
Abstract
Using a daily diary methodology, we examined how social environments support or fail to support sexual identity disclosure, and associated mental and physical health outcomes. Results showed that variability in disclosure across the diary period related to greater psychological well-being and fewer physical symptoms, suggesting potential adaptive benefits to selectively disclosing. A multilevel path model indicated that perceiving autonomy support in conversations predicted more disclosure, which in turn predicted more need satisfaction, greater well-being, and fewer physical symptoms that day. Finally, mediation analyses revealed that disclosure and need satisfaction explained why perceiving autonomy support in a conversation predicted greater well-being and fewer physical symptoms. That is, perceiving autonomy support in conversations indirectly predicted greater wellness through sexual orientation disclosure, along with feeling authentic and connected in daily interactions with others. Discussion highlights the role of supportive social contexts and everyday opportunities to disclose in affecting sexual minority mental and physical health.
Abundant evidence suggests that disclosure of one’s lesbian, gay, or bisexual (LGB) identity, or coming out, is important for developing a stable identity, coming to self-acceptance, and reducing the psychological harm caused by holding a stigma, or a socially devalued trait (e.g., Cain, 1991; Ragins, 2004). Identifying as LGB can be difficult and sometimes even dangerous, as individuals may experience prejudice, discrimination, and stigmatization from peers, coworkers, and family members, leaving them vulnerable to both acute and chronic stress (Dean et al., 2000; Mays & Cochran, 2001; Meyer, 2003). Accordingly, making decisions about disclosing sexual orientation can have important implications for a LGB person’s well-being. Given this, it is important to understand what promotes positive disclosure experiences.
To investigate this issue, we apply a self-determination theory (SDT; R. M. Ryan & Deci, 2000) framework to understand the social factors that influence everyday decisions about disclosure and the experiences that follow. Notably, coming out is not a one-time experience; rather on an everyday basis, most LGB persons must weigh the potential costs and benefits of concealing versus disclosing their sexual identity to others (Mohr & Fassinger, 2000). Thus, we use an experience-sampling design to explore how others influence these disclosure decisions, specifically by focusing on SDT’s concept of autonomy support, as well as how these decisions about being out are linked with daily psychological and physical wellness.
Decisions to Come Out
Unlike people with a visible stigma (e.g., obesity, physical disability), individuals with a concealable stigma (e.g., a nonheterosexual identity; mental illness) regularly face decisions about whether, how much, and to whom they disclose (Pachankis, 2007). Coming out as LGB is a dynamic, ongoing process as opposed to one discrete event (e.g., Bohan, 1996; Mohr & Fassinger, 2000). For example, a diary study by Beals, Peplau, and Gable (2009) found that, on average, lesbian and gay participants explicitly considered disclosing their sexual orientation to others 3 times over a 2-week period.
Moreover, LGB individuals are selective in how much and to whom they disclose their sexual identity. For example, 51% of LGB individuals are not out to most people at work (Human Rights Campaign, 2010). Similarly, D’Augelli (2006) found that only 23% of youth were out to everyone in their life. As these findings suggest, coming out or being out is not all-or-nothing—outness, or one’s degree of openness regarding sexual orientation, often varies with different people in one’s life (Mohr & Fassinger, 2000).
Decisions about disclosing a concealable stigma can be stressful and affect well-being. Frable, Platt, and Hoey (1998) found that individuals with concealable stigmas reported lower day-to-day social confidence and self-esteem, and greater anxiety and depression than those with a visible stigma or no stigma. This may be because deciding to disclose a stigmatized identity can mean choosing between two undesirable outcomes: risking rejection, or concealing an important part of oneself.
Risks of Coming Out
Negative attitudes or intolerance toward LGB individuals can make disclosure a risky task, keeping many people “in the closet.” For example, sexual prejudice can exist in workplaces, motivating LGB individuals to keep their sexual identity concealed. Indeed, 58% of LGB individuals reported hearing derogatory comments from coworkers (Human Rights Campaign, 2010). D’Augelli (2006) found 38% of LGB youth feared being verbally attacked, and 28% feared physical assault at school. In addition, 81% reported experiencing verbal harassment, 38% reported physical threats, and 15% reported physical assaults.
Even with close others, the threat of rejection can keep individuals from disclosing their LGB identity. D’Augelli (2002) found that approximately one quarter of mothers and one third of fathers reacted to their child’s disclosure with intolerance or nonacceptance. In their sample, 39% reported losing a friend because of their sexual orientation, which also emerged as a risk factor for suicide attempts and worse mental health. D’Augelli, Hershberger, and Pilkington (1998) found that LGB youth who had come out to family experienced more verbal and physical abuse, and were more suicidal than those youth who concealed their sexual orientation. Such consequences make it clear why some choose to conceal their LGB identity.
Reasons to Come Out
Given these risks, why would LGB individuals choose to come out at all? The consensus across literatures is that although concealment may be effective at helping avoid the risks of disclosure, it can be costly to mental and physical health (see Pennebaker & Chung, 2011). Concealment of sexual orientation has been found to predict greater depression and anxiety (e.g., Schrimshaw, Siegel, Downing, & Parsons, 2013; Ullrich, Lutgendorf, & Stapleton, 2003), more smoking (Pachankis, Westmaas, & Dougherty, 2011), and more rapid HIV disease progression (Cole, Kemeny, Taylor, & Visscher, 1996; Ullrich et al., 2003). Experimental studies (Critcher & Ferguson, 2014) found that those who had to conceal their sexual orientation showed performance decrements on cognitive and physical tasks compared with those who did not conceal, illustrating that concealment taxes cognitive and self-regulatory resources (Baumeister, Vohs, & Tice, 2007; Quinn, 2006). In addition, concealment affects relationship quality and social support (Uysal, Lin, Knee, & Bush, 2012), particularly with the LGB community, which is an important source of support for LGB individuals that can help buffer psychological distress (Meyer, 2003; Pachankis, 2007). In short, concealing prevents people from reaping the intrapersonal and interpersonal benefits of freely being oneself.
These pitfalls of concealment suggest, conversely, many of the benefits of coming out—improving mental and physical well-being, freeing up cognitive and emotional resources, and bringing more closeness and connectedness into relationships. More than just avoiding the costs of concealment, coming out can facilitate self-acceptance, and ameliorate some of the distress caused by stigma (e.g., Cain, 1991; Ragins, 2004). Indeed, at the daily level, LGB individuals experienced greater well-being on days they disclosed their sexual orientation (Beals et al., 2009). Coming out enables people to more fully be themselves with others, as well as to incorporate their sexual identity with other aspects of themselves (Meyer, 2003). This is important insofar as integration of one’s experiences and identities has long been seen as important for health and wellness (e.g., Rogers, 1961; Weinstein, Deci, & Ryan, 2011).
