
Abstract
People sometimes perceive social environments as unpleasantly crowded. Previous work has linked these experiences to incidental factors such as being hungry or hot and to the relevance of the social environment for an individual’s current goals. Here, we demonstrate that crowding perceptions and evaluations also depend on specific, active threats for perceivers. Eight studies test whether infectious disease threats, which are associated with crowded conditions, increase such reactions. Across studies, pathogen threat made dense social environments seem more crowded and generated more negative affect toward these environments. These perceptions and negative feelings were more influenced by pathogen threat relative to other threats of physical danger. Finally, reactions to pathogen threat affected people’s choice of crowded versus uncrowded environments to inhabit. This research suggests that interpretations of social environments depend on the unique threats and opportunities those environments afford to individuals.
Think of the last time you were taking a subway during rush hour, shopping in a mall during holiday season, or going dancing in a club on a Saturday night. What do these situations have in common? They are all everyday experiences in which people congregate in large groups, or crowd together. Now imagine that you happened to find yourself in one of these places during a bad flu season or following a terrorist attack. Would your perceptions of how crowded this situation is change, and if so, why? In five studies, we investigate the psychological experience of crowding by identifying how social perceptions are influenced by environmental threats, in particular the threat of infectious disease.
Psychological States of Crowding
The psychology of human crowding first received widespread empirical attention in the 1970s, following the rise of environmental psychology or the study of the interplay between human behavior and the environment (see Oishi & Graham, 2010, for a brief history). By the 1990s, however, research on social density, and environmental psychology more generally, had waned. Today, research examining socioecological and environmental influences on human behavior has breathed new life into this and related topics (e.g., Gelfand et al., 2011; Sng, Neuberg, Varnum, & Kenrick, 2017).
Although recent studies like these have investigated objective environmental qualities related to crowding such as population and spatial density, perceptions of crowding are inherently subjective in nature. Crowding is commonly defined as a state of psychological stress resulting from a high ratio of people to amount of space in the surrounding environment (Altman, 1975; Stockdale, 1978; Stokols, 1972). Whereas density involves a direct judgment of the relationship between the number of people and the surrounding physical space, crowding involves a subjective affective response (Rapoport, 1975; Stokols, 1972) as a function of attributions of arousal to social density. For instance, people exposed to a dense environment who attributed their arousal to an annoying noise or a painting experienced less crowding and negative downstream consequences of crowding (Worchel & Teddie, 1976; Worchel & Yohai, 1979). As long as density is made a salient cue, even arousal generated by unrelated factors can produce crowding experiences (Gochman & Keating, 1980). Emphasizing its connection to subjective experience, crowding has historically included dimensions such as confinement (decreases in spatial freedom inhibiting the feeling of goal achievement; Harrell & Hurt, 1976; though see Machleit, Kellaris, & Eroglu, 1994).
Crowding produces a range of negative outcomes, including increased discomfort and withdrawal from social interactions (Baum & Valins, 1979), heightened competition and aggression (Stokols, Rall, Pinner, & Schopler, 1973), interpersonal hostility (Griffit & Veitch, 1971), and reduced shopper satisfaction (Machleit et al., 1994). In one recent study, for example, exposure to crowded images was enough to activate self-protective motivations that decreased risk-taking and increased prevention-focus orientation (Maeng, Tanner, & Soman, 2013).
Given the potential impact of such adverse outcomes, researchers have cast a broad net in exploring predictors of crowding experiences well beyond straightforward increases in social density. Some early work showed that crowding perceptions are affected by features incidental to the experience, such as high ambient temperatures (Griffit & Veitch, 1971) or momentary hunger and arousal (Stokols, 1972). However, most research has focused on features central to social interaction. This work shows that crowding is elevated by group-specific factors, such as the composition of the social environment (e.g., in-group vs. out-group members; Novelli, Drury, Reicher, & Stott, 2013) and person-specific factors, such as current motivations. Active goals can boost perceptions of crowding when those goals conflict with aspects of the social setting (Cozby, 1973). For instance, a person at a party may enjoy interactions with many others, but be uncomfortable with the distractions caused by the same number of people while studying. A crowded dance club may be exciting and fun whereas a crowded subway may be distressing. Similarly, expectations guide reactions to crowds. Accordingly, shoppers express more satisfaction when their expectations of store crowdedness are met than when crowdedness exceeds their expectations (Machleit, Eroglu, & Mantel, 2000).
Existing work on crowding has thus focused on features of the person and the situation inherent to experiences within dense social environments. Research considering incidental influences has been limited to general states like annoyance (e.g., hunger, warmth). Yet, crowds afford additional threats and opportunities to individuals, ones that exist because other people can act as agents (even unwitting ones) of harm and safety. Here, we argue that incidental cues of infectious disease are especially likely to shift appraisals of dense social situations toward threat, resulting in elevated perceptions of these situations as crowded and confining.
Crowding and Infection Risk
Why might infectious disease cues be especially connected to crowding perceptions? An emerging literature within evolutionary social psychology has highlighted the behavioral immune system (BIS), a system of specialized cognitive, behavioral, and emotional mechanisms by which people manage pathogenic threats (e.g., Ackerman, Tybur, & Mortensen, 2018; Mortensen, Becker, Ackerman, Neuberg, & Kenrick, 2010; Wang, Michalak, & Ackerman, in press). Specifically, the BIS is a first line of defense functionally designed to minimize contact with harmful viruses and bacteria before costly engagement of the physiological immune system becomes necessary.
Perhaps the most common bias associated with the BIS involves overperception of dangers associated with infection. This occurs for two reasons. First, detection of pathogens is imprecise; we can only observe their symptoms in most cases. Second, in contexts of uncertainty, threat detection mechanisms are adapted to prioritize minimization of relatively costly detection errors (Haselton & Nettle, 2006); here, the error of missing a pathogenic cue and becoming infected is greater than that of perceiving pathogen threats where none actually exist. Consistent with this idea, people concerned about germs are more lenient in categorizing targets along dimensions heuristically, but not truly, associated with disease such as physical disfigurement and obesity (Miller & Maner, 2012), and these people find it more difficult to look away from targets displaying such cues (e.g., Ackerman et al., 2009). Such prior studies have focused entirely on how pathogen threats influence perception of individuals or abstract conceptual groups (e.g., illegal immigrants), but we suggest that perceptions of social environments should also be susceptible to these threat management processes.
Due to the increased potential for human contact, dense social environments carry a higher likelihood of disease transmission than sparse environments. Indeed, population density is linked to increased likelihood of parasite and pathogen infection in an array of animals, including humans (Jones et al., 2008; Møller, Dufva, & Allander, 1993). Moreover, BIS activation has been tied to general social avoidance and increased introversion (Mortensen et al., 2010), which again suggests that people should be averse to socially dense situations. In such environments, the actual threats are not people per se, but rather the pathogens they potentially harbor. Because most pathogens are essentially invisible, and the symptoms they cause may be delayed or hidden, it can be quite difficult to identify actual pathogen carriers. A simpler solution involves strengthening aversion to social contact with many individuals, a behavior that could be supported by mechanisms that exaggerate the perceived density of social environments one encounters. To produce a functional outcome, this response pattern should also be accompanied by increased negativity to the idea of occupying such environments.
