
Abstract
The relationship between beliefs about the causes of a policy-relevant issue (causal beliefs) and attitudes towards that policy (policy support) is complicated, with contradictory empirical results. The current research offers an explanation for this: causal beliefs only predict policy support when they are specific and correspond with the policy. We test this across six studies (N = 10,728; quota-representative samples of U.K. and US populations) within two policy domains (obesity and alcohol). In study 1, we test whether specific-corresponding beliefs are stronger correlates of policy support than other causal beliefs. In studies 2 and 4, we test whether communicating specific-corresponding causal evidence can increase policy support. In studies 3 and 4, we identify and confirm the psychological mechanism: perceived policy effectiveness. Study 5 involves a meta-analysis of the experimental studies. This provides support for our theory: specific-corresponding causal beliefs affect policy support, but general and non-corresponding causal beliefs do not.
Introduction
People’s attitudes towards public policies are a key determinant of policy implementation (Burstein, 2003; Lax & Phillips, 2012; World Health Organization, 2024). Because of the importance of these attitudes, many studies have been conducted to understand the myriad factors that explain why the public support or oppose a particular policy. In some cases, the results are replicable and generalisable (e.g., perceived policy effectiveness; see Reynolds et al. (2020) for a review). However, studies that investigate how people’s beliefs about the causes of a policy problem such as obesity, climate change, and criminal behaviour (i.e., causal beliefs) affect policy support have produced conflicting results, failures to replicate, and no clear account of why some results are statistically significant, while others are not (Ortiz et al., 2016; Pearl & Lebowitz, 2014; Reynolds et al., 2020b).
Causal beliefs have their origins in attribution theories (Heider, 1958; Kelley & Michela, 1980). When people encounter real-world behaviours, events, or societal issues, they regularly and spontaneously form causal explanations for these phenomena (Gendolla & Koller, 2001; Weiner, 1985). In the context of policy attitudes, people’s causal beliefs about policy issues are frequently correlated with policy support in domains such as obesity, alcohol use, climate change, marriage equality, and crime (Bostrom et al., 2012; Crandall et al., 2001; Genschow et al., 2017; Linos & West, 2003; Martin et al., 2000; Mazzocchi et al., 2015; Whitehead, 2014; Zucker & Weiner, 1993) suggesting that causal beliefs may be important in shaping policy support. For example, if people do not believe that burning fossil fuels causally influences climate change, then they are much less likely to support climate change policies that aim to reduce the burning of fossil fuels. This includes policies such as carbon taxes, frequent-flyer levies, or banning the sale of new vehicles with internal combustion engines.
In contrast to widely replicated correlations, experimental evidence is mixed. Many studies have been conducted in the domain of obesity with one systematic review and meta-analysis of the experimental evidence (Reynolds et al., 2022). The results show that, on average, evidence containing information about environmental causes of obesity are ineffective at changing causal beliefs and support for obesity policies. Although some individual studies in the review showed significant results (Ortiz et al., 2016; Pearl & Lebowitz, 2014), an independent replication of these studies produced null results (Reynolds et al., 2020b). Mixed results have also occurred in other domains such as environmental policies – where the causes of climate change or pollution are communicated before measuring support for environmental policies (Jang, 2013; Kim & Kim, 2023; Myers et al., 2023). If there is a causal effect of causal beliefs on policy support, then we argue that this might be difficult to detect due to flawed conceptualisations of causal beliefs. This can cause researchers to measure the wrong beliefs, the wrong attitudes, and design sub-optimal interventions. It is these flawed conceptualisations that this research addresses.
Examples of these flawed conceptualisations are evident throughout the literature. For example, within the obesity context multiple studies reported interventions with general or non-specific causal messages such as “Many obese people want to lose weight, but they do not do so because of societal influences” (McGlynn & McGlone, 2019), and “Everyone makes choices about what they eat, but the food environment influences what choices are available. . .” (Pearl & Lebowitz, 2014). We argue that these messages are too vague to influence attitudes towards specific policies. Furthermore, when specific examples of environmental causes are mentioned in the intervention content, these studies do not always measure support for the specific, corresponding policy. For example, in a study by Barry et al. (2013)), the intervention stated, “scientific studies indicate that living in neighbourhoods where it is difficult to . . . find safe places to exercise,” but this was followed by a measurement of support for dietary policies, but not a measurement of support for policies relating to creating safe places to exercise. Similarly, Pearl and Lebowitz (2014) included a message with multiple specific causal messages such as, “highly processed foods that are high in sugar and fat are easily available and much cheaper than healthier foods” but only measured support for some of the corresponding policies, and in this case, that did not include support for either food taxes or healthy food subsidies. The mixed evidence for an effect of causal belief interventions on policy support is therefore unsurprising: we propose that causal beliefs will only influence policy support when the two correspond.
Specificity-Correspondence Theory
The argument at the core of our Specificity-Correspondence Theory is that some causal beliefs shape people’s policy attitudes, but other causal beliefs do not. Although attribution theories (Kelley & Michela, 1980) offer various dimensions of causal beliefs (e.g., dynamic vs. stable, internal vs. external, controllable vs. uncontrollable), none of these explain the conflicting results within this field. We therefore propose two new dimensions: general versus specific and corresponding versus non-corresponding, defined in Table 1.
A New Conceptual Framework for Categorising Beliefs About the Causes of a Policy Problem.
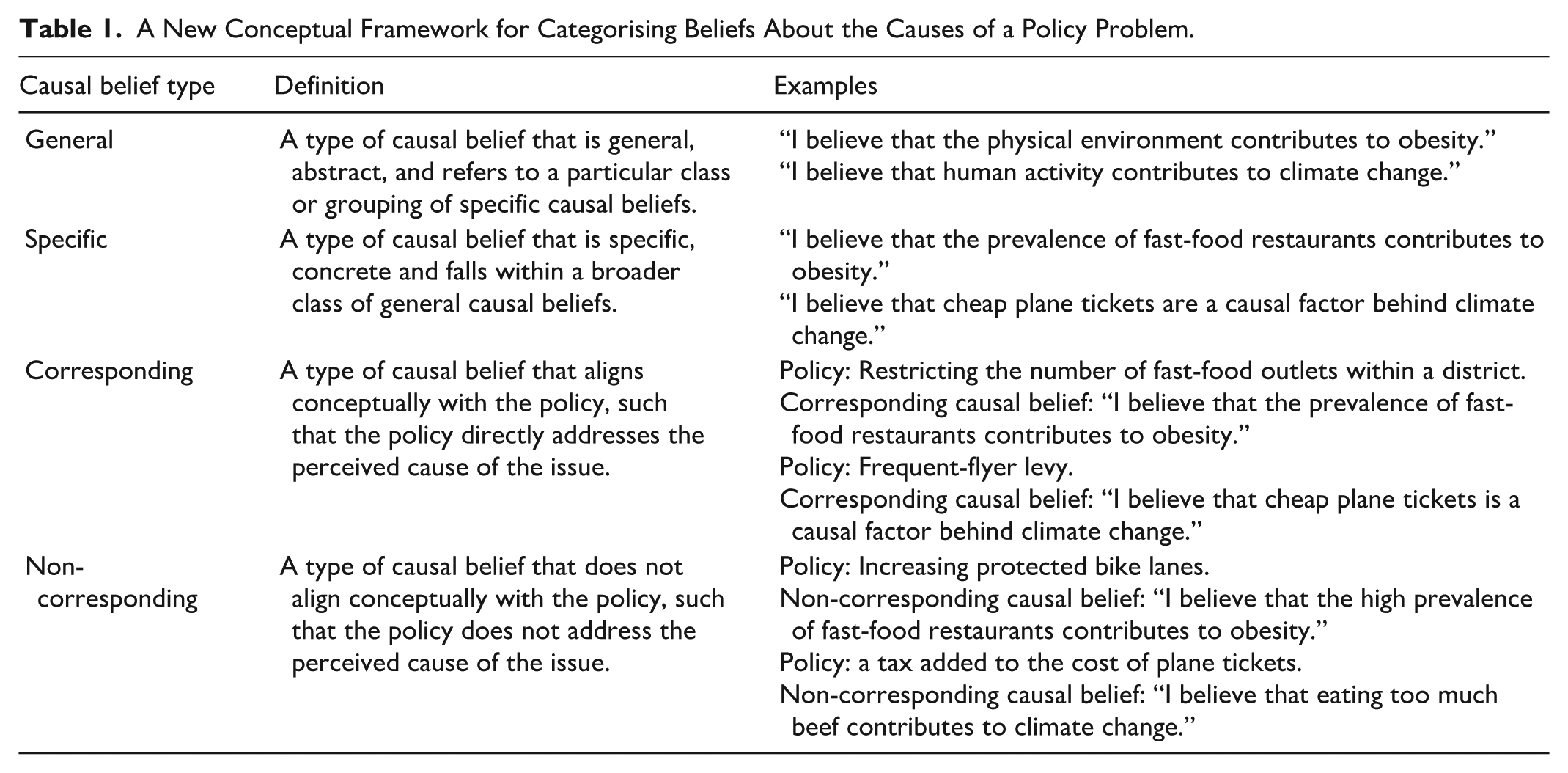
With this new conceptual framework for understanding different types of causal beliefs, we can describe the main predictions of our new theory. The first is that specific and corresponding causal beliefs have a causal influence on policy support. Conversely, specific-non-corresponding causal beliefs and general causal beliefs do not have a direct causal influence on policy support. The other main predictions of this theory – which are not the primary focus of this paper – relate to the structure of causal beliefs and are described in Supplemental Material 1.
How Beliefs About the Causes of the Policy Problem Affect Policy Support
We also propose a mechanism to explain why causal beliefs affect policy support: perceived policy effectiveness. In doing so, we integrate our theory with another modern theory of policy support: The Integrative Public-Policy-Acceptance Framework (IPAC Framework; Grelle & Hofmann, 2024; see Figure 1). In the IPAC Framework, one of the proximal determinants of policy support is the perceived effectiveness of the policy, defined as people’s beliefs about how effective a policy will be at achieving its goals. It is this construct which we propose as the mediator between specific-corresponding beliefs and policy support. The reasoning is that people may judge a policy’s effectiveness at solving an issue by how well the policy addresses the cause of the issue itself. For instance, if someone believes that one of the causes of obesity is fast-food advertising, then our theory predicts that this person is likely to believe that restricting fast-food advertising is an effective obesity-prevention policy.