Outcomes of Disclosure Depend on Reactions from Others
Increasingly, research has shown that a confidant’s reaction largely determines people’s experiences following a sensitive disclosure (Chaudoir & Fisher, 2010; Rodriguez & Kelly, 2006). For example, women who disclosed that they had an abortion to close but nonsupportive others (e.g., family member, friend) felt more depressed and coped with the abortion in less effective ways compared with those who told supportive others or those who did not disclose at all (Major & Gramzow, 1999). Adolescents disclosing an LGB identity to parents and caregivers who reacted with acceptance reported lower depression, fewer suicide attempts, less drug use, and less sexual risk–taking behaviors (C. Ryan, Huebner, Diaz, & Sanchez, 2009; C. Ryan, Russell, Huebner, Diaz, & Sanchez, 2010) as compared with adolescents who had parents and caregivers with rejecting responses to disclosure. Reactions from important people may have more of an impact on wellness than the act of disclosing itself. For example, D’Augelli (2002) found that parents’ reactions to their children’s LGB identity disclosure were predictive of youth’s mental health symptoms, whereas the disclosure itself had less impact, even after controlling for quality of the parent–child relationship.
Although studies have looked at antecedents of disclosure, as well as outcomes of disclosure, little empirical research has looked at these two processes together (Chaudoir & Fisher, 2010). This work aims to fill that gap. Given that the consequences of disclosure for an LGB individual largely depend on the reactions of the confidants, it seems plausible that they look for cues of threat or support to predict when disclosure will result in benefits versus harm. To understand how relationships can make people feel more or less safe to disclose, we focus on the SDT concept of autonomy support, or acceptance and support for being oneself (Lynch, La Guardia, & Ryan, 2009).
Autonomy Support and Being Oneself
According to SDT, people have basic psychological needs for autonomy, competence, and relatedness. Satisfaction of these needs promotes people’s natural propensity toward psychological growth and wellness, whereas having these needs thwarted contributes to ill-being and psychopathology (R. M. Ryan, Deci, Grolnick, & La Guardia, 2006). The need for autonomy refers to the extent that people are behaving in accord with their beliefs and feelings, and being themselves. The opposite of autonomy is feeling controlled, or a sense of pressure to act in certain ways. Acting autonomously is associated with a number of positive outcomes such as better mental health (e.g., R. M. Ryan et al., 2006), physical health (e.g., Williams, Grow, Freedman, Ryan, & Deci, 1996), and better relationships (Patrick, Knee, Canevello, & Lonsbary, 2007).
When people feel support for autonomy, they feel accepted for who they are. Autonomy support helps people to behave in ways that are consistent with their beliefs and interests and express themselves authentically (La Guardia & Ryan, 2007; Lynch et al., 2009). Indeed, autonomy support aids integration and congruence within individuals (R. M. Ryan, 1995; R. M. Ryan & Deci, 2000). For example, Weinstein and colleagues (2011) found that contextual support for autonomy helped people to integrate positive and negative memories or events into their self-concept, even the ones they judged as shameful, which had benefits to well-being.
Perceiving someone as controlling might lead an individual to conceal a stigmatized identity rather than risk rejection or negative judgments. One common form of control is conditional regard, or conveying that one is only loveable under certain conditions (Roth, Assor, Niemiec, Ryan, & Deci, 2009). LGB individuals have an identity that may be regarded as unacceptable or unlovable, potentially making it feel less safe to be oneself with conditionally regarding others.
Autonomy and Disclosure
Autonomy has been theoretically and empirically linked to disclosure as both antecedent and outcome. People are more likely to present different aspects of their personality with autonomy-supportive others (Lynch et al., 2009). Directly related to the present work, Legate, Ryan, and Weinstein (2012) found that autonomy support was a robust predictor of coming out as LGB across varied relationship contexts. Importantly, the benefits of coming out were limited to autonomy-supportive contexts, whereas benefits to wellness from disclosing were absent in controlling contexts.
Uysal and colleagues (Uysal, Lin, and Knee, 2010; Uysal et al., 2012) found that self-disclosure enhanced personal and relationship well-being because it satisfied basic psychological needs for autonomy, relatedness, and competence, whereas concealment led to worse relationship well-being because it thwarted these psychological needs. Closely related to this research, Beals and colleagues’ (2009) experience-sampling study found that gay and lesbian individuals experienced greater well-being on days when they disclosed versus concealed their sexual identity, in part because they felt supported and understood—what SDT would conceptualize as satisfying psychological needs for autonomy and relatedness. This research builds off of work by Beals and colleagues (2009) and Legate and colleagues (2012) by examining day-to-day fluctuations in disclosure and psychological well-being and for the first time explores day-to-day fluctuations in physical symptoms based on environmental support and decisions about disclosure.
The Current Research
Our aim in the present research was to understand the social conditions surrounding disclosure experiences within daily interactions, testing the link between disclosure and physical health in addition to psychological well-being, and addressing the question of why disclosing relates to wellness. First, we set out to replicate a cross-sectional finding from Legate et al. (2012) using an experience-sampling methodology—that it is not harmful to people’s well-being to vary in how out they are across their relationships. This null hypothesis was a basic premise of the research: People will naturally vary in their disclosure according to the support provided by the social environment. Building on that premise, we further tested the hypothesized path model depicted in Figure 1. Specifically, we posited a multilevel mediation model in which people will vary in how out they are across their daily interactions based on the autonomy support they perceive (Path a1), with higher levels of autonomy support in a conversation predicting higher levels of disclosure in that conversation. In turn, we predicted that higher disclosure would predict greater need satisfaction (Path b), which in turn would predict greater well-being (Path c1) and fewer physical symptoms (Path c2). That is, we expected that autonomy support would have an indirect effect on well-being and physical symptoms through disclosure (first mediator) and need satisfaction (second mediator). In addition, given the strong links between autonomy support and need satisfaction in previous studies (e.g., Adie, Duda, & Ntoumanis, 2011; R. M. Ryan & Deci, 2000), we hypothesized that interacting with autonomy-supportive people would also directly predict greater need satisfaction (Path a2), and in turn greater psychological well-being (Path c1) and fewer physical symptoms (Path c2). Although we intended to test these indirect effects at both the within- and between-person levels using multilevel modeling, we expected these indirect effects to operate primarily at the level of interactions—the within-person level.
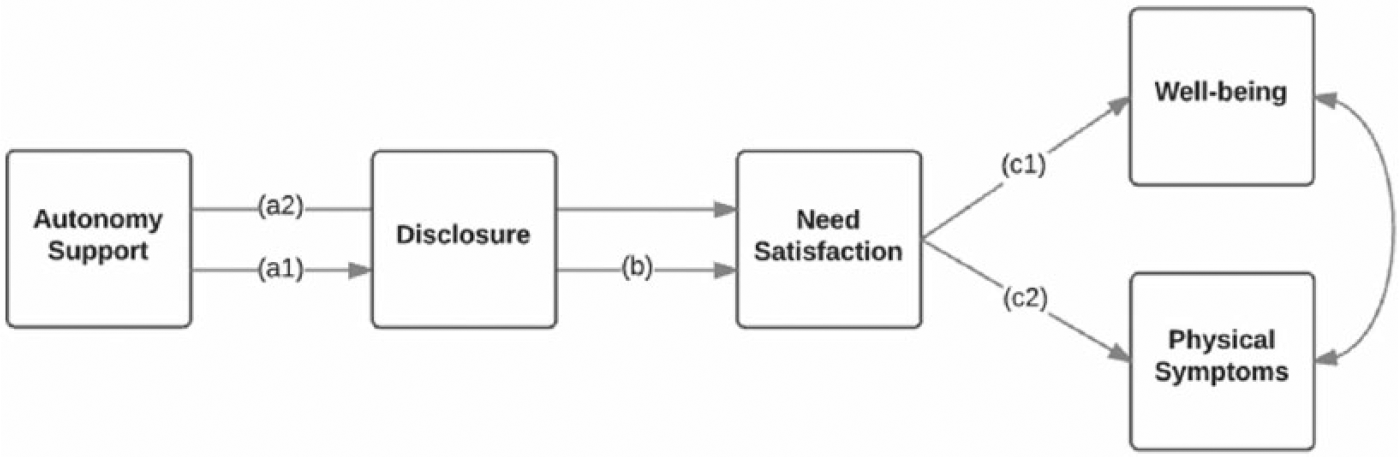
Hypothesized multilevel path model tested at both within- and between-person levels.