To further test functionality, we also predict that this response to infectious disease threat will differ from responses to certain other types of threats. For instance, given that exposure to crowded environments increases accessibility of self-protective concepts and behaviors like prevention focus and risk aversion (Maeng et al., 2013), physical safety-related threats may evoke strong crowding perceptions and aversions, something previous work has not examined. Building off of work linking crowding perceptions with attributions of arousal to social density (e.g., Gochman & Keating, 1980; Worchel & Teddie, 1976), we might expect that any situation where density is salient and people are aroused will lead people to feel crowded.
However, we maintain that these crowding perceptions will be largely threat-specific. Physical safety threats are typically associated with a specific person or environment rather than an imperceptible cause (e.g., pathogens). For example, the danger of accidental physical harm may be reflected by the structure of the environment (e.g., potholes in the street, unsafe materials in a room), and the danger of interpersonal physical aggression may be reflected by explicit behaviors of a violent person (e.g., angry emotional expressions, intimidating actions). Therefore, biases to perceive social situations as more crowded would do little to reduce the costs of these targeted threats.
Current Research
Because other humans are vectors of pathogen transmission, we predict that pathogen threats increase perception of social situations as more crowded and confining and elevate reluctance to enter these situations. Consistent with existing research which finds that pathogen threat cues most strongly affect people highly concerned about germs (e.g., Duncan, Schaller, & Park, 2009), we further examine whether this effect emerges primarily for chronically germ-averse people. To test this, we measure participants’ degree of germ aversion, as assessed by the subscale of the Perceived Vulnerability to Disease Scale (PVD; Duncan et al., 2009). In addition to germ aversion, the PVD scale also captures experiences with previous illnesses through a Perceived Infectability subscale. Because this subscale focuses on perceptions of internal susceptibility and is thus conceptually less relevant to perceptions of external situations, we focus here on the Germ Aversion subscale only. Finally, we predict that the expected pattern will emerge when people are primed with the specific threat of infectious disease and be attenuated for other physical threats.
We present one online pilot test and five larger tests of these predictions. In the pilot study and Study 1, we test the hypothesis that pathogen threat cues increase crowding perceptions relative to a nonthreatening control condition. In later studies, we compare pathogen threats with threats of physical safety involving accidents (Studies 2 and 3) and other dangerous situations involving personal harm (Studies 4 and 5). Finally, we present an internal meta-analysis of the central findings. For supplementary studies and additional measures, analyses, and discussion of the main study results, see the Supplementary Online Materials (SOM).
Pilot Study
Method
We ran a pilot test on Amazon’s Mturk with 64 participants (50% female, Mage = 35.6 years; see SOM for an additional pilot correlational study). We randomly assigned participants to read either a neutral control story about a person organizing their desk for school or a story designed to cue disease concern about a person volunteering at a hospital (these stories have been previously validated; White, Kenrick, & Neuberg, 2013). For example, the neutral story read as follows: Imagine you are in your house, in the room where you study. You have decided to organize your workspace because the semester has just begun and you want to be organized. You have already bought your books for classes and you have a syllabus and some initial paperwork for each class.
The disease story read as follows: You’re not enjoying your biology course. During one week you had to operate on a pig preserved in a foul-smelling formaldehyde solution. The next week’s assignment is volunteer work in the geriatric ward of the local hospital. You recall visiting your great-grandmother in the hospital, and remember how the sight of all those elderly patients made you feel a bit queasy.
Next, participants rated the crowdedness of four visual scenes featuring large numbers of people. These were presented in random order and included images of an airport, subway, store, and pool. Specifically, we asked people to answer the following crowding perception questions: “How likely are the people to bump into or brush against each other?” (1-not at all, 7-very likely), “How crowded do you think this scene is?” (1-empty, 7-very crowded), and “How would you feel in this scene?” (1-unconfined, 7-confined). Following the ratings of the scenes, participants completed the PVD scale. We included a free-response exclusion check question asking people to recall the story they read at the beginning of the study. We also included a manipulation check question, which asked participants how worried they felt when they read the story at the beginning of the study (1-not at all, 7-very). Participants finally provided demographics.
Results
Two people failed the exclusion check and were excluded. We averaged all crowding items across all scenes (a = .73). We then conducted a linear regression analysis predicting perceptions of crowding from threat condition (effect coded as −1, 1), germ aversion (centered; M = 4.28, SD = 0.90), and their interaction. The main effect of threat condition was not significant (p = .15), whereas the main effect of germ aversion was significant, b = .31, SE = .09, 95% confidence interval (CI) = [0.12, 0.50], t(58) = 3.33, p = .002, r = .40, such that the higher people scored on germ aversion, the more crowded they perceived the scenes to be.
Notably, a significant interaction between threat condition and germ aversion emerged, b = .20, SE = .09, 95% CI = [0.01, 0.39], t(58) = 2.09, p = .04, r = .26 (all r effect sizes refer to partial correlations; see Figure 1). Simple slopes analysis conducted using the MODPROBE tool (Hayes & Matthes, 2009) revealed that for participants cued with pathogen threat, germ aversion positively predicted ratings of scene crowding, b = .51, SE = .15, 95% CI = [0.22, 0.80], t(58) = 3.47, p = .001, r = .41. In contrast, this did not occur in the no-threat condition, p > .25. Simple slopes analysis also revealed that differences between threat conditions were significant when germ aversion was +1SD from the mean, b = .30, SE = .12, 95% CI = [0.06, 0.53], t(58) = 2.51, p = .01, r = .31, and not when germ aversion was −1SD from the mean, p > .25. Thus, initial evidence from the pilot study suggests that when pathogen threat is salient, high levels of chronic germ concerns predict greater perceptions of crowding. Given the limitations of the pilot study, we examined this finding using larger samples and more expansive experimental methods in the next studies.