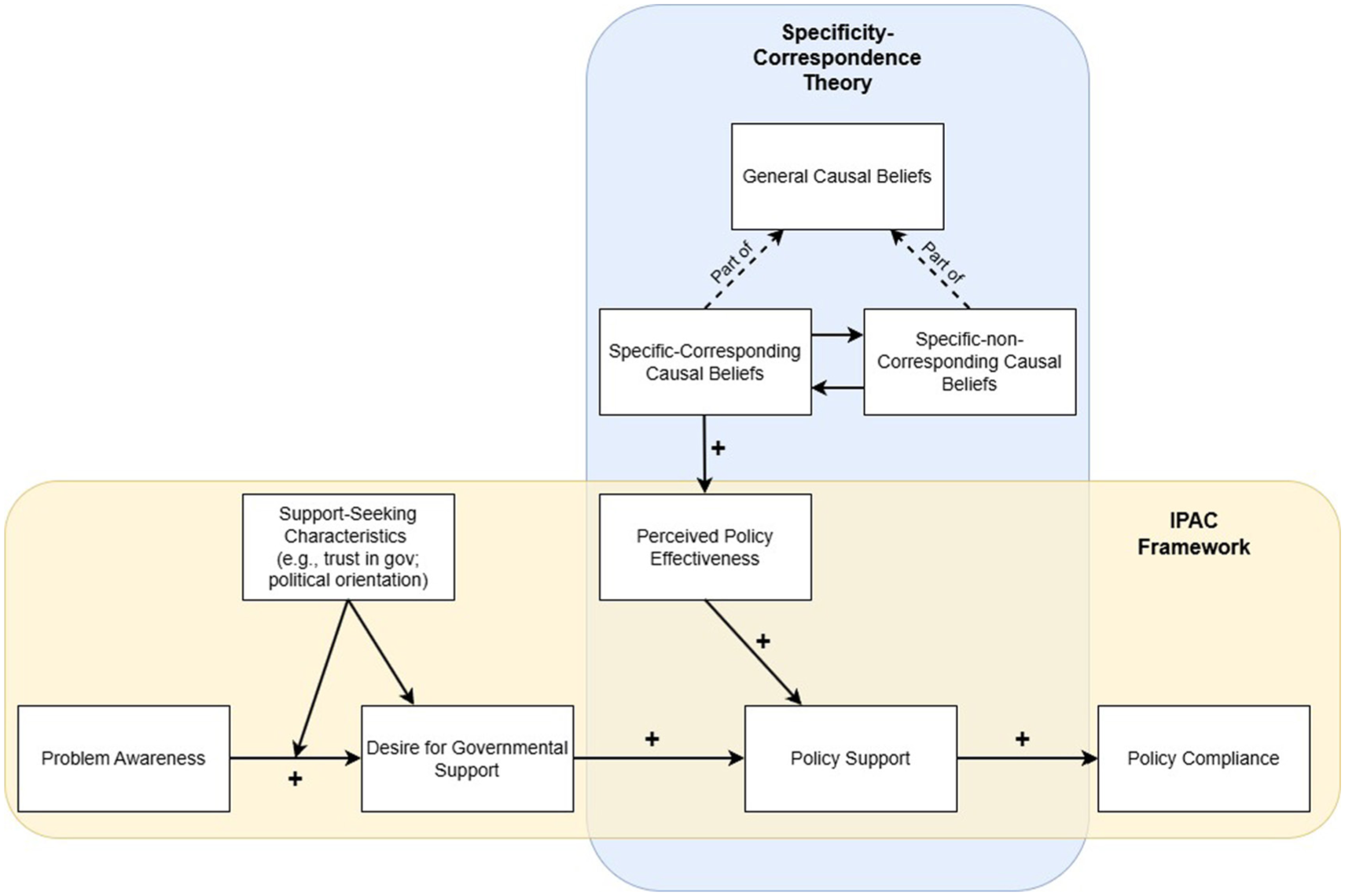
A visual representation of the integration between our Specificity-Correspondence Theory and the IPAC Framework. Note that we simplify some parts of the IPAC Framework for clarity. We use the formal theory specification tool developed by West et al. (2019) to describe our theory in this figure and Supplemental Material 1.
Research Overview
The current research includes one novel cross-sectional study, three novel experiments, secondary data analysis of three existing datasets, and an internal meta-analysis of the three experiments. To test the generalisability of Specificity-Correspondence Theory we selected one domain that has received a lot of prior research – namely, obesity – and one domain that has yet to receive any experimental investigation – namely, alcohol. Within each domain we test the theoretical predictions on multiple policies to further probe the generalisability of our theory.
Study 1
In study 1, we hypothesised that causal beliefs will be correlated with policy support and that correlations between policy support and corresponding beliefs are larger relative to correlations between policy support and non-corresponding or general causal beliefs.
Methods
The hypotheses, materials, and analysis plan were preregistered on the Open Science Framework (https://osf.io/g7pxf/overview. There were no deviations from the preregistration. We report all manipulations, measures, and exclusions in these studies. This study was approved by the College of Health and Life Sciences Research Ethics Committee at Aston University.
Participants
Five hundred one U.K. residents were recruited by MRFGR (www.mrfgr.com) in return for points that can be exchanged for prizes from the agency between 7 August 2023 and 11 August 2023. The sample was nationally representative using a quota-method based on age, sex, region, and socio-economic status (see Supplemental Material 2 for full demographic breakdown and sample size calculation). The mean age was 48.0 (SD = 17.5; min = 18, max = 92), and 51% were female. Participants were automatically screened out if they failed the attention check question.
Design and Measures
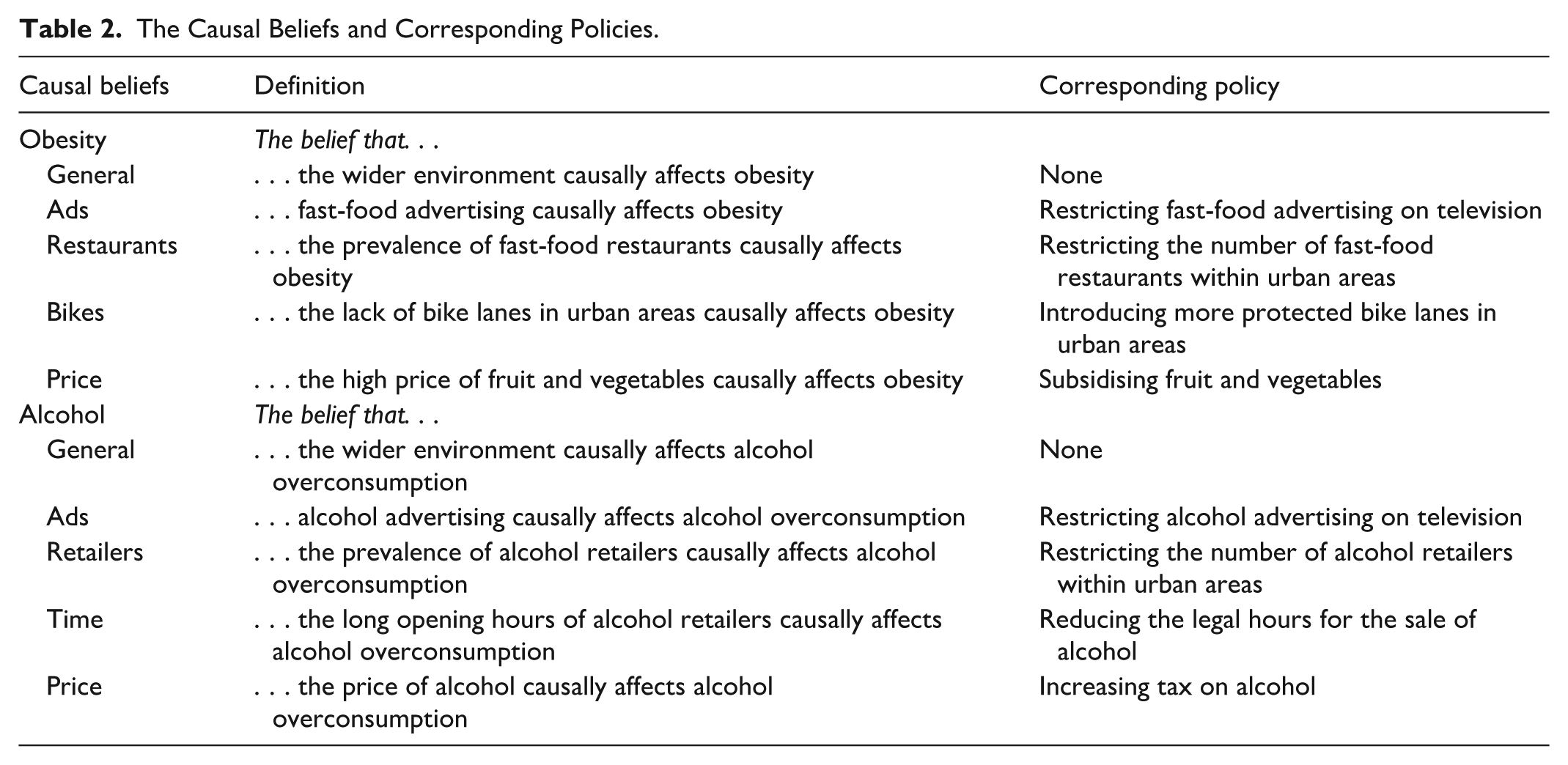
The design was a cross-sectional, observational online survey. All data, code, and materials can be found in the OSF folder (Reynolds et al., 2023). Table 2 shows all the policy and causal belief domains.
The Causal Beliefs and Corresponding Policies.
Policy Support
Policy support was defined as an attitude towards the implementation of a specific public policy. There were eight questions with a single item measuring support for each policy, each with a 7-point response scale (1 = strongly oppose, 7 = strongly support; Mantzari et al., 2022). For obesity-related policies, these were: a subsidy that reduces the price of fruit and vegetables, banning fast-food advertising on TV, increasing protected cycle lanes in city and town centres, and limiting the number of fast-food restaurants within city and town centres. For alcohol-related policies, these were: increasing alcohol tax, restricting the hours of sale of alcohol, banning alcohol advertising, and limiting the number of retailers within city and town centres.
Causal Beliefs
Causal beliefs were defined as a belief about factors that have a causal influence on a salient issue, in this case, the causes of obesity and alcohol. There were 20 items with 7-point response scales (1 = Strongly disagree, 7 = Strongly agree) adapted from previous research (Reynolds et al., 2020b). General causal beliefs were measured using two questions for the environment’s role in influencing obesity and two questions for the environment’s role in alcohol consumption (e.g., “The physical, economic, and social environment in which people live contributes to the overconsumption of alcohol”). There were 16 items measuring specific causal beliefs, two for each of the chosen eight policies (e.g., “The low price of alcohol contributes to the overconsumption of alcohol” [alcohol tax policy]; “Fast-food advertising on television contributes to the high rates of obesity” [banning fast-food advertising policy]). The Cronbach’s alpha for all causal belief item pairs ranged from .91 to .96 indicating excellent internal consistency for all variables.
Analysis
All analyses were conducted in R v4.3.1 (R Core Team, 2022). In some cases, the assumptions for Pearson’s r analyses were not met, so we conducted Spearman’s Rho correlations as the primarily analysis and Pearson’s r as a sensitivity analysis as specified in our preregistration. This is to ensure our results are robust to other plausible analytical choices (Aczel et al., 2026). Tests of correlational differences were conducted using the psych package (Revelle, 2007). Exploratory (not preregistered) OLS regression models in which all causal beliefs were entered as predictors of policy support into each model were also conducted and are reported in Supplemental Material 2. All results have been computationally reproduced by a second researcher.
Results
The correlational analyses support our hypotheses that specific causal beliefs correlate with support for the corresponding policy. Out of the eight tests (four obesity, four alcohol), all eight hypotheses were supported.
The tests of correlation differences also support the hypotheses that corresponding causal beliefs have larger correlation coefficients relative to non-corresponding causal beliefs. The statistical comparisons suggest that the correlation coefficients between policy support and corresponding causal beliefs were significantly larger than the correlation coefficients between policy support and non-corresponding causal beliefs in 19/32 analyses (coefficients numerically larger in 30/32 correlations). Table 3 shows these results.
Tests of Correlational Differences Between Policy Support and Corresponding Causal Beliefs Versus Policy Support and Non-Corresponding or General Causal Beliefs.
