) Low power field shows a cystic lesion in parotid gland with focal rupture and foreign body reaction. Keratinous material is seen in the cystic space. (B) 40X) The cystic lesion is composed of epidermis, skin adnexa and cartilage nodules. No immature component is observed. (C) 100X) Ruptured cyst with adjacent foreign body reaction to cystic content and hair shaft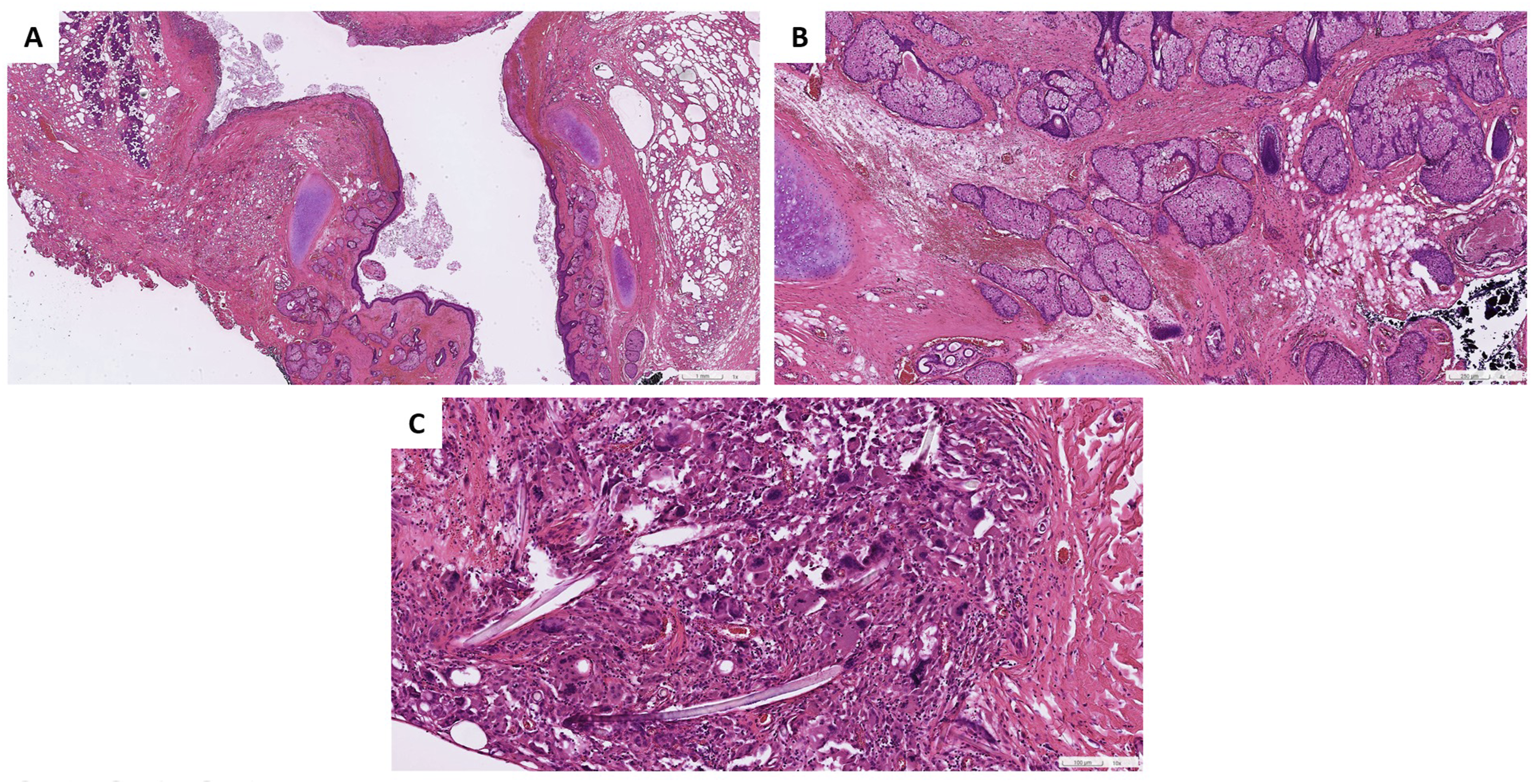
The patient was evaluated in our clinic at 1 week and 1 month postoperatively, during which no clinical evidence of tumor recurrence or complication was noted. However, the patient was subsequently lost to follow-up due to personal reasons. A detailed chronological timeline of the patient’s clinical course is summarized in Figure 3. Timeline of clinical course and interventions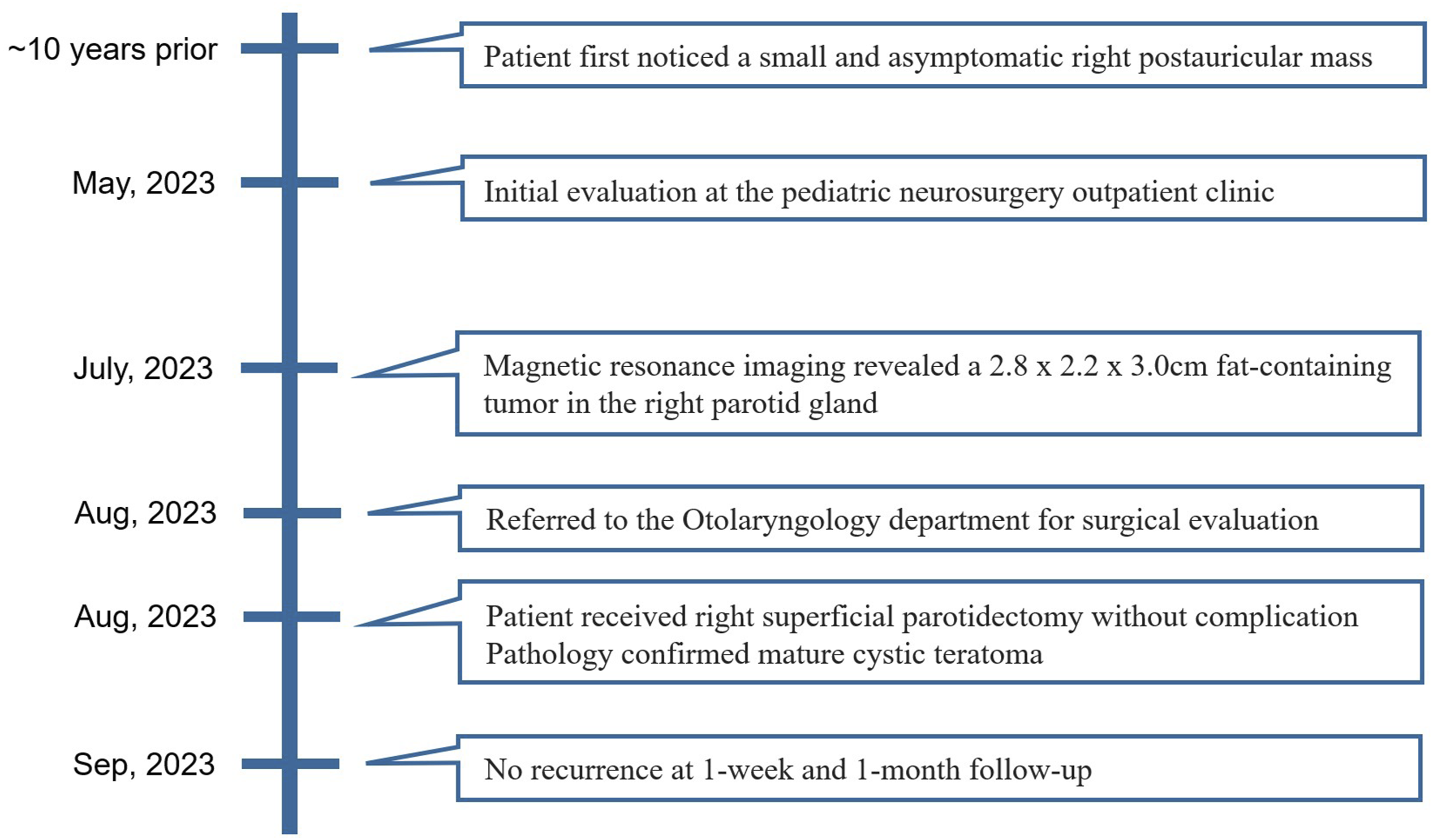
Discussion
Epidemiologically, although teratomas typically arise in the gonadal region, approximately 15% of these tumors occur in extragonadal area, with only 3% to 5% located in the head and neck. While nearly 90% of head and neck teratomas develop during infancy or childhood, comprising 0.47% to 6% of all pediatric teratomas, parotid gland involvement remains exceptionally uncommon, with only a limited number of cases reported.1-3 We reviewed the literature to provide a detailed analysis of the previously documented cases.1-16 These reports indicate a female predominance, with a female-to-male ratio of 3:1. Patient ages ranged from 3 months to 36 years. The tumor occurred more frequently on the left side. Most tumors were located in the superficial lobe, although one case extended into the deep lobe and the parapharyngeal space. 1 Tumor sizes ranged from 1 cm to 6 cm on imaging studies.
