
Abstract
The aim of this research was to examine predictors of pain detection accuracy. In Study 1 (n = 160, undergraduates), the predictors were distal factors (empathy, emotion recognition, family history, and past experiences with pain), and in Study 2 (n = 104, undergraduates), the predictor was a proximal factor (an experimentally induced experience of pain). Results showed that having past and an immediate experience with pain as well as being more empathic were associated with higher pain detection accuracy scores. Men were more accurate at detecting pain than women in both studies. Our findings contribute to a growing literature on pain detection and empathy.
When observing visceral experiences, such as someone in pain, the perceiver is always lacking the sensations and somatic information that allow for an accurate interpretation of what the situation feels like for the person enduring the pain. Loewenstein (1996) theorized that when making decisions about others, people are likely to ignore or radically underweight the impact of visceral factors on them and have difficulty predicting the behavior of others who are experiencing intense visceral factors.
In accordance with Loewenstein’s (1996) argument, it is well documented that physical pain is poorly assessed by perceivers through underestimation or even failure to recognize that pain is being experienced (K. D. Craig, 2009; Melzack, 1990). Prkachin, Berzins, and Mercer (1994) showed perceivers videotapes of shoulder pain patients undergoing a painful series of movements of their shoulder. Patients and perceivers provided ratings of the pain. Although perceivers could make coarse distinctions among patients’ pain states, they were not sensitive to precisely how much pain the patients were experiencing and tended to underestimate the intensity of the patients’ suffering.
According to the evolutionary theory, understanding another person’s pain coevolved alongside pain behaviors. The person in pain benefited if his or her expression of pain was followed by observer support and assistance in recovery and survival, protection from danger, and obtaining of basic needs (Prkachin, 1997; Prkachin, Currie, & Craig, 1983). The observer also benefited from the signal of pain by gaining important information about potential danger. But limited research has been done on what traits or experiences may increase the ability to recognize and accurately detect the intensity of pain another person is feeling. A recent experience of pain may benefit a perceiver’s ability to understand and accurately detect how that pain feels for someone else because the pain experience is more readily available to the perceiver. Moreover, some people may be generally better perceivers of others’ pain, either learned through a past history of experiences caring for someone in pain or through their own past painful experiences. The ability to understand another person’s pain may also reflect a trait form of empathy that allows one to understand others’ feelings in general more accurately.
The present two studies examined (a) distal trait correlates of pain detection accuracy and (b) the proximal effect of a recent experience of pain on pain detection accuracy. Distal properties are defined as traits or enduring properties of the self that a person carries from one experience to another. Proximal properties are transitory states that change as a function of an immediate experience or event. In Study 1, we hypothesized that people higher in trait empathy and emotion recognition, and those who self-reported having a history of pain for themselves or helping others in pain would be more accurate at the pain detection tests (Ruben & Hall, 2013). In Study 2, participants were randomly assigned to undergo a pain procedure in the laboratory, or no pain experience, and were then asked to judge the intensity of videotaped pain expressions in the same pain detection tests as in Study 1. We hypothesized that those with a recent experience of the same type of pain would have increased pain detection accuracy compared with those who did not experience the pain.
Distal Correlates of Pain Detection Accuracy
Empathy for Pain
Past theory and research have proposed that empathy, not just for pain, is affected by both proximal and distal properties (Goubert et al., 2005). Empathy involves sharing the perceived emotion of another—having an emotional response that originates from another’s emotional state or condition and is congruent with that state (Eisenberg & Strayer, 1990).
Hall, Andrzejewski, and Yopchick (2009) conducted a meta-analysis of the psychosocial correlates of interpersonal sensitivity and found a significantly positive, though weak, relationship between empathy and accuracy in interpersonal sensitivity tasks. It was hypothesized that there would be a positive relationship between self-reported ability to empathize with others, as assessed through the Interpersonal Reactivity Index (IRI; Davis, 1980) and ability to accurately detect pain. The IRI has two scales that are relevant to our hypothesis, the empathic concern (EC) scale and the personal distress (PD) scale. The EC scale measures feelings of compassion toward others in distress while the PD scale measures personal feelings of distress when facing other people’s negative experiences (Davis, 1980). We hypothesized that people higher on the EC scale and the PD scale would have higher pain detection accuracy because all three skills require the ability to understand others in distress.
Though self-reported empathy was hypothesized to be a distal correlate of pain detection accuracy, among other tests of interpersonal sensitivity such as emotion recognition tests, past research has shown inconsistent relationships between tests. For example, the Diagnostic Analysis of Nonverbal Accuracy 2–Adult Facial Expressions (DANVA2-AF; Nowicki & Duke, 1994), a test of accuracy of recognizing emotional expressions in the face, was unrelated to accuracy for judging another person’s thoughts and feelings (Lewis & Hodges, 2011). The authors reason that judging facial expressions may require a bottom-up approach that requires perception of immediate cues while judging thoughts and feelings requires a top-down approach that relies on mental representations. It was expected that there would be a positive correlation between the DANVA2-AF and pain detection accuracy because pain detection accuracy and emotion recognition both require perceivers to use bottom-up approaches related to the target person’s nonverbal expressions to judge how that person is feeling.
Though typically not discussed as an emotion, pain has conceptual similarity to negative emotions such as fear, anger, disgust, and sadness. Both pain and negative emotions act as social signals that provide information to perceivers about a person’s state (Simon, Craig, Gosselin, Belin, & Rainville, 2008). They also share physiological reactivity and phenomenological aspects, and both are recognized and experienced as aversive states. For example, the anterior cingulate cortex (ACC), a site of physical pain processing (Rainville, 2002), is also activated during social pain (Eisenberger, Lieberman, & Williams, 2003). The periaqueductal gray (PAG), a region that receives input from the body’s injury detection mechanism or nociceptive system (A. D. Craig & Dostrovsky, 1999), is activated in rat pups in distress on separation from their mother (Panksepp, 1998). Finally, DeWall et al. (2010) found that acetaminophen, a physical pain suppressant, reduced reports of social pain and reduced neural responses to social rejection in the dorsal anterior cingulate cortex (dACC) and anterior insula (AI), regions associated with social pain and the affective component of physical pain. The overlapping brain regions associated with both negative emotions and physical pain are mostly documented in the person experiencing pain. Limited research has addressed how perceivers view physical pain and negative emotions of others and how these types of accuracy are related. One study showed that physical pain has distinct facial expressions that are recognized by perceivers with specificity and sensitivity when compared with other negative emotional expressions (Simon et al., 2008).
Past Memory and Family History of Pain
Another distal factor that has yet to be examined in the context of pain detection accuracy is one’s memory or self-reported past experiences with pain and family history of pain. It was hypothesized that having a history of experiencing pain and a memory of observing a loved one in pain would predict ability to accurately detect pain. According to Jackson, Meltzoff, and Decety (2005), prior experiences with pain could lead to more accurate judgments of others because the information is more readily available to the perceiver and the perceiver may have learned how to judge pain accurately through practice associated with seeing the expressions. To our knowledge, past research examining family history of pain has only examined its effect on self-perceptions of experimentally induced pain, not on judgments of others’ pain. In the studies that have examined the effect of family history of pain on self-perceptions of experimentally induced pain, results showed that those who report a greater frequency of pain in their family also experience higher intensities of experimental pain, especially in females (Fillingim, Edwards, & Powell, 2000). This enhanced feeling of pain in people who self-report higher frequencies of a family history of pain may allow these people to understand another person’s pain more accurately. By feeling higher intensities of pain, these people may in turn judge higher pain intensities in others, making them more accurate, as past research has shown an overall underestimation when making judgments of others’ pain (Forrest, Hermann, & Andersen, 1989; Grossman, Sheidler, Swedeen, Mucenski, & Piantodosi, 1991).