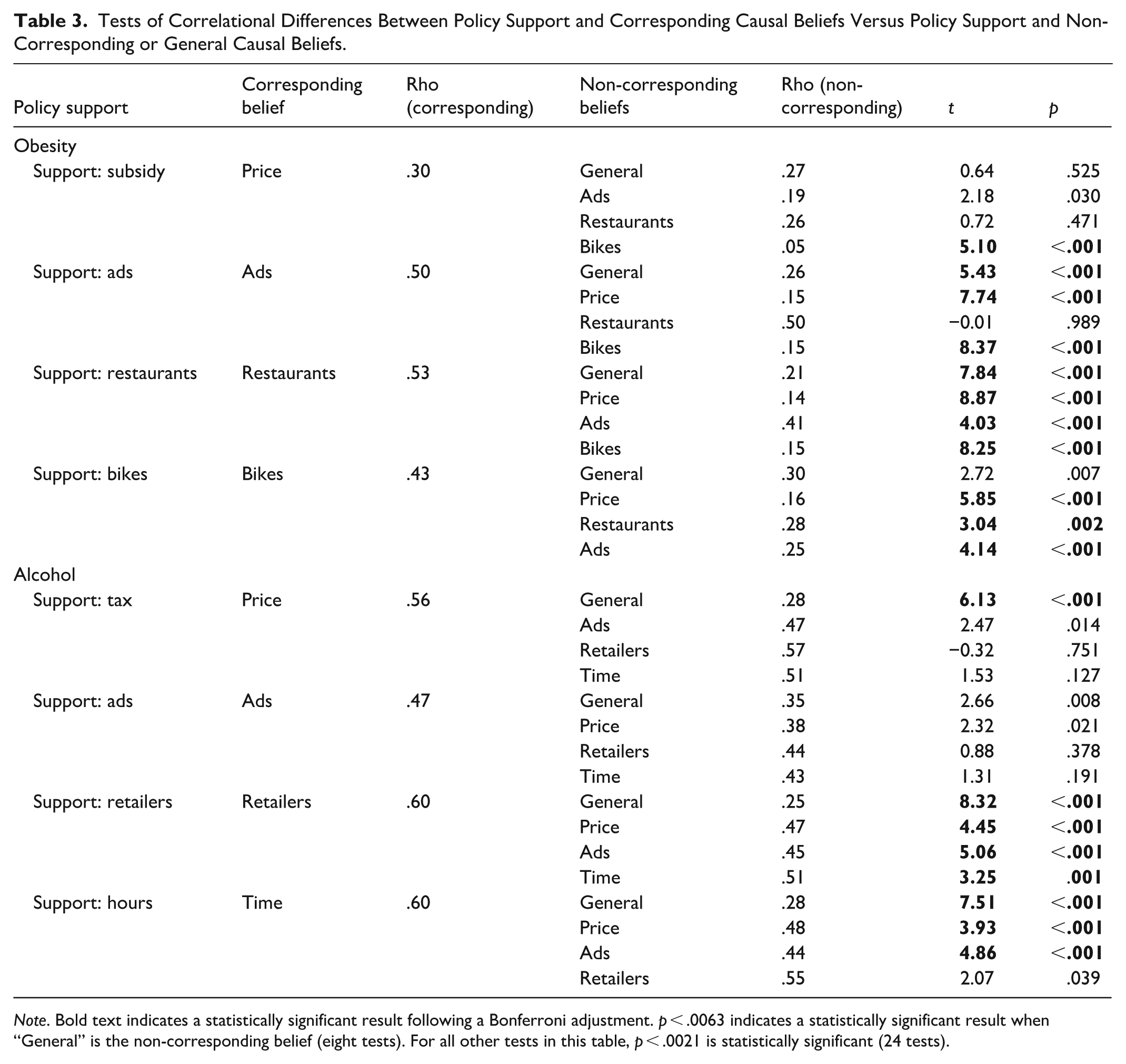
Note. Bold text indicates a statistically significant result following a Bonferroni adjustment. p < .0063 indicates a statistically significant result when “General” is the non-corresponding belief (eight tests). For all other tests in this table, p < .0021 is statistically significant (24 tests).
The sensitivity analysis using Pearson’s r instead of Spearman’s rho produced similar, but more convincing, results with 21/32 significant correlational differences, all in the predicted direction. Exploratory regression models were also tested and are reported in Supplemental Material 2, which show that corresponding causal beliefs are significant predictors after including all causal beliefs in the models 100% of the time. In comparison, 56% (18/32) of non-corresponding and general causal beliefs are significant in regression models that do not include the specific-corresponding causal belief, whereas only 34% (11/32) are significant when the specific-corresponding causal belief is included.
Discussion
These findings provide initial support for Specificity-Correspondence Theory: public support for policies is better predicted by corresponding causal beliefs than by non-corresponding causal beliefs across obesity and alcohol domains. Exploratory regression analyses suggest that many non-corresponding and general causal beliefs become non-significant predictors of policy support when corresponding beliefs are included in the model, which strengthens the evidence for this theory further. Although this study cannot demonstrate that corresponding causal beliefs causally affect policy support, the results are consistent with that interpretation. The second preregistered study aimed to address the limitations of these correlational analyses to examine whether there was experimental evidence that causal beliefs can influence policy support.
Study 2
Study 2 takes an experimental approach to addressing this paper’s central hypothesis aiming to provide stronger causal evidence for whether specific-corresponding causal beliefs affect policy support. We focus here on one policy domain – obesity – and two policies, as a preliminary test. We hypothesised that corresponding interventions (messages designed to change corresponding causal beliefs) would increase policy support but that non-corresponding and general interventions would not.
To substantiate our classification of causal beliefs, we also tested our prediction that the other two types of causal beliefs (specific-non-corresponding and general) do not influence policy support.
Method
The hypotheses, materials, and analysis plan were preregistered on the Open Science Framework (https://osf.io/pgf5w/overview). There were no deviations from the registration. We report all manipulations, measures, and exclusions in these studies. This study was approved by the College of Health and Life Sciences Research Ethics Committee at Aston University.
Participants
A total of 2,393 U.K. residents were recruited by MRFGR (www.mrfgr.com) between 5 July 2024 and 14 August 2024. The sample was approximately nationally representative using a quota-method based on age, sex, region, and socio-economic status (see Supplemental Material 3 for the full demographic breakdown and sample size calculation). The mean age was 52.8 (SD = 17; min = 18, max = 93), and 51% were female. Participants were automatically screened out if they failed the attention check question.
Design
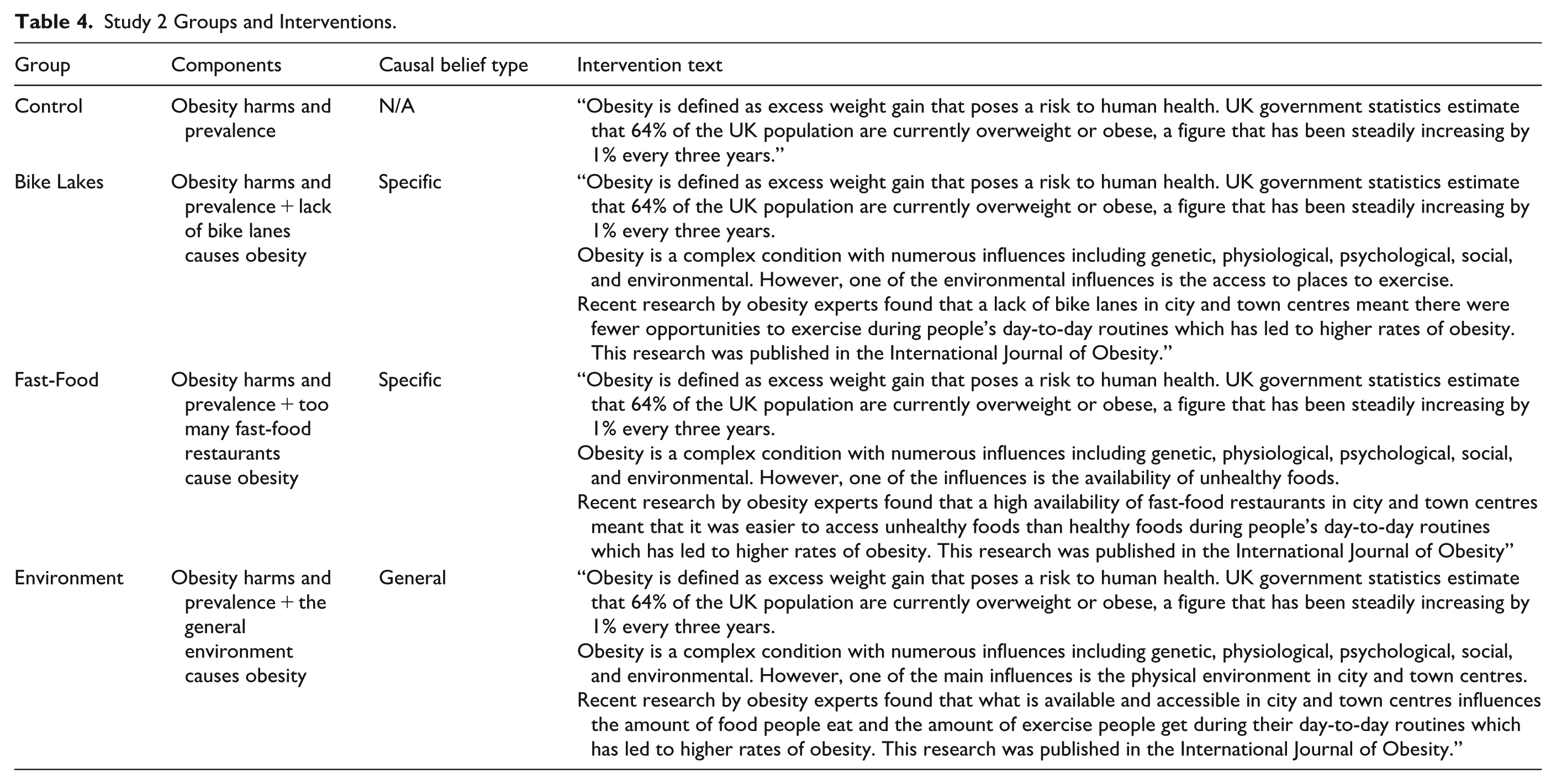
The design was a randomised pre-post experiment embedded within an online survey, specifically, a 4 (Intervention Group) × 2 (Pre-Post Measurement) mixed design. Participants were randomly allocated to one of four intervention groups using the randomisation feature in SurveyMonkey (www.surveymonkey.com). The interventions assigned to each group are detailed in Table 4 and based on similar formats used in previous research (Ortiz et al., 2016; Reynolds et al., 2020b) but altered to focus on more specific causes of obesity for the Bike Lanes and Fast-Food interventions for the two specific interventions. In all four groups, participants first received information about the harms and prevalence of obesity, followed by unique intervention messages for all groups except the control group.
Study 2 Groups and Interventions.
Measures
All measurements described below were administered twice: once before and once after the intervention/control messages. All data, code, and materials can be found in the OSF folder (Reynolds et al., 2023).
Policy Support
The co-primary outcomes of support for (a) protected bike lanes and (b) restricting the number of fast-food outlets, were created by taking the mean value from two items each (e.g., “Do you support or oppose the government increasing the number of protected bike lanes in city and town centres?”) and measured on 7-point response scales (e.g., 1 = Strongly oppose, 7 = Strongly support). The internal consistency was excellent for all four variables (αrange = .88–.96).
Causal Beliefs
The specific causal beliefs measured were that obesity is causally influenced by (a) a lack of protected cycle lanes in town and city centres, (b) the large number of fast-food restaurants in town and city centres, and the general causal belief measured was that obesity is causally influenced by (c) the physical, economic and social environment in general. Each variable was also created by taking the mean value from two items and measured on 7-point response scales (e.g., 1 = strongly disagree, 7 = strongly agree). The internal consistency was excellent for all six variables (αrange = .85–.95).
Analyses
All analyses were conducted in R v4.3.1 (R Core Team, 2022). The effect of interventions on the post-intervention measure of the outcomes was evaluated using OLS regressions in which the pre-intervention measure of the outcome was used as a covariate. The assumptions for OLS regressions including normal distribution of residuals (checked via QQ-plot and histogram of residuals) showed some minor deviations, but as regression is fairly robust to minor deviations, we kept this as the main analysis. We conducted robust regressions using a Huber M-estimator as sensitivity analyses which replicated the results from the OLS regressions. This was done using the rlm() function in the “MASS” package (Ripley et al., 2025). All results have been computationally reproduced by a second researcher.
Results
Effect of the Corresponding Interventions
There were two confirmed manipulation checks: both specific interventions significantly changed the corresponding causal belief in the predicted direction (see Table 5). One out of two tests provided support for the main preregistered hypothesis; namely, communicating evidence that restricting fast-food restaurants causes obesity significantly increased support for restricting fast-food restaurants. However, communicating evidence that a lack of bike lanes influences obesity did not change support for increasing the number of bike lanes.
The Effect of the Interventions on the Corresponding Policy Support and Causal Beliefs.
