
Abstract

Radon
The radioactive gas radon (radon-222) is a ubiquitous source of exposure and a recognised source of lung cancer, second only to smoking. It is present in all buildings and underground locations, but levels can vary considerably from location to location depending on factors such as underlying geology and type of building. For many individuals, including some workers, it is the main contributor to radiation exposure.
Despite its importance, protection against radon was relatively slow to appear in the Commission’s canon of recommendations. This may have been, in part, due to a previous emphasis on protection from overtly man-made sources of exposure, such as nuclear power and the use of radiation in medicine.
A major step forwards occurred in 1991 with publication of the Commission’s 1990 Recommendations (ICRP, 1991), which drew attention to the need for protection against natural sources of radiation in dwellings and workplaces. The Commission pursued this theme, issuing its recommendations for protection against radon-222 at home and work in Publication 65 (ICRP, 1993). This publication developed some of the key strategies for protection against radon, including the delineation of radon-prone areas in order to focus protection resources, and the use of criteria in the form of measured levels of radon gas that could aid decisions on the need for remedial action. Measured levels corresponding to annual effective doses in the range of 3–10 mSv were recommended for intervention in dwellings. Protection in workplaces was, however, considered separately from protection in dwellings. Interestingly, although radon was a source of internal exposure, the Commission did not recommend the use of the dosimetric human respiratory tract model for the assessment and control of radon exposure. Instead, radon exposure was converted to effective dose by direct comparison of the detriment associated per unit effective dose and per unit exposure (dose conversion convention).
In 2007, the Commission issued new recommendations for a system of radiological protection (ICRP, 2007). These evolved from the 1990 Recommendations (ICRP, 1991) by providing a system of protection that applied to all exposures to ionising radiation from any source, regardless of size and origin. Emphasis was placed on application of the principle of optimisation of protection. The 2007 Recommendations (ICRP, 2007) distinguish between planned, emergency, and existing situations of radiation exposure. Most radon exposures are existing exposure situations because the source of the exposure is present when a decision on control has to be taken. Protection is achieved by application of reference levels and optimisation.
In 2010, Publication 115 updated estimates of the risk of lung cancer associated with exposure to radon and its progeny (ICRP, 2010). An important conclusion was that the detriment-adjusted nominal risk coefficient for exposure to radon should be taken to be approximately twice that assumed previously. This report was accompanied by the ICRP Statement on Radon that, among other matters, revised the upper values for radon reference levels, taking account of the new findings on the risk of lung cancer. It also announced the Commission’s intention to provide dose coefficients for radon calculated using its dosimetric models.
At around this time, a Task Group of Committee 4 had been established to elaborate the 2007 protection principles specifically for protection against radon, taking account of the report on the risk of lung cancer. The Task Group report is published in this issue of the Annals of the ICRP. It represents another stage in the evolution of the Commission’s recommendations for protection against radon. The report describes and clarifies application of the 2007 system for protection of members of the public and workers against radon exposures in dwellings, workplaces, and other types of location. Developing on previous recommendations, the report recommends an integrated approach for protection against radon exposure in all buildings, whatever their purpose and status of their occupants. The management of radon exposure is largely based on optimisation with a reference level. A value for the reference level, in terms of effective dose, of approximately 10 mSv year−1, consistent with previous recommendations, continues to be recommended by the Commission. The basis for management of exposures in workplaces with enhanced levels of natural radioactivity presents particular problems. This report recommends a graded approach for workplaces using, initially, the same derived reference level as used for other buildings and locations. If, despite all reasonable efforts, exposures remain above reference levels, the relevant requirements of the system of protection for occupational exposure should be applied.
This report marks a significant step forwards in the development of a coherent system of protection applicable to all sources and situations, with the optimisation principle occupying a central role. The general protection strategy presented in this report could, and indeed should, act as a model for addressing other circumstances of exposure to high levels of natural background radiation.
The Commission has further work underway to provide a complete system of protection for radon. Specifically, dose coefficients for radon, applicable to a number of different situations, will be published shortly.
JOHN R. COOPER
FORMER ICRP MAIN COMMISSION MEMBER
References
Editorial
In January 2012, the International Commission on Radiological Protection (ICRP) welcomed our first Assistant Scientific Secretary, Dr Michiya Sasaki. Dr Sasaki joined the ICRP Scientific Secretariat in Ottawa, Canada as a cost-free expert for just over 2 years. During that time, he acted as Associate Editor of the Annals of the ICRP from Publication 120 (ICRP, 2013) to Publication 125 (ICRP, 2014). He also helped to improve the work of the ICRP Scientific Secretariat, and the Commission as a whole, in many other ways.
Arrangements between the Commission and the Central Research Institute of Electric Power Industry (CRIEPI) to lend Dr Sasaki to the Commission on a cost-free basis were established before March 2011, but, understandably, events in Fukushima Prefecture delayed his arrival in Ottawa considerably. Nonetheless, it was particularly fortuitous to have a well-connected Japanese Assistant Scientific Secretary during the last 2 years, given the significantly increased attention of the Commission and all other organisations interested in radiological protection on events during and following the accident at Fukushima Daiichi nuclear power plant. Dr Sasaki played a central role in enabling the Commission to engage effectively with citizens, experts, government organisations, non-profit organisations, and others in Japan at a time when this engagement was critical.
Although we are sorry to see Dr Sasaki’s term with the Commission come to an end, following an international open call for expressions of interest, CRIEPI has again agreed to assign a cost-free expert to the ICRP Scientific Secretariat. Dr Nobuyuki Hamada began work with the Commission in March 2014, at first remotely from his laboratory in Tokyo, and then stationed at the ICRP Scientific Secretariat in Ottawa, Canada from May 2014.