Proximal Correlates of Pain Detection Accuracy
Recent Experience of Pain
So far, the trait form of empathy and its relation to pain detection accuracy have been addressed. A fundamental component of empathy is a sense of understanding the personal experience of another person (Goubert et al., 2005). We propose that the proximal experience of undergoing a pain task allows perceivers to make more accurate judgments when watching target persons undergo the same pain task. The shared representation model of pain empathy argues that observing another person in pain automatically activates affective and somatosensory pain representations in the perceiver, which may in turn allow for a better understanding of the experience of pain in someone else (Jackson, Rainville, & Decety, 2006). Thus, one’s ability to automatically empathize with another person in pain, just by having the experience of the pain task, may increase recognition, assessment, and accuracy when judging another person’s pain. Empathy not only includes cognition—the ability to know what another person is feeling—but also affective and behavioral responses, such that one actually feels what the other person is feeling. We propose that having a recent experience of pain evokes empathy by allowing the perceivers to understand the personal experience of the target persons in the videotaped pain detection tests (Ruben & Hall, 2013), which in turn increases the perceiver’s ability to accurately assess pain compared with those perceivers who did not undergo the pain task. It should be mentioned that a perceiver can be accurate in detecting the intensity of pain of another person without necessarily feeling an affective response or empathy, though we predict that empathy helps in making a more informed judgment.
In Study 2, experiencing the same painful task prior to making judgments about someone else in pain would allow the perceiver to feel (whether consciously or nonconsciously) what the person in pain was feeling and it would allow the perceiver to make a more accurate assessment of how much pain the person was experiencing compared with someone who had not had the same painful experience. Only one study that we are aware of has examined the effect of an experimental pain task on judgments of the same type of pain. Robinson and Wise (2004) examined the effect of giving the cold pressor task before or after making judgments of videotaped, cold pressor task targets’ pain. Participants given the cold pressor task prior to making their pain judgments rated the videotaped targets as in more pain than those participants given the cold pressor task after making judgments of the targets’ pain. The authors inferred that the experience of the same type of pain prior to making judgments increased their accuracy because of the past literature that has shown an overall underestimation of others’ pain; however, they did not calculate actual accuracy scores.
Numerous fMRI studies have shown that observing photographs of another person in pain (Botvinick et al., 2005; Jackson et al., 2005) or watching a loved one experiencing pain (Singer et al., 2004) activates similar brain regions—anterior cingulate, AI, the cerebellum, and the thalamus—as experiencing pain oneself. In one study, the affective qualities of the pain regions in the brain were activated while watching a loved one in pain (bilateral AI, rostral anterior cingulate cortex, brainstem, and cerebellum; Singer et al., 2004). The activation of the affective dimensions of the brain while observing someone in pain has many functional benefits. These benefits include predicting the effects of the stimuli on the self, staying away from the threat or danger of a painful stimulus, and also understanding the emotions another person is feeling while undergoing pain so one is better able to support and help that person cope with the pain (Williams, 2002).
This past research has implied that accuracy in judging another person’s pain may be partly due to the activations of similar affective and somatosensory brain regions as if the person making the judgments were in pain himself or herself. Similar to watching someone else in pain, experiencing pain provides relevant information to the perceiver when making judgments about the intensity of pain someone else is feeling.
Suppressed, Genuine, and Exaggerated Pain Expressions
Although pain is a private experience, it is often experienced in the presence of another person. Pain serves as a sign of threat not only for the sufferer (Eccleston & Crombez, 1999) but also for onlookers who are more likely to attend to a person who is displaying painful behaviors and facial expressions (Cano, Barterian, & Heller, 2008; K. D. Craig, 2004; Goubert et al., 2005; T. Hadjistavropoulos & Craig, 2002). Although nonverbal expressions of pain have been shown to be more automatic than self-reports of pain, nonverbal expressions can be controlled through higher mental processes to gain resources such as pain medications (T. Hadjistavropoulos & Craig, 2002), to maximize proximity and solicit assistance and empathic responses from others (Sullivan et al., 2010), or even to avoid attention or control pain as documented in lung cancer patients (Wilkie, Keefe, Dodd, & Copp, 1992).
These nonverbal expressions of pain are particularly important to understand in nonverbal populations, including infants and people with cognitive or physical impairments who cannot self-report their pain levels (Herr et al., 2006). For these reasons, we were interested in how perceivers interpret these pain expressions and how accurate perceivers are in judging the intensity of pain when they have knowledge of the type of expression. Many studies have shown that suppressed, genuine, and exaggerated pain displays vary in their use of facial expressions and intensities of expressions (Hill & Craig, 2002; Larochette, Chambers, & Craig, 2006). Perceivers are better than chance at discriminating between exaggerated and genuine pain, but only marginally (H. D. Hadjistavropoulos, Craig, Hadjistavropoulos, & Poole, 1996; Poole & Craig, 1992). To replicate and extend past research findings, we examined the distal and proximal correlates of pain detection accuracy for three types of real pain: suppressed, genuine, and exaggerated.
Finally, we examined gender effects in pain detection accuracy. Past research examining gender differences in pain detection accuracy is limited. Prkachin, Mass, and Mercer (2004) found that women outperformed men in judging pain in a signal detection framework showing observers 1-s videotapes of no pain or moderate pain. This is consistent with a large body of earlier research finding females to be more accurate than males in a number of domains, for example, in judging emotions (Hall, 1984). However, Roberts and Pennebaker (1991) found that men were more accurate than women at judging their own interoceptive states or internal states, based on a review of the literature, which could have a bearing on accuracy on pain judgment as discussed later.
Present Research
To recap, the present research aimed to examine distal and proximal correlates of accurate pain detection for three types of real pain: suppressed, genuine, and exaggerated. The distal factors were the tendency to empathize, emotion recognition accuracy, past experiences with pain, and family history of pain, and the proximal factor was experiencing pain in the task.
Study 1
Method
Participants
One hundred sixty (63 male and 97 female) introductory psychology students were recruited at Northeastern University for partial fulfillment of course requirements. Participants ranged in age from 17 to 25 years. One hundred participants were Caucasian, 35 were Asian American, 12 were identified as Other, 10 were Hispanic American, and 3 were African American.
Materials
Pain detection tests
Participants’ accuracy of detecting pain in others was measured with newly developed pain detection tests (Ruben & Hall, 2013). The pain detection tests contain 51 target persons (46% female) who were videotaped while undergoing a 15-min tourniquet task (Smith, Egbert, Markowitz, Mosteller, & Beecher, 1966) and were asked to suppress their pain expressions (Ntarget = 19), show genuine expressions of pain (Ntarget = 16), or exaggerate their pain expressions (Ntarget = 16). The tourniquet task involves wearing an inflated blood pressure cuff around the upper arm while performing handgrip exercises, which causes an increasing sensation of ischemic muscle pain by occluding blood flow to the arm and hand. Video clips were selected individually for each target person and included the first 30 s of the tourniquet task (activation), the 30 s leading up to each target’s pain threshold (the point at which each participant self-reported actual physical pain), and the 30 s leading up to each target’s tolerance time (the point at which each participant ended the task). All of the clips of the target persons who displayed a suppressed expression were compiled into a Suppressed Pain Detection Test and the same was done to create a Genuine Pain Detection Test and an Exaggerated Pain Detection Test. Each detection test consisted of approximately 50, 30-s video clips that were randomly ordered by clip (activation, threshold, and tolerance) and target. The three types of clips (activation, threshold, and tolerance) were distributed evenly across Pain Detection Tests. There was an average of 37% activation clips, 32% threshold clips, and 31% tolerance clips in the suppressed, genuine, and exaggerated pain detection test. Each clip had a corresponding pain rating made by the original target person at the end of that 30-s video clip on a visual analog scale (VAS; 100 mm in length).