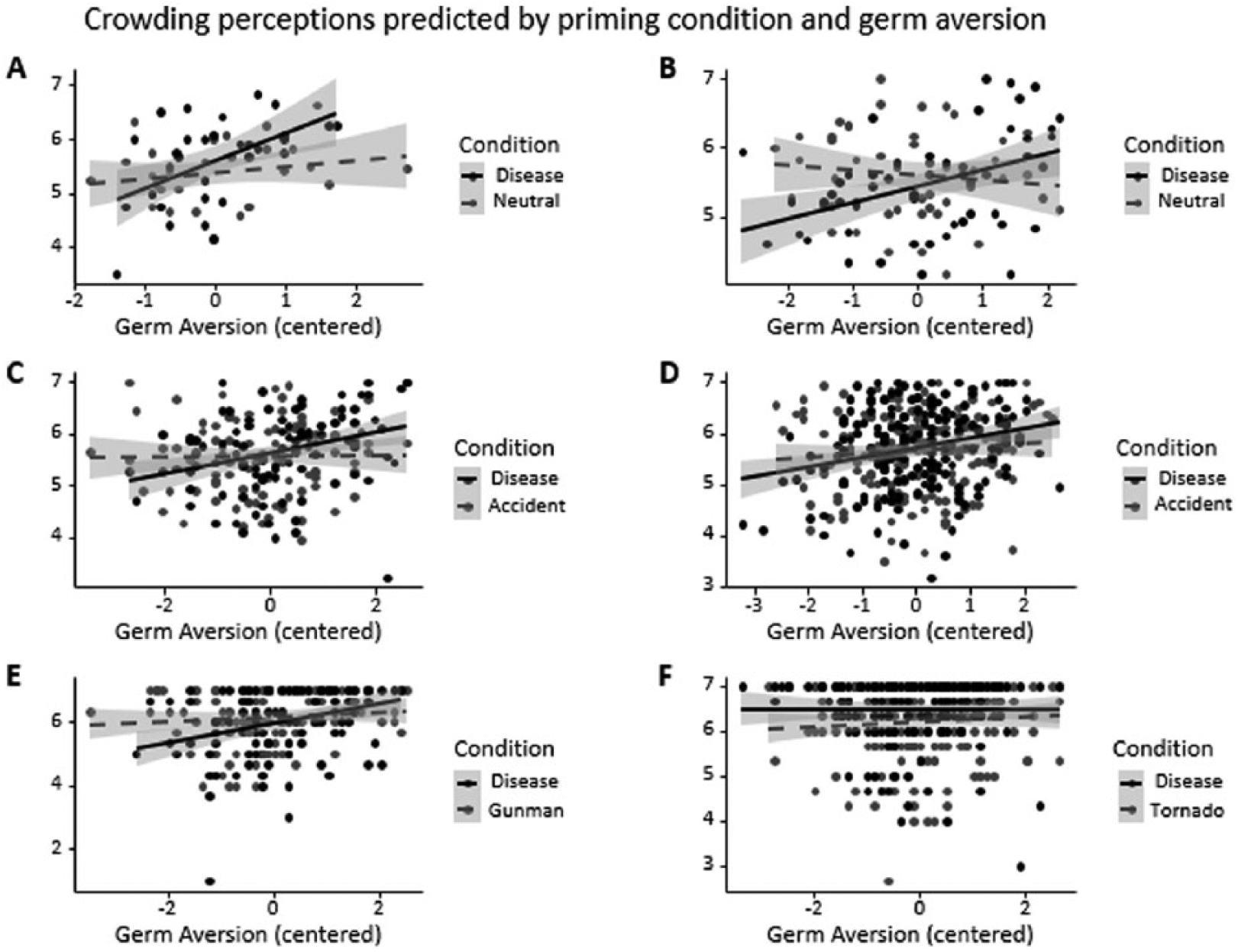
Crowding perceptions as predicted by threat condition and germ aversion for pilot study (Graph A), Study 1 (Graph B), Study 2 (Graph C), Study 3 (Graph D), Study 4 (Graph E), and Study 5 (Graph F) where higher numbers indicate greater crowding perception.
Study 1
Method
Participants were 102 MTurk workers (52% female, Mage = 38.4 years) who participated for a small payment. In this study, we used a convention of 50 participants per manipulated condition, but in subsequent studies increased this sample size to a minimum of 100 per condition, providing at least 85% power based on the interaction effect size obtained in the pilot study (see SOM for how this was calculated). Study 1 used a 2 (threat condition: pathogen threat, no threat; between-subjects) × 2 (scene valence: negative, positive; within-subjects) mixed design. Participants were randomly assigned to read one of the two vignettes used in the pilot study.
Participants then viewed pictures of three scenes considered negative when socially dense (taken from the second pilot study: subway, pool, store) and three scenes considered more positive when socially dense (bar, coffee shop, club), each featuring large numbers of people in random order. In the pilot study, the scenes used were considered negative when crowded, and thus the addition of positive scenes in the current study allowed us to test whether anticipation of a negative experience is necessary for pathogen cues to influence crowding perceptions. Participants responded to the same three questions from the pilot study on crowding perceptions for each context. They also responded to two measures of affective/motivational evaluation: “How much would you want to be present in this situation?” (1-not at all, 7-very much) and “How do you feel when you look at this picture?” (1-negative, 7-positive). These were included to assess motivation to enter or avoid each situation. Finally, participants completed the PVD scale, answered an exclusion check (i.e., “What was the story you read about?”), and demographic questions.
Results
We excluded two participants for failing the exclusion check. Initial analyses revealed that scene valence did not significantly moderate any of the effects of interest, specifically the interaction between threat condition and germ aversion (see SOM for analyses including scene valence). We therefore averaged all crowding perception questions (i.e., touch likelihood, confinement, crowding) across positive and negative scenes into one measure of crowding, a = .90. We ran a linear regression analysis with threat condition (effect coded −1, 1) and germ aversion (centered; M = 4.57, SD = 1.19) and the interaction between these as predictors of crowding perceptions. No main effect of threat condition (p = .15) or germ aversion (p = .17) emerged. However, a significant interaction between threat condition and germ aversion emerged, b = .15, SE = .06, 95% CI = [0.04, 0.27], t(96) = 2.68, p = .01, r = .26. Simple slopes analysis (see Figure 1) demonstrated a similar pattern to our pilot test in which germ aversion positively predicted crowding perception, but only for people cued with pathogen threat, b = .24, SE = .07, 95% CI = [0.09, 0.38], t(96) = 3.27, p = .002, r = .32, and not for people in the no-threat condition, p > .25. Interestingly, in this study, the difference between the no-threat and threat conditions was greatest for those −1SD in germ aversion, b = –.27, SE = .09, 95% CI = [–0.46, –0.09], t(96) = −2.91, p = .004, r = .28, rather than for those +1SD in germ aversion, p > .25.
Next, we examined the affective/motivational reactions people had toward the scenes. Scene valence again did not moderate the key interaction, so we averaged both affect questions (i.e., want to be in the scene, feelings about the scene) across positive and negative scenes, a = .91. Analysis using this composite revealed no significant main effects of threat condition or germ aversion on affect, all ps > .25. However, we found a significant interaction between threat condition and germ aversion, b = –.20, SE = .10, 95% CI = [–0.41, 0.00], t(96) = −1.99, p = .05, r = .20 (see Figure 2). Simple slopes analysis showed that for participants cued with pathogen threat, increased levels of germ aversion were associated with a more negative response to the scenes, b = –.26, SE = .13, 95% CI = [–0.52, –0.01], t(96) = −2.03, p = .05, r = .20. In contrast, this pattern was not present in the no-threat condition, p > .25. This difference in threat versus no-threat conditions was marginally significant for those at −1SD in germ aversion, b = .30, SE = .17, 95% CI = [–0.03, 0.63], t(96) = 1.83, p = .07, r = .18, but not those who scored higher (+1SD) in germ aversion, p > .25.