Dr Hamada received a B.Sc. from Ibaraki Prefectural University of Health Sciences and M.Sc. and Ph.D. from Nagasaki University. He was a postdoctoral fellow at the National Institute of Radiological Sciences and Tohoku University Institute of Development, Aging and Cancer, and an associate professor at Gunma University. In 2010, he joined the Radiation Safety Research Center at CRIEPI as a research scientist. For more than 15 years, his focus has been radiobiology, including research on non-targeted effects, heavy ion effects, and response of primary normal human lens epithelial cells. He has authored or co-authored approximately 80 papers in peer-reviewed international journals, and is the recipient of more than a dozen prestigious awards including the 2013 Michael Fry Research Award of the US Radiation Research Society, and awards from the Japan Radiation Research Society.
We are pleased to welcome Dr Hamada to the ICRP family as Assistant Scientific Secretary and Associate Editor of the Annals of the ICRP.
CHRISTOPHER H. CLEMENT
ICRP SCIENTIFIC SECRETARY, EDITOR-IN-CHIEF
References
Radiological Protection against Radon Exposure
ICRP Publication 126 Approved by the Commission in April 2014
© 2014 ICRP. Published by SAGE.
Keywords: Radon exposure; Prevention; Mitigation; Dwellings; Buildings; Workplaces
Preface
At its meeting in Porto, Portugal in November 2009, the Main Commission of ICRP approved the formation of a new Task Group, reporting to Committee 4, to develop guidance on radiological protection against radon exposure.
The terms of reference of the Task Group were to prepare a publication that describes and clarifies application of the 2007 Recommendations of the Commission for protection against radon exposure in dwellings, workplaces, and other types of location. The publication should present the characteristics of this existing exposure situation, and discuss cases in which exposure to radon should be considered as a planned exposure situation. The publication should also provide guidance on application of the radiological protection principles, as well as appropriate individual dose restrictions and the way to manage the risks of radon through a national action plan.
The publication should be developed from previous relevant ICRP publications, such as Publication 65 (ICRP, 1993) on protection against radon-222 at home and at work, Publication 101, Part 2 (ICRP, 2006b) on the optimisation of radiological protection, Publication 103 (ICRP, 2007) presenting the latest general recommendations of ICRP, and Publication 115 (ICRP, 2010) on the risk of lung cancer from radon and its progeny, which includes the Commission’s Statement on Radon adopted in November 2009, as well as the experience gained by many organisations and countries in the control of radon exposure.


Committee 4 critical reviewers were:
J. Simmonds W. Zeller S. Liu
Main Commission critical reviewers were:
J. Cooper (2009–2012) A. Gonzalez (2009–2012) J. Harrison (2013) E. Vañó (2013)
In addition, Céline Bataille and Sylvain Andresz, acting as Secretary of the Task Group, provided fruitful scientific assistance. Numerous helpful comments were also received from André Poffijn, Ludovic Vaillant, a French mirror group, several experts from Public Health England (UK), and through the ICRP consulting process. The Task Group would like to thank all of these people, as well as Centre d'étude sur l'Evaluation de la Protection dans le domaine Nucléaire (CEPN) (France), for facilities and support during its meetings. The Task Group is also grateful to Michiya Sasaki, the first ICRP Assistant Scientific Secretary, for his contributions.
The Task Group worked mainly by correspondence and met twice on 28–30 April 2010 and 19–21 September 2010 at CEPN, Fontenay-aux-Roses, France.
The membership of Committee 4 during the period of preparation of this report was:
Executive Summary
The objective of this report is to describe and clarify application of the Commission’s system for protection of members of the public and workers against radon exposures in dwellings, workplaces, and other types of location. Radon has two main isotopes. Radon-222 is a radioactive decay product of radium-226, which is present in the earth’s crust in varying concentrations. As radon is a gas, it is capable of movement from the soil to indoors. This movement is dependent on various factors such as the type of soil, building, and/or location. Radon-220 is a radioactive decay product of radium-224 in the thorium-232 decay chain that is also present in the earth’s crust. Both radon-222 and radon-220 can also be released from building materials to the indoor atmosphere. The indoor radon concentration can vary by several orders of magnitude from one building to another. The focus of this report is radon-222. Radon can be inhaled; as it is inert, nearly all of the gas inhaled is subsequently exhaled. However, the inhaled short-lived radon progeny aerosol can deposit within the respiratory tract. Depending on the diffusion properties of the aerosol, the decay products present in the air deposit in the nasal cavities, on the walls of the bronchial tubes, and in the deep lung. Two of these short-lived progeny, polonium-218 and polonium-214, emit alpha particles, and the energy deposited by these alpha particles represents the major contributor to radiation exposure that may lead to health effects. In Publication 115 (ICRP, 2010), the Commission reviewed and analysed epidemiological studies on the association between lung cancer and radon exposures (ICRP, 2010). For both underground mines and homes, there is strong evidence that radon and its progeny can cause lung cancer. As a consequence, the Commission recommended, for radiological protection purposes, a detriment-adjusted nominal risk coefficient for lung cancer in a mixed adult population of non-smokers and smokers of 8 × 10−10 per Bq h m−3 for exposure to radon-222 gas in equilibrium with its progeny [5 × 10−4 per working level month (WLM)]. This is approximately twice the value used by the Commission in Publication 65 (ICRP, 1993). For solid tumours other than lung cancer and leukaemia, there is no consistent evidence, to date, for increased incidence associated with exposures to radon and its progeny. Within the system of radiological protection, radon exposure has the characteristics of an existing exposure situation as the source is unmodified concentrations of ubiquitous primordial natural activity in the earth’s crust (ICRP, 2007). Human activities such as construction of buildings or operation of mines may create or modify pathways that increase exposure to radon and its progeny. These pathways can be controlled by preventive and mitigating actions. However, the source itself cannot be modified, and thus already exists when a decision on control has to be taken. However, in some workplaces, the radon exposure situation may be deemed to be a planned exposure situation from the outset by national authorities. Such workplaces include uranium mines associated with the nuclear fuel cycle. Radon is not likely to give rise to an emergency exposure situation, although the discovery of very high concentrations in a location may require the prompt implementation of protective actions. The philosophy of Publication 103 (ICRP, 2007) compared with Publication 60 (ICRP, 1991) is to recommend a consistent approach for the management of all types of exposure situations. This approach is based on application of the optimisation principle implemented using appropriate individual dose restrictions: dose constraints or reference levels. Optimisation involves endeavouring to reduce doses as far below constraints or reference levels as is reasonably achievable, regardless of the initial level of exposure. Day-to-day life at home and at work inevitably leads to some exposure to radon. In common with many other existing exposure situations, radon exposures can be very heterogeneous. The level of exposure is highly dependent