Method
Participants
Participants were recruited through emails sent to local LGB university organizations and fliers posted in local businesses and community centers. Requirements to participate were being above age 18; identifying as gay, lesbian, or bisexual; and owning a smartphone (to access surveys over the diary period). There were 71 respondents (34 female, 36 male, and one transgender male). Of these, 45% identified as gay, 21% as lesbian, and 34% as bisexual (bisexuals were 83% female). Ages ranged from 18 to 51 years (M = 23.5 years, standard deviation [SD] = 6.9 years). The majority (77.5%) were Caucasian (14.1% Hispanic, 4.2% Asian/Pacific Islander, and 4.2% Other/Multiracial). Individuals were reimbursed US$50 to encourage compliance given the participant burden (Bolger, Davis, & Rafaeli, 2003). Before study recruitment, the sample size was estimated for between-person effects, which are more important to establish than lower levels in the model (i.e., within-person effects; Snijders, 2005). We used G*Power (Faul, Erdfelder, Lang, & Buchner, 2007) and effect sizes in Legate et al. (2012) ranging from r = .23 to .67 with alphas set at .05 and power set at .95. This revealed a minimum sample of 60 participants. 1
Procedure
During an initial session, procedures for the 2-week period were explained. Most initial sessions were conducted individually, but four were conducted in small groups of two to three. Participants were instructed that text messages would randomly alert them 3 times per day on their smartphones (randomized within each of the three 2-hr intervals), prompting them to complete a short survey. During this initial session, participants also completed a baseline survey containing demographic questions, assessments of mental and physical health, and three baseline measures that were not used in our analyses (general levels of being out, autonomy support from important people in one’s life, and general feelings of need satisfaction).
Researchers set up a unique survey link on each participant’s phone through which they would report on the most recent personal interaction they had, or, if no new conversation had occurred since taking the last survey, to report on the next interaction that happened. A “personal interaction” was described as one lasting at least 3 min—with anyone except for romantic partners—in which personal matters were discussed. Even casual exchanges qualified as personal conversations if they involved a question such as “what did you do over the weekend?” as did more intimate conversations. Participants were instructed not to report on conversations involving only work matters or exchanges of information that were completely impersonal as we wanted to maximize the likelihood that sexual orientation would be a relevant topic to bring up in conversation. Furthermore, they were told that relevant interactions may or may not include explicitly discussing or signaling sexual orientation, and examples of indirect ways this could happen were provided (e.g., referencing one’s partner, inhibiting expression of certain interests or gestures). Finally, we told participants that whenever interacting with more than one person (e.g., a group of coworkers), to think about the overall experience with the group when answering questions.
Diary data from two participants were not recorded due to a malfunction on the survey website. Of the total 2,098 interactions from the remaining participants (N = 69), 39 (1.9%) were excluded because they lasted less than 3 min. On average, participants reported on 30 interactions (about two per day) over the 2 weeks (SD = 10.5; range = 2-46). The overwhelming majority of the sample completed at least one survey per day, with only five participants (7%) completing fewer than 14 surveys total. The average interaction lasted 30 min, though the median was 20 min. This discrepancy between mean and median resulted because of a small number of interactions lasting 3 or more hours (n = 37; 1.7% of all interactions), inflating the mean.
Baseline measures
Psychological well-being
Psychological well-being scores were derived from four well-validated instruments used in Legate et al. (2012). Risk for depression was assessed with three items from the Center for Epidemiological Studies–Depression Scale (CES-D; Radloff, 1977): sad, depressed, and lonely. Self-esteem was measured with three items from the Rosenberg Self-Esteem Scale (Rosenberg, 1965) satisfied with myself, feel useless (reverse coded), and have a positive attitude toward myself. Three items assessing anger were adapted from the State-Trait Anger Scale (Spielberger, Jacobs, Russell, & Crane, 1983) mad or irritated, angry, and hostile. Finally, three anxiety items from the General Health Questionnaire (Goldberg & Hillier, 1979) were used: scared or panicky, edgy or anxious, and nervous and uptight. Participants were asked to rate their feelings over the last month on a 5-point scale from not at all true to very true. Subscales demonstrated good internal consistency (Depressive Feelings α = .85, Self-Esteem α = .87, Anger α = .84, Anxiety α = .84), as did the composite of subscales (α = .91).
Physical symptoms
Baseline physical symptoms were measured through the Patient Health Questionnaire (PHQ-15; Kroenke, Spitzer, & Williams, 2002). The PHQ-15 is a brief questionnaire with three cutoff points indicating low, medium, and high symptom severity (scores of 5, 10, and 15, respectively). Participants indicated the degree to which they have been bothered by different physical symptoms (e.g., stomach pain, headaches) over the past 4 weeks on a 1 (not bothered at all) to 3 (bothered a lot) scale (α = .88).
Diary measures
Highly abbreviated measures were used for diary assessments.
Autonomy support
We selected and adapted two top-loading items from the Autonomy Support Questionnaire (Deci, La Guardia, Moller, Scheiner, & Ryan, 2006) to assess perceived autonomy support from interaction partners for the brief diary assessments (“I feel he/she tried to understand how I see things in the interaction” and “He/she listened to my thoughts and ideas in the interaction”), and rated on a 1 (strongly disagree) to 4 (strongly agree) scale. Multilevel reliability estimates for the two items were calculated (Geldhof, Preacher, & Zyphur, 2014) showing good reliability at the within-person level (α = .87) and excellent reliability at the between-person level (α = .97).
Disclosure
Because sexual orientation is not always relevant to people’s conversations, participants were instructed that these four items assessed disclosure along with the internal experience of feeling comfortable discussing it should the topic arise (vs. constrained or inhibited). One item, “I felt open and comfortable about my sexual identity with this person” assessed participants’ level of comfort with disclosing sexual identity during each interaction on a 1 (strongly disagree) to 4 (strongly agree) scale. A second item assessed explicit disclosure with the question, “How out were you in this conversation?” rated on a scale from 1 (definitely concealed) to 4 (definitely out). In addition, two items from the Self-Concealment Scale (Larson & Chastain, 1990) were modified to assess how much the participant concealed sexual identity during each interaction: “There are lots of things associated with my sexual identity that I kept from this person” and “I was afraid I’d reveal something about my sexual identity to him/her that I didn’t want to,” rated on a 1 (strongly disagree) to 4 (strongly agree) scale. Concealment items were reversed, and the four items were combined into an aggregate disclosure variable, which showed good reliability within persons (α = .86) and between persons (α = .93).