The clinical presentation of parotid teratomas is typically nonspecific, which require advanced radiological imaging in differential diagnosis. The tumor often present as painless masses without specific symptoms, making diagnosis challenging through physical examination alone. Therefore, preoperative radiological investigations, such as ultrasound, computed tomography (CT), and MRI are essential. Ultrasonography aids in assessing tumor size and composition, often revealing heterogeneous hyperechoic signals. CT and MRI provide detailed preoperative evaluations, outlining tumor dimensions, cystic walls, adjacent structures, as well as identifying specific components like fat, calcifications, teeth, or hair follicles. MRI is particularly sensitive to fat components, showing high signal intensities on T1WI and T2WI and hypointense signals on fat-suppressed sequences, which confirms the presence of lipid-rich components. 9 The differential diagnosis of a fat-containing lesion in parotid gland should encompass lipoma, angiolipoma, and dermoid cysts. Unlike other uniform fat-containing lesions, the mature teratomas often display heterogeneous characteristics, including well-defined cystic components, calcifications, and specific fat-fluid levels, which are distinctive from other possible lesions.1,16 In our case, despite ten years of asymptomatic growth, the MRI findings suggested a fat-containing lesion, which raised the suspicion of a teratoma.
Fine-needle aspiration (FNA) can also assist in the differential diagnosis.3,6,8,9,11-13,16 Ohta et al described the details of cytologic findings including squamous cells, sebaceous gland-like cells and some hair shafts. 8 Although FNA is a valuable tool commonly used for initial evaluation, it is frequently inconclusive or non-diagnostic for parotid teratomas. Due to the tumor’s rarity and heterogeneous tissue composition, FNA carries a risk of sampling error and misdiagnosis. 9 Therefore, definitive diagnosis relies on complete surgical excision and subsequent histopathological examination.
Complete surgical excision, either partial or total parotidectomy with facial nerve preservation, remains the treatment of choice for parotid teratomas. Most tumors are encapsulated and non-invasive, facilitating surgical dissection and separation from surrounding tissues. The choice between partial and total parotidectomy depends on tumor’s size and location. Postoperative complications are rare; one case reported temporary facial paralysis and incomplete eyelid closure that resolved spontaneously within four months. 1 Another case reported transient facial lower trunk paresis that recovered within a few days. 16 In the present case, a superficial parotidectomy was performed without complications, such as facial nerve palsy or tumor recurrence.
A definitive diagnosis relies on histopathological examination, which demonstrates mature tissue derivatives from multiple germ layers. Most cases exhibit cystic structures containing sebaceous glands and hair follicles. Cartilage was identified microscopically in eight cases. One case featured a tooth, and two cases demonstrated thyroid tissue.3,11,16 Three cases reported tissues from all three germ cell layers, including brain tissue or neural tissue, cartilage, and mucinous epithelium.2,3,16 All reviewed cases demonstrated mature tissue components without malignant transformation. Our case displayed a cystic lesion lined with epidermis, skin adnexa, and cartilage nodules.
Regular follow-up is essential due to the potential risk of malignancy and recurrence. Although most teratomas are benign mature cysts, they carry a risk of malignant transformation, which is notably higher in adults compared to children. The incidence of malignant change is 26% and 10%, respectively. 11 Furthermore, in situ recurrence has been reported following incomplete resection. 1 Consequently, clinicians must ensure regular, long-term follow-up to monitor for early recurrence or malignant changes.2,13,16 Our surveillance protocol consisted of scheduled follow-up evaluations at 3 months, 6 months, and annually thereafter. However, the patient was lost to follow-up due to personal reasons.
In conclusion, teratomas of the parotid gland are extremely rare. Preoperative imaging, including ultrasound, CT, and MRI, plays a crucial role in diagnosis and surgical planning. Surgical resection with facial nerve preservation is the treatment of choice, offering a low incidence of postoperative complications and recurrence.
Footnotes
Acknowledgments
We wish to covey special thanks to the colleagues of the Department of Pathology, Mackay Memorial Hospital for providing microscopic pictures and the related information.
Ethical Considerations
The study was approved by the Ethics Committee of Mackay Memorial Hospital, Taipei, Taiwan (24MMHIS076e).
Consent to Participate
Patient consent was waived as the waiver will not adversely affect the rights and welfare of the subjects. A waiver of informed consent from the patient was approved by the Institutional Review Board committee of Mackay Memorial Hospital, Taipei, Taiwan.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Sharing does not apply to this article because no data sets were generated or analyzed during the study.