
Abstract
Middle ear adenomatous neuroendocrine tumors (MEANT) are rare neoplasms frequently misdiagnosed due to their nonspecific clinical presentations. We present the case of a 25-year-old woman who reported a 2-month history of tinnitus, dizziness, and left-sided conductive hearing loss. Otoendoscopy and computed tomography revealed a well-circumscribed, vascular soft-tissue mass in the epitympanum extending to the mastoid antrum, which was subsequently managed with complete transcanal endoscopic excision. Histopathological evaluation confirmed a well-differentiated neuroendocrine tumor. A definitive diagnosis was established through comprehensive immunohistochemical profiling, demonstrating positive staining for INSM-1 and chromogranin-A, alongside a low Ki-67 proliferation index of less than 3%. Following the procedure, the patient exhibited stable hearing and no clinical or radiologic evidence of tumor recurrence over an 8-year follow-up period. Ultimately, this case highlights the critical importance of utilizing the 2022 WHO classification and immunohistochemical markers to accurately diagnose MEANT. Furthermore, it underscores a vital clinical caveat: while complete surgical excision is the definitive treatment, the tumor's established propensity for delayed recurrence mandates indefinite, long-term clinical and radiologic surveillance.
Significance Statement
This report highlights the clinical importance of accurate diagnosis and long-term management of middle ear adenomatous neuroendocrine tumors (MEANT). Because of its nonspecific presentation, MEANT is frequently misdiagnosed. By aligning with the 2022 WHO classification and emphasizing the critical role of immunohistochemical profiling (e.g., INSM-1), this study provides a clear framework for definitive diagnosis. Furthermore, it underscores a vital clinical caveat: while complete surgical excision is the definitive treatment, the tumor's established propensity for delayed recurrence mandates indefinite, long-term clinical and radiologic surveillance.
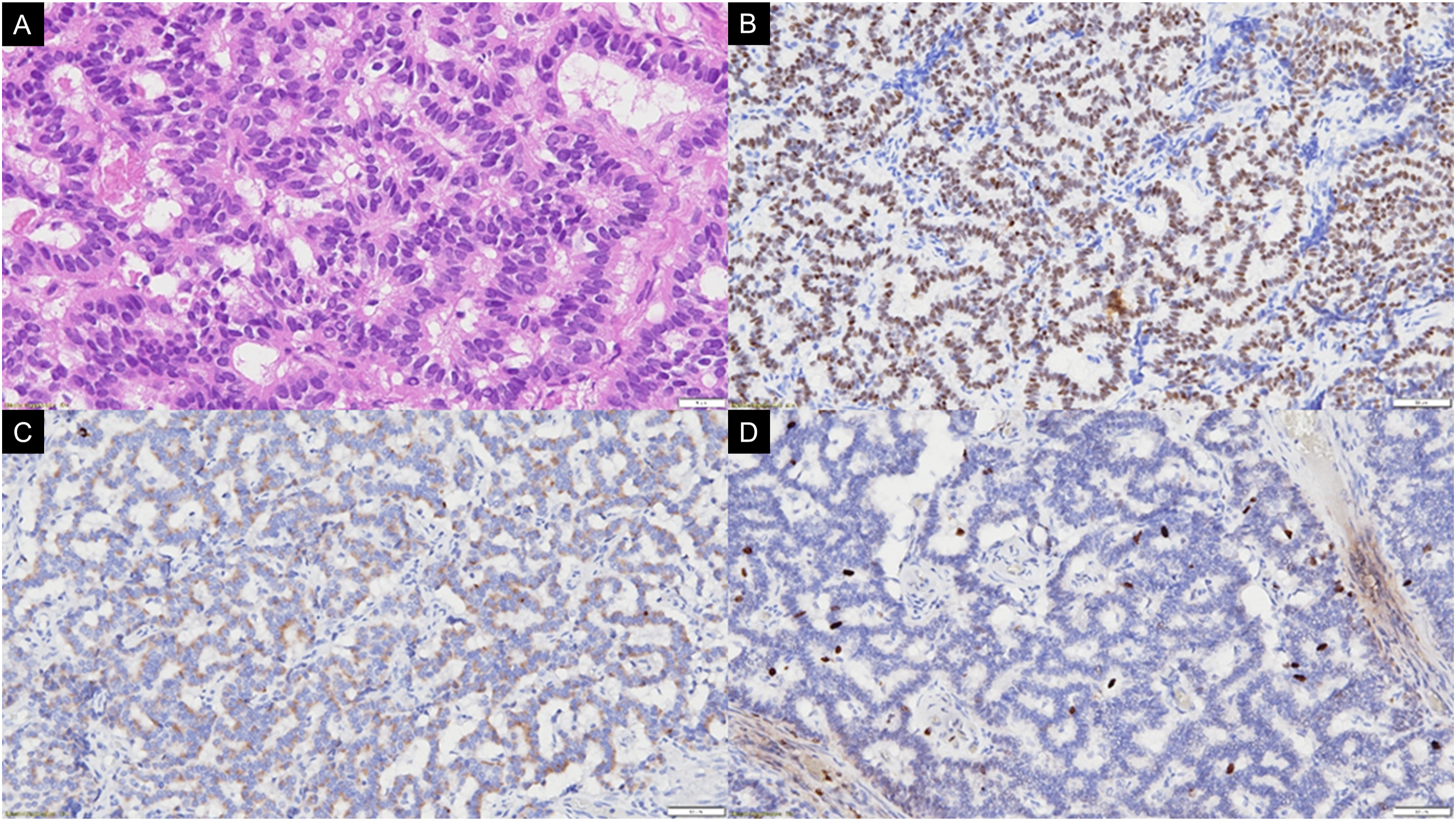