Study 1 participants were asked to assess the target person’s pain after watching the entire 30-s video clip on the same pain VAS, so that the accuracy of each participant across clips could be assessed by correlating their judgments of pain with the actual intensity of pain the target persons reported.
Other measures
Participants’ trait empathy was measured with the Interpersonal Reactivity Index (IRI; Davis, 1980) and participants’ emotion recognition ability was measured with the Diagnostic Analysis of Nonverbal Accuracy 2–Adult Facial Expressions (DANVA2-AF; Nowicki & Duke, 1994).
The IRI consists of 28 items comprising four subscales: Perspective Taking (PT), Fantasy (FS), EC, and PD. The PT subscale measures the tendency to adopt the perspective of others, the FS subscale measures the tendency to identify with characters from fictional situations, the EC subscale measures feelings of compassion toward others in distress, and the PD subscale measures personal feelings of distress when facing other people’s negative experiences (Davis, 1980). The DANVA2-AF is a 24-item test of decoding four emotions (happy, sad, angry, or fearful) in photographs of posed facial expressions (Nowicki & Duke, 1994). Participants completed a family history and self-history of pain experiences: whether they had experienced acute pain (defined as pain caused from a traumatic injury, surgical procedure, or medical disorder that did not last longer than expected) or chronic pain (defined as pain that is persistent often lasting more than 6 months or longer than expected), what type of pain it was, and how long it persisted. Participants were also asked whether they had observed someone else (i.e., a family member or close friend) in acute or chronic pain, what type of pain it was, and how long the person’s pain persisted.
Finally, participants completed demographic information including their age, ethnicity, and gender.
Procedure
The research received approval from the Office of Human Subject Research Protection of Northeastern University and informed consent was obtained from each participant. Participants were randomly assigned to one of the three pain detection tests. Fifty-one participants took the suppressed pain detection test, 55 took the genuine pain detection test, and 54 took the exaggerated pain detection test. Participants made ratings every 30 s about how much pain they thought the target persons in the videotape were experiencing on a 0 to 100 VAS from “no pain at all” to “the most intense pain they could imagine.” Participants were told about the pain detection test they would be watching to make them understand (with no explicit instruction other than the type of Pain Detection Test) that people who were asked to suppress their pain may appear to be experiencing no pain when in fact they are in pain while people exaggerating their pain may appear to be experiencing a maximum amount of pain when they are only experiencing a moderate intensity of pain (see Appendix A for the script). Participants were then given the DANVA2-AF (Nowicki & Duke, 1994), the IRI, the questionnaire on their experiences with acute and chronic pain, and the demographics questionnaire.
Results
Target pain ratings
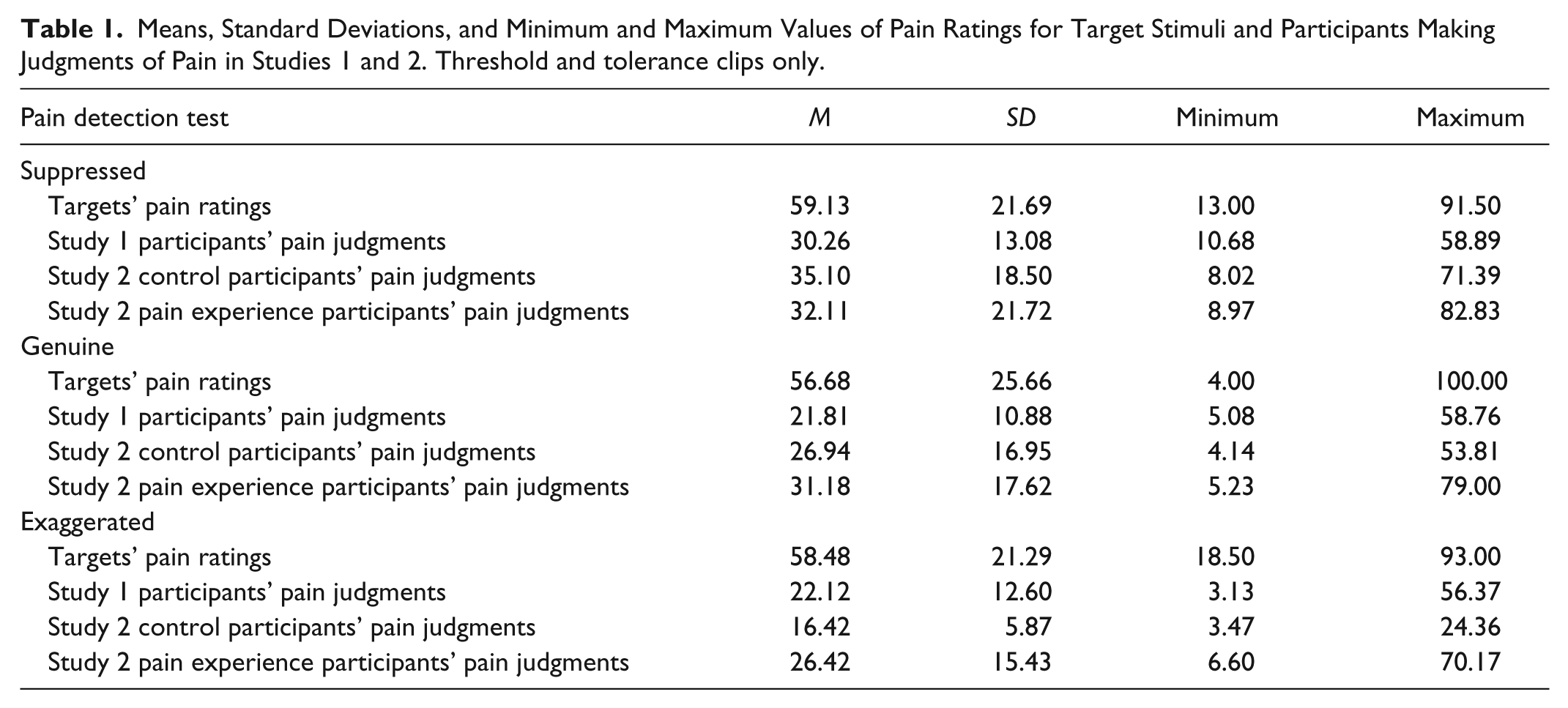
The threshold and tolerance clips were used for all further analyses as these were the clips that showed pain. There were no significant differences in targets’ own pain ratings according to the expression condition they had been assigned to, F(2, 59) = 0.10, p = .91 (see Table 1 for means, standard deviations, and minimum and maximum pain ratings).
Means, Standard Deviations, and Minimum and Maximum Values of Pain Ratings for Target Stimuli and Participants Making Judgments of Pain in Studies 1 and 2. Threshold and tolerance clips only.