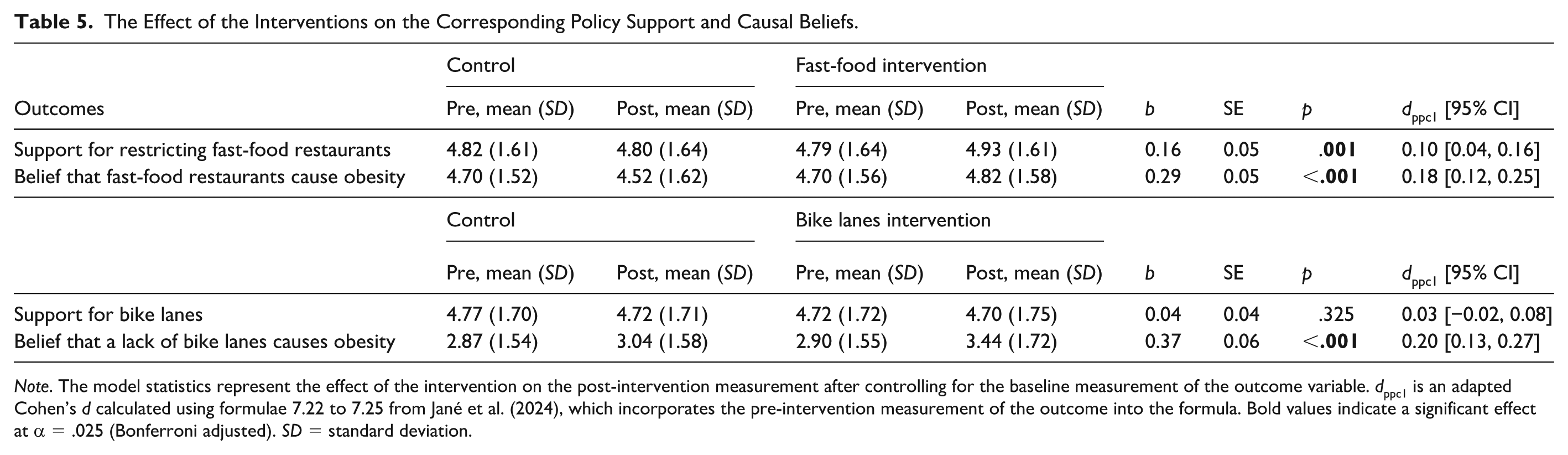
Note. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024), which incorporates the pre-intervention measurement of the outcome into the formula. Bold values indicate a significant effect at α = .025 (Bonferroni adjusted). SD = standard deviation.
Non-Corresponding and General Results
The results in Table 6 show that the two specific-non-corresponding interventions and one general environment intervention did not significantly change support for any policies, which supports our main hypotheses.
The Effect of the Interventions on the Non-Corresponding Policy Support and Causal Beliefs.
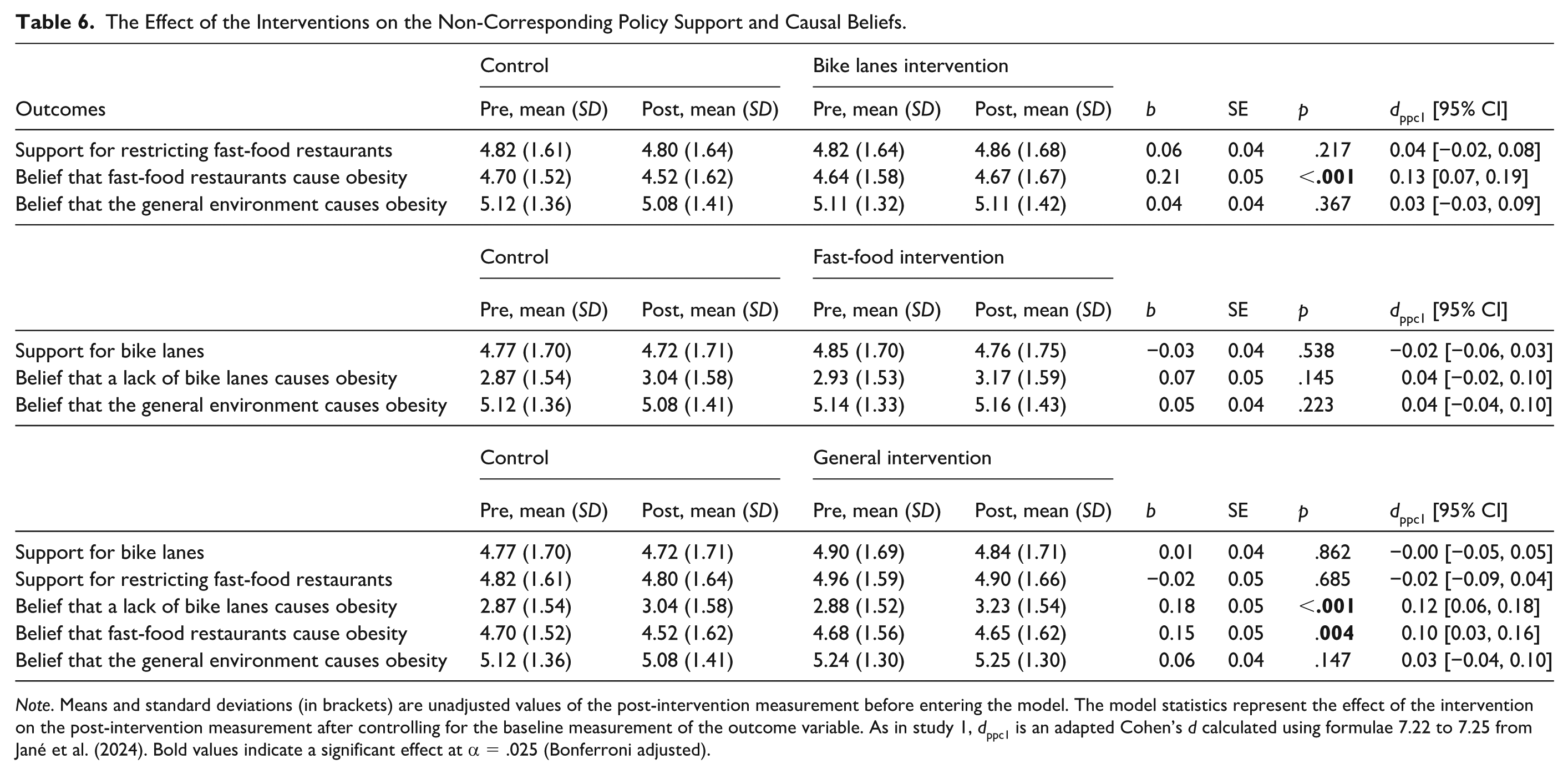
Note. Means and standard deviations (in brackets) are unadjusted values of the post-intervention measurement before entering the model. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. As in study 1, dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024). Bold values indicate a significant effect at α = .025 (Bonferroni adjusted).
These results do, however, show some significant effects of interventions on non-corresponding causal beliefs, suggestive of a cross-over effect. The bike lanes intervention significantly changed the causal belief that fast-food restaurants contribute to obesity, although the fast-food restaurant intervention did not significantly change the bike lanes causal belief. Furthermore, the general environment intervention significantly changed both bike lanes and fast-food causal beliefs but did not change general environment causal beliefs.
Discussion
Study 2 shows partial support for the hypothesis that there is a causal relationship between specific causal beliefs and support for the corresponding policy. Both of our targeted interventions were successful at changing the corresponding causal belief, however this only led to an increase in support for one policy: restricting fast-food restaurants. The bike lanes intervention did not increase support for more bike lanes. We discuss the potential reason for the null effect in the study 4 discussion and general discussion.
None of the interventions increased support for a non-corresponding policy, providing further support for Specificity-Correspondence Theory. We now turn our attention to identifying a potential mediator underlying why specific-corresponding causal beliefs may affect policy support.
Study 3
In study 2, we provide some preliminary evidence for a causal relationship between causal beliefs and policy support. In study 3, we aimed to test whether this relationship is mediated by perceived policy effectiveness by conducting exploratory secondary data analysis of three publicly available datasets from two published papers (Petrescu et al., 2016; Reynolds et al., 2018) that contain measures of: (a) causal beliefs, (b) beliefs about policy effectiveness, and (c) policy support.
Method
Participants
Two datasets are reported by Petrescu et al. (2016). The first dataset includes a sample of N = 1,093 U.K.-based participants recruited from the market research company Dynata (www.dynata.com; previously Survey Sampling International). The second includes N = 1,082 participants recruited within the USA using Amazon MTurk. A third dataset is reported by Reynolds et al. (2018), which included N = 1,648 participants recruited in the United Kingdom from the polling agency YouGov. These datasets were selected as they contain all three variables that were needed to test our hypotheses. We did not use any of the other variables from these studies. See Supplemental Tables S4.1 to S4.3 for demographic information. The analyses reported here were not conducted or reported in the original papers.
Measures
Policy Support
Policy support was measured by taking the mean score of three questions in all three datasets: (a) “Do you support or oppose this policy?” (1 = strongly oppose, 7 = strongly support), (b) “How acceptable do you find this policy?” (1 = completely unacceptable, 7 = strongly acceptable), and iii. “How much are you in favour of this policy being introduced?” (1 = strongly in favour, 7 = strongly against) with responses recorded on 7-point scales. There were five policies included in the two datasets published by Petrescu et al. (2016), each targeting sugar sweetened beverages (SSBs): reducing portion sizes, changing the shape of the drink containers, changing their shelf location in stores, increasing taxation on SSBs, and a health education campaign about the harms of SSBs. There was one policy included in the dataset published by Reynolds et al. (2018): a tax on sweets and confectionary.
Causal Beliefs
One environmental causal belief was measured in the Petrescu et al. (2016) paper with a single item on a 7-point scale, “People are overweight because there are so many unhealthy foods around.” One environmental causal belief was measured in Reynolds et al. (2018) by taking the mean of two items: “People are obese because there are so many unhealthy foods around” and “The availability of unhealthy foods is to blame for the high rates of obesity” both on a 7-point scale (1 = strongly disagree, 7 = strongly agree).
Effectiveness Beliefs
Beliefs about the effectiveness of the policy at reducing obesity in Petrescu et al. (2016) were measured with a single item: “How effective do you think this policy will be?” on a 7-point scale (response labels not provided).
Beliefs about the effectiveness of the policy at reducing obesity in Reynolds et al. (2018) was measured by taking the mean of two items: “The new chocolate and sweet tax will reduce obesity among children” and “The new chocolate and sweet tax will help solve England’s problem with obese children” both on a 7-point scale (1 = strongly disagree, 7 = strongly agree).
Analysis
Mediation analyses were conducted using the Mediation package (Tingley et al., 2014) within R v4.3.1. In total, there were 11 mediation models tested, 1 for each policy, with 5 policies in each of the 2 Petrescu et al. (2016) datasets and 1 policy in the Reynolds et al. (2018) dataset. In these models, X = causal beliefs, M = effectiveness beliefs, and Y = policy support. Due to the multiple testing of the same hypothesis, a Bonferroni adjustment was applied, resulting in α = .0045. All results have been computationally reproduced by a second researcher.
Results
There were significant mediation effects (average causal mediation effect) in all 11 mediation models (all p < .001), and all had medium-to-large effect sizes. On average, 50% (range: 27%–68%) of the relationship between environmental causal beliefs and support for obesity policies was accounted for by beliefs about policy effectiveness. The full results from are presented in the Supplemental Table S4.4. One model for illustration is presented below in Table 7.
Mediation Model Testing Whether Beliefs About Policy Effectiveness Mediates the Relationship Between Causal Beliefs and Policy Support.
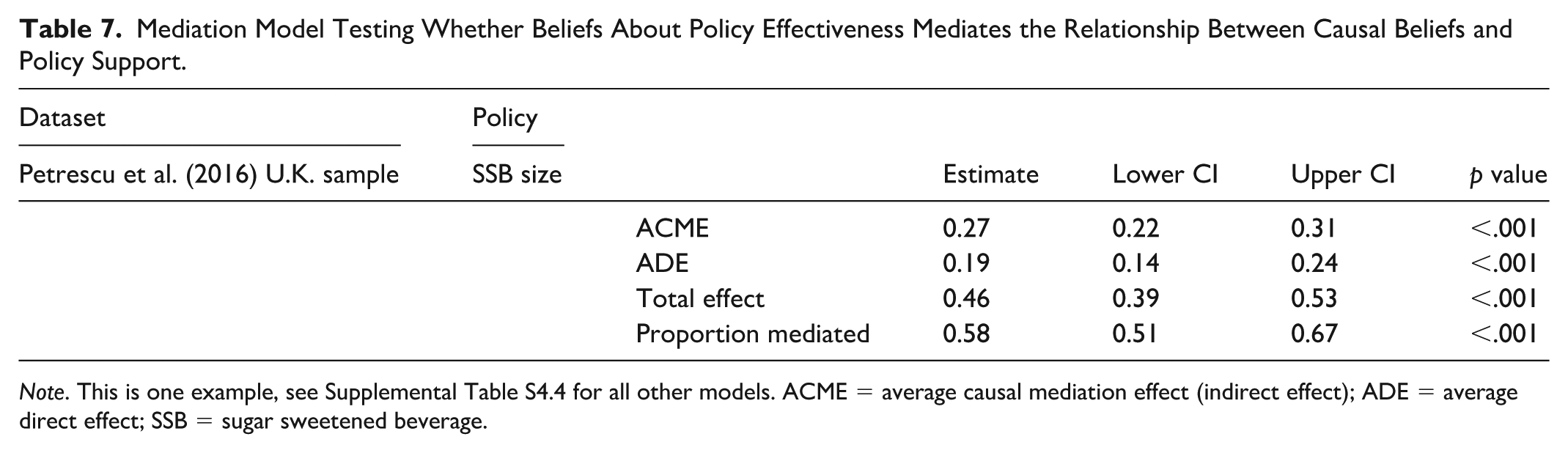
Note. This is one example, see Supplemental Table S4.4 for all other models. ACME = average causal mediation effect (indirect effect); ADE = average direct effect; SSB = sugar sweetened beverage.