upon individual behaviour. The role of self-help protective actions is therefore crucial. The characterisation of the exposure situation is a prerequisite to its control. Domestic radon exposure management should address a number of issues (e.g. environmental, health, economic, architectural, and educational) involving a wide range of stakeholders. Control of indoor radon exposure poses many challenges. As individuals move from place to place in the same area, a radon protection strategy should be developed by national authorities, and implemented in a consistent and integrated manner in the various locations. As much radon exposure occurs in the home, a radon protection strategy should address exposure in dwellings from a public health perspective. In many buildings, the level of radon can be well above the concentration that has been shown to represent potential health risks, and a commitment is needed to reduce overall exposure of the general population and the highest individual exposures. The strategy should be straightforward, appropriately scaled with other health hazards, supported and implemented on a long-term basis, and involve all stakeholders. The national radon protection strategy also has to address these challenges in terms of responsibilities, notably the responsibility of the individual householder towards the occupants, of the builder or the seller of a property towards the buyer, of the landlord towards the tenant, of the employer towards the employee, and, generally speaking, of the responsible person for any building towards its users. All of these factors impact on the potential for enforcement of the radon strategy. The range of responsibilities drives the need for a radon strategy that is based on effectiveness and realism. Any radon protection strategy should aim to maintain and/or reduce radon concentrations to a level that is as low as reasonably achievable, keeping in mind that it is not feasible to eliminate indoor radon completely. The Commission considers that, in most situations, a national radon protection strategy would be justified as radon is ubiquitous; it represents a significant source of radiation exposure, being the second leading cause of lung cancer after smoking; and, in most circumstances, it can be controlled. A radon protection strategy can also have positive consequences on other public health policies such as tobacco control and indoor air quality. Characterisation of the situation, including the assessment of radon concentrations and identification of radon-prone areas, as well as considerations about public health priorities and social and economic factors, are necessary for national authorities to frame and implement a radon protection strategy. Although the absolute risk of lung cancer arising from radon exposure is significantly greater in smokers than in non-smokers, the Commission’s recommendations for protection against radon do not distinguish between smokers and non-smokers. Characterisation of the exposure situation is also a prerequisite for application of the optimisation principle. This principle is the driver for controlling radon exposure in order to maintain or reduce exposure to a level that is as low as reasonably achievable, taking the prevailing economic and societal circumstances into account. As with the control of other sources of radiation, the Commission recommends the use of a source-related individual dose restriction in conjunction with the optimisation of protection. It is the responsibility of the appropriate national authorities, as with other radiation sources, to establish their own national reference levels of dose and derived reference level of concentration, and to apply the process of optimisation of protection within their country. The objective is both to reduce the overall risk to the general population and, for the sake of equity, the individual risk to the most exposed individuals. In both cases, the process is implemented mainly through the management of buildings rather than individual exposures, and should result in radon concentrations in ambient indoor air that are as low as reasonably achievable below the national reference level. Radon exposure can only be controlled by actions on exposure pathways. Individuals gain benefit from the situation, and support is provided to individuals to reduce their doses. Given these considerations, the appropriate reference level should correspond to an annual dose in the range of 1–20 mSv, as recommended by the Commission for existing exposure situations (ICRP, 2007, Table 5). The Commission considers that a value of the order of 10 mSv, as indicated in Publication 65 (ICRP, 1993), should remain a benchmark for setting a reference level for radon exposure. As most radon control measures are applied to buildings, it is appropriate to establish derived reference levels for radon set in terms of concentration in air, which is a measurable quantity, expressed in Becquerel per cubic metre (Bq m−3). In Publication 103 (ICRP, 2007), the Commission recommended upper values for derived reference levels of 600 Bq m−3 for homes and 1500 Bq m−3 for workplaces. In response to its review of radon epidemiology in Publication 115 (ICRP, 2010) and the increase of the nominal risk coefficient by approximately a factor of 2, the Commission reduced the upper reference level for homes to 300 Bq m−3 in the associated Statement on Radon. A radon concentration of 300 Bq m−3 in homes corresponds to an annual dose of approximately 10 mSv using the dose conversion convention, based on the revised nominal risk coefficient (ICRP, 2010). The Statement on Radon also referred to a level of 1000 Bq m−3 as an entry point for applying occupational radiological protection requirements, replacing the upper reference level of 1500 Bq m−3. In its Statement on Radon, the Commission also signalled its intention to publish dose coefficients for intakes of radon and its progeny calculated using reference biokinetic and dosimetric models. Based on new dose coefficients, 300 Bq m−3 corresponds to a higher annual dose but within the range of 1–20 mSv in homes. For the practical implementation of a radon protection strategy, the Commission continues to recommend an upper value of the derived reference level of 300 Bq m−3 for radon-222 in dwellings. The Commission strongly encourages national authorities to set a national derived reference level that is as low as reasonably achievable in the range of 100–300 Bq m−3, taking the prevailing economic and societal circumstances into account. This is consistent with the ICRP Statement on Radon (ICRP, 2010) and the World Health Organization’s (WHO) Handbook on Indoor Radon (WHO, 2009). In assessing compliance with the derived reference level, measurements should be representative of the annual mean concentration of radon in a building or location. For simplicity, considering that individuals going from place to place in the same area in their daily life should be protected on the same basis, regardless of the location, the Commission recommends using the same upper value of 300 Bq m−3 in mixed-use buildings, which are used by both members of the public and workers. The Commission now recommends that a graded approach should be applied for the control of radon exposures. In such an approach, the radon protection strategy should start with a programme that aims to encourage relevant decision makers to promote self-help protective actions, such as measurement and, if needed, remediation. This process can be implemented through information, advice, assistance, and, where necessary, more formal requirements. The use and level of enforcement of these various actions should be dependent upon the degree of legal responsibility for the situation, and the level of ambition of the national radon protection strategy. A specific graded approach should be implemented for workplaces, replacing the entry level of 1000 Bq m−3 for applying occupational protection requirements. Where