Judge pain ratings
There was a significant difference in judge pain ratings across the 3 clips according to the pain detection test participants were assigned to, F(2, 159) = 8.05, p < .001. Tukey post hoc tests confirmed at the p < .001 level that participants rated the suppressed pain targets (M = 30.26, SD = 13.08) as displaying significantly greater levels of pain than the genuine (M = 21.81, SD = 10.88) and exaggerated pain targets (M = 22.12, SD = 12.60). Although targets were not reporting significant differences in pain levels, judges perceived differences in how much pain the suppressed, genuine, and exaggerated targets were experiencing.
Pain detection accuracy
Accuracy scores were calculated by correlating each participant’s pain ratings of the target persons with the target persons’ pain self-ratings. Accuracy scores were transformed into Fisher z scores for analyses and transformed back into Pearson correlation coefficients for presentation. Results for the Kolmogorov–Smirnov test for normality indicated that the accuracy scores did not deviate significantly from a normal distribution. Three outliers were found (one in the genuine pain detection test and two in the exaggerated pain detection test). All analyses were rerun without these outliers and no differences emerged, so the following analyses contained the outliers.
A one-sample t test was conducted against zero to examine whether participants’ accuracy was above chance levels. On the exaggerated pain detection test, participants performed better than chance. On the suppressed and genuine pain detection tests, participants were at the chance level (see Table 2 for means and t tests).
Accuracy on Pain Detection Tests (r) in Studies 1 and 2.
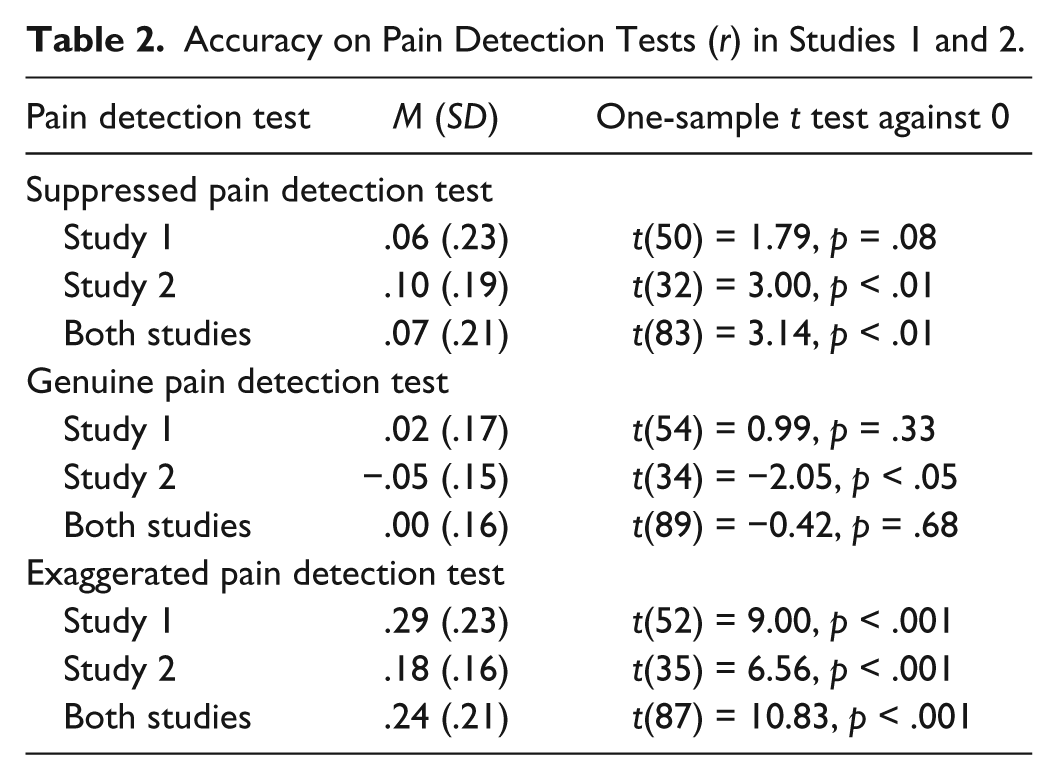
A one-way analysis of variance (ANOVA) examining differences in accuracy by pain detection tests (suppressed, genuine, or exaggerated) was significant, F(2, 157) = 24.37, p < .001. A Tukey post hoc analysis showed that the exaggerated pain detection test participants were significantly more accurate than the suppressed pain detection test participants and the genuine pain detection test participants, but there was no significant difference between accuracies on the suppressed and genuine pain detection tests (see Table 2 for means).
Distal Correlates of Pain Detection Accuracy
Because accurately detecting pain in others has been proposed as a form of empathy, this claim was tested by correlating participants’ scores on the four scales of the IRI (Davis, 1980) with their pain detection accuracy score on one of the three pain detection tests that they were randomly assigned to. Combining the three test conditions (suppressed, genuine, and exaggerated), pain detection accuracy was correlated with EC, r(157) = .18, p < .05. That is, the more accurate the participants were in detecting pain in the target persons, the more they reported feeling compassion for others in distress. The PD subscale of the IRI showed a nonsignificant positive correlation with pain detection accuracy, r(157) = .12, p = .12. When examining the correlation between the scales of the IRI and pain detection accuracy by test (suppressed, genuine, and exaggerated), there were no longer significant correlations between EC and accuracy; only a marginally significant result remained for the suppressed pain detection test, r(49) = .26, p = .07. The lack of effect within tests is most likely due to a lack of power as splitting the correlation by test decreased the sample size by one third.
Pain detection accuracy was examined in relation to a test of emotion recognition, the DANVA2-AF (Nowicki & Duke, 1994). This correlation was nonsignificant, r(157) = −.04, p = .60, as were the correlations between pain detection accuracy and the four subtest emotion accuracies of the DANVA2-AF: happy r(156) = −.06, p = .49; sad r(156) = −.06, p = .47; angry r(156) = .03, p = .74; and fearful r(156) = −.04, p = .67. It did not vary with high- or low-intensity emotion stimuli: high intensity, r(156) = −.04, p = .61; low intensity, r(156) = −.05, p = .53. These findings show that pain detection accuracy as a skill was not related to the skill of emotion recognition in static photographs.
Participants reported their experiences with acute and chronic pain, through personal experiences and family history of pain, that is, watching a loved one or someone close experience this type of pain. Participants’ open-ended responses were coded for the type of pain and how long it persisted into three major types of pain: somatic (musculoskeletal), visceral (internal), and neuropathic (nerve) pain, and also whether the pain they reported was acute (less than 3 months) or chronic (persisting for 6 months or longer). Accuracy on the pain detection tests was marginally correlated with the report of watching a loved one in acute pain, r(157) = .14, p < .08, and was significantly correlated with the report of watching a loved one experience neuropathic pain, r(157) = .16, p = .05. There were no significant correlations between the participants’ reported own past pain and their pain detection accuracy.
To examine the individual contributions of these distal correlates, pain detection accuracy scores were simultaneously regressed on the scores on the four subscales of the IRI, accuracy on the DANVA2-AF, experience with watching a loved one in acute pain, experience with watching a loved one in chronic pain, and experiencing their own acute or chronic pain (0 = no, 1 = yes), and participants’ gender (0 = male, 1 = female). The overall regression model was significant, F(10, 157) = 2.40, p = .01. EC and reported experience with a loved one in acute pain were significant positive predictors of pain detection accuracy. The PD subscale of the IRI was a marginally significant positive predictor of pain detection accuracy. An unpredicted result that would require further research to understand was the significant negative relationship between the fantasy-seeking subscale of the IRI and pain detection accuracy. Finally, gender was a significant predictor of pain detection accuracy, with males performing better than females (see Table 3 for standardized coefficients). These regressions were also performed for the separate pain detection tests and similar results emerged though not as significant due to the reduction in power by splitting the sample into one third. See Table 4 for a correlation matrix of all variables.
