
Abstract
Acute mastoiditis is a recognized intratemporal complication of acute otitis media in children, but progression to frank temporal bone osteomyelitis with extensive cortical necrosis is exceptionally rare in infancy. This report presents a 1-year-old infant with refractory acute mastoiditis complicated by destructive temporal bone osteomyelitis. High-resolution computed tomography with 3D reconstruction demonstrated extensive cortical loss. Emergency subtotal mastoidectomy and radical debridement were performed. Deep intraoperative culture yielded multidrug-resistant Staphylococcus hominis, and histopathology confirmed osteomyelitis. The child improved rapidly on targeted linezolid therapy and completed a 4-week course with complete clinical and laboratory resolution. This case highlights the importance of early imaging, deep tissue sampling, and targeted therapy in rare infant temporal bone osteomyelitis.
Significance Statement
High-resolution CT and 3-dimensional reconstruction were decisive in distinguishing destructive temporal bone osteomyelitis from uncomplicated mastoiditis in this infant whose condition worsened despite intravenous antibiotics. The images demonstrated mastoid cortical loss, justified urgent operative intervention, and provide a concise teaching example of when imaging changes management in severe pediatric ear infection.
Introduction
Temporal bone and skull base osteomyelitis are uncommon entities in pediatric practice, and destructive disease in infancy is particularly unusual.1,2 When acute mastoiditis fails to improve on appropriate intravenous antibiotics, imaging becomes critical for determining whether infection has progressed from coalescent mastoiditis to destructive bone involvement. 3 This Imaging Clinic report focuses on the CT findings that prompted urgent intervention in a 1-year-old child.
Case Presentation
A previously healthy 1-year-old girl presented with fever, irritability, purulent otorrhea, and progressive post-auricular swelling despite broad-spectrum intravenous antibiotics. Examination showed erythema, tenderness, fluctuation, and anteroinferior displacement of the pinna. Because there was no clinical improvement after 72 hours of therapy, urgent high-resolution CT of the temporal bone was obtained.
The patient subsequently underwent urgent subtotal mastoidectomy with radical debridement. Intraoperatively, the mastoid cortex was fragmented, devitalized, and frankly necrotic. Deep intraoperative culture yielded multidrug-resistant Staphylococcus hominis susceptible to linezolid, and histopathology confirmed osteomyelitis. After surgery, the patient received linezolid at 10 mg/kg every 8 hours for a total of 4 weeks with weekly hematologic monitoring. 4
Clinical follow-up at 3, 6, and 12 months showed sustained improvement in appetite and activity, complete wound healing, and no recurrent fever, otorrhea, or other new complaints. The parents declined repeat imaging because of concern about additional radiation exposure in infancy, so outcome assessment relied on serial clinical evaluations in accordance with ALARA-focused practice. 5