workers’ exposure to radon is not considered as occupational (e.g. office buildings), the first step is to reduce the concentration of radon to a level that is as low as reasonably achievable below the same derived reference level as set for dwellings. The corresponding annual dose is usually lower than that in dwellings, because the time spent in workplaces is usually less than the time spent at home. If difficulties are met in the first step, a more realistic approach is recommended as a second step, consisting of optimising protection using the actual parameters of the exposure situation, such as occupancy, together with a reference level of the order of 10 mSv annual dose. If, despite all reasonable efforts to reduce radon exposure in workplaces, the exposure persists above the reference level expressed in dose, the workers should be considered as occupationally exposed. In such cases, the Commission recommends application of the relevant requirements for occupational exposure (ICRP, 2007, Section 5.4.1). The Commission also recommends application of the same requirements in workplaces where, from the outset, exposure of workers to radon is considered as occupational by national authorities. Such workplaces may include thermal spas, caves, and other underground workplaces. Regardless of whether or not workers are considered as occupationally exposed, their exposure should be kept below the upper value of the range for existing exposure situations (20 mSv year−1). The occupational dose limit should apply when the national authorities consider that the radon exposure situation should be managed as a planned exposure situation. To be effective, the national radon protection strategy should be established with a long-term perspective. The process for significantly reducing the risks of radon to the general population usually takes several decades of consistent effort, rather than several years. The Commission considers that, for the sake of clarification, the distinction should be made between prevention, aiming to maintain exposure at a level that is as low as reasonably achievable under the prevailing circumstances, especially in new buildings, and mitigation, aiming to reduce exposure to a level that is as low as reasonably achievable in existing buildings. As a consequence, a radon protection strategy should include preventive actions. Regardless of the indoor location, the category of individuals present, and the type of exposure situation, it is possible to address radon exposure by considering the issue of radon exposure during the planning, design, and construction phases of a building. Preventive actions are implemented through land planning and building codes for new buildings, and for renovation of old buildings. This also means the integration of the radon protection strategy in a manner consistent with other strategies concerning buildings, such as indoor air quality or energy saving, in order to develop synergies and avoid contradictions. (aa) The mitigation part of the national radon protection strategy addresses existing buildings and locations. As far as possible in such cases, the control of exposure should be ensured through the management of the building or location and the conditions of its use, whatever the category of individuals present. The main steps are measurements and, when needed, corrective actions to mitigate exposures. (bb) The national radon protection strategy should be implemented through a national radon action plan established by national authorities with the involvement of relevant stakeholders. The action plan should establish a framework with a clear infrastructure, determine priorities and responsibilities, and describe the successive steps to deal with radon in the country. Depending on the exposure conditions, it should identify stakeholders, such as those who are exposed and those who should provide support or implement action; address ethical issues, particularly those associated with responsibilities; and provide information, guidance, support, and conditions for sustainability. (cc) The national action plan should also deal with radon measurement techniques and protocols; radon surveys to identify radon-prone areas; methods for mitigating radon exposure and their applicability in different situations; supporting policies, including information, training, and involvement of stakeholders; and assessment of effectiveness. The issue of buildings with public access and workplaces should also be addressed with a specific graded approach reflecting legal responsibilities. The national action plan should be evaluated and reviewed periodically, including the value of the derived reference level.
Main Points
People are exposed to radon at home, in workplaces, and in mixed-use buildings. Variability of indoor radon concentrations results in a very heterogeneous distribution of exposures. Outdoor radon exposure is generally not an issue. There is strong evidence that exposures to radon and its progeny may result in lung cancer. Radon exposure is the second leading cause of lung cancer after smoking. Radon exposure is an existing exposure situation as the source is unmodified concentrations of ubiquitous primordial natural activity in the earth’s crust. Only pathways can be controlled. National authorities should characterise the exposure situation and develop a national radon protection strategy. As much radon exposure occurs in the home, this strategy should address exposure in dwellings from a public health perspective, and should have a commitment to reduce the overall exposure of the general population and the highest individual exposures. The strategy should be straightforward and realistic; integrated, in order to be consistent for all buildings; graded according to the situation and responsibilities; and should not distinguish between smokers and non-smokers. It should be considered in conjunction with other public health policies, such as energy saving, non-smoking, and indoor air quality. The radon protection strategy should include preventive actions in new buildings and mitigating actions in existing buildings. The management of radon exposure is mainly based on application of the optimisation principle with an appropriate reference level. This level should correspond to an annual dose in the range of 1–20 mSv as recommended by the Commission. The Commission considers that a value of the order of 10 mSv annual dose should remain a benchmark for setting a reference level for radon exposure. For practical implementation of the radon protection strategy, the upper value for the derived reference level recommended by the Commission in dwellings continues to be 300 Bq m−3 as an annual mean concentration. The same value is recommended for all other buildings and workplaces. The Commission strongly encourages national authorities to set a national derived reference level that is as low as reasonably achievable in the range of 100–300 Bq m−3, taking the prevailing economic and societal circumstances into account. In most workplaces, radon exposures of workers are adventitious and are not considered to be occupational. The Commission recommends a specific graded approach in workplaces with the following steps:
optimising protection using the common derived reference level for all buildings and workplaces; optimising protection using the actual parameters of the exposure situation, such as occupancy, together with a reference level of 10 mSv annual dose; and applying the relevant requirements for occupational exposure when, despite all reasonable efforts, the exposure remains above the reference level. The relevant requirements for occupational exposure apply in workplaces where, from the outset, exposures of workers to radon are considered as occupational by national authorities. The occupational dose limit should apply when the national authorities consider that the radon exposure situation should be managed as a planned exposure situation.