Prediction of Pain Detection Accuracy (r) from Distal Correlates.
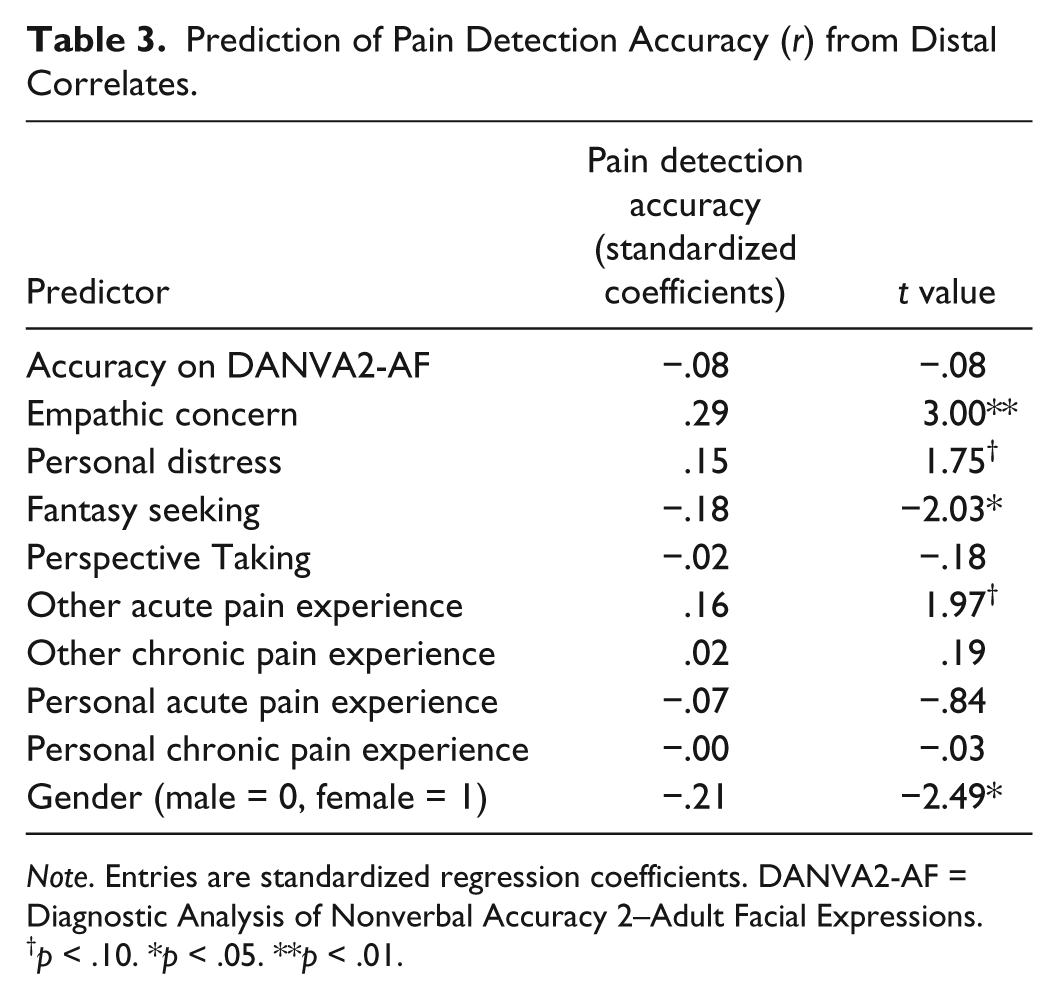
Note. Entries are standardized regression coefficients. DANVA2-AF = Diagnostic Analysis of Nonverbal Accuracy 2–Adult Facial Expressions.
p < .10. *p < .05. **p < .01.
Intercorrelations of Pain Detection Accuracy, Participant Gender, and Distal Variables (Study 1).
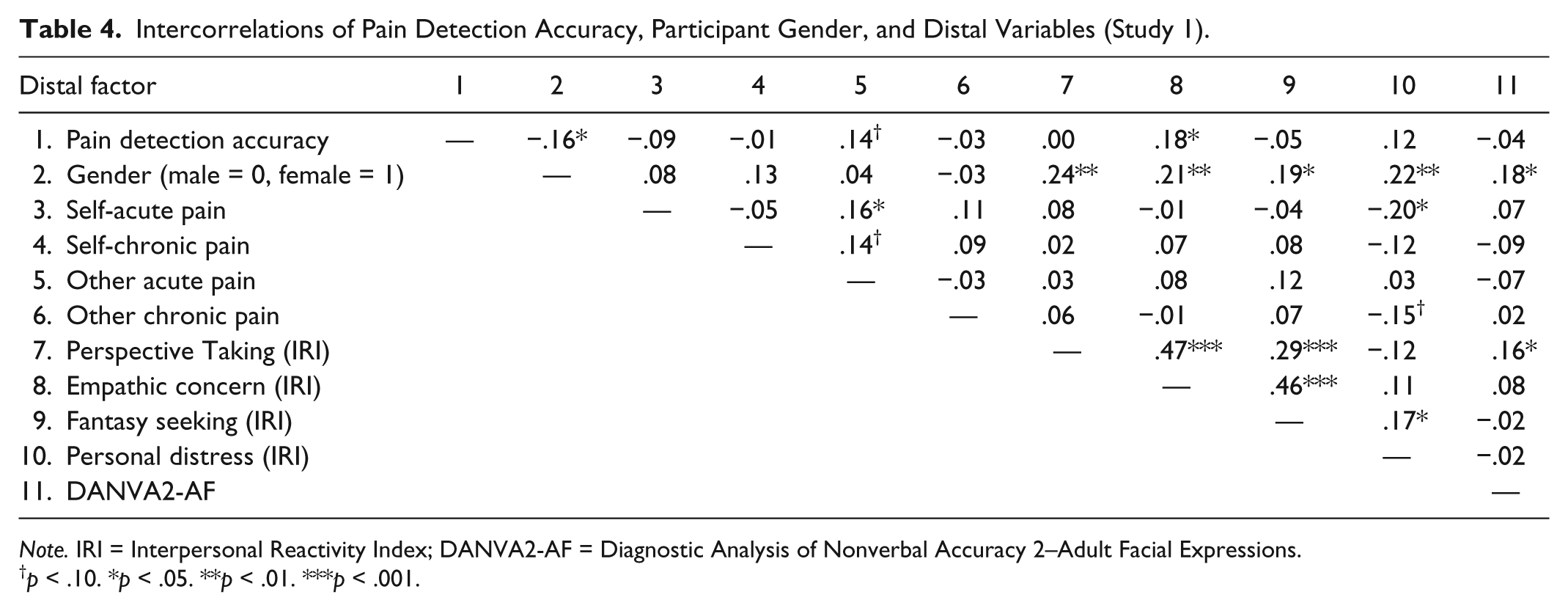
Note. IRI = Interpersonal Reactivity Index; DANVA2-AF = Diagnostic Analysis of Nonverbal Accuracy 2–Adult Facial Expressions.
p < .10. *p < .05. **p < .01. ***p < .001.