Discussion
This secondary data analysis shows that perceived effectiveness is a significant mediator explaining – on average – 50% of the relationship between causal beliefs and policy support. This result is particularly convincing given the replicability of the result across all 11 models with a conservative alpha adjustment, the generalisability of the model across 6 policies, 2 countries, and 3 samples, and the strength of the mediation effect.
While this result is clearly robust, the interpretation of this result should not be overstated. There are numerous limitations to conducting mediation on observational data (Pirlott & MacKinnon, 2016); namely that the results do not demonstrate whether X has a causal effect on M and whether M has a causal effect on Y. In studies 4a and 4b, we aim to address the first of these limitations.
Studies 4a and 4b
Studies 4a and 4b are replications and extensions of studies 2 and 3. The replication element involves testing the replicability of the intervention that successfully changed policy support in Study 2. The extension element involves firstly examining if the result generalises to new policies and domains, with one new obesity policy (restricting fast-food advertising) and two new alcohol policies (restricting hours of alcohol sales, restricting the number of alcohol retailers). Furthermore, we address some of the limitations of the mediation models in study 3 by testing for a causal effect of causal beliefs on the hypothesised mediator (perceived policy effectiveness).
As in study 2, we hypothesised that specific and corresponding interventions would significantly increase policy support but that non-corresponding ones would not. We also hypothesised that the effect of the corresponding interventions on obesity policy support would be mediated by perceived policy effectiveness.
Method
The hypotheses, materials, and analysis plan were preregistered on the Open Science Framework (https://osf.io/8gw5j/overview). There were no deviations from the registration. We report all manipulations, measures, and exclusions in these studies. This study was approved by the College of Health and Life Sciences Research Ethics Committee at Aston University.
Participants
A total of 4,011 U.K. residents (4a obesity: N = 2,010; 4b alcohol: N = 2,001) were recruited by OnePoll (www.onepoll.com) and were rewarded with points which can be claimed back for monetary rewards. Data collection for both occurred between 21 May 2025 and 30 May 2025. The points in this study were equivalent to approximately £1. The sample was approximately nationally representative using a quota-method based on age, sex, and region (see Supplemental Material 5 for full demographic breakdown and sample size calculation). Participants were automatically screened out if they failed the attention check question.
Design
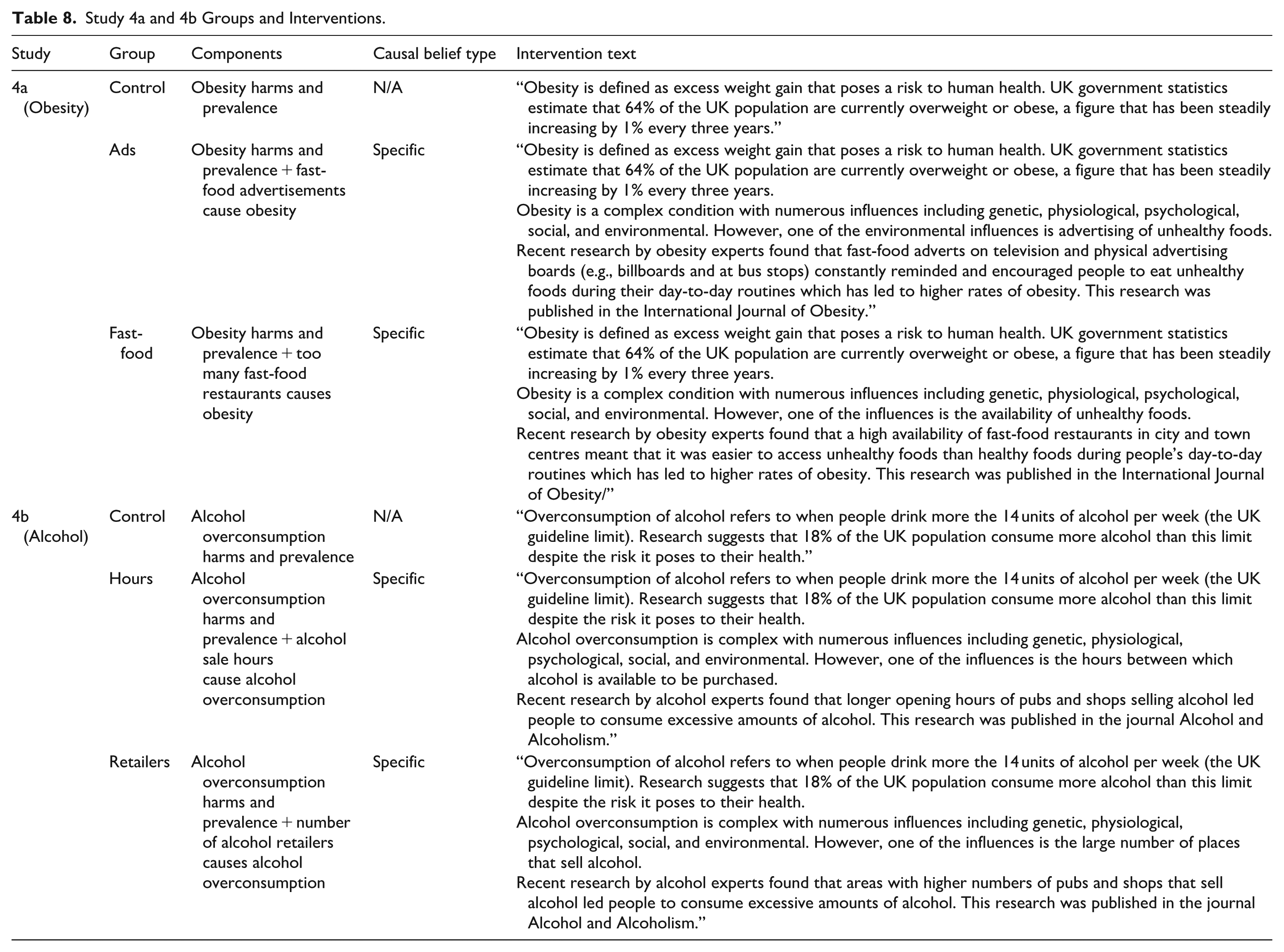
The designs used in Studies 4a and 4b were randomised pre-post experiments embedded within online surveys; specifically, 3 (Intervention Group) × 2 (Pre-Post Measurement) mixed designs. Participants were randomly allocated to one of three groups in each sub-study using the randomisation feature in SurveyMonkey (www.surveymonkey.com). The six groups and interventions are summarised in Table 8 and were similar to study 2 but adapted to focus on different policies. In all six groups, participants received information about the harms and prevalence of obesity (4a) or alcohol overconsumption (4b), followed by unique intervention messages for all groups except the control group. The core variables were measured before and after the intervention messages.
Study 4a and 4b Groups and Interventions.
Measures
All measurements described below were measured twice: once before the intervention and once after. All data, code, and materials can be found in in the OSF folder (Reynolds et al., 2023).
Policy Support
The co-primary outcomes for Study 4a were support for (a) restricting fast-food advertisements and (b) restricting the number of fast-food outlets. For 4b, it was support for (a) restricting alcohol retailer hours of sale and (b) the number of alcohol retailers in cities and towns. These variables were created by taking the mean value from two items each measured on 7-point response scales (e.g., 1 = strongly oppose, 7 = strongly support). The internal consistency was excellent for these variables (αrange = .95–.97).
Policy Effectiveness Beliefs
The hypothesised mediator – beliefs about the effectiveness of the four policies – was measured with a single item, each with a 7-point response scale.
Causal Beliefs
Beliefs about the causes of obesity/alcohol overconsumption were measured as a manipulation check. For study 4a, this included the belief that obesity is causally influenced by (a) too many fast-food advertisements and (b) the large number of fast-food restaurants in town and city centres. For Study 4b, this included the belief that alcohol overconsumption is influenced by (a) the hours that alcohol retailers can sell alcohol, and (b) the number of alcohol retailers in towns and city centres. Each variable was also created by taking the mean value from two items each (e.g., “The large number of fast-food restaurants in town and city centres contributes to the high rates of obesity”) and measured on 7-point response scales (e.g., 1 = strongly disagree, 7 = strongly agree). The internal consistency was excellent for all variables (αrange = .92–.97).
Analyses
All analyses were conducted in R v4.3.1 (R Core Team, 2022). The effect of interventions on the post-intervention measure of the outcomes was evaluated using OLS regressions in which the pre-intervention measure of the outcome was used as a covariate. The assumptions for OLS regressions including normal distribution of residuals (checked via QQ-plot and histogram of residuals) showed some minor deviations, but as regression is fairly robust to minor deviations, we kept this as the main analysis. We conducted robust regressions using a Huber M-estimator as sensitivity analyses which replicated the results from the OLS regressions. This was done using the rlm() function in the “MASS” package (Ripley et al., 2025). All results have been computationally reproduced by a second researcher.
Results
Corresponding Results
There were three out of four confirmed manipulation checks; three specific interventions changed their corresponding causal belief however the fast-food restaurant intervention did not (see Tables 9 and 10). These three interventions also significantly strengthened the belief that the policy would be effective.
The Effect of the Obesity Interventions on the Corresponding Policy Support, Causal Beliefs, and Effectiveness Beliefs.
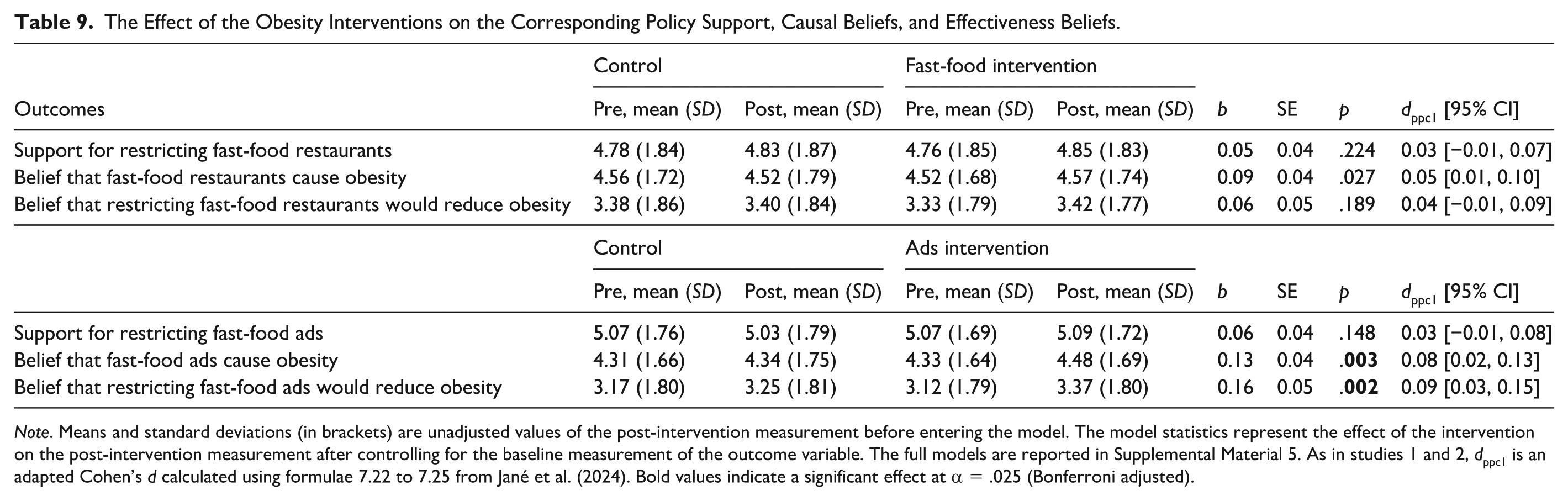
Note. Means and standard deviations (in brackets) are unadjusted values of the post-intervention measurement before entering the model. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. The full models are reported in Supplemental Material 5. As in studies 1 and 2, dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024). Bold values indicate a significant effect at α = .025 (Bonferroni adjusted).