Need satisfaction and thwarting
Need satisfaction/thwarting experienced during each interaction was assessed with items modified from the Basic Need Satisfaction in Relationships Scale (La Guardia, Ryan, Couchman, & Deci, 2000) and the Psychological Need Thwarting Scale (Bartholomew, Ntoumanis, Ryan, Bosch, & Thøgersen-Ntoumani, 2011). One item measured autonomy satisfaction (“In the interaction I was able to be myself”) and autonomy thwarting (“In the interaction I felt pushed to behave in certain ways”). Similarly, one item measured relatedness satisfaction (“In the interaction I felt understood and supported”) and relatedness thwarting (“In the interaction I felt rejected”). Items were rated on a 1 (strongly disagree) to 4 (strongly agree) scale. Need thwarting items were reverse coded and combined with need satisfaction items into a composite that showed good within-person (α = .79) and between-person (α = .91) reliabilities.
Psychological well-being
Two items from each well-being construct used in the initial session were used to assess state well-being following each interaction. Participants rated how they were feeling “right now” on a scale ranging from 1 (not at all true) to 4 (very true). Two items (sad, depressed) were averaged to create a composite of depressive feelings, as well as for self-esteem (satisfied with myself, feel useless, reverse coded), anxiety (anxious, calm, reverse coded), and anger (mad or irritated, angry). All four constructs were combined into one aggregate well-being variable that showed good reliability: αwithin = .80, αbetween = .91.
Physical symptoms
Momentary physical symptoms were assessed using the PHQ-15. Participants indicated whether they were experiencing any of 15 symptoms (e.g., stomach pain, headaches) “right now,” assessed dichotomously (i.e., yes/no) with total number of symptoms being the outcome of interest.
Conversation length
Finally, conversation length was assessed, and participants also specified the relationship type (e.g., mom) and the individual’s initials for each interaction. All of our materials, procedures, and data are publicly available on the study’s project page (osf.io/kq6st).
Results
Preliminary Analyses
Descriptive statistics and intercorrelations for primary study variables are presented in Table 1. ANOVAs examined for sexual orientation differences across study variables. Results showed that across the diary period, bisexuals perceived less autonomy support, disclosed their sexual orientation less, felt less need satisfaction, and reported more physical symptoms, F(2, 68) = 3.62-7.76, ps = .001-.03, as compared with lesbians and gay men (who did not differ). Across the 2-week period, perceived autonomy support, levels of disclosure, and need satisfaction differed across relationship type, F(11, 1995) = 32.42-35.50, ps < .001. Close friends provided the most autonomy support of any targets (ps < .001), and participants were most out (ps < .001), and felt the most autonomy and relatedness in interactions with them (ps < .001). Related, people overwhelmingly interacted with close friends more than any of the other 11 targets (see Figure 2). Because of the many differences across sexual orientation and relationship types, we included these variables as controls in multilevel analyses.
Means, Standard Deviations, and Correlations of Study Variables at the Between-Person Level.
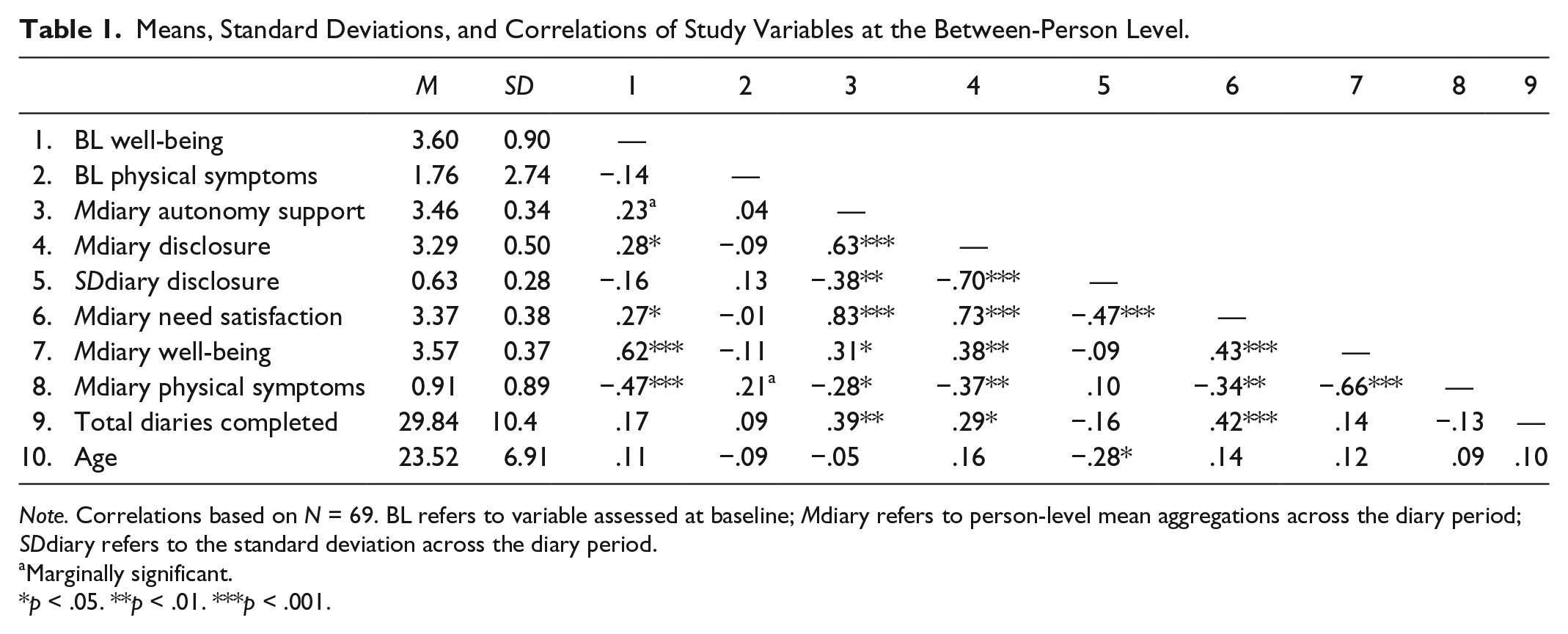
Note. Correlations based on N = 69. BL refers to variable assessed at baseline; Mdiary refers to person-level mean aggregations across the diary period; SDdiary refers to the standard deviation across the diary period.
Marginally significant.
p < .05. **p < .01. ***p < .001.