Glossary
Categories of exposure
The Commission distinguishes between three categories of radiation exposure: medical, occupational, and public.
Derived reference level
Numerical value expressed in an operational or measurable quantity, corresponding to the reference level set in dose.
Employer
An organisation, corporation, partnership, firm, association, trust, estate, public or private institution, group, political or administrative entity, or other persons designated in accordance with national legislation with recognised responsibility, commitment, and duties towards a worker in his/her employment by virtue of a mutually agreed relationship. A self-employed person is regarded as being both an employer and a worker.
Equilibrium equivalent concentration
The activity concentration of radon gas, in equilibrium with its short-lived progeny, that would have the same potential alpha energy concentration as the existing non-equilibrium mixture.
Equilibrium factor
The ratio of the equilibrium equivalent concentration to the radon gas concentration. In other words, the ratio of potential alpha energy concentration for the actual mixture of radon decay product to that which would apply at radioactive equilibrium.
Existing exposure situation
A situation resulting from a source that already exists when a decision on control has to be taken, including natural background radiation, long-term contaminated areas after a nuclear accident or a radiological emergency, and residues from past practices that were operated outside the Commission’s recommendations.
Exposure pathway
A route by which radiation or radionuclides can reach humans and cause exposure.
Graded approach
For a system of control, such as a national system or a safety system, a process or method in which the stringency of the control measures and conditions to be applied are commensurate, to the extent practicable, with the likelihood and possible consequences of, and the level of risk associated with, loss of control.
Medical exposure
Exposure incurred by patients as part of their own medical or dental diagnosis or treatment; by persons, other than those occupationally exposed, knowingly, while voluntarily helping in the support and comfort of patients; and by volunteers in a programme of biomedical research involving their exposure.
Member of the public
Any individual who receives an exposure that is neither occupational nor medical.
National radon survey
A survey undertaken to determine the radon concentration distribution that is representative of radon exposure to the population within a country.
Naturally occurring radioactive material
Radioactive material containing no significant amounts of radionuclides other than naturally occurring radionuclides. Materials in which the activity concentrations of the naturally occurring radionuclides have been changed by some processes are included.
Occupational exposure
All exposures of workers incurred at work as a result of situations that can reasonably be regarded of being the responsibility of the operating management.
Operating management
The person or group of persons who directs, controls, and assesses an organisation at the highest level. Many different terms are used, including chief executive officer, director general, managing director, and executive group.
Optimisation of protection
The process of determining what level of protection makes exposures, and the probability and magnitude of potential exposures, as low as reasonably achievable, taking economic and societal factors into account.
Planned exposure situations
Situations involving the deliberate introduction and operation of sources. Planned exposure situations can give rise to exposures that are anticipated to occur (normal exposures) and to exposures that are not anticipated to occur (potential exposures).
Potential alpha energy concentration
The concentration of short-lived radon-222 or radon-220 progeny in air in terms of the alpha energy emitted during complete decay from radon-222 progeny to lead-210 or from radon-220 progeny to lead-208 of any mixture of short-lived radon-222 or radon-220 in a unit volume of air. The SI unit for potential alpha energy concentration is J m−3.
Public exposure
Exposure incurred by members of the public from radiation sources, other than occupational and medical exposures.
Radon-220 progeny
The decay products of radon-220, used in this report in the more limited sense of the short-lived decay products from polonium-216 through polonium-212 or thallium-208.
Radon-222 progeny
The decay products of radon-222, used in this report in the more limited sense of the short-lived decay products from polonium-218 through polonium-214. Radon progeny are sometimes referred to as ‘radon decay products’ or the more historic term ‘radon daughters’.
Radon-prone area
A geographic area or an administrative region defined on the basis of surveys indicating a significantly higher radon concentration than in other parts of the country.
Reference level
In existing exposure situations, this represents the level of dose or risk above which it is judged to be inappropriate to plan to allow exposures to occur, and below which optimisation of protection should be implemented. The chosen value for a reference level will depend upon prevailing circumstances of the exposure under consideration.
Risk
Risk relates to the probability that an outcome (e.g. lung cancer) will occur. Terms relating to risk are grouped together here.
Relative risk
The ratio of the incidence rate or the mortality rate from the disease of interest (i.e. lung cancer) in an exposed population to that in an unexposed population.
Excess relative risk
Relative risk – 1.
Risk coefficient
Increase in risk per unit exposure or per unit dose. In general, expressed as excess relative risk per working level month, per J h m−3, per 100 Bq m−3, or per Sv.
Detriment
Detriment is an ICRP concept. It reflects the total harm to health experienced by an exposed group and its descendants as a result of the group’s exposure to a radiation source. Detriment is a multidimensional concept. Its principal components are the stochastic quantities: probability of attributable fatal cancer; weighted probability of attributable non-fatal cancer; weighted probability of severe heritable effects; and length of life lost if the harm occurs.
Worker
Any person who is employed, whether full time, part time, or temporarily, by an employer, and who has recognised rights and duties in relation to her/his job.
Working level
The historical unit for potential alpha energy concentration, defined as any combination of the short-lived progeny of radon in 1 m3 of air that will result in the emission of 1.30 × 108 MeV m−3 of potential alpha energy, which is approximately equal to 2.08 × 10−5 J m−3.