The Effect of the Alcohol Interventions on the Corresponding Policy Support, Causal Beliefs, and Effectiveness Beliefs.
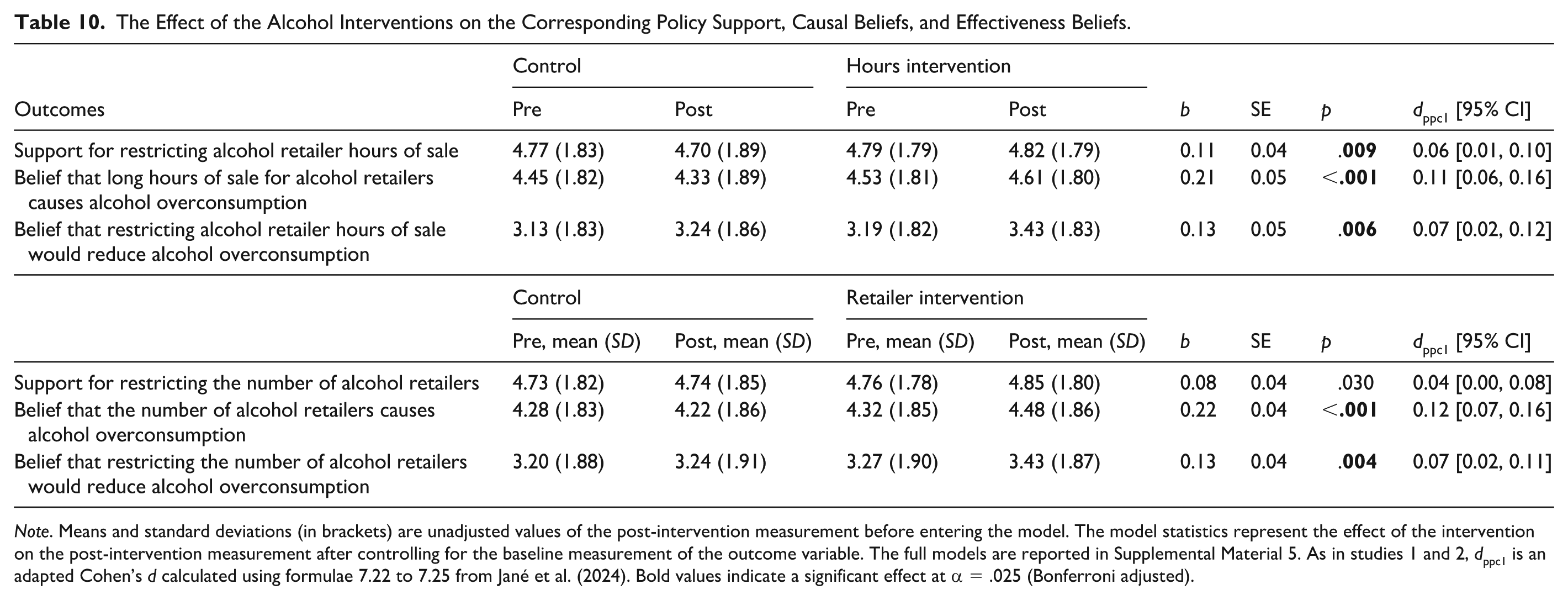
Note. Means and standard deviations (in brackets) are unadjusted values of the post-intervention measurement before entering the model. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. The full models are reported in Supplemental Material 5. As in studies 1 and 2, dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024). Bold values indicate a significant effect at α = .025 (Bonferroni adjusted).
Only one intervention increased support for the corresponding policy after the Bonferroni adjustment. This intervention was the message communicating that the number of alcohol retailers is a cause of alcohol overconsumption.
Mediation Results
Four mediation models were tested to evaluate the model: corresponding causal belief [intervention] → beliefs about policy effectiveness → policy support. Three out of four mediation models showed significant indirect effects, and these were the same three interventions that successfully changed causal beliefs and beliefs about policy effectiveness: fast-food advertising (Study 4a), alcohol hours, and alcohol retailers (both 4b). The effect sizes were large for the three significant models, suggesting that 63% (ads), 38% (hours) and 42% (retailer) of the effect was mediated by beliefs about policy effectiveness (48% on average). The confidence intervals were large – suggesting uncertainty in the proportion mediated. Collectively, this provides support for the hypothesis that beliefs about policy effectiveness mediate the relationship between causal beliefs and policy support. Table 11 summarises these results.
Results of the Four Mediation Models Testing Whether Effectiveness Beliefs Mediate the Relationship Between Causal Belief Interventions and Policy Support.
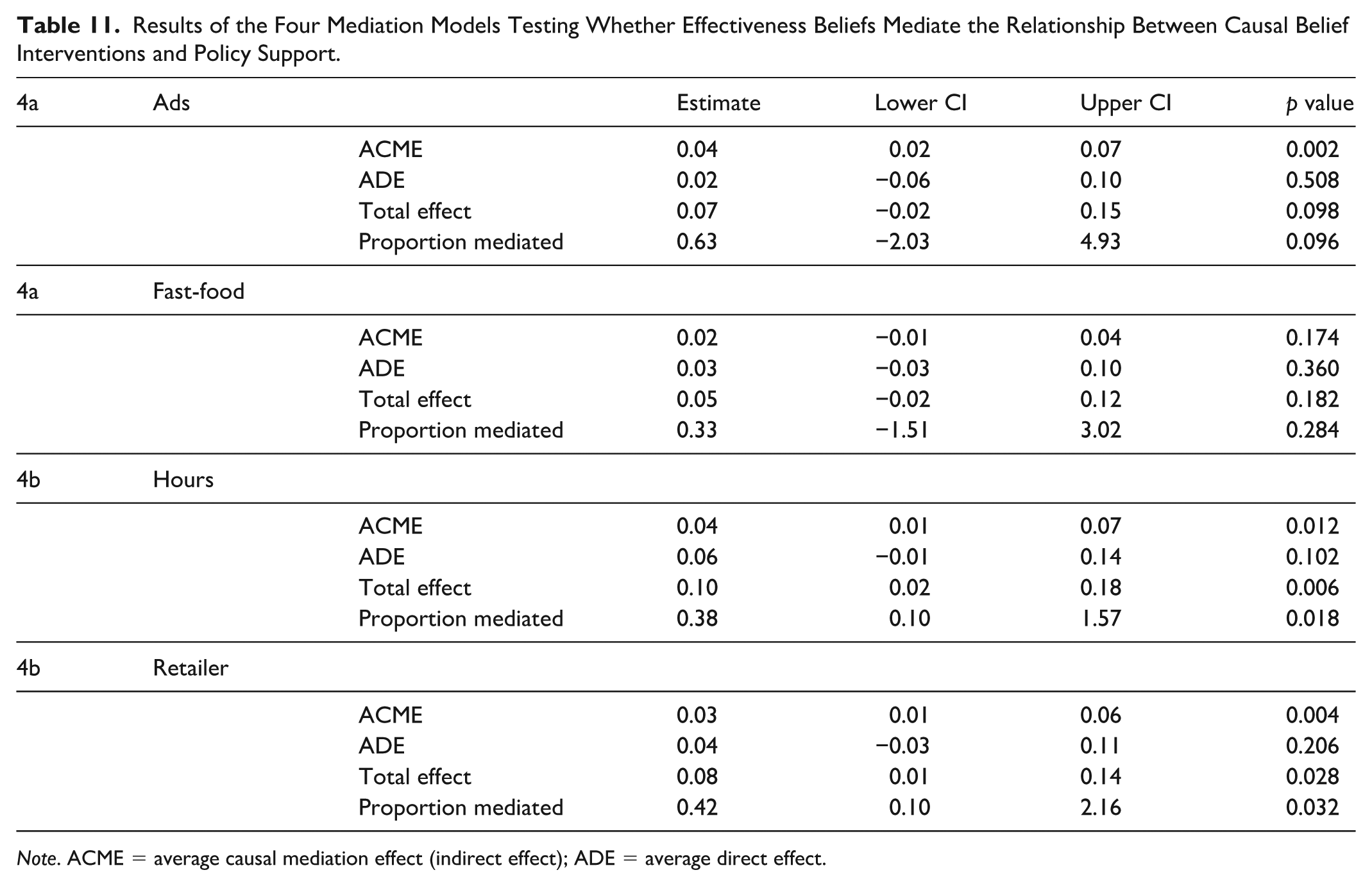
Note. ACME = average causal mediation effect (indirect effect); ADE = average direct effect.
Non-Corresponding Results
The results in Tables 12 and 13 show that none of the four non-corresponding interventions changed support for any policies which supports our main hypothesis.
The Effect of the Obesity Interventions on the Non-Corresponding Policy Support, Causal Beliefs, and Effectiveness Beliefs.
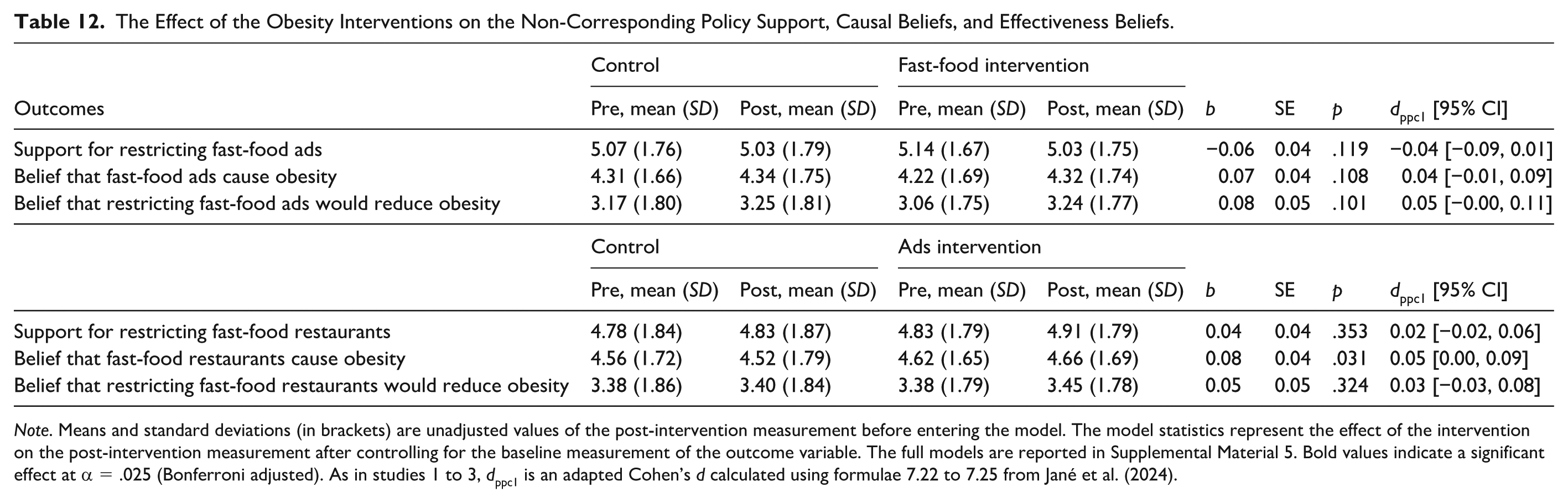
Note. Means and standard deviations (in brackets) are unadjusted values of the post-intervention measurement before entering the model. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. The full models are reported in Supplemental Material 5. Bold values indicate a significant effect at α = .025 (Bonferroni adjusted). As in studies 1 to 3, dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024).
The Effect of the Alcohol Interventions on the Non-Corresponding Policy Support, Causal Beliefs, and Effectiveness Beliefs.