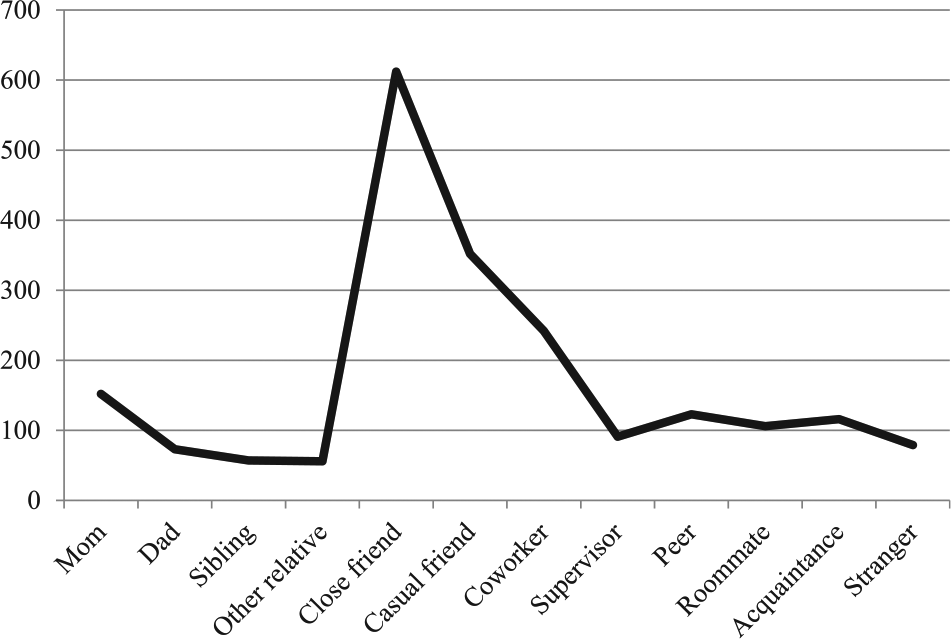
Number of interactions with each target across 2 weeks.
To examine our first hypothesis—that variability in disclosure across interactions would be unrelated to mental and physical wellness—means and SDs of disclosure were computed for each person across the 14-day period. Ordinary least squares regressions were used to regress psychological well-being and physical symptoms (aggregated over the 14-day period) onto SD scores for disclosure, controlling for mean levels of disclosure and sexual orientation (dummy coded). Surprisingly, we found that more variability in disclosure across the diary period (M = .63, SD = .28) was related to greater well-being, β = .36, t(66) = 2.32, p = .02, and fewer physical symptoms, β = −.35, t(66) = −2.25, p = .03, after controlling for average levels of disclosure (well-being: β = .61, t[66] = 3.79, p < .001; physical symptoms: β = −.53, t[66] = −3.35, p = .001). Therefore, more variability in disclosure after controlling for average levels of disclosure was related to greater wellness outcomes.
Multilevel Modeling
Mplus software (Version 7.4; Muthén & Muthén, 1998-2014) was used to test the hypothesized multilevel path model (Figure 1). In multilevel structural equation modeling (SEM), variance is divided into within-person and between-person components, which allows us to see how much variance is explained at the conversation level (Level 1) as well as at the mean level across the diary period (Level 2). This modeling approach allowed us to simultaneously test the proposed multistep mediation hypotheses at both Levels 1 and 2 (see Preacher, Zyphur, & Zhang, 2010). Multilevel models not only accommodate the nested structure of the data, but they are also better suited than ordinary least squares regression to handle missing data (Bolger & Shrout, 2007; Little & Rubin, 1987). Expectably, a source of missing data was the number of diary surveys provided—63 participants (93%) reported on one or more personal interactions each day, 43 participants (63%) reported on two or more personal interactions each day, and 11 participants (16%) reported the maximum of three personal interactions each day. As suggested by Preacher and colleagues (2010), we examined intraclass correlation coefficients to determine the variance explained at the between-person level (.25-.42), verifying that there was enough variance for models at both between- and within-person levels.
Level 1 effects
Within specific diary assessments following social interactions, we built a model directly corresponding to our conceptual model (see Figure 1). Thus, autonomy support was allowed to predict both disclosure and need satisfaction, disclosure predicted need satisfaction, and need satisfaction predicted both well-being and physical symptoms. To control for the stability of the two outcome variables (well-being and physical symptoms) across conversations, we included levels of those variables from the previous assessment as predictors at Level 1 (modeling autoregressive paths for the outcomes). As the time intervals between assessments varied, we also included a variable coding time (in hours) between assessments as a predictor and allowed that variable to moderate the autoregressive paths (expecting those paths to be weaker for longer intervals between assessments; for example, Reis, Sheldon, Gable, Roscoe, & Ryan, 2000). In other words, an individual’s well-being score from their second diary occurrence was predicted by their well-being score on their first diary occurrence, the time between the first and second assessments, and the interaction between the first well-being assessment and time.
To control for potential differences across relationship types, we included dummy variables at Level 1 representing three relationship types—close friends, family (that combined mom, dad, sibling, and other relative), and stranger (that combined strangers and acquaintances) as these three dummy-coded relationships account for 55% of all conversations. We specifically selected family and close friends to see the effects of close relationships, and to examine how the model held across even the most distant relationship type, we selected strangers and acquaintances. In each of these variables, the interactions with the targeted relationship type were coded 1, and all others were coded as 0. Thus, by including those three dummy variables at Level 1, highly close and highly distant relationships were compared with all other relationship types (which can be considered to have intermediate levels of closeness, for example, coworkers, casual friends, roommates). We modeled these as main effects, and also tested for potential moderations with autonomy support when predicting disclosure and need satisfaction. This examined whether the effect of autonomy support on disclosure and need satisfaction was stronger for certain relationships—directly testing that moderation through the included interaction terms.
Level 2 effects
Following recommendations for testing multilevel mediation (Preacher et al., 2010) in addition to testing our conceptual meditational model at Level 1, we also tested the same meditational associations at Level 2 to examine whether average levels of each of the constructs in the model (Figure 1) would show a comparable pattern of mediation. As past research shows bisexuals are at higher risk of psychological distress (e.g., Semlyen, King, Varney, Hagger, & Johnson, 2016) and our own data revealed that bisexuals differed from lesbians and gay men on many variables, we included dichotomous variables at Level 2 coding sexual orientation using bisexuals as the reference group (i.e., separately coding gay and lesbian respondents) allowing those variables to predict endogenous variables. As the number of diaries completed varied widely across participants, we also included the total number of diaries the participant completed (grand-mean centered) as a Level 2 predictor of endogenous variables. In addition, baseline levels of well-being predicted average well-being, and baseline physical symptoms predicted average physical symptoms across the diary period (both baseline variables were grand-mean centered). Dichotomous variables coding sexual orientation (at Level 2) and relationship type (at Level 1) were entered uncentered. As the main variables of interest were modeled at both the within- and between-person levels, they were entered uncentered per the recommendations of Preacher and colleagues (2010). To focus the tests of our mediation hypotheses on patterns of results across all participants, the conversation-level effects (i.e., Level 1) were set as fixed. For all multilevel results, unstandardized regression coefficients and their 95% confidence intervals (CIs) are presented in the text and in Table 2.
Multilevel Mediation Model Coefficients.