A 25-year-old woman presented with a 2-month history of tinnitus, dizziness, and left-sided conductive hearing loss. Otoendoscopy revealed a well-circumscribed, gray-white, vascular mass behind the tympanic membrane (Figure 1A). Computed tomography showed that a soft-tissue lesion in the epitympanum extended to the mastoid antrum (Figure 1B). The patient underwent transcanal endoscopic excision of the tumor (Figure 2). Histopathologic examination demonstrated a well-differentiated neuroendocrine tumor (Figure 3A), with positive immunohistochemical staining for INSM-1 (Figure 3B) and chromogranin-A (Figure 3C). The Ki-67 proliferation index was less than 3% (Figure 3D). At 8 years of follow-up, hearing levels remained stable, and serial magnetic resonance imaging and endoscopic examinations showed no evidence of recurrence. Clinical and radiologic presentation. (A) Transcanal endoscopic view of the left ear demonstrating a well-circumscribed, gray-white, vascularized retrotympanic mass. (B) High-resolution computed tomography of the temporal bone showing focal soft tissue opacification within Prussak’s space without evidence of significant osseous erosion Endoscopic Middle Ear Tumor Resection and Tympanoplasty. (A) Preoperative endoscopic view of the middle ear tumor mass, which is well-visualized behind the intact tympanic membrane. (B) Initiation of tympanomeatal flap elevation from the posterosuperior external auditory canal wall. (C) Continued elevation of the tympanomeatal flap to fully expose the middle ear cavity and tumor. (D) Atticotomy (epitympanic bone removal) performed using a diamond burr for enhanced access to the tumor mass. (E) Gross visual appearance of the exposed tumor within the epitympanum and attic region. (F) View of the middle ear cavity following en-bloc resection of the tumor, showing the surgical bed. (G) Placement and positioning of a tragal cartilage graft to reconstruct the osseous defect in the external auditory canal. (H) Final postoperative view showing the reconstructed ear canal and a secure graft with intact tympanic membrane Representative histopathology and immunohistochemistry. (A) The tumor exhibits diverse architectural patterns, including tubular, glandular, and rosette-like arrangements. Neoplastic cells display relatively fine chromatin and occasional nuclear inclusions (H&E, original magnification ×40). (B) Strong nuclear expression of INSM1, a sensitive marker for neuroendocrine neoplasms (original magnification ×20). (C) Diffuse cytoplasmic immunoreactivity for chromogranin A confirms neuroendocrine differentiation (original magnification ×20). (D) The Ki-67 proliferation index is low (less than 2%), consistent with a well-differentiated, low-grade neoplasm (original magnification ×20)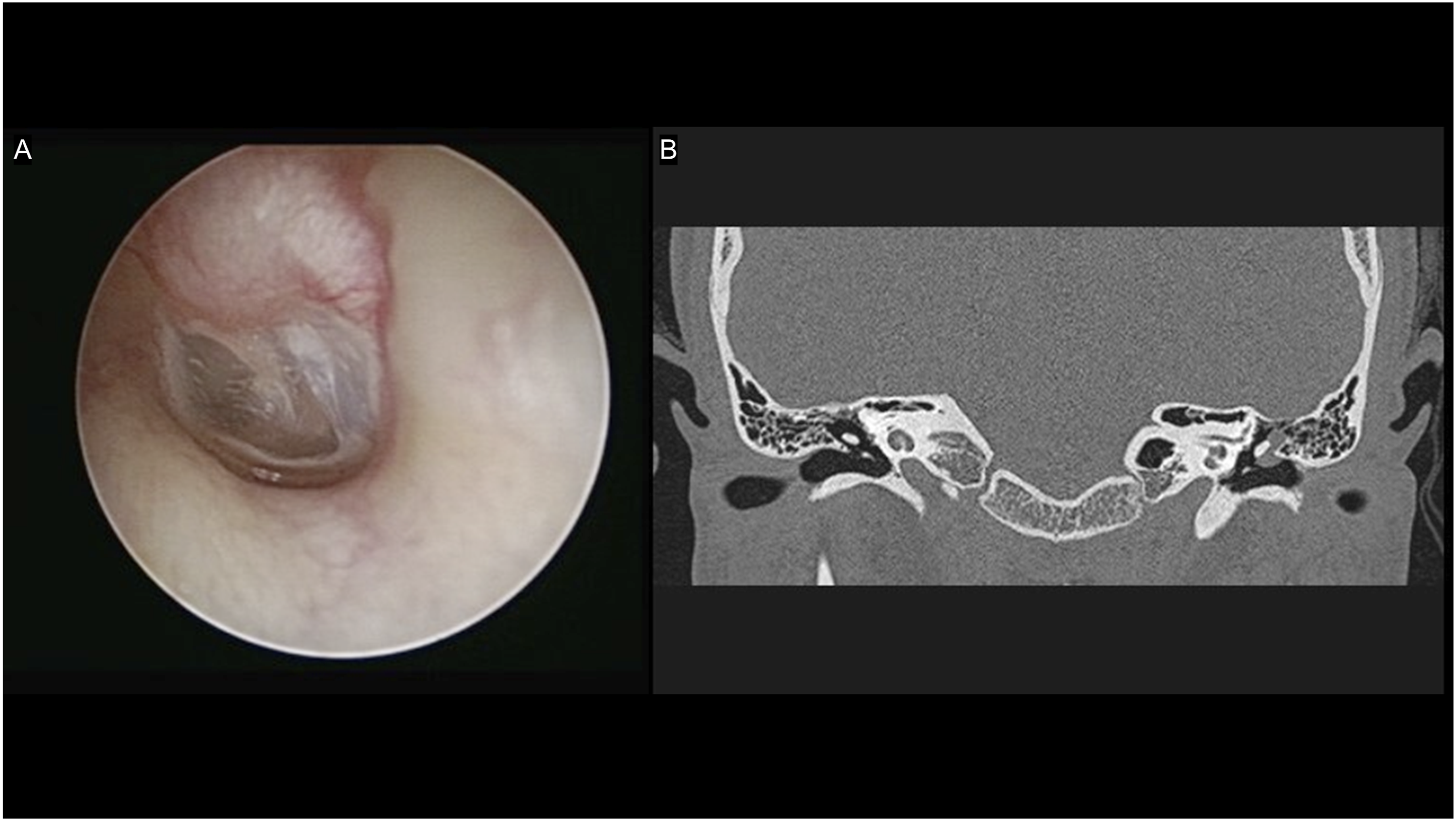

Discussion
Nomenclature and Classification
The nomenclature of middle ear neuroendocrine neoplasms has historically been a source of confusion, with terms such as “middle ear adenoma,” “carcinoid tumor of the middle ear,” and “adenomatous neuroendocrine tumor” often used interchangeably. However, the 2022 WHO classification of head and neck neuroendocrine neoplasms has standardized these entities as well-differentiated neuroendocrine tumors (NET). These are graded G1–G3 based on mitotic count and Ki-67 index, distinguishing them from high-grade neuroendocrine carcinomas (NEC) characterized by TP53 or RB1 alterations. The currently preferred contemporary designation is middle ear adenomatous neuroendocrine tumor (MEANT). 1
Epidemiology and Pathogenesis
MEANT demonstrates no clear sex predilection, typically presenting at a mean age of 45 years (range 19–80 years). The histogenesis remains a subject of ongoing debate; although the normal middle ear mucosa lacks identifiable neuroendocrine cells, MEANT consistently expresses neuroendocrine markers. This suggests the tumor likely derives from pluripotent endodermal stem cells within the middle ear mucosa that are capable of bidirectional mucinous and neuroendocrine differentiation.
Clinical and Radiologic Presentation
Clinical symptoms are largely nonspecific and frequently overlap with more prevalent middle ear pathologies. Patients most commonly present with conductive or mixed hearing loss (∼90%), aural fullness (∼50%), and tonal tinnitus (∼46%). Less frequent findings include pulsatile tinnitus, facial nerve paresis, and rarely carcinoid syndrome. 2 Otoscopy typically reveals a nonspecific retrotympanic mass, which may lead to an initial misdiagnosis of temporal bone paraganglioma (31%) or cholesteatoma (15%). Computed tomography (CT) of the temporal bone generally demonstrates a well-defined soft tissue mass within the middle ear cavity; while ossicular erosion may be present, aggressive osteolysis is typically absent. 3