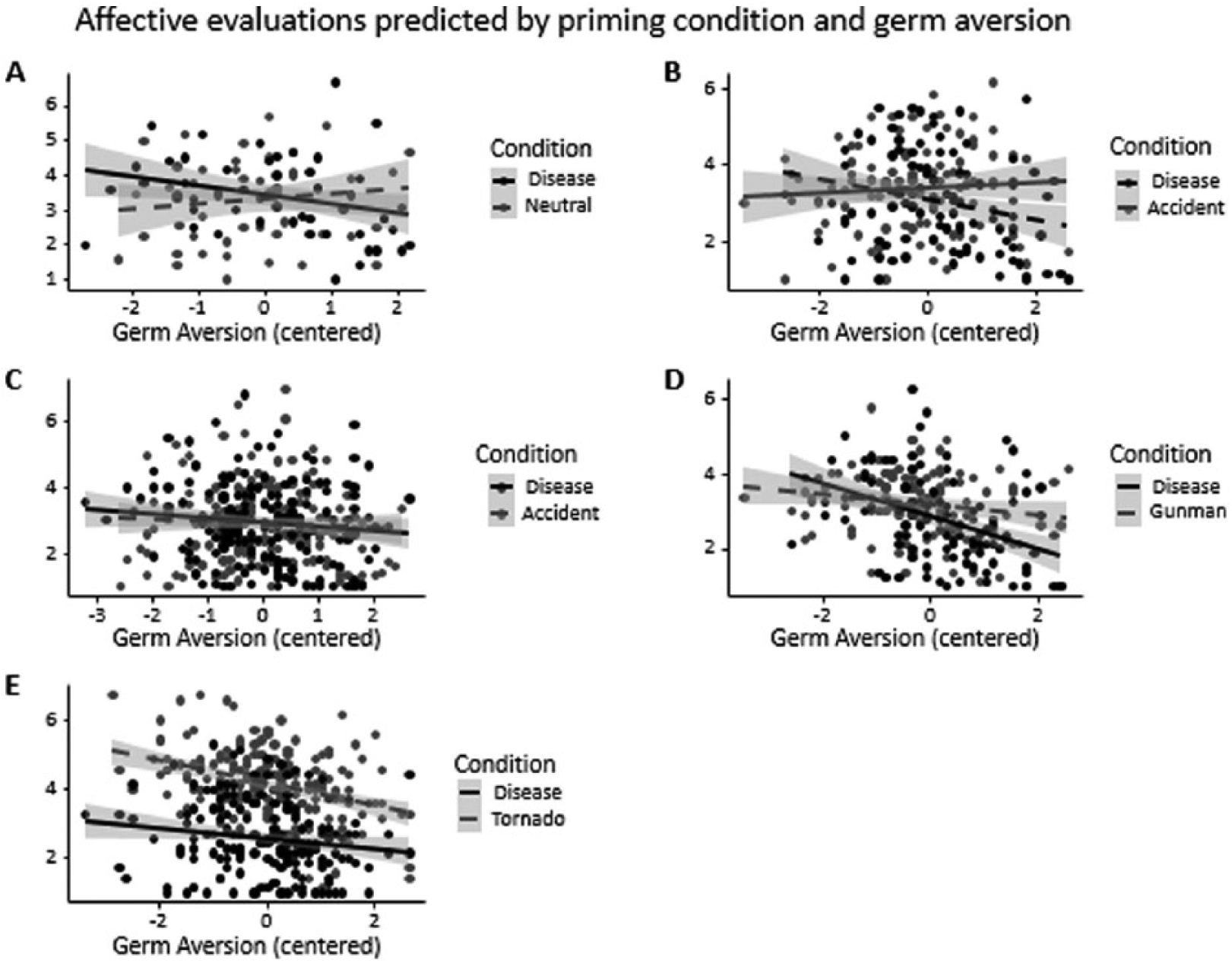
Affective evaluations as predicted by threat condition and germ aversion for Study 1 (Graph A), Study 2 (Graph B), Study 3 (Graph C), Study 4 (Graph D), and Study 5 (Graph E) where lower numbers indicate more negativity.
Study 2
Method
Does any type of threat increase perceptions of crowding? Study 2 tested this by replicating Study 1 but replacing the neutral condition with a threat of personal harm. Participants were 208 people (53% females, Mage = 36.74 years) recruited from MTurk. Participants either viewed a slideshow about dangerous household and vehicular accidents being on the rise in the United States (Faulkner et al., 2004) or viewed a slideshow about how diseases were on the rise in the United States (Hill, Prokosch, & DelPriore, 2015). Then they viewed the same scenes and were asked the same questions as in Study 1. Unlike Study 1, however, the affective evaluation questions were replaced with variations on the same theme, “How much would you want to be present in this exact situation?” (1-not at all, 7-very) and “How comfortable would you be in this situation?” (1-not at all, 7-very).
Results
Two participants failed the manipulation check and were excluded. Again, a model with scene valence as a predictor yielded no significant interactions between scene valence and the other independent variables (see SOM). Therefore, we collapsed all crowding perception (a = .78) and affect/motivation ratings (a = .84) into separate composites across scenes.
A linear regression analysis was conducted with threat condition (effect coded) and germ aversion (centered; M = 4.42, SD = 1.18) as well as their interaction as predictors of crowding perceptions. No significant main effect of threat condition emerged, p > .25. However, this analysis did reveal a significant main effect of germ aversion such that people who scored higher on germ aversion tended to perceive more crowding in the scenes, b = .10, SE = .04, 95% CI = [0.02, 0.19], t(202) = 2.44, p = .02, r = .17. Notably, a significant interaction between threat condition and germ aversion emerged, b = .10, SE = .04, 95% CI = [0.01, 0.18], t(202) = 2.24, p = .03, r = .16 (see Figure 1). As was found in our previous studies, people with higher levels of chronic germ aversion perceived the scenes as more crowded if they had viewed the disease slideshow—simple slope: b = .20, SE = .06, 95% CI = [0.08, 0.32], t(202) = 3.34, p = .001, r = .23—but not if they viewed the accidents slideshow (p > .25). The difference between disease and accident threat was greater for those high (+1SD) in germ aversion, b = .14, SE = .07, 95% CI = [0.00, 0.28], t(202) = 1.92, p = .06, r = .13, than those low (–1SD) in germ aversion, p = .21.
Affect was next regressed on threat condition and germ aversion (centered) as well as their interaction. A marginal effect of threat condition emerged such that overall, people who were exposed to the disease slideshow rated the scenes as less pleasant, b = –.15, SE = .08, 95% CI = [–0.32, 0.01], t(202) = −1.81, p = .07, r = .13. No main effect of germ aversion emerged (p = .19). However, we again found a significant interaction between germ aversion and threat condition, b = –.18, SE = .07, 95% CI = [–0.32, –0.04], t(202) = −2.57, p = .01, r = .18 (see Figure 2). Looking at the simple slopes, when cued with disease, people who were chronically germ averse felt more negative and wanted to avoid crowded situations, b = –.28, SE = .10, 95% CI = [–0.47, –0.08], t(202) = −2.73, p = .01, r = .19. However, when cued with accidents, germ aversion did not make a difference (p > .25). This difference between threat conditions was more strongly felt when germ aversion was high (+1SD), b = –.37, SE = .12, 95% CI = [–0.60, –0.13], t(202) = −3.09, p = .002, r = .21, than when germ aversion was low (–1SD), p > .25.
Unlike in earlier studies, an independent-samples t test on germ aversion with prime condition as the predictor showed that germ aversion scores were influenced by the prime, t(204) = −2.39, p = .02, r = .17. Given the analytical issues this association raises, we next replicated the current study using a design intended to rule out prime effects on chronic concern.