Working level month
The cumulative exposure from breathing an atmosphere at a concentration of one working level for a working month of 170 h.
1. Introduction
1.1. Background
The Commission has previously published recommendations on protection against radon exposure. In Publication 65 (ICRP, 1993), the Commission reviewed the existing knowledge about the health effects of inhaled radon and its progeny, and developed a framework for the management of radon exposure in both dwellings and workplaces in line with the general recommendations published 2 years previously (ICRP, 1991). In Publication 101, Part 2 (ICRP, 2006b), the Commission updated its recommendations on the optimisation of radiological protection. Publication 101, Part 2 (ICRP, 2006b) did not contain specific provisions on radon exposure, but re-inforced the importance of the optimisation principle in radiological protection as applicable in all exposure situations, and recommended broadening the process to involve relevant stakeholders. At the same time, the Commission revised its general recommendations in Publication 103 (ICRP, 2007), in which a section is devoted to radon in dwellings and workplaces. This section broadly confirmed the recommendations of Publication 65 (ICRP, 1993), and introduced the concept of reference level to replace the concept of action level. More recently, the Commission reviewed available scientific information on risk due to radon. In 2009, the Commission adopted a statement summarising its updated position on radon exposure at home and in workplaces, with revised risk detriment values and reference levels. The ICRP Statement on Radon was published with Publication 115, presenting a review of the risk of lung cancer associated with radon and its progeny (ICRP, 2010). Since Publication 65 (ICRP, 1993), many countries have gained experience in the implementation of radon policies to control radon exposure. In addition, international organisations have provided scientific information and guidance on this issue. In particular, the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) has published a report on radon exposure and risks (UNSCEAR, 2009), and the World Health Organization (WHO) has published a handbook dealing with the management of indoor radon exposure from a public health perspective (WHO, 2009). More recently, the key recommendations of the ICRP Statement on Radon have been integrated into the International and European Basic Safety Standards (IAEA, FAO, ILO, OECD/NEA, PAHO, UNEP, WHO, 2011; EURATOM, 2014). The purpose of this report is to update and revise the recommendations on controlling exposure to radon, taking the above publications into account. It also considers the revised dose coefficients for the inhalation and ingestion of radionuclides, including radon and its progeny, to be presented in detail in other ICRP publications.