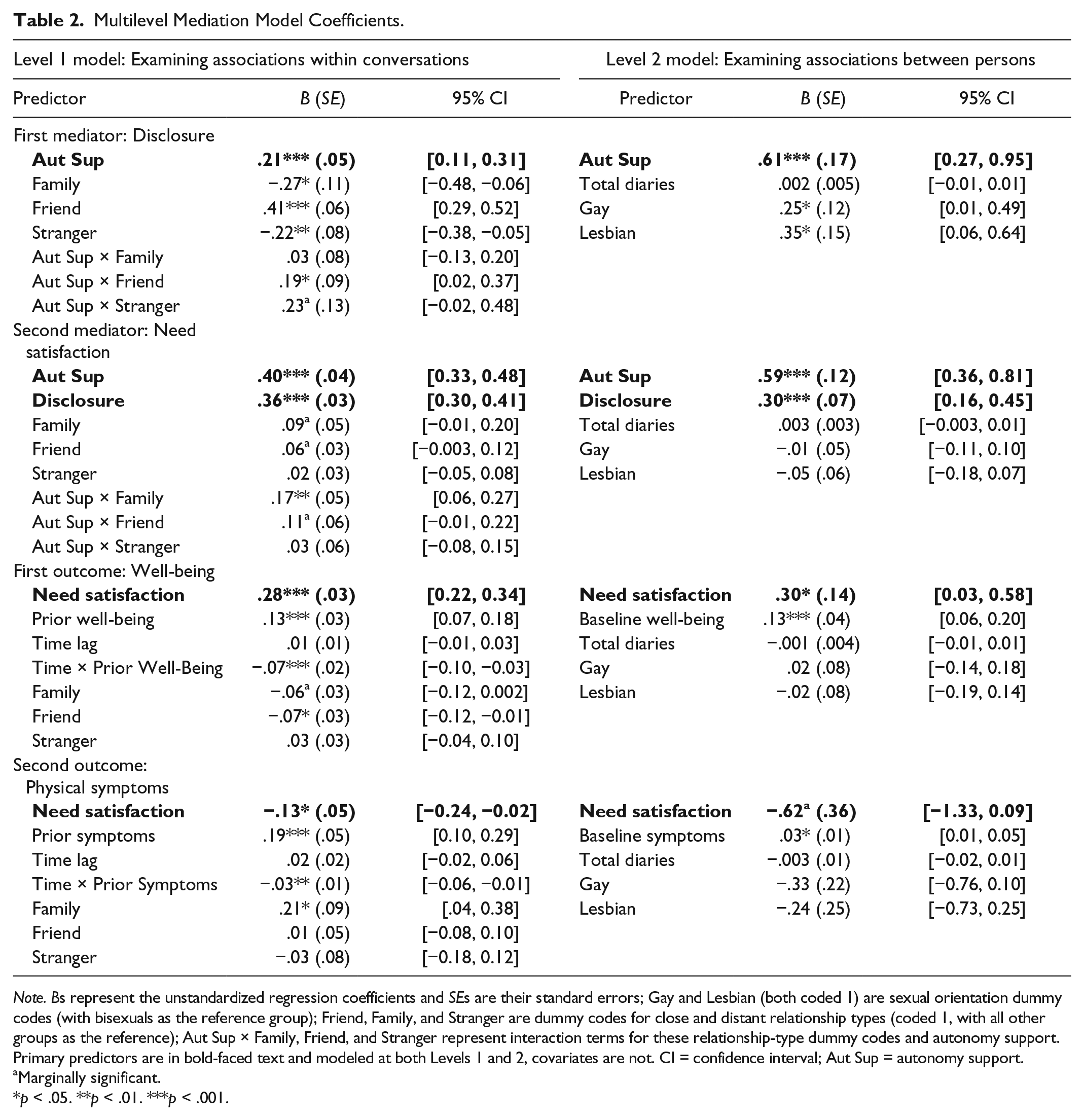
Note. Bs represent the unstandardized regression coefficients and SEs are their standard errors; Gay and Lesbian (both coded 1) are sexual orientation dummy codes (with bisexuals as the reference group); Friend, Family, and Stranger are dummy codes for close and distant relationship types (coded 1, with all other groups as the reference); Aut Sup × Family, Friend, and Stranger represent interaction terms for these relationship-type dummy codes and autonomy support. Primary predictors are in bold-faced text and modeled at both Levels 1 and 2, covariates are not. CI = confidence interval; Aut Sup = autonomy support.
Marginally significant.
p < .05. **p < .01. ***p < .001.
Model fit
To evaluate model fit, we followed recommendations by Kline (2005) and Marsh, Hau, and Wen (2004): a comparative fit index (CFI) and Tucker–Lewis index (TLI) above .95, and the root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) below .08. Using these benchmarks, our model showed good fit to the data, χ2(34, N = 69) = 50.63, p = .03, CFI = .99, TLI = .98, RMSEA = .02, SRMRwithin = .01 SRMRbetween = .07. The model also accounted for reasonably large amounts of variance in the predicted (i.e., endogenous) variables: 66% of within-person and 88% of between-person variance for disclosure, 87% within and 97% between for need satisfaction, 20% within and 61% between for physical symptoms, and 89% within and 94% between for well-being.
Predicting disclosure
The first path (a1) in our hypothesized model (Figure 1) was significant at both levels. Thus, at the individual conversation level (Level 1), perceiving autonomy support during conversations predicted more disclosure in those conversations (B = .21, SE = .05, p < .001, CI = [0.11, 0.31]). Similarly, across all conversations (Level 2), perceiving more autonomy support across the entire diary period predicted higher average levels of disclosure across all conversations (B = .61, SE = .17, p < .001, CI = [0.27, 0.95]). The main effects of relationship type suggested that people disclosed sexual orientation significantly more in conversations with close friends (B = .41, SE = .06, p < .001, CI = [0.29, 0.52]) and significantly less with family (B = −.27, SE = .11, p = .01, CI = [−0.48, −0.06]) and strangers (B = −.22, SE = .08, p = .01, CI = [−0.38, −0.05]) as compared with relationships of intermediate levels of closeness (e.g., coworkers, roommates). The interaction terms testing differences in links between autonomy support and disclosure across specific types of relationships suggested that perceiving autonomy support in conversations with close friends—and marginally, from strangers—was more strongly linked to disclosure (friends: B = .19, SE = .08, p = .03, CI = [0.02, 0.37]; strangers: B = .23, SE = .13, p = .07, CI = [−0.02, 0.48]) as both effects suggested a stronger positive association between autonomy support and disclosure for those two relationship types when compared with relationships of intermediate closeness. Thus, relationship type significantly moderated that predictive link. The number of diaries completed did not significantly predict average disclosure across conversations (p > .50) but sexual orientation did—gay men and lesbians disclosed more than bisexuals across the diary period, Bs = .25 and .35, respectively, ps < .05. 2
Predicting need satisfaction
As hypothesized, disclosing was associated with more need satisfaction in the conversation (Path b). This was true for disclosure predicting need satisfaction at the level of conversations (B = .36, SE = .03, p < .001, CI = [0.30, 0.41]) and for average levels of disclosure predicting need satisfaction across the diary period (B = .30, SE = .15, p < .001, CI = [0.03, 0.58]). People also experienced more need satisfaction with autonomy-supportive others (Path a2) at the level of individual conversations (B = .40, SE = .04, p < .001, CI = [0.33, 0.48]) and averaged across the diary period (B = .59, SE = .12, p < .001, CI = [0.36, 0.81]). Examining differences across relationship types, people marginally felt more need satisfaction in conversations with close friends (B = .06, SE = .03, p = .06, CI = [−0.003, 0.12]) and family (B = .09, SE = .05, p = .09, CI = [−0.01, 0.20]) compared with relationships of intermediate closeness. Links between autonomy support and need satisfaction varied meaningfully across relationship types: Perceiving autonomy support in conversations with family and close friends was especially linked to need satisfaction following conversations with those people (family: B = .17, SE = .05, p = .002, CI = [0.06, 0.27]; friends: B = .11, SE = .06, p = .07, CI = [−0.01, 0.22]) when compared with relationships of intermediate closeness. However, the number of diaries completed and sexual orientation did not significantly predict average need satisfaction across conversations (ps > .30).