To examine the gender difference in judging pain, independent-sample t tests were performed on each pain detection test. Although this trend emerged for each pain detection test, the difference was only marginally significant in the genuine pain detection test, t(53) = 1.94, p < .10 (males, M = 0.08, SD = 0.20; females, M = −0.01, SD = 0.14). There were no significant interactions between the type of pain detection test and gender, meaning that the gender difference was approximately the same for all of the tests.
Discussion
Participants in Study 1 were more accurate than chance when judging exaggerated pain, significantly more than when judging suppressed and genuine pain, both of which were at the chance level. Study 1 confirmed past studies showing that people in general are not very good at judging pain, though this is one of the first studies to examine accuracy in judging ischemic muscle pain. In spite of generally low levels of accuracy, there were individual differences in pain detection accuracy as reflected in the correlations with other variables. Study 1 showed that three distal factors were related to pain detection accuracy: empathy, past experience of other’s acute pain, and gender. The EC scale of the IRI (Davis, 1980) was positively correlated with pain detection accuracy. The PD subscale of the IRI was not significantly correlated with pain detection accuracy, though the correlation was positive and the effect was marginally significant in a multiple regression model. Pain detection accuracy was unrelated to an emotion recognition task, the DANVA2-AF (Nowicki & Duke, 1994), which provides evidence that pain detection, as a skill, is distinct from other measures of interpersonal sensitivity. This is not to say that pain and emotion perception require different psychological processes but being a good judge of negative emotions may require different skills from being a good judge of pain. This finding is also in accordance with most research showing that interpersonal accuracy tasks are only weakly correlated with each other (Hall, 2001).
Participants’ family history of pain or self-reported memories of past experiences observing another person in pain were also positively correlated with pain detection accuracy even when controlling for other distal factors in the regression (IRI, DANVA2-AF, and gender). Participants’ self-reports of past experiences with their own pain were not correlated with their pain detection accuracy. Although it was proposed that past experiences with pain would lead to higher pain detection accuracy, the way participants remember their own pain may be quite different from the way they remember watching a loved one suffer through pain; hence, the need for Study 2 arises. One example of this fading memory of one’s own pain over time can be seen in the memory of childbirth pain. Past research has shown that about half of women remember childbirth pain as less painful after 5 years compared with immediately after, and 2 months after giving birth (Waldenstrom & Schytt, 2009).
Males in our study were significantly more accurate at detecting pain compared with females. This finding is particularly interesting in light of earlier research on interpersonal judgment accuracy. We postpone discussion of this finding until Study 2.
Study 2
To test the effect of the immediate or proximal experience with pain, participants were either assigned to receive a shortened acute ischemic muscle pain task (the tourniquet task) or no task, and were then asked to complete one of the three pain detection tests used in Study 1. It was hypothesized that in line with the shared representation model of pain, participants who experienced pain would be more accurate at judging pain in others.
Method
Participants
One hundred four (35 male, 69 female) undergraduate students from Northeastern University participated. Participants ranged in age from 18 to 22. Sixty participants were non-Hispanic White, 28 participants were Asian or Asian American, 8 were Other, 6 participants were African American, 1 participant was Hispanic American, and 1 participant was Native American.
Each participant was asked health questions prior to starting the study to ensure their eligibility for participation. Qualified students who were enrolled in Introductory Psychology received partial course credit for their participation. Individuals who failed to meet the qualifying criteria were dismissed and granted their partial course credit; this occurred for 20 participants, who were not included in the total sample of 104 participants.
Materials
Questionnaires
Health prescreening questions determined whether participants had any health conditions that would preclude their participation in this study (i.e., high or low blood pressure, heart disease, circulatory problems, Reynaud’s disease, diabetes, neurological disorders, feelings of numbness in hands and feet, used drugs/analgesics/antidepressants, experienced recent symptoms of influenza, or had not eaten in the last 3 hr to preclude fainting).
The demographics questionnaire assessed age, gender, and ethnicity. A VAS was used to rate one’s experience from “no pain at all” to “the worst possible pain” every 30 s throughout the pain task. The pain detection tests described in Study 1 were used to assess participants’ accuracy at judging pain in others.
Procedure
This study had two phases. In Phase I, participants were randomly assigned to undergo a shortened tourniquet task (pain experience condition) or no task (controls), and then all participants completed Phase II. The research received approval from the Office of Human Subject Research Protection of Northeastern University and informed consent was obtained from each participant. In the pain experience condition (n = 62), 22 participants were told to suppress their pain expressions, 21 were told to show a genuine expression of pain, and 15 were told to exaggerate their pain expression (also randomly assigned). In Phase II, they took the pain detection test that matched their condition from Phase I. Forty-two participants were controls who began their experimental session with Phase II, with random assignment to one of the three pain detection tests: 14 took the suppressed pain detection test, 13 took the genuine pain detection test, and 21 took the exaggerated pain detection test.
Phase I
Participants in the pain experience condition were asked health prescreening questions to ensure that they were free of chronic pain and had no known health problems that would put them at risk during the tourniquet procedure prior to the start of the study. The informed consent explained that they had the right to end the study at any time without penalty.
The pain experience participants were given a shortened version of the tourniquet task used in Study 1. The experimenter told the participant to suppress, exaggerate, or show a genuine pain expression throughout the procedure. If the participant did not end the task prematurely, the experimenter ended the task after a maximum of 2.5 min by deflating the cuff. If the participant expressed a desire to end the procedure prior to the time limit of 2.5 min, the experimenter came in and immediately assisted the participant in deflating the cuff if the participant had not already done so. Once the tourniquet task ended, the blood pressure cuff was removed.
Phase II
Participants then completed Phase II of the study in which they were assigned to watch the suppressed pain detection test, the genuine pain detection test, or the exaggerated pain detection test according to the expression they were randomly assigned to express in Phase I (controls were randomly assigned to one of the tests at the beginning of the experiment). Participants assigned to the experience condition in Phase I were told that they would be watching videotapes of the same type of expression that they had expressed in Phase I (suppressed, genuine, or exaggerated). Control participants were told that they would watch video clips of past participants undergoing a painful task in the laboratory that involved wearing an inflated blood pressure cuff around their arm to a very high pressure while performing several handgrip exercises. All participants were told about the pain detection test they were going to watch to aid them in making the correct intensity of pain judgment (see Appendix A for script).
Results
Judge pain ratings
There was a significant difference in judge pain ratings according to pain detection test they were assigned to, F(2, 103) = 4.46, p < .05. Tukey post hoc tests confirmed at the p < .05 level that participants rated the suppressed pain targets (M = 33.38, SD = 20.17) as displaying significantly greater levels of pain than the exaggerated pain targets (M = 21.60, SD = 13.00) but not different from the genuine pain targets (M = 29.56, SD = 16.75). There was not a significant difference between pain ratings of the genuine pain targets and exaggerated pain targets. Although targets were not reporting significant differences in pain levels (see Results from Study 1), judges perceived differences in how much pain the suppressed and exaggerated targets were experiencing.
Pain detection accuracy
Accuracy scores were created the same way as in Study 1, by correlating each participant’s pain rating of the target persons with the target persons’ self-reported pain across the threshold and tolerance video clips. Accuracy scores were transformed into Fisher z scores for all analyses and transformed back into correlation coefficients for presentation. Results for the Kolmogorov–Smirnov test for normality indicated that the accuracy scores did not deviate significantly from a normal distribution. There was one outlier in the genuine pain detection test. All analyses were rerun without this outlier and no differences emerged, so the following analyses contained the outlier.