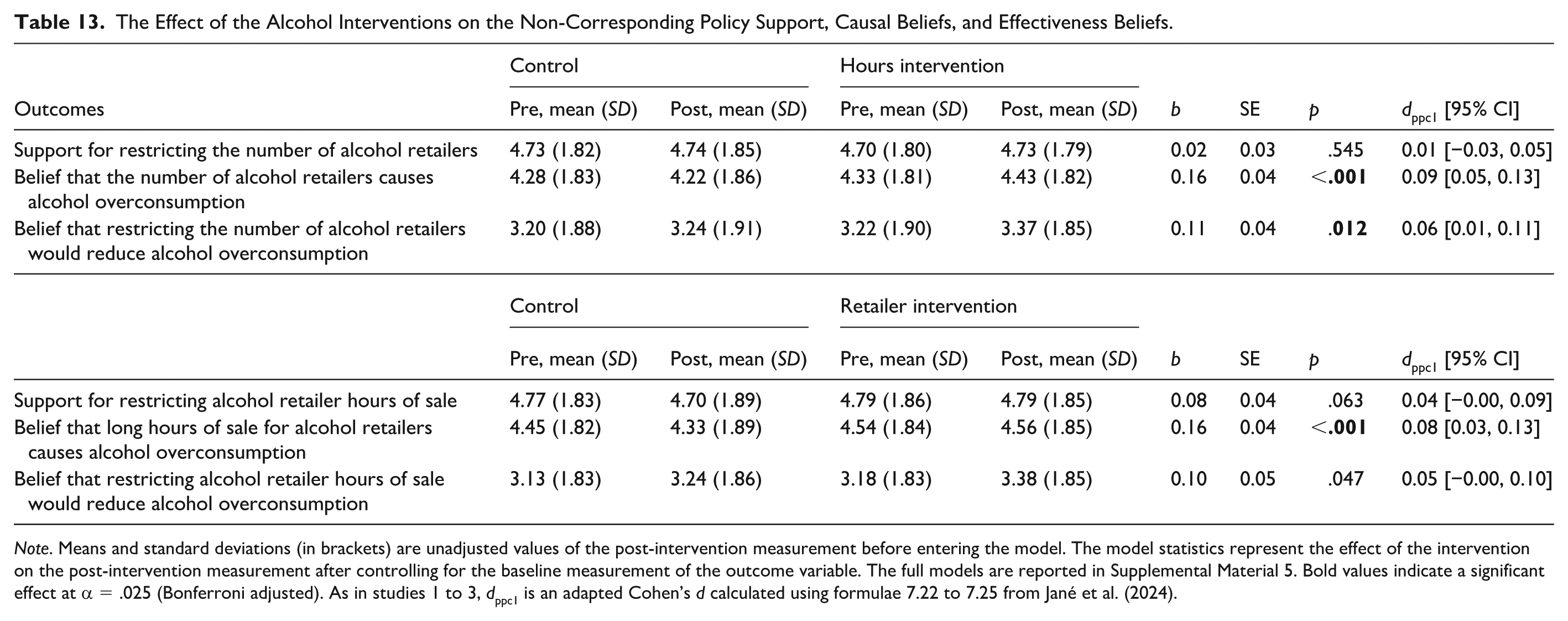
Note. Means and standard deviations (in brackets) are unadjusted values of the post-intervention measurement before entering the model. The model statistics represent the effect of the intervention on the post-intervention measurement after controlling for the baseline measurement of the outcome variable. The full models are reported in Supplemental Material 5. Bold values indicate a significant effect at α = .025 (Bonferroni adjusted). As in studies 1 to 3, dppc1 is an adapted Cohen’s d calculated using formulae 7.22 to 7.25 from Jané et al. (2024).
These results do, however, show some significant effects of the interventions on non-corresponding beliefs. Both alcohol interventions changed the non-corresponding causal belief, with one – the hours intervention – also changing the non-corresponding belief about policy effectiveness. None of the obesity interventions changed any non-corresponding belief or policy support.
Discussion
The results of study 4 show partial support for the central hypotheses that to change policy support, specificity and correspondence of causal belief interventions is required. One out of four of the specific and corresponding causal belief interventions successfully increased support for the corresponding policy, but no interventions changed support for the non-corresponding policy. Although this is consistent with our theory regarding the importance of correspondence between interventions and policies, three out of four of the interventions did not significantly increase support. This suggests either that the results do not generalise well or that there are other factors that determine the causal effect of causal beliefs on policy support. The likely explanation for this is the challenge of changing causal beliefs (see Reynolds et al., 2022). Three out of four interventions strengthened the corresponding causal beliefs and effectiveness beliefs; however, the associated effect sizes were very small. If the degree of belief change was larger, we might expect to see greater changes in policy support. To more reliably detect effects of this size, either larger sample sizes or meta-analyses are needed.
The mediation analyses provide strong support our hypotheses, with three out of four mediation models (the same three interventions that successfully changed the corresponding causal beliefs) showing significant mediation pathways from X (causal belief intervention) to Y (policy support) via M (beliefs about policy effectiveness). The effect sizes were large with 48% of the relationship between causal beliefs interventions and policy support being mediated by beliefs about policy effectiveness.
Study 5
We finally report the results of an exploratory internal meta-analyses which synthesise the experiments reported in this paper. This also provides additional statistical power, which is needed due to the small effect sizes that likely reflect the challenges in changing causal beliefs using interventions.
Method
Meta-analyses were conducted to quantitatively synthesise the experimental results across studies 2, 4a and 4b. Studies 1 and 3 were too dissimilar in design and measures to be eligible for inclusion. We provide the overall summary effect as well as breaking down the results by key subgroups: specific-corresponding, specific-non-corresponding, and general interventions. Meta-regressions were used to test whether these different subgroups are significantly different from each other. All analyses were conducted in R v4.3.1 (R Core Team, 2022) using the Metafor package (Viechtbauer, 2010). All results have been computationally reproduced by a second researcher.
In line with Cochrane guidance (Higgins et al., 2019), the sample size for the control group and general environment group was divided by two for each analysis to avoid violating the assumption of independence of observations. This ensures that when the estimates are used twice in each meta-analysis, it does not incorrectly assume that these sample sizes were larger than they were.
Results
Policy Support
In line with our theory, interventions containing evidence about specific-corresponding causal factors led to greater support for policies relative to the control groups in a random effects meta-analysis, d = 0.04, 95% CI [0.02, 0.07], p < .001, k = 6, N = 5,809 (see Figure 2). Furthermore, the meta-regression testing whether intervention type (specific-corresponding vs. specific-non-corresponding vs. general) moderated the overall effect was statistically significant, QM(df = 2) = 6.18, p = .046.
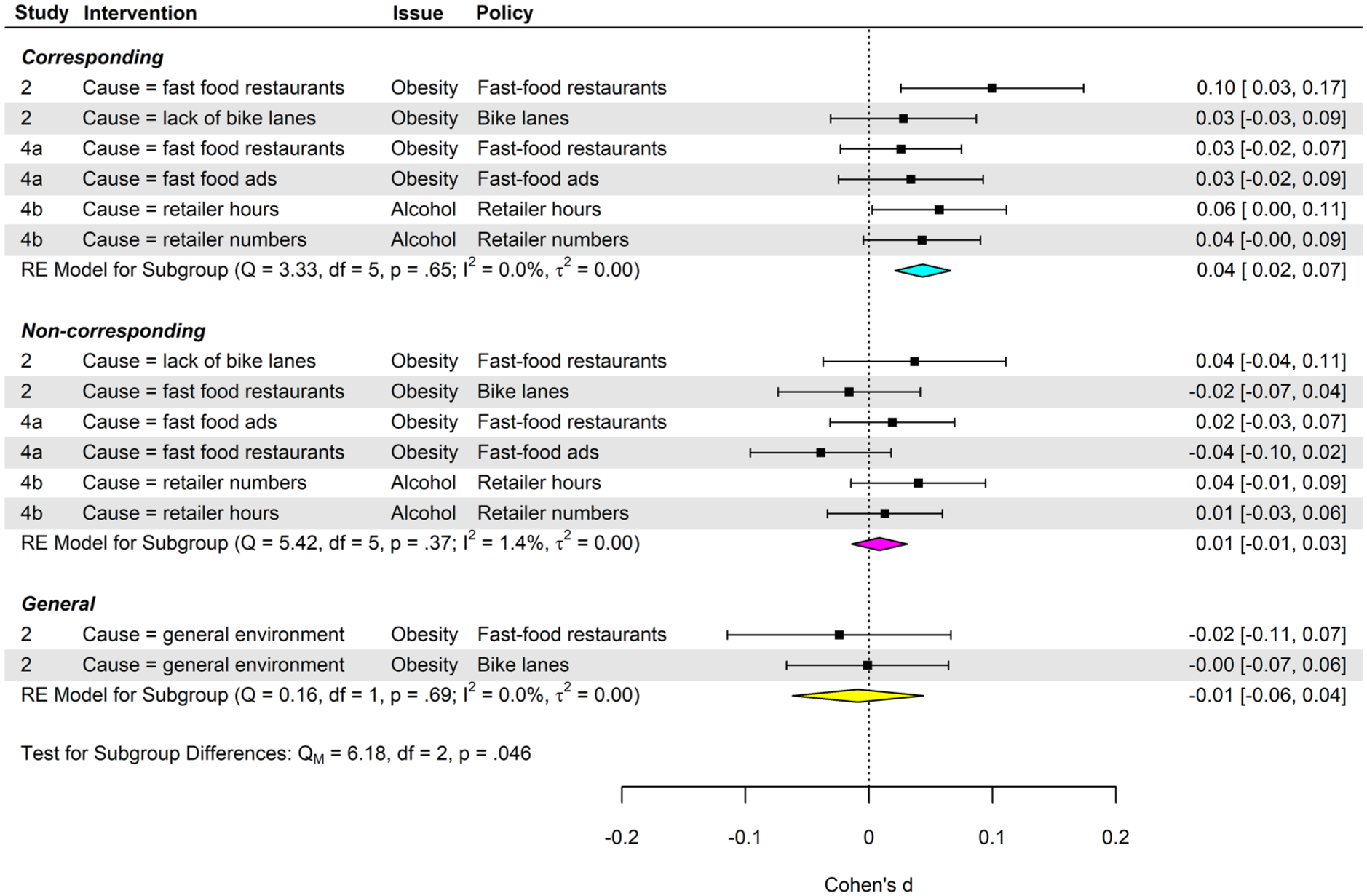
Forest plot by subgroup; the effect of interventions on policy support.
Also supporting our theory, neither specific-non-corresponding interventions nor general causal interventions changed policy support in a random effects meta-analysis, d = 0.01, 95% CI [−0.01, 0.03], p = .463, k = 6, N = 5,809 and SMD = −0.01 [−0.06, 0.04], p = .742, k = 2, N = 1,197, respectively (see Figure 3). These meta-analyses provide support for our Specificity-Correspondence Theory.
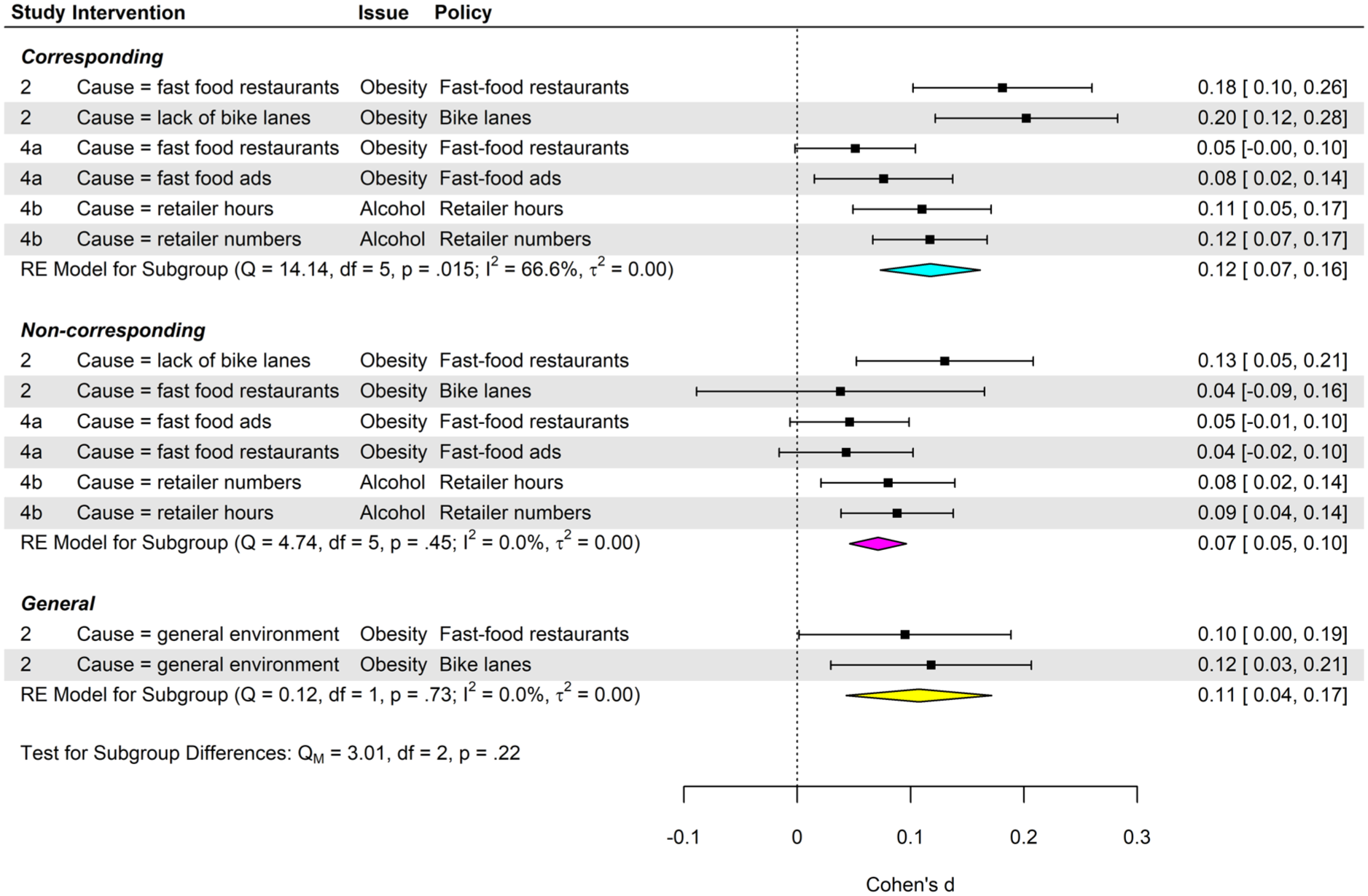
Forest plot by subgroup; the effect of interventions on causal beliefs.