Predicting well-being
Consistent with hypothesis, experiencing need satisfaction predicted higher well-being (Path c1). This was true for predicting well-being following each conversation (B = .28, SE = .03, p < .001, CI = [0.22, 0.34]) and for predicting average levels of well-being across the diary (B = .30, SE = .14, p = .03, CI = [0.03, 0.58]). This was true even after controlling for levels of well-being following the previous diary assessment (B = .13, SE = .03, p < .001, CI = [0.07, 0.18]), and more recent reports showed a stronger predictive link between previous and current well-being (B = −.07, SE = .02, p < .001, CI = [−0.10, −0.03]). Surprisingly, having conversations with friends and, marginally family, predicted lower well-being (friends: B = −.07, SE = .03, p = .02, CI = [−0.12, −0.01]; family: B = −.06, SE = .03, p = .06, CI = [−0.12, 0.002]) compared with relationships of intermediate closeness. At Level 2, baseline well-being predicted higher average well-being across the diary period (B = .13, SE = .04, p < .001, CI = [0.06, 0.20]). In contrast, the number of diaries completed and sexual orientation did not significantly predict average well-being across conversations (ps > .50).
Predicting physical symptoms
Experiencing need satisfaction in a conversation predicted fewer physical symptoms following that conversation (Path c2: B = −.13, SE = .05, p = .02, CI = [−0.24, −0.02]) but average levels of need satisfaction only marginally predicted fewer average symptoms across the diary period (B = −.62, SE = .36, p = .09, CI = [−1.33, 0.09]). At Level 1, symptoms reported during the prior interaction predicted more current symptoms (B = .19, SE = .05, p < .001, CI = [0.10, 0.29]), and that predictive link was especially strong when prior symptoms were reported more recently (B = −.03, SE = .01, p = .002, CI = [−0.06, −0.01]). Turning to differences across relationship types, conversations with family predicted more physical symptoms (B = .21, SE = .09, p = .02, CI = [0.04, 0.38]) compared with relationships of intermediate closeness. At Level 2, baseline physical symptoms predicted greater average symptoms across the diary period (B = .03, SE = .01, p = .01, CI = [0.01, 0.05]). In contrast, sexual orientation and total number of diaries failed to emerge as significant predictors (ps > .10, CIs pass through 0).
Indirect effects
In this same path model, we estimated all possible indirect effects at the within-person (i.e., at the level of individual conversations) and between-person (i.e., at the level of averages across all conversations) levels, which reduces Type 1 error and a potential confounding of the mediation effect (Preacher et al., 2010). We calculated 95% Monte Carlo CIs for all two- and three-path indirect effects using Tofighi and MacKinnon’s (2016) web-based utility, as this method is recommended in smaller samples and does not assume that indirect effects are normally distributed (Preacher et al., 2010). Although all within-person and some between-person indirect effects were significant (Table 3), we were most interested in the mediation paths of autonomy support predicting well-being and physical symptoms through disclosure and need satisfaction. These indirect effects were significant at the within-person level for both well-being (B = .02, SE = .006, CI = [0.01, 0.03]) and physical symptoms (B = −.01, SE = .005, CI = [−0.02, −0.002]), supporting our model at the level of individual conversations. In addition, one of the corresponding between-person indirect effects emerged as significant (well-being: B = .06, SE = .03, CI = [0.004, 0.14]) whereas the other effect was not significant (physical symptoms: B = −.11, SE = .08, CI = [−0.30, 0.02]). In sum, the reason that everyday experiences of receiving autonomy support predicted greater well-being and fewer physical symptoms was because they helped people be more out about their sexual orientation, which in turn satisfied needs for autonomy and relatedness. Average levels of disclosure and need satisfaction also helped explain the link between average levels of autonomy support and well-being across the diary period. Importantly, this mediation model seemed to operate more robustly at the level of daily interactions (as opposed to people’s mean levels of autonomy support and disclosure), suggesting that everyday opportunities to experience autonomy support and disclose have potent links to everyday mental and physical health.
Indirect Effects at the Within- and Between-Person Levels.
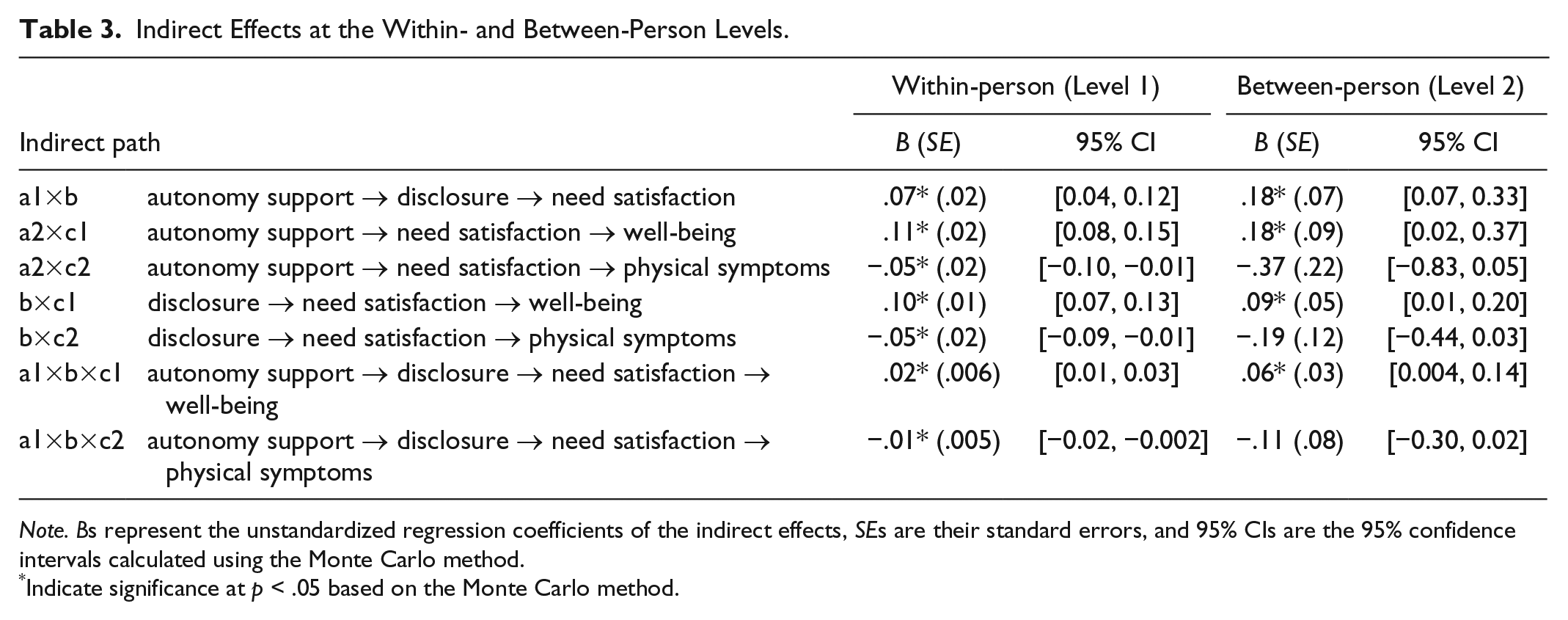
Note. Bs represent the unstandardized regression coefficients of the indirect effects, SEs are their standard errors, and 95% CIs are the 95% confidence intervals calculated using the Monte Carlo method.