Histopathology and Immunohistochemistry
Definitive diagnosis relies upon comprehensive histopathological evaluation. MEANT exhibits diverse architectural patterns, including trabecular, solid, glandular, and organoid arrangements. The neoplastic cells are typically small and uniform, characterized by the classic “salt and pepper” neuroendocrine chromatin. A diagnostic hallmark is the evidence of dual differentiation, the presence of both epithelial/glandular and neuroendocrine cell populations.
Immunohistochemical profiling is essential for confirmation. The tumors are characteristically positive for cytokeratins (pan-CK and variable CK7) and neuroendocrine markers, including synaptophysin, chromogranin A, neuron-specific enolase (NSE), INSM1, and ISL1. 4 Conversely, they are negative for TTF-1, CDX2, and PAX8, which aids in excluding metastatic neuroendocrine tumors from other primary sites. Myoepithelial markers are also consistently negative. The Ki-67 index is typically low, reflecting its status as a well-differentiated, low-grade neoplasm.
Management and Prognosis
Complete surgical excision remains the mainstay of treatment. 5 Given the documented propensity for delayed recurrence, sometimes occurring decades after the initial surgery, indefinite long-term surveillance involving clinical examination and periodic imaging is strongly recommended.
Footnotes
Ethical Considerations
We confirm that written informed consent has been obtained from the patient for the publication of this case report. Additionally, this study has received approval from the Institutional Review Board (IRB).
Funding
This work was supported in part by grants from the Ministry of Science and Technology, Taiwan (NSTC 113-2314-B-016-011-MY3 to C.P.S.), and the Tri-Service General Hospital grants (TSGH-A-115005 to C.P.S.).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Protocol
The Institutional Review Board of Tri-Service General Hospital, National Defense Medical University, had approved this study. (No. A202515046).