Discussion
The results of these meta-analyses provide support for Specificity-Correspondence Theory: the specific-corresponding interventions significantly increased policy support whereas specific-non-corresponding and general interventions did not. Although the specific-corresponding interventions changed the targeted causal beliefs the most, there were no statistically significant differences with specific-non-corresponding nor general interventions.
General Discussion
The studies presented in this paper test several claims for our proposed Specificity-Correspondence Theory that can explain previous conflicting and inconsistent findings relating to whether people’s beliefs about the causes of a societal issue influence their attitudes towards government policies that aim to tackle that issue. The central claims of this theory are that, for any given policy, there is a distinction between different types of causal beliefs and that only one of these types of causal beliefs has a causal effect on support for that policy. We integrated this theory to extend the IPAC Framework (Grelle & Hofmann, 2024) by identifying one psychological mechanism – beliefs about policy effectiveness – that explain how and why any specific-corresponding causal belief affects policy support. We summarise the evidence for these three claims below.
Do Corresponding Causal Beliefs Affect Policy Support?
The main prediction of Specificity-Correspondence Theory is that specific-corresponding causal beliefs influence policy support, but that specific-non-corresponding and general causal beliefs do not. The correlational evidence reported in study 1 provided initial support for this claim, specifically that relationships between policy support and specific-corresponding causal beliefs are stronger than with specific-non-corresponding and general causal beliefs. The exploratory regression analyses provide additional evidence in support for this prediction of the theory by showing that most specific-non-corresponding and general causal beliefs are no longer significant predictors of policy support after controlling for specific-corresponding causal beliefs.
Subsequent experimental evidence targeting causal beliefs strongly supports our theoretical claim that specific-non-corresponding and general causal interventions do not affect policy support. This was clear in studies 2, 4a, and 4b where none of these interventions changed policy support, and this was then confirmed by the meta-analysis. These findings provide one explanation for why experiments across multiple policy domains that communicate causal belief interventions fail to increase support for policies (Jang, 2013; Myers et al., 2023; Reynolds et al., 2022), Namely, that these studies conflate different types of interventions by including some that we classify as specific-non-corresponding and some we classify as general.
The most important tests of our theory are whether interventions that contain information about the causes of a societal issue can increase support for the corresponding policy. We find partial support for this claim across studies 2 and 4b. Although only two out of six of the interventions we tested had statistically significant effects on policy support after the Bonferroni adjustment, the meta-analysis shows that there was an effect on average, yet at a smaller magnitude than we expected. The challenge that we identified here – reported previously in the systematic review of causal belief interventions (Reynolds et al., 2022) – is that it is difficult to change people’s causal beliefs sufficiently to engender substantial change in policy support. The meta-analytic summary effect sizes suggest that changing causal beliefs by d = 0.12 yielded a change in policy support of d = 0.04. While this does provide evidence that changing corresponding beliefs changes policy support, the effect size on policy support is approximately half the magnitude of what is currently considered useful in applied contexts such as policy communication strategies (World Health Organization, 2024). However, we argue that this is theoretically and practically meaningful. There is clearly a causal link, and if such interventions are combined with methods that have been effective with other messages (such as repeatedly exposing people to the same message; Fazio & Sherry, 2020; Fazio et al., 2022) then we may see an increase in the degree of change in causal beliefs, which may in turn have larger effects on policy support. In other contexts, where people do not have such firmly rooted causal beliefs, we also predict the effects will be larger.
On the surface, the results reported here seemingly support the overall conclusions of many correlational studies (Bostrom et al., 2012; Crandall et al., 2001; Genschow et al., 2017; Linos & West, 2003; Martin et al., 2000; Mazzocchi et al., 2015; Whitehead, 2014; Zucker & Weiner, 1993) and some individual experiments (Jang, 2013; Ortiz et al., 2016; Pearl & Lebowitz, 2014) but contradict the results of the systematic review (Reynolds et al., 2022). The reality is more complex. We argue that previously published significant correlations between causal beliefs and policy support likely reflect a confounding effect. Whereby the correlations between often measured general causal beliefs and policy support are explained by both variables being highly correlated with the specific-corresponding causal beliefs, which explains the relationship. There is a similar story with the experimental data. Our results imply that any interventions containing information about the general or non-corresponding causes of a societal issue only change policy support by indirectly changing specific-corresponding causal beliefs.
How Do Causal Beliefs Affect Policy Support?
The next claim that we sought to test was whether corresponding causal beliefs affect policy support by changing beliefs about policy effectiveness. This theoretically derived psychological mechanism was informed by the recent IPAC Framework, which proposes perceived policy effectiveness as a proximal determinant of policy support (Grelle & Hofmann, 2024).
We find strong support for this claim across Studies 3, 4a, and 4b. In study 3, which involved secondary data analysis of 3 publicly available datasets, we find significant indirect effects in all 11 tested models with large effect sizes: on average, 50% of the relationship was accounted for by the mediator. In two experiments in Studies 4a and 4b, we found evidence for a significant indirect effect in the 3/4 of models also with large effect sizes – 48% explained by the mediator. Crucially, this approach extends study 3’s cross-sectional design by providing novel causal evidence that corresponding causal beliefs (X) affect policy effectiveness (M)
The main limitation of the mediation models tested in studies 4a and 4b is that there was not a randomisation of the mediator to test whether policy effectiveness beliefs had a causal effect on policy support. However, this is one of the most replicable effects already identified in this field (Mantzari et al., 2022; for review, see: Reynolds et al., 2020a). Taken together, the results of the studies reported in this manuscript and the existing literature provide strong evidence that any effects of causal beliefs on policy support are largely mediated through beliefs about policy effectiveness. This therefore provides a theoretical extension of the IPAC Framework (Grelle & Hofmann, 2024) by offering an account of how some beliefs about policy effectiveness are formed and/or updated.
Limitations and Future Research
The six studies reported here test the main hypotheses in multiple ways, mixing study designs, contexts, samples, and analytical approaches to establish the replicability and generalisability of our theory. However, there are limits to the claims we can make here. First, the samples were mostly recruited from the United Kingdom, with one hypothesis replicated in a US sample. These samples were also recruited via online participant panels, which are self-selecting and may not reflect lab or field settings, however these are needed due to large sample sizes needed to test small effects. These small effects are also worth highlighting. Within this field, d = 0.1 is a typical benchmark for ensuring sufficient change in policy support – equivalent to an approximately 4% point increase in policy support (World Health Organization, 2024). The current study on average reported effects of half that magnitude suggesting that the practical uses of this approach would need to be combined with more effective messaging to ensure changes in the target causal beliefs, to yield larger changes in policy support. Furthermore, the pattern of results – particularly in correlational comparisons in study 1 – shows that correlational coefficients between policy support and corresponding beliefs versus policy support and non-corresponding beliefs vary in magnitude between the alcohol domain and the obesity domain. Although the difference between corresponding and non-corresponding causal beliefs is evident, the magnitude of this difference is smaller for alcohol and larger for obesity. This perhaps reflects that the non-corresponding causal beliefs are more distinct within the case of obesity due to the broader array of causal factors (Butland et al., 2007). As the current research only tests Specificity-Correspondence Theory in two health policy domains (obesity and alcohol), it is unclear how well the theory would perform in other domains, particularly non-health domains. Testing the theoretical predictions in domains such as climate change policies, immigration policies, technology policies would be valuable for further confirmation and testing the boundary conditions of this theory.
Conclusions
Across four novel studies, secondary analyses of three existing datasets, and internal meta-analyses, we provide support for a new Specificity-Correspondence Theory: specific-corresponding, but not specific-non-corresponding or general causal beliefs, influence people’s attitudes towards government policies, and this operates mainly through changing beliefs about policy effectiveness. This paper provides more evidence that (some) causal beliefs do affect policy support, develops a new theory of policy support, extends the recent IPAC Framework (Grelle & Hofmann, 2024) by providing a novel explanation for how people form beliefs about policy effectiveness, and crucially, explains the mixed and contradictory findings that are prevalent within this field.
Supplemental Material
sj-docx-1-psp-10.1177_01461672261456781 – Supplemental material for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support
Supplemental material, sj-docx-1-psp-10.1177_01461672261456781 for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support by James P. Reynolds, Tess Langfield and Charlotte R. Pennington in Personality and Social Psychology Bulletin
Supplemental Material
sj-docx-2-psp-10.1177_01461672261456781 – Supplemental material for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support
Supplemental material, sj-docx-2-psp-10.1177_01461672261456781 for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support by James P. Reynolds, Tess Langfield and Charlotte R. Pennington in Personality and Social Psychology Bulletin
Supplemental Material
sj-docx-3-psp-10.1177_01461672261456781 – Supplemental material for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support
Supplemental material, sj-docx-3-psp-10.1177_01461672261456781 for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support by James P. Reynolds, Tess Langfield and Charlotte R. Pennington in Personality and Social Psychology Bulletin
Supplemental Material
sj-docx-4-psp-10.1177_01461672261456781 – Supplemental material for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support
Supplemental material, sj-docx-4-psp-10.1177_01461672261456781 for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support by James P. Reynolds, Tess Langfield and Charlotte R. Pennington in Personality and Social Psychology Bulletin
Supplemental Material
sj-docx-5-psp-10.1177_01461672261456781 – Supplemental material for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support
Supplemental material, sj-docx-5-psp-10.1177_01461672261456781 for ArticleWhen and Why Beliefs About the Causes of a Policy Problem Predict Policy Support by James P. Reynolds, Tess Langfield and Charlotte R. Pennington in Personality and Social Psychology Bulletin
Footnotes
Acknowledgements
We are grateful to Dr. Maria Goodwin, Violetta Vysevkova, and Natasha D’Ambrogio for determining the computational reproducibility of some of the analyses.
Ethical Considerations
All novel studies received approval from the Aston University HLS ethics committee. Numbers: #HLS2110, #HLS21176, and #HLS21229. Studies 3 and 5 reported in this manuscript are secondary data analysis and meta-analysis, respectively, which did not need ethical approval.
Consent to Participate
Participants from all studies were provided with a study information sheet and then provided consent to participate and for their responses to be used in publications arising from their data. This consent was provided digitally using the platform Qualtrics.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by U.K. Research and Innovation (UKRI) under the U.K. government’s Horizon Europe funding guarantee (grant number EP/X042758/1; awarded to James Reynolds) and is sponsored by Aston University. The funder had no role in the design, data collection, analysis, or reporting of this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.