Indicate significance at p < .05 based on the Monte Carlo method.
Discussion
In this study, we examined antecedents and consequences of everyday experiences of being out. Although past studies have highlighted the relations between disclosure and mental and physical health, novel to this study, we investigated factors affecting moment-to-moment decisions to disclose and their effects on mental and physical health using hypotheses derived from SDT. An experience-sampling design was used to capture experiences of coming out or being out as they occurred, limiting retrospective bias and clarifying day-to-day patterns in decisions about disclosure and their links to wellness.
Although the sample was generally out about their sexual identity, people did vary in how out they were to various targets across the 2 weeks. As expected, this variability was not harmful to wellness. Unexpected, however, was that more variability predicted greater well-being and fewer physical symptoms. Taken together, these results suggest that selectively revealing one’s sexual orientation to others does not have clear costs, and may at times yield adaptive benefits. This finding supports a basic premise of this research that even though coming out is usually a good thing for health and wellness, it is adaptive to do so selectively.
A major goal of this research was to examine how receiving autonomy support is associated with decisions about sexual identity disclosure, and how these decisions in turn are associated with daily mental and physical health. Perceptions of autonomy support during interactions indeed predicted being more out and feeling more need satisfaction in a conversation, which in turn predicted greater well-being and fewer physical symptoms. In other words, when people perceived that someone accepted them for who they are, they were more out about their sexual orientation with that person, they felt they could be themselves (autonomy) and felt closer (relatedness) to that person, and they felt better—mentally and physically—following those conversations. Importantly, these indirect paths predicting well-being and physical symptoms were consistently operating at the level of conversations, whereas these indirect paths were inconsistent at the level of averages across the diary period. This is in line with recent findings looking at first coming out experiences—when confidantes reacted positively to people’s first sexual identity disclosure, it predicted higher current levels of well-being because people experienced more autonomy need satisfaction in that relationship (W. S. Ryan, Legate, & Weinstein, 2015). Taken together, these findings suggest that each disclosure opportunity comes with the possibility of boosting need satisfaction, well-being, and buffering against physical health symptoms, and that having accepting, autonomy-supportive others in one’s life reduces barriers to disclosing.
Novel to this research is our focus on everyday physical health. Our data are consistent with research revealing the deleterious costs of concealing sexual orientation on physical health (e.g., Cole et al., 1996; Juster, Smith, Ouellet, Sindi, & Lupien, 2013), but this is the first study examining day-to-day fluctuations in physical health that correspond to day-to-day disclosure decisions and experiences of environmental support. This suggests that it is not just overall concealment or a lack of support that produces negative health outcomes, but that momentary decisions to conceal from others and feeling a lack of support correspond to expressing more physical symptoms that same day.
Limitations and Future Directions
Limitations of this research should be noted. First, study recruitment resulted in a sample that was highly “out.” Research on LGB individuals and other stigmatized populations often encounters this issue, as those more comfortable with their identity are more likely to volunteer (Corrigan et al., 2010). We suspect, in fact, that the dynamics we explored might be even stronger in a less out sample, where selectivity is likely to be even more salient. In addition, although effects were tested at the level of daily interactions, diary data are still fundamentally correlational and cannot directly speak to causality. It is possible, for example, that disclosing sexual orientation in a conversation drives perceptions of the confidante as more accepting. If this were the case, people would not be selectively disclosing based on autonomy support perceived during their interactions with others, but instead, an individual difference characteristic or some other property of interactions would be driving the disclosure and experiences that follow. Both experimental and longitudinal methods would allow for causal statements about the role of autonomy support in coming out, and represent crucial future directions of this research.
Finally, our brief diary assessment does not assess all aspects of autonomy support—these top-loading items from our longer measure of autonomy support mainly captured an active interest in and respect for the other’s perspective. Although these are indeed core elements of autonomy support (R. M. Ryan et al., 2006), and are reliable indicators of that larger construct, they do not, by themselves, directly tap all facets of the construct. Teasing apart different aspects of autonomy support and their respective contribution to disclosure and wellness outcomes thus represents an important direction of future experimental and experience-sampling research. In addition, the current results also have implications for researchers interested in acceptance and empathy, as these results also support the importance of these specific facets of autonomy support for LGB disclosure decisions and wellness.
We observed strong links in our model at both the within- and between-person levels, indicating the value of receiving autonomy support and disclosure in each conversation in one’s life, as well as the additive value of those experiences. Just as autonomy support from each conversation as well as the aggregated autonomy support across the diary period uniquely predicted disclosure and need satisfaction, it is also very likely that the global autonomy support from specific interaction partners plays a role as well. Teasing apart the variance from different sources—autonomy support in each conversation, the general autonomy supportiveness of people one interacts with, and the total amount of autonomy support from all people in one’s life—represents an important step for future research in this area.
Despite its limitations, this work addresses several gaps in the literature. This diary methodology elucidated patterns in sexual orientation disclosure at the level of interactions, showing that autonomy support predicts disclosure, which in turn predicts shifts in mental and physical health because of need satisfaction. Importantly, this work is the first to date to examine how disclosure decisions relate to physical health on a daily basis, extending the coming out literature and contributing to a better understanding of health disparities faced by sexual minorities (Mustanski, Birkett, Greene, Hatzenbuehler, & Newcomb, 2014).
Implications
These findings elucidate how family members, coworkers, friends, and others can affect LGB individuals’ mental and physical health on a day-to-day basis. Identifying ways that social interactions support LGB health represents an essential step in closing the health disparities gap faced by sexual minorities. Furthermore, this work is relevant to building interventions within social support systems such as families, workplaces, and schools. For example, the Family Acceptance Project (C. Ryan et al., 2009) is an intervention that provides education to families about the importance of accepting their lesbian, gay, bisexual, and transgender (LGBT) children (and the costs of rejecting them), not just after they come out but well before that. These findings also suggest the potential value of implementing similar interventions in other contexts such as workplaces and schools, especially benefiting LGB youth and adults as they navigate the coming out process. This research also has implications for clinicians working with LGB youth and adults, suggesting that it could be beneficial for clinicians to help LGB clients consider and cope with potential costs of coming out to people who may be judgmental or rejecting.
Finally, this work has implications for other groups with a concealable stigma such as transgender individuals and individuals with mental illness, as similar processes may operate for other sensitive disclosures. Indeed, programs like Coming Out Proud (Corrigan et al., 2010) have been implemented to empower those with a mental illness to disclose their experiences with mental illness with the aim of reducing the negative effects of stigma. Notably, the first module in the program has participants consider the costs and benefits of disclosure, demonstrating that disclosure is a selective process. The current data suggest that finding autonomy-supportive others can contribute to the health and wellness of all individuals who face stigma, allowing them to be who they are in everyday social interactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The online supplemental material is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.