A one-sample t test was conducted against zero to examine whether participants were making their judgments above chance levels for both conditions together. On the suppressed and exaggerated pain detection tests, participants performed better than chance. On the genuine pain detection test, participants were at the chance level (see Table 2 for means, standard deviations, and t tests).
The effect of pain experience and gender on pain detection accuracy
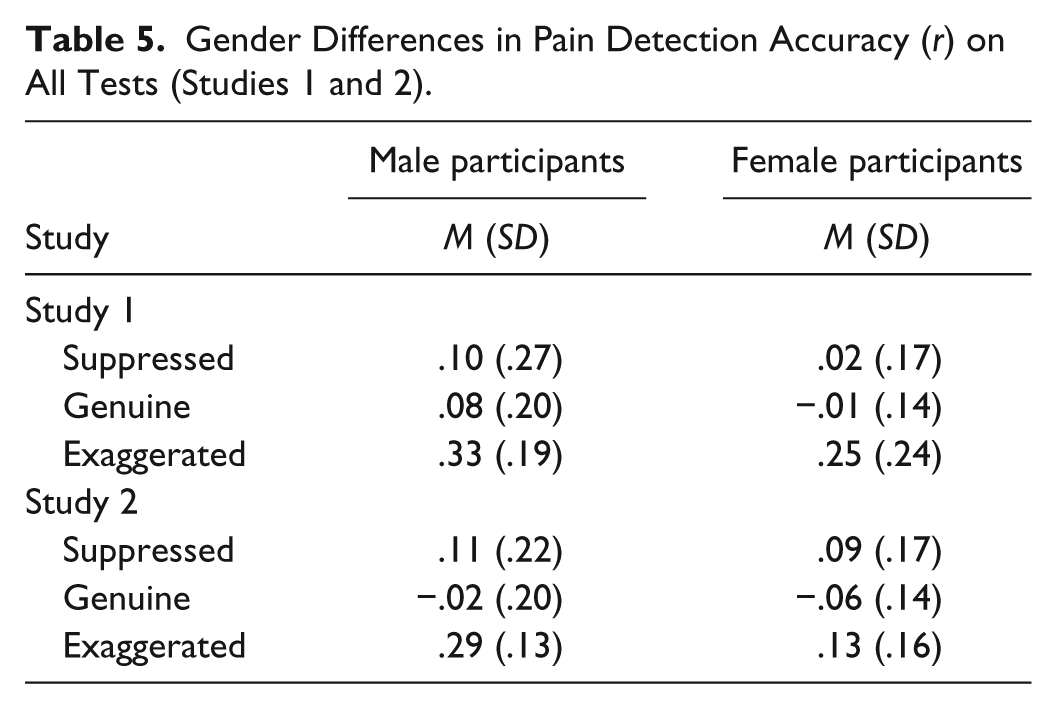
A 3 (pain detection test: suppressed, genuine, exaggerated) × 2 (male vs. female) × 2 (pain experience vs. no pain experience) ANOVA was performed predicting pain detection accuracy. The ANOVA showed main effects of the pain detection test, gender, and pain experience on pain detection accuracy. There were no significant interactions. The pain detection test effect, F(2, 89) = 17.81, p < .001, showed that judges were significantly more accurate at detecting pain on the exaggerated and suppressed pain detection test compared with judges of the genuine pain detection test (p < .05; see Table 2). The gender effect, F(1, 89) = 5.60, p < .05, showed that males were significantly more accurate than females at judging pain, regardless of test and pain experience (see Table 5 for means).
Gender Differences in Pain Detection Accuracy (r) on All Tests (Studies 1 and 2).
Finally, in keeping with the main hypothesis, the pain experience effect, F(1, 89) = 3.91, p = .05, showed that participants who experienced pain in Phase I had significantly higher pain detection accuracy scores in Phase II (M = 0.11, SD = 0.16) than controls (M = 0.05, SD = 0.23; see Figure 1). 1
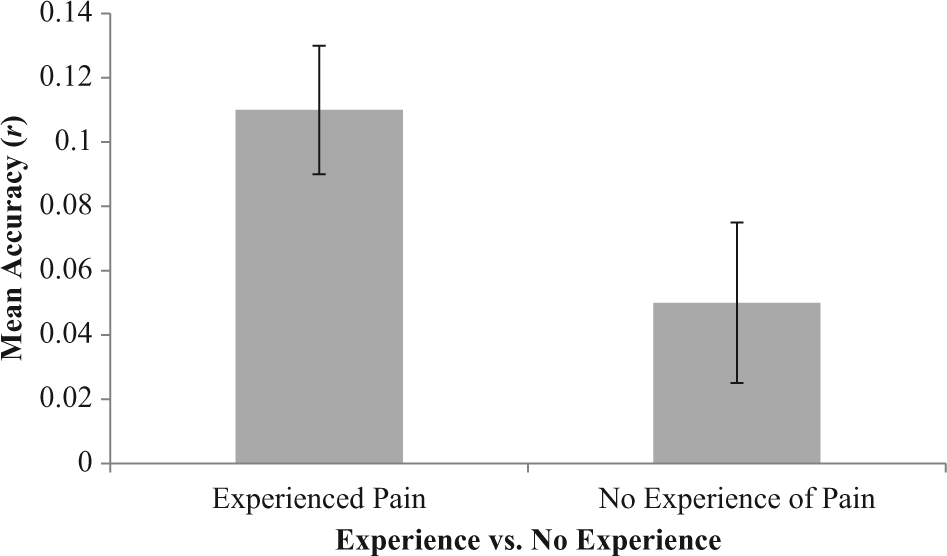
Pain detection accuracy test scores (r) by experimental manipulation of experiencing pain or not experiencing pain (controls): Study 2.
An examination of the original pain ratings made by targets and participants judging pain, prior to creating accuracy scores for each participant, revealed that experiencing pain in Phase II increased judgments of pain in the pain detection tests as compared with the controls who did not experience pain. Table 1 shows that this is particularly true for the genuine and exaggerated conditions where participants who experienced pain tended to have higher pain judgment ratings of the targets. For those who did not experience pain, it appears that these participants had a relatively restricted range and tended to use the lower end of the pain scale when judging targets’ pain. Though there was a shift in the experience participants’ perceptions of pain, this increase in perceptions of pain would not have affected accuracy as accuracy correlations are not affected by a systematic increase or decrease in the means of the variables being correlated, but accuracy correlations are affected by more variance in ratings, which was also found.
Discussion
As in Study 1, the average accuracy levels for judging pain were low. Participants performed below chance on the genuine pain detection test. This finding supports the past literature that has shown that forms of intense acute pain, such as emergency room pain, tend to be underestimated and poorly assessed by physicians and nurses (Ducharme & Barber, 1995; Guru & Dubinsky, 2000). The consistent findings of generally low accuracy on judging genuine pain expressions highlights the need to understand how people perceive others’ pain, how past experiences and empathy for others play an important role in understanding pain, and how pain detection accuracy can be increased. In the suppressed and exaggerated pain detection tests, participants performed better than chance but still at very modest levels. We also replicated our finding from Study 1 that males were significantly more accurate at judging pain compared with females across the type of pain detection test (suppressed, genuine, or exaggerated) regardless of the experimentally manipulated experience of pain.