Study 3
Method
In Study 3, PVD was measured 1 week in advance of all other study procedures (which otherwise were identical to Study 2). We ran 365 MTurk participants (52% female, Mage = 36.22 years) who completed both parts of the survey (attrition rate: 18%).
Results
We excluded three manipulation check failures and four participants who had seen the manipulation twice. We again averaged across scenes on crowding perceptions (a = .91) and affective evaluations (a = .92). Examining the effect of prime (effect coded), germ aversion (centered; M = 4.22, SD = 1.06), and their interaction on crowding perceptions, no main effect of prime emerged (p > .25), but a significant positive relationship between germ aversion and crowding perception was revealed, b = .13, SE = .04, 95% CI = [0.05, 0.20], t(353) = 3.32, p = .001, r = .17. Unlike the prior study, the prime by germ aversion interaction was merely trending, b = .06, SE = .04, 95% CI = [–0.01, 0.14], t(353) = 1.61, p = .11, r = .09, although the direction of the interaction mirrors what was found earlier (see Figure 1). Repeating the same regression analysis on affective reactions, we also only found a trending main effect of germ aversion, b = –.10, SE = .06, 95% CI = [–0.21, 0.02], t(353) = −1.61, p = .11, r = .09, such that those who were higher in germ aversion felt more negatively about the scenes. The main effect of prime and the interaction (see Figure 2) were not significant, all ps > .25.
Study 4
Method
Study 4 included three substantive changes from prior designs. First, we contrasted pathogen threat cues with cues relevant to a different type of interpersonal threat—physical aggression. Second, threat cues were presented as explicitly relevant to the decision context, whereas in previous studies, threat was cued in a more incidental manner. Finally, we investigated choice behavior as a consequence of shifts in affect and crowding perceptions. Participants were 236 MTurk users (54% female, Mage = 35.46 years) randomly assigned to read scenarios matching one of two conditions. In the pathogen threat condition, the participant is cast as a shopper in a mall that comes under quarantine due to reports of an Ebola outbreak. For instance, the scenario read as follows: You learn that there is reason to believe that some people in the mall have been exposed to Ebola, an infectious disease that could be left fatal if left untreated. Officials believe exposure happened ten minutes ago in a specific area of the mall, so not everyone has been directly exposed.
In the aggression threat condition, the mall was undergoing lockdown due to reports of an active shooter. For instance, the scenario read as follows: You learn that there have been sightings of a suspicious person in the mall wearing dark sunglasses and carrying several weapons. It’s unclear if anyone has been hurt yet, and if so, who has been hurt. You hear that the suspicious person was last sighted ten minutes ago walking around the open areas in the mall.
In both of the stories (see SOM), the participant runs into a nearby store to find a large group of people there. Participants were also told at this point that there is an empty store nearby they could move to with no adverse consequences. Participants then rated eight items that described affective reactions to being in the socially dense space (e.g., “How threatened do you feel?” “How safe do you feel about waiting in the store you are currently in?” “How much do you trust the people in the store?” “How disgusted do you feel?” etc.) and the three items used in the previous studies to assess perceptions of space crowdedness.
To measure choice, participants were reminded that an alternative, empty store existed that they could wait in during the scenario, and they chose whether to remain in the current, more crowded store or move to the empty store. This choice was measured using both a 6-point continuous scale (1-remain at the crowded store, 6-go to a nearby empty store) and a binomial choice item (current store vs. empty store). Finally, we included two exclusion checks, one asking people to identify the content of the scenario and one question asking people to identify how many people were in the room they had entered immediately after hearing about the threat (response options: “empty,” “a couple,” and “many”).
Results
We excluded 14 people for failing at least one of the manipulation check questions (the reported results hold when these people are included). Given the expanded number of affect/motivation evaluation questions, we first submitted these to a principal components analysis using a promax rotation. Based on the scree plot and our theoretical predictions, we extracted one factor (λ = 9.02, all item loadings > .56) which explained 44.11% of the variance. We therefore collapsed across these items by averaging them together to obtain one measure of affect/motivation in the situation (a = .81), such that positive scores indicated more positive evaluations. As before, we collapsed the three crowding items into a composite measure (a = .80).
Perceptions and affect
Linear regression analysis of crowding perceptions revealed no main effect of the scenario manipulation (effect coded; p = .11), but a main effect of germ aversion (centered; M = 4.46, SD = 1.13) indicated that higher chronic levels of germ aversion were associated with higher crowding perceptions, b = .19, SE = .06, 95% CI = [0.07, 0.30], t(218) = 3.28, p = .001, r = .22. As in Studies 1 to 2, we also found a significant interaction between germ aversion and scenario type, b = .12, SE = .06, 95% CI = [0.01, 0.23], t(218) = 2.06, p = .04, r = .14, such that participants’ germ aversion was predictive of crowding perceptions only when they read about the Ebola outbreak—simple slope: b = .31, SE = .08, 95% CI = [0.14, 0.47], t(218) = 3.65, p = .003, r = .24. This relationship did not emerge for those participants who read about the active gunman (p = .37; see Figure 1). This difference in crowding perceptions between scenario manipulations was driven by those 1SD lower in germ aversion, b = –.24, SE = .09, 95% CI = [–0.42, –0.06], t(218) = −2.58, p = .01, r = .17, and not by those 1SD greater in germ aversion, p > .25.
Analysis of the affect evaluation composite showed two main effects. The scenario led participants who read about an Ebola outbreak to feel more negative about their current room context than participants who read about an active shooter, b = –.16, SE = .07, 95% CI = [–0.29, –0.03], t(218) = −2.38, p = .02, r = .16. In addition, the more germ averse people were, the more negatively they felt about the situation, b = –.29, SE = .06, 95% CI = [–0.40, –0.17], t(218) = −4.87, p < .001, r = .31. We also found a significant interaction between germ aversion and scenario type, b = –.15, SE = .06, 95% CI = [–0.26, –0.03], t(218) = −2.49, p = .01, r = .17 (see Figure 2). Teasing this interaction apart, for those high in chronic levels of germ aversion, reading about the Ebola outbreak led people to feel more negatively about being with a large group of people, b = –.43, SE = .09, 95% CI = [–0.60, –0.26], t(218) = −5.03, p < .001, r = .32; this relationship was in the same direction, though the effect was marginal for those reading about the active gunman, b = –.14, SE = .08, 95% CI = [–0.30, 0.02], t(218) = −1.74, p = .08, r = .12. The difference between experimental conditions was primarily driven by those higher in germ aversion (+1SD), b = –.32, SE = .09, 95% CI = [–0.51, –0.14], t(218) = −3.47, p = .001, r = .23, while the simple slope at −1SD was not significant, p > .25.
Choice
Examining the effects of scenario manipulation (effect coded), germ aversion (centered), and their interaction on the continuous choice measure revealed that scenario condition affected preferences, b = .54, SE = .10, 95% CI = [0.35, 0.74], t(218) = 5.52, p < .001, r = .35, such that people who read the Ebola scenario preferred the empty store more (M = 5.43, SD = 1.24) than people who read the gunman scenario (M = 4.29, SD = 5.43). There was no interaction between germ aversion and scenario condition (p > .25), though a trending main effect of germ aversion did emerge, b = .14, SE = .09, 95% CI = [–0.03, 0.32], t(218) = 1.66, p = .10, r = .11, such that people who were higher on germ aversion showed a slightly greater preference for the empty room.