1.2. Scope
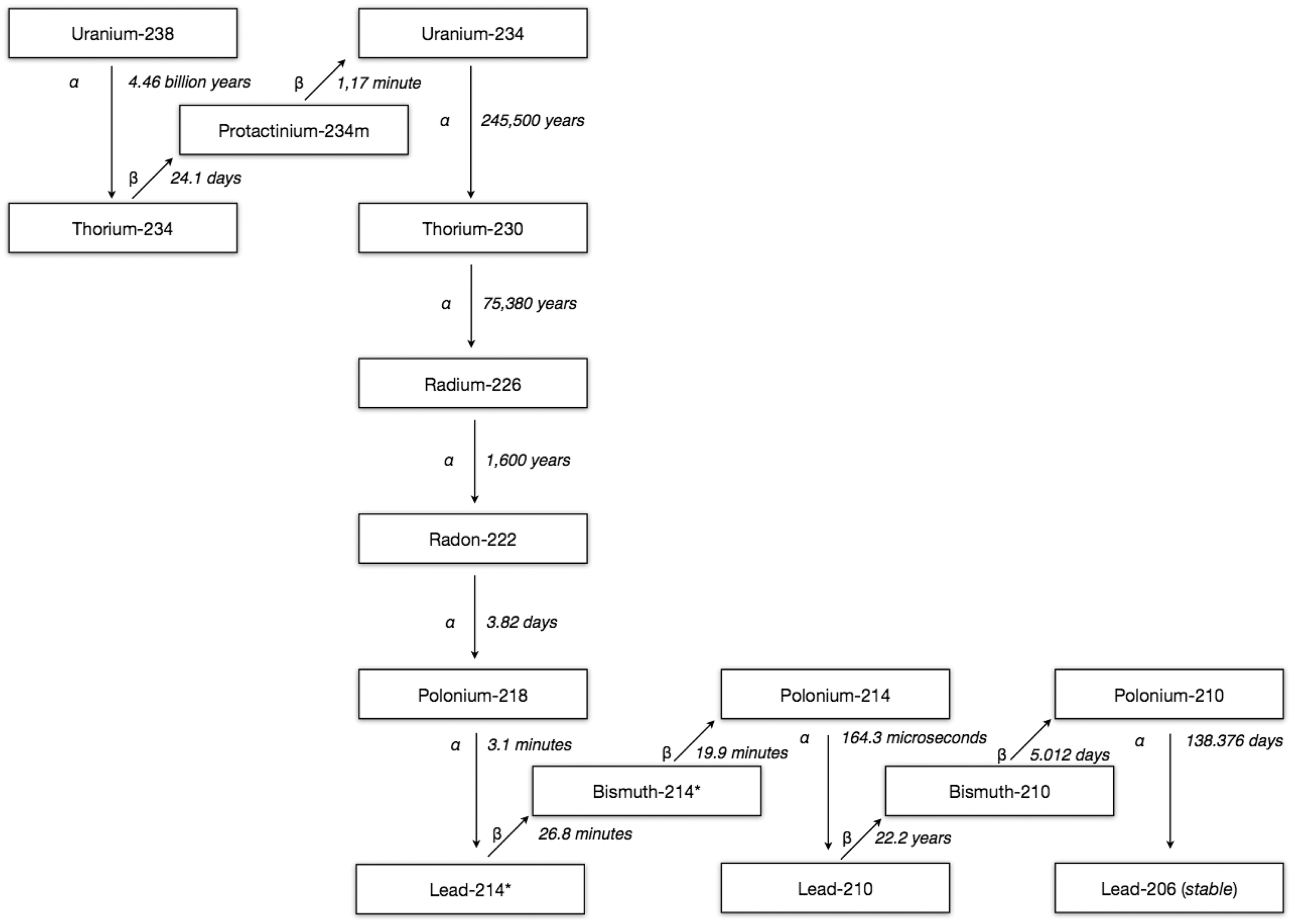
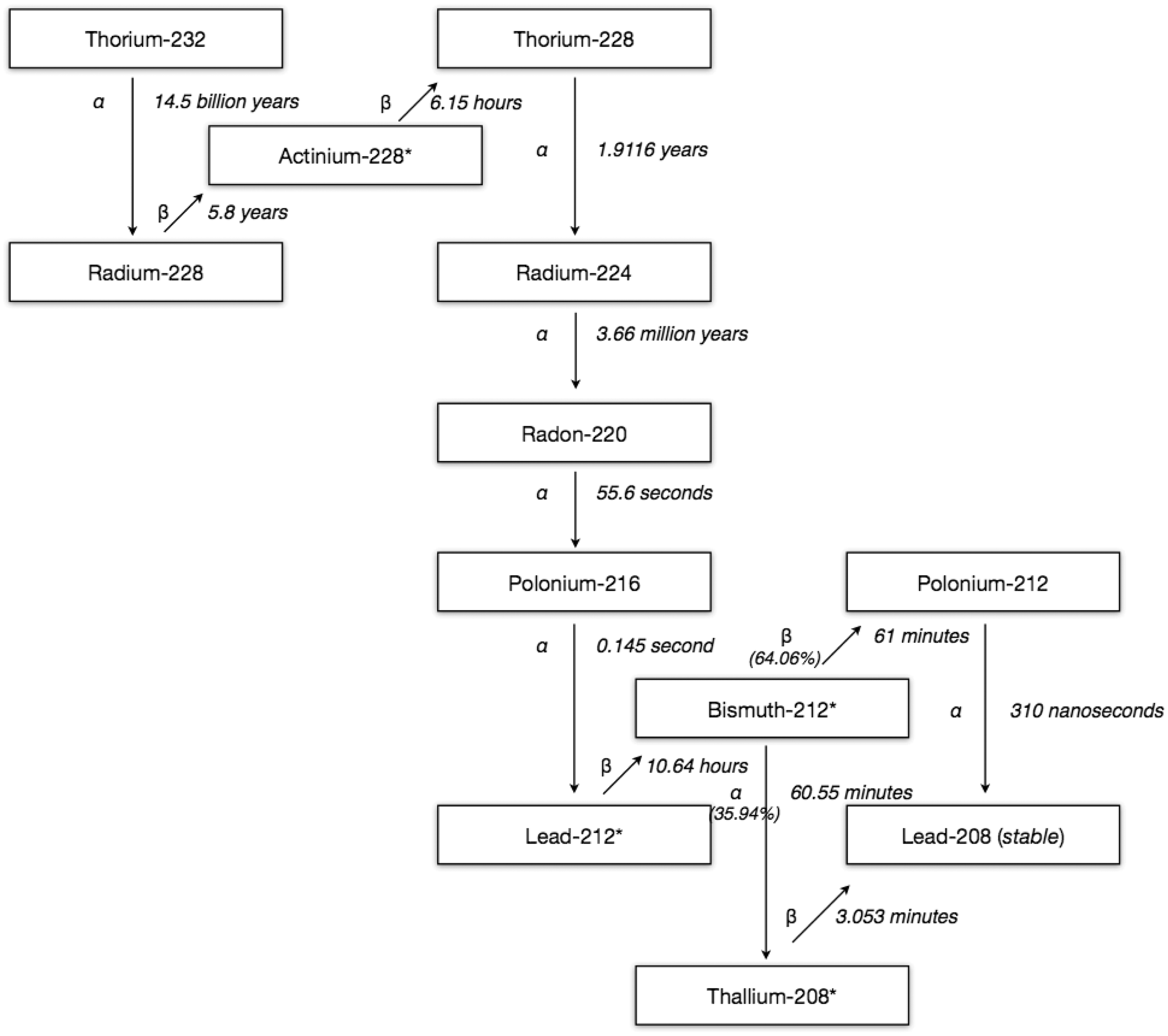
Radon is a radioactive decay product of uranium-238, uranium-235, and thorium-232. In the case of the uranium-238 series, the resulting isotope is radon-222, which is a direct decay product of radium-226 (Fig. 1.1). In the case of the uranium-235 series, the resulting isotope is radon-219 (Fig. 1.2). In the case of the thorium-232 series, the resulting isotope is radon-220, a direct decay product of radium-224 (Fig. 1.3). Human exposure to radon is mainly due to radon-222 or, more precisely, its short-lived progeny. Due to its short half-life, exposure to radon-220 in ambient indoor air is generally less significant. The contribution of radon-219 to exposure is insignificant because migration is not significant due to the short half-life, and therefore it is not considered in this publication. People are exposed to radon-222 and radon-220 in dwellings as members of the public or in workplaces as workers. People are also exposed to radon in public or private places open to the public, such as town halls, post offices, schools, hospitals, housing for the elderly, jails, shops, and entertainment buildings, either as members of the public (e.g. customers, users, visitors, pupils) or as workers (e.g. staff, porters, shopkeepers, guides, guards, teachers, nurses). There can also be the case of workers who may be inhabitants, such as caretakers. This report is applicable to the control of radon-222 exposures in any location and for all individuals. Guidance related to radon-220, which is a lesser health concern, is mainly focused on provisions related to building materials (see Section 4.4). The objective of this report is to describe and clarify application of the Commission’s system for protection against radon exposure. It is focused on the management of buildings, such as dwellings, mixed-use buildings, and most workplaces, for the general protection of members of the public and workers who are not considered as occupationally exposed. For specific workplaces such as uranium mines, where workers are often considered as occupationally exposed, no new provisions are recommended for the management of individual exposures. Uranium-238 decay products.*Isotope is also a significant gamma emitter. Uranium-235 decay products. *Isotope is also a significant gamma emitter. Thorium-232 decay products. *Isotope is also a significant gamma emitter.