Regardless of the specific pain detection test, participants assigned to experience pain performed significantly better at detecting pain levels than participants who did not experience pain, which may be due in part to the participants’ increasing variance that may have allowed for a more sensitive discrimination between clips compared with the control participants who had a restricted variance of pain ratings, especially for the genuine and exaggerated pain detection tests.
General Discussion
Current theories suggest that empathy for pain should improve one’s ability to accurately detect pain in others. Our findings suggest that there are several distal and proximal factors that contribute to pain detection accuracy; empathy and past experiences with pain are among these. In Study 1, self-reported EC for others in distress was positively correlated with pain detection accuracy. It was also found that having a family history of acute pain was positively correlated with pain detection accuracy, but having a memory of one’s own pain was not correlated with pain detection accuracy. Study 2 showed that having an immediate experience of pain increased pain detection accuracy.
In Studies 1 and 2, participants had the highest accuracy on the exaggerated pain detection test. In real life, pain expression is often managed deliberately to gain attention or resources. Perhaps the exaggerated pain detection test is most like a real-life judgment for undergraduate participants but not necessarily for emergency room physicians or oncologists who are used to discriminating or at least exposed to different expressions of pain on a daily basis. An alternative explanation could be that our participants were good judges of the stereotypes of pain. Both targets and the participants may have a shared understanding of what exaggerated pain looks like that led to the greater accuracy in this test. Past research has shown that judges’ ratings of patients’ pain experiences corresponded better to the severity of distress deliberately posed rather than the severity of distress actually experienced (Poole & Craig, 1992). Although in our tests target pain ratings did not vary between the suppressed, genuine, and exaggerated conditions under which they were videotaped, perhaps the severity of pain experienced under the exaggerated condition (and across conditions) coincided better with the expression of pain under that condition, making it a smoother transaction for the receiver of the message, the participants making the pain rating judgment, to understand the expressions of the targets. Both explanations contribute to a better understanding of genuine and suppressed pain as neither of these tests had high accuracy, which highlights the poor recognition of suppressed and genuine pain and perhaps the lack of a shared representation of these types of pain expressions.
In Studies 1 and 2, we found that men were significantly more accurate at judging pain compared with women. Most interpersonal sensitivity literature finds women to be more accurate than men. In fact, even in our study, women performed significantly better than men on the DANVA2-AF, a test of emotion recognition. However, a review by Roberts and Pennebaker (1991) found that men were more accurate than women at judging their own interoceptive states or internal states. For example, men are more accurate at detecting their own heartbeats and finger temperature (Pennebaker, 1982), blood pressure (Pennebaker & Watson, 1988), and blood glucose level (Cox et al., 1985). The authors of the review reasoned that men tend to infer their emotions more from internal physiological cues such as heart rate and blood pressure, whereas women infer their emotions from contexts such as social settings. Although men in our study did not know the physiological reactivity of the target persons in the videotapes, perhaps men are more practiced at making accurate judgments of interoceptive processes, such as their own pain, based on their physiological reactivity, and therefore could possibly make judgments about the target person’s pain intensity more accurately than women. Men in our study may have also felt more physiologically aroused by those target persons who were experiencing more pain and then may have based their judgments on their own physiological reactivity. However, the interpretation of the gender difference in pain detection accuracy must remain speculative, as we do not have the physiological data to support the interoception interpretation and the gender difference was not the same as in Prkachin et al. (2004).
Control participants, who did not experience pain, performed worse on the pain detection tests than those who experienced pain. The participants who did not experience pain may have lacked the somatic input and empathy to allow for better recognition of others’ similar pain. In some real-life contexts, however, there may actually be a benefit for the perceiver to not always accurately identify the pain level of another person (Jussim, 1991). To understand completely what another person is feeling or suffering could create harmful cognitive and affective demands if the perceiver then feels pain and suffering as a result (Hodges & Klein, 2001). To not suffer excessively and have difficulty helping the person who is actually suffering as Schaller and Cialdini (1988) propose, participants in our study were acting in a way that was most adaptive for themselves and for the person in pain. This may explain the gender difference in pain detection accuracy. Women in our study may have responded in a way that would have been most adaptive for themselves and for the person in pain in a real-life setting. As Goubert, Craig, and Buysse (2009) explain, perceivers who display a moderate amount of accuracy for judging others’ pain might be the most effective caregivers. This was the case in our study; even when judges were most accurate, on the exaggerated pain detection test, they were still not close to being perfect judges of pain and would certainly fall into the modest range. This is similar to the empathic accuracy literature in which Ickes (2003) has shown that accuracy in interpersonal judgments is far from perfect; perceivers are often only “good enough” (Fiske, 1993). Caregivers who are more accurate at detecting pain may feel others’ pain more, which may diminish their ability to be effective caretakers. Caretakers who are incredibly empathic toward their suffering loved ones may be accurate in identifying the emotion, state, or intensity of pain their loved one is experiencing, but recognizing or acknowledging the cue is only part of being a good caretaker. This accurate assessment of another persons’ pain may create cognitive and affective obstacles in the caregivers’ ability to behave in a supportive manner and relieve the distress of the person suffering.
Past research has shown that in clinical settings, doctors and nurses who work with trauma populations and chronic patients are at higher risk of compassion fatigue and burnout (Kearney, Weininger, Vachon, Harrison, & Mount, 2009). Finding a balance for clinicians and caregivers when making judgments about their patients’ and loved ones’ pain may be a difficult skill, but our study suggests that understanding or feeling a moderate amount of their pain, through empathy, may benefit both parties by allowing the perceiver a window into the patient’s experience and giving the right kind of treatment and support to the patient. Future research should address how training can increase pain detection accuracy by altering one’s ability to empathize “just enough.”
This research adds to the existing literature as emotion recognition has hardly ever been simultaneously studied with pain recognition, and even when studied together, the pain and emotion stimuli were posed. Simon et al. (2008) showed that although there were overlapping action units and misattribution for observers in the posed expression of pain and the six basic emotions (namely fear), pain and the emotions were clearly recognized and discriminated by participants. Although we would assume that the ability to recognize pain facial expressions and other emotion expressions, especially negative emotion expressions, should be related, in our study pain detection accuracy and the DANVA2-AF, a test of emotion recognition, were not correlated. The stimuli in the pain detection tests and DANVA2-AF were quite different. The pain detection tests used dynamic spontaneous stimuli while the DANVA2-AF used static photographs of posed emotion expressions. This difference in target stimuli could have contributed to the lack of relationship between pain detection accuracy and emotion recognition especially because posed expressions often have a greater intensity compared with spontaneous expressions. Even in our study, the exaggerated target stimuli were experiencing pain, not just faking their pain, as many studies often use posed actors.
One limitation of this research is that the experience of ischemic muscle pain induced in the laboratory may not translate to accurately understanding the experience of other types of pain in the real world. Therefore, we recommend generalizing these findings with caution.
Understanding another’s pain is a difficult and complex skill, yet a skill that has health and safety implications for the person in pain as well as for the person judging the pain. Our research suggests that empathy and experience with pain can only help one’s ability in discriminating how much pain another person is experiencing. Future research should attempt to train more empathic clinicians and caretakers and possibly even give them an experience of pain or have them remember a time when they experienced a loved one in pain to increase their accuracy at judging patients’ pain.
Footnotes
Appendix A
Acknowledgements
The authors thank Curtis Pitegoff and Matt Poon for their assistance in conducting this research. The first author thanks Carol Wilson for her past and present support, instruction, and mentorship and Herbert Ruben for his inspiration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.