We used logistic regression to test effects on the binomial choice item, yielding results similar to those for the continuous choice measure. The manipulation predicted choices, b = .79, SE = .18, 95% CI = [0.45, 1.17], z(218) = 4.34, χ2 = 18.85, p < .001, r = .28. Those who read the Ebola scenario preferred the empty room (89%) more than people who read the gunman scenario (62%). There was no main effect of germ aversion and no interaction between the scenario condition and germ aversion on choice, all ps > .25. Thus, actual choices were influenced by experiences with pathogen threat, though, unlike the affect and perception effects, this influence did not emerge as a person by situation interaction.
Finally, as in Study 2, an independent-samples t test showed that germ aversion was influenced by scenario condition, t(220) = −2.51, p = .01, r = .17. Given this result, we replicated the current study using a similar method to Study 3 in which PVD was measured separately from the rest of the study procedures.
Study 5
Method
To address the influence of prime on germ aversion, we ran a series of studies with PVD measured either 1 week before or after the main study manipulation, thereby decoupling these factors. In Study 5, PVD was measured a week in advance. Several replication studies were required because of manipulation failures and ceiling effects, as explained below. The last of this series is reported as Study 5, and all additional studies are reported in SOM. Furthermore, all studies are included in the subsequent internal meta-analysis.
Participants were 371 Mturk workers (55% female, Mage = 35.56 years) who completed both parts of the survey. We had an attrition rate of 17%. We retained the original design as Study 4, but with several changes. Because disgust is more relevant to the disease scenario, including this item in the affective evaluations composite could bias our finding in favor of this condition, and thus it was removed. In addition, the physical safety scenario about a gunman was replaced with one about a dangerous tornado because the manipulation checks for the gunman scenario did not replicate results from Study 4. Specifically, whereas in Study 4 the gunman scenario was seen as significantly more fear-inducing than the Ebola scenario, in our first replication study (see SOM Study 1 for more details), this difference did not emerge. In our second replication study (see SOM Study 2 for details), we attempted to address this by replacing the gunman scenario with a scenario in which the participants shelters from a tornado. The tornado scenario was pretested to elicit more fear and more concern about personal safety than the disease scenario. An excerpt of the tornado scenario read as follows: The announcement says that officials have learned there are sightings of a dangerous weather event approaching the mall. It seems that the mall is in the path of a major tornado that has touched down a block away. It’s unclear if anyone has been hurt, and if so, who has been hurt.
We also replaced Ebola with tuberculosis because we were concerned that the Ebola threat evoked very high levels of arousal, perhaps contributing to the ceiling effect findings. Comparing people’s responses to the Ebola versus tuberculosis scenarios, it did seem the case that tuberculosis was perceived as less worrisome (see “Manipulation Checks” sections in SOM). However even in SOM Study 2, the ceiling effect on crowding perceptions remained, potentially obscuring any interactive effect of germ aversion and pathogen threat manipulation.
In Study 5, we again attempted to resolve the ceiling effect issue from the previous scenario studies. We reasoned that, unlike Studies 1 to 3 in which participants viewed photographs as part of the manipulations, no photos were used in the later scenario studies, perhaps encouraging all participants to imagine very socially dense environments, and thus creating a ceiling effect in crowding perceptions. Therefore, participants in the current study were told to imagine waiting in a store and were provided a photograph of this store that was somewhat ambiguous in social density (previously used in the pilot study and Studies 1-3). That is, the photograph showed a moderately socially dense environment but it did not reveal the full number of people or the size of the store, which should allow for subjectivity in crowding perceptions, but should also restrict participants from assuming high levels of crowdedness in the store. Finally, in contrast to prior scenario studies, participants learned about the alternate, empty room they could choose to wait in only when receiving the choice question and not with the rest of the measures, as in earlier studies. This was done to minimize the chance of participants contrasting socially dense room against the empty room, thus exacerbating perceptions of crowdedness in the dense room.
Results
We excluded five people who failed the manipulation check, as well as 13 people who were able to access the survey twice and were able to see the manipulation. Given that germ aversion was measured several days in advance, scenario condition did not predict germ aversion, p > .25.
Perceptions and affect
We again averaged across crowding perception items (a = .70) and affective evaluation items (a = .89). Examining the effects of scenario manipulation (effect coded), germ aversion (centered; M = 4.36, SD = 1.11), and their interaction on crowding perceptions, we found a main effect of scenario condition, b = .13, SE = .04, 95% CI = [0.05, 0.22], t(349) = 3.16, p = .002, r = .17, such that people who read the tuberculosis scenario perceived the room to be more crowded (M = 6.47, SD = 0.76) than people who read the tornado scenario (M = 6.20, SD = 0.82). There was no main effect of germ aversion, p > .25, nor was the interaction significant, p > .25 (see Figure 1).
We then examined the effects of scenario manipulation (effect coded), germ aversion (centered), and their interaction on affect. We again found a main effect of scenario condition, b = –.79, SE = .05, 95% CI = [–0.89, –0.68], t(349) = −14.82, p < .001, r = .62, such that people who read the tuberculosis scenario felt more negatively (M = 2.57, SD = 1.07) than people who read the tornado scenario (M = 4.13, SD = 1.00). The main effect of germ aversion was also significant, b = –.24, SE = .05, 95% CI = [–0.33, –0.14], t(349) = −4.97, p < .001, r = .26, such that people who scored highly on germ aversion were more likely to feel negatively. The interaction was only marginally significant, b = .09, SE = .05, 95% CI = [–0.01, 0.18], t(349) = 1.83, p = .07, r = .10 (see Figure 2).
Choice
As in Study 4, the current study featured both a continuous choice item, with higher scores indicating a greater preference for the empty room, and a dichotomous forced choice item. For the continuous choice item, we tested the effects of scenario manipulation (effect coded), germ aversion (centered), and their interaction. Replicating the previous study, we found a main effect of scenario condition, b = .71, SE = .08, 95% CI = [0.56, 0.85], t(349) = 9.28, p < .001, r = .44, such that people in the disease condition preferred the emptier room (M = 5.51, SD = 0.98) than the people in the tornado condition (M = 4.09, SD = 1.79). The effect of germ aversion on choice was also significant, b = .16, SE = .07, 95% CI = [0.02, 0.30], t(349) = 2.30, p = .02, r = .12, such that higher levels predicted more preference for the empty room. The interaction was not significant, p > .25. Similar patterns emerged for the forced choice question. Again replicating the previous study, people were more likely to choose the empty room if they were given the tuberculosis scenario, b = 1.22, SE = .17, 95% CI = [0.91, 1.57], z(349) = 7.27, χ2 = 52.8, p < .001, r = .36. Whereas only 52% of people in the tornado scenario chose to move to the empty room, almost everyone chose to move to the empty room in the tuberculosis scenario (92%). Neither the main effect germ aversion, p = .14, nor the interaction were significant, p = .19.