1.3. Structure
Section 2 presents the characteristics of radon exposure, mainly focused on radon-222. It provides a brief history of the control of radon-222, with a description of the radon sources and transfer mechanisms, as well as the nature and the quantification of the associated health risks. The main challenges in developing a national radon protection strategy are also outlined. Section 3 presents the system of protection for radon exposure. After an explanation on how to deal with the categories of individuals exposed in the different types of exposure situations, three sections are devoted to justification of protection strategies, optimisation of protection, and application of dose limits when relevant. Section 4 provides guidance on the implementation of protection strategies for the control of radon exposure, depending on the situation. Section 4.1 addresses the control of exposure in buildings through a national action plan. Sections 4.2 and 4.3 focus on prevention and mitigation, respectively, and Section 4.4 focuses on building materials. Sections 4.5 and 4.6 address the radon protection of workers in general workplaces and in uranium mines, respectively. Finally, Section 4.7 is devoted to stakeholder interactions.
2. Characteristics of Radon Exposure
2.1. Historical perspective
The existence of a high mortality rate among miners in central Europe was recognised before the 17th Century, and the main cause of their death was identified as lung cancer in the late 19th Century (Haerting and Hesse, 1879). In 1924, it was suggested that these lung cancers could be attributed to radon exposure (Ludewig and Lorenzer, 1924). These first observations were an incentive to take measurements of radon. Early radon measurements were largely confined to environmental studies of diverse phenomena, such as atmospheric electricity, atmospheric transport, and exhalation of gases from soil. Monitoring programmes for exposure to radon progeny in uranium mines were developed in the 1950s to control worker exposure. The first indoor radon measurements were made in the 1950s (Hultqvist, 1956), but attracted little attention. From the 1970s, however, there were an increasing number of measurements of elevated radon levels in dwellings in some countries. Over the last 10 years, comprehensive radon surveys in dwellings and workplaces, as well as management strategies, have been implemented in many countries. Radon was formally identified as a cause of lung cancer in 1986 (WHO, 1986; IARC, 1988). At that time, the main source of information on risks of radon-induced lung cancer was epidemiological studies of underground miners (ICRP, 1993). Since the 1990s, several studies have provided informative data on risks at lower levels of exposure, and shown higher risks from radon at chronic low-rate exposures (e.g. Lubin et al., 1997; NRC, 1998; EPA, 1999, 2003; Tomášek et al., 2008). In addition, recent combined analyses of lung cancer data from case–control studies of residential radon exposure have demonstrated increased risks at lower levels of exposure (Lubin et al., 2004; Darby et al., 2005, 2006; Krewski et al., 2006). A more comprehensive review of the history of the control of radon exposure is given in Publication 65 (ICRP, 1993).
2.2. Radon sources and transfer
Radon-222 is a radioactive decay product of uranium-238, which is present in the earth’s crust in varying concentrations (at parts per million levels). Radon-222 has a half-life of 3.82 days and is the direct decay product of radium-226. In the course of radioactive decay, the resulting products generally remain in the rock where the atom decays. In the case where the decay product is gaseous, the atom is capable of movement. If it is created in a pore space next to a fracture or a discontinuity in the rock, it can move from its point of production. The air in the soil is heavily loaded with radon, with concentrations between 2000 and 106 Bq m−3, usually measured 0.5–1 m beneath the soil surface (Cothern and Smith, 1987; Winkler et al., 2001). Radon in pore spaces is mainly transported by diffusion, with the transport rate depending on the porosity and permeability of the soil, or by convection, dependent on the presence of cracks and faults. The movement of dissolved radon via ground water is another significant mechanism of transport. Some radon gas can pass from the soil into the atmosphere before it decays. The quantity of radon emanating from the soil is typically small, and is diluted rapidly in the air, with the extent of dilution depending on atmospheric stability, presence of wind, and level of turbulence (related to the vertical temperature gradient). Therefore, the concentration of radon-222 in atmospheric air is generally low but variable. Measurements over land vary between 1 and 100 Bq m−3. Typical outdoor levels of radon-222 are of the order of 10 Bq m−3, with lower levels near coasts and over small islands (UNSCEAR, 2000, 2009). Radon-220 is a radioactive decay product of thorium-232, which is present in the earth’s crust in varying concentrations. Radon-220 has a much shorter half-life (T1/2 = 55 s) than radon-222, so it does not move significantly from its source. Its behaviour in the environment is quite different from that of radon-222. The main source of radon-220 in indoor air is from building materials. There is considerable variability in radon-220 gas concentrations from place to place. In general, the average indoor levels of radon-220 gas in different countries are in the range of 0.2–12 Bq m−3 (UNSCEAR, 2000, 2009). Exposures to radon-220 do not normally present radiological protection problems, except in some particular cases such as some traditional housing. While the radon concentration from soil to outdoor air is diluted rapidly, this is not the case if the flux enters closed premises such as dwellings (Fig. 2.1). Depending on the ventilation rate of the building, radon gas can accumulate compared with outdoor air. Depending on meteorological parameters and, in particular, the temperature difference between outdoor and indoor air, there is a pressure differential between the soil and the foundations of the building. This causes an enhanced flow of radon-rich soil air, depending on the permeability of the floor slab resting on the soil and the ventilation of the sub-slab crawl space, if this exists. This pressure-driven flow is generally much more important than transfer of radon by diffusion. In the absence of pressure differences, the transfer of radon by diffusion is reduced as a result of the higher density of the solid foundations compared with the soil surface. The transfer of radon from the soil to buildings depends on several parameters:
the composition of the soil (chemistry, geology, soil