Imaging Findings
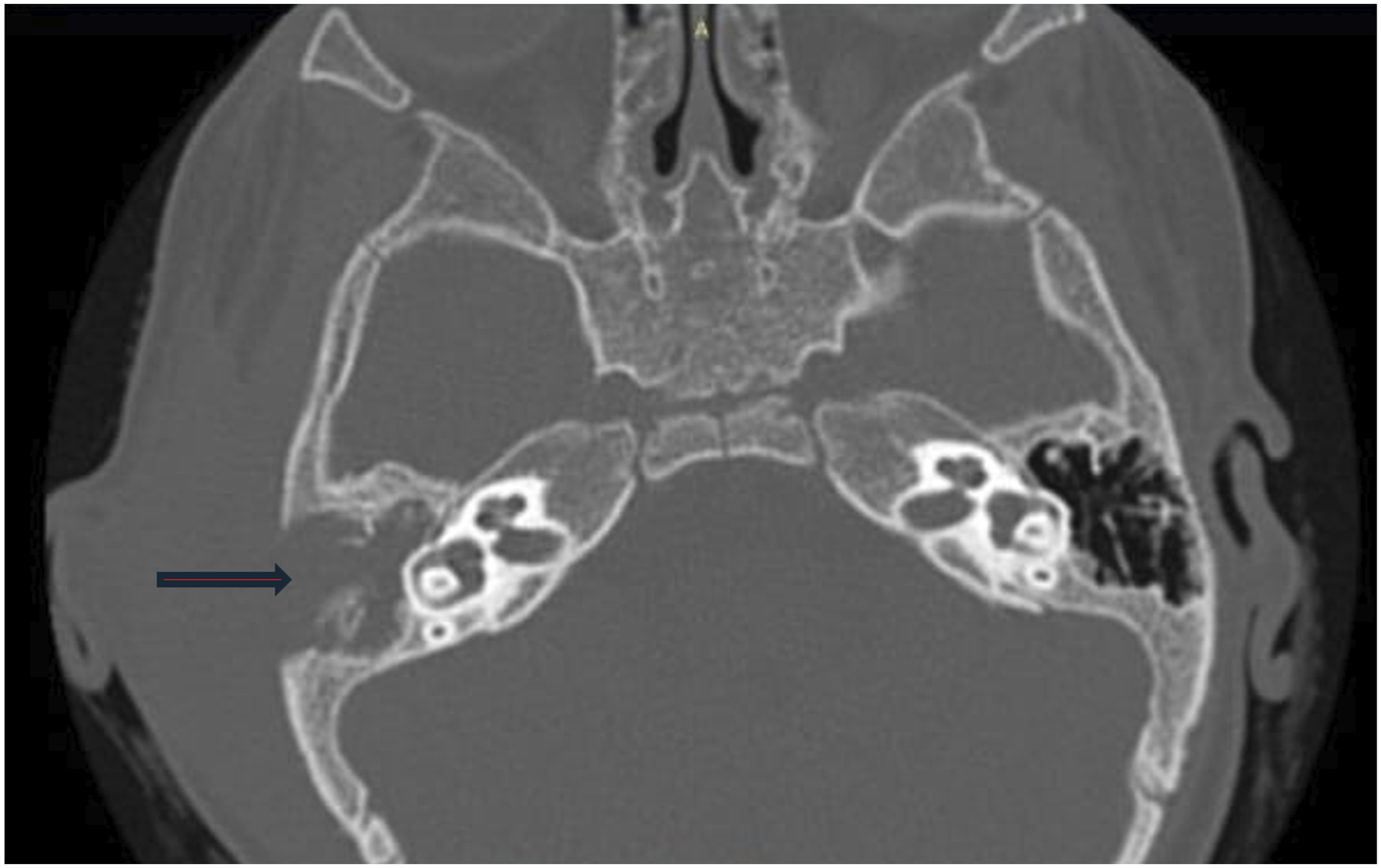
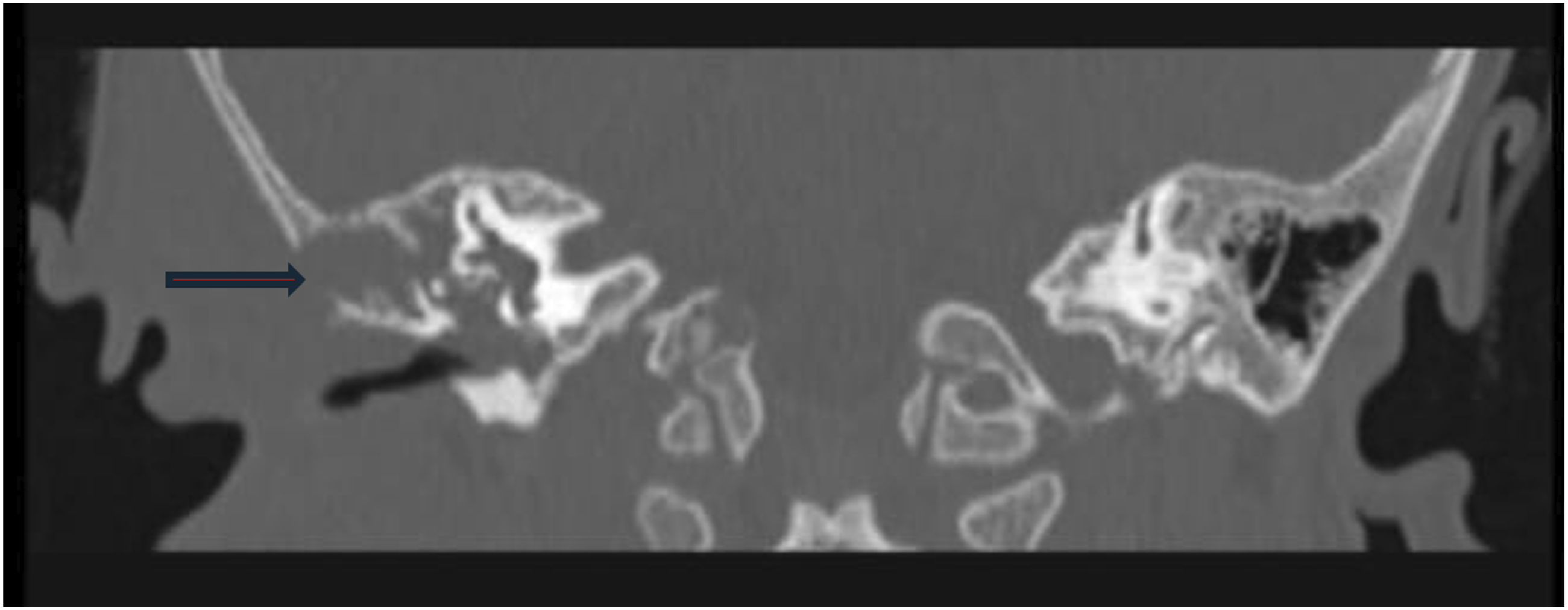
CT demonstrated complete opacification of the mastoid air-cell system with loss of intercellular septations, consistent with coalescent mastoiditis. More importantly, axial and coronal images showed a large destructive cortical defect involving the mastoid process with adjacent soft-tissue abnormality. Three-dimensional volume-rendered reconstruction most clearly depicted the irregular geometry and extent of the cortical breach, helping distinguish aggressive osteomyelitis from uncomplicated mastoid inflammation and supporting immediate operative management (Figures 1-3). Three-dimensional CT reconstruction demonstrating a large irregular destructive cortical defect over the mastoid region, highlighting the extent of temporal bone involvement Axial high-resolution CT image showing mastoid opacification, loss of normal bony septations, and focal cortical destruction with adjacent soft-tissue abnormality Coronal CT image confirming cortical erosion of the mastoid process and associated inflammatory soft-tissue change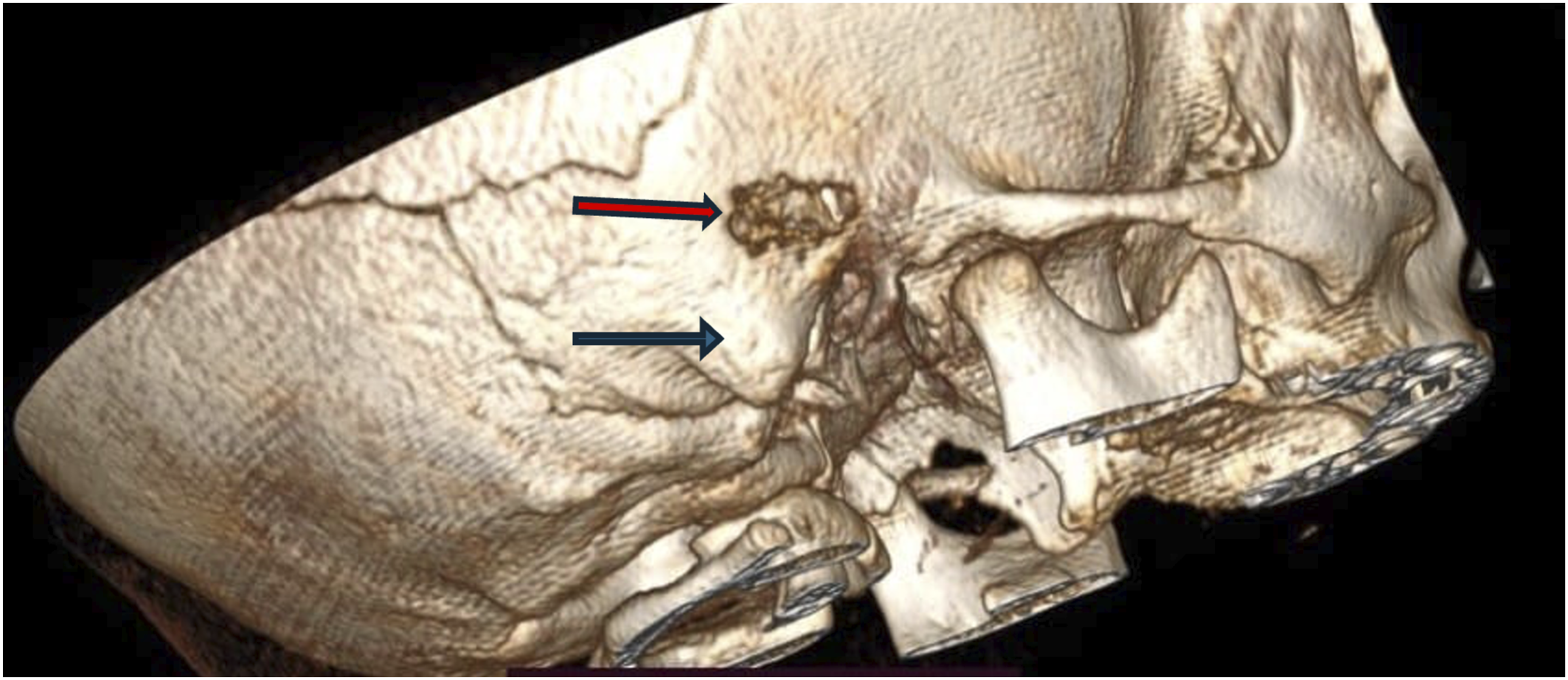
Discussion
The principal educational point in this case is that worsening mastoiditis in an infant should not be interpreted as simple persistent infection when CT demonstrates cortical destruction. The imaging pattern here indicated progression beyond uncomplicated mastoiditis to destructive temporal bone osteomyelitis and materially altered management.1-3
The main differential considerations included refractory acute mastoiditis with subperiosteal abscess, chronic destructive ear disease, and neoplasm. These possibilities became less likely once CT showed frank cortical loss, surgery confirmed necrotic bone, and histopathology demonstrated osteomyelitis. The deep intraoperative recovery of Staphylococcus hominis also correlated with both pathology and clinical response to directed therapy, supporting its role as a true pathogen rather than superficial contamination. 6
Although interval CT might have documented remodeling, serial clinical follow-up at 3, 6, and 12 months showed durable recovery, and the parents reasonably declined additional radiation exposure. This should be acknowledged as a limitation, but it does not negate the strong clinicoradiologic, operative, microbiologic, and histopathologic concordance in the diagnosis. 5
Strengths of the case include the quality of the CT and 3D images, the concordance between imaging and operative findings, and confirmation by both deep culture and pathology. Limitations include the single-case design and the absence of repeat radiologic or formal long-term audiologic follow-up.
Footnotes
Consent for Publication
Informed consent was obtained from the patient’s parents for the publication of this case report and any accompanying clinical images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declare that there are no conflicts of interest regarding the publication of this manuscript.