Internal Meta-Analyses
The findings presented in this article demonstrate not only relatively consistent patterns but also variation in the significance levels of certain effects, in particular the interaction of prime condition and germ aversion on crowding perceptions and affect. Therefore, we conducted an internal meta-analysis of these measures as a means of determining overall reliability and effect size. To do this, we used R’s metafor package (Viechtbauer, 2010), which has been used in other recent meta-analyses (e.g., Shariff, Willard, Andersen, & Norenzayan, 2016). We included the pilot test and Studies 1 to 5 as well as the two additional scenario studies reported in the SOM. Because of the variation across studies in designs and findings, we used a random effects model.
We first present the meta-analysis for crowding perception as the dependent variable, and then the meta-analysis for affect/motivation as the dependent variable. Each analysis includes tests of the main effects and interactions, and when applicable, the simple slopes for prime conditions (see SOM for meta-analysis of the simple effects at high and low levels of germ aversion). Finally, we test whether the effect of the simple slope for the disease condition significantly differs from the effect for the control condition.
Examining the main effects and interaction for crowding perceptions, a Cochran’s test revealed that these studies were significantly heterogeneous, all Q(df = 7) > 14.91, ps < .05, supporting the choice of a random effects model. Across the eight studies, the average effect size of the interaction between germ aversion and condition on crowding perceptions was r = .09, SE = .04, p = .02, 95% CI = [0.01, 0.16], indicating the presence of a reliable, if small effect (see Figure 3). Examining main effects, prime condition on its own did not predict crowding perceptions, r = .02, SE = .04, p > .25, 95% CI = [–0.05, 0.09]. However, germ aversion did reliably predict greater crowding perceptions, r = .14, SE = .03, p < .0001, 95% CI = [0.08, 0.21].
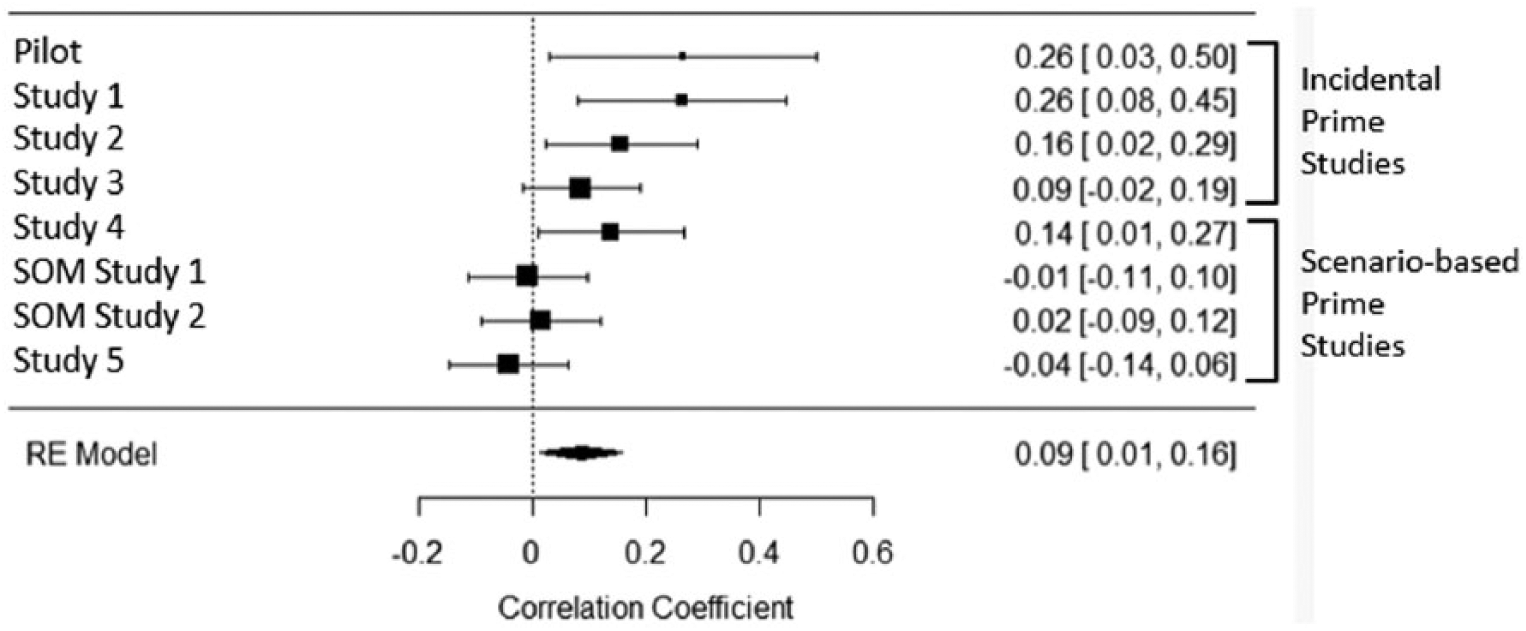
Meta-analytic effect of the interaction of prime and germ aversion on crowding perceptions with random effects (RE) model.
We next examined the meta-analytic effects of the simple slopes within threat condition (i.e., testing each slope against zero). To do this, we computed separate random effects meta-analyses for disease prime and control primes. Germ aversion was related to crowding perceptions in the disease prime condition, r = .17, SE = .05, p = .001, 95% CI = [0.07, 0.27]. The meta-analysis also revealed a weaker, though reliable relationship between germ aversion and crowding in the control conditions, r = .05, SE = .02, p = .03, 95% CI = [0.005, 0.09]. We compared these two estimates of effect size r against each other, and indeed this test revealed that the disease primes produced significantly larger effect sizes than the control primes, r = .12, SE = .06, p = .03, 95% CI = [0.01, 0.23].
As mentioned in Study 5, we suspected that there might be a moderation of this meta-analytic effect of the interaction on crowding perceptions by the type of manipulation we used. That is, whereas the pilot study and Studies 1 to 3 used picture-based stimuli and incidentally framed primes, Studies 4, 5, and SOM Studies 1 and 2 used scenario-based stimuli where the participant was actually immersed in the crowded situation, as well as a prime that was more life-threatening. Our test of moderation indicated that there was a significant moderation by study manipulation, QM(df = 1) = 6.25, p = .01, such that there was a reduction in effect size for the interaction in the studies that were more scenario-based, r = –.07, SE = .03, 95% CI = [–0.12, –0.02], p = .01. This moderator accounted for 70.70% of the heterogeneity in the effect, strong evidence that the differences in manipulation type account for the different patterns we see across the studies.
We also ran a similar meta-analysis of participants’ affect/motivation evaluation ratings, which were collected in seven of the studies (not included in the pilot study). We chose a random effects model for the same reasons as before, as supported by a significant Cochran’s tests of heterogeneity, all Q(df = 6) > 14.91, all ps < .02. Based on this analysis, we found that the interactive effect of condition and germ aversion does not reliably predict affect, r = –.07, SE = .04, p = .06, 95% CI = [–0.15, 0.00]. However, the average effect size of the main effect of condition was reliable and moderate, r = –.28, SE = .11, p = .01, 95% CI = [–0.50, –0.07]. Finally, examining the main effect of germ aversion on affective evaluations, we found a reliable small effect, r = –.20, SE = .04, p < .0001, 95% CI = [–0.27, –0.13].
In sum, we find both a reliable interactive effect of prime condition and germ aversion on crowding perceptions, along with a reliable main effect of germ aversion. We also find that the relationship between germ aversion and crowding perception is significantly greater in the disease prime condition in contrast to the control prime conditions, as would be expected if people high in chronic disease concern are particularly sensitive to situational pathogen cues. Finally, with respect to affective evaluations, we find reliable main effects of condition and germ aversion. Thus, over all current studies, infectious disease threats reliably interact with individual differences in germ aversion to predict perceptions of crowding, and disease threats also predict strong negative affective evaluations of these crowds.
General Discussion
Do people change their perceptions of social situations when confronting particular threats? Here, we found that the threat of infectious disease led germ-averse people to perceive socially dense environments as more crowded and confining. Disease cues also led people to feel more negative when thinking about entering these environments. And when given the option, disease-threatened people subsequently chose to occupy empty places rather than spend time with groups. Notably, these crowding experiences were attenuated in the presence of physical accident, extreme weather, and interpersonal violence cues. Internal meta-analyses indicated that the pathogen threat effects were reliable, if small in magnitude. Thus, experiences with crowding appear connected to concerns about infection, even more than they are to concerns about other, noncommunicable sources of danger.
Although these effects were reliable, substantive variation was present in the pattern of association between predictors and outcomes, both within and across studies. To illustrate this, in Studies 1, 2, and 4, we found a significant interaction between germ aversion and situational prime on crowding perceptions and affective evaluations. However, in Study 5, only main effects of prime and germ aversion predicted these outcomes. Furthermore, all choice decisions across studies were influenced solely by main effects. Summarizing these patterns in the internal meta-analyses, we observed that crowding perceptions were not consistently predicted by the prime, but rather by the interaction between germ aversion and prime, whereas affective evaluations were predicted by the situational prime, but not the interaction between the prime and germ aversion.
One potential reason is that the type of manipulations (incidental vs. scenario-based primes) we used may have led to the ceiling effects witnessed in Studies 4 and 5 as well as the main effects found for affect and choice. The first set of studies used manipulations featuring factual information, such as charts showing the rise of accidents or infectious diseases (Studies 2 and 3), in which the key threats were incidental to the social perception task. The latter set of studies (Studies 4 and 5) differed in that they used scenarios representing strong life-or-death situations in which the threat was embedded within the social perception task itself. Compared with these latter studies, the manipulations in the first set of studies may have also been less severe or even ambiguous in their consequences, as witnessed in the hospital prime where a nurse does not seem to make a big fuss about the protagonist being sneezed on while volunteering (pilot study and Study 1). Differences in affective intensity would be consistent with the fact that the average amount of worry felt after the inductions was greater (for both the disease and control threat priming conditions) following the scenario manipulations than following the incidental primes (see SOM for these analyses). Both the disease and personal safety scenarios could have increased participants’ arousal, leading them to feel especially crowded (see Worchel & Teddie, 1976; Worchel & Yohai, 1979). This may also explain why we see only main effects for affect and choice; the scenarios could have overwhelmed the effect of individual differences, such that even those people who were not chronically concerned about disease still desired to avoid crowds of potential Ebola-carriers.
It is also possible that the nature of the dependent measures themselves resulted in differences in perceptions, affect, and choice. For instance, people asked to make choices about entering crowded versus uncrowded environments may act conservatively by avoiding potential dangers. Such conservative decision making would be consistent with the tendency to minimize costly errors (Haselton & Nettle, 2006). Specifically, when a person’s life is on the line (Studies 4 and 5), typical patterns of cognition may be overwhelmed by salient emotions, driving a universal desire to avoid dangerous situations. Thus in the context of our results, this emotional response may have wiped out interactions with individual differences, producing only a main effect of situational threat. Inconsistencies between the emergence of main effects and interactions represent a key issue facing the BIS literature (see Ackerman, Hill, & Murray, in press).
Despite the study differences, our findings do offer convergent evidence that pathogen concerns play a role in how people perceive and feel about social situations, expanding upon early crowding literature by identifying a potentially important predictor of crowding experience. Our results suggest that crowding experiences may not be solely the result of arousal attributed to social density, as demonstrated by early work (Worchel & Teddie, 1976; Worchel & Yohai, 1979), but rather as a response to specific threats of infectious disease. Why do we find that responses to dense social environments are more closely tied to infectious disease threat than other threats? Unlike many other threats, humans themselves represent means through which pathogens are transmitted, and the microscopic nature of pathogens makes accurate detection difficult. Crowded environments also limit people’s ability to escape germ exposure and may obscure identification of who, specifically, is infected. In short, crowds afford unique threats to individuals from the perspective of infection risk. In contrast, more identifiable dangers (e.g., predators, aggressors) are often associated with the desire to seek safety in numbers (e.g., Hamilton, 1971), making crowds an opportunity for individuals to conceal themselves within a larger group. This said, participants facing nondisease threats in our studies still generally preferred to avoid crowded areas (perhaps because the crowd consisted of strangers).
Finally, viewing social environments from the perspective of pathogen transmission risk may broaden our understanding of day-to-day behaviors and even societal phenomena. Disease outbreaks and indicators could influence decisions made in close proximity to others, from deciding to shop at a less crowded store to avoiding relocation to a densely populated city. At a societal level, our findings may inform coping mechanisms in urban environments. Late social psychologist Stanley Milgram (1970) noted that structural components in large cities are designed to limit human contact, such as a setting of boundaries in social transactions (e.g., self-service kiosks), and an increase in anonymity (e.g., unlisting of phone numbers). This produces a paradox of increased social isolation—despite greater potential access to social relationships in cities, city inhabitants nevertheless feel more lonely and isolated. Based on our findings, this paradox may be explained as a coping mechanism wherein the threat of pathogen transmission posed by social density is reduced. Extending such directions from earlier work, scholars have recently stressed the importance of studying the psychological effects of social ecologies (e.g., Oishi & Graham, 2010; Sng et al., 2017). The current research adds to this framework by highlighting how the experience of different social environments can itself be shaped by the specific threats and opportunities these environments afford.
Supplemental Material
SupplementalMaterials_PSPB_Revised – Supplemental material for The Infectiousness of Crowds: Crowding Experiences Are Amplified by Pathogen Threats
Supplemental material, SupplementalMaterials_PSPB_Revised for The Infectiousness of Crowds: Crowding Experiences Are Amplified by Pathogen Threats by Iris M. Wang and Joshua M. Ackerman in Personality and Social Psychology Bulletin
Supplemental Material
wang_online_appendix – Supplemental material for The Infectiousness of Crowds: Crowding Experiences Are Amplified by Pathogen Threats
Supplemental material, wang_online_appendix for The Infectiousness of Crowds: Crowding Experiences Are Amplified by Pathogen Threats by Iris M. Wang and Joshua M. Ackerman in Personality and Social Psychology Bulletin
Footnotes
Acknowledgements
We thank Nicholas Michalak for assistance with data analysis, and Oliver Sng and Allison Earl for feedback on results. We thank our research assistants for help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Science Foundation Grant BCS-1226731 to Joshua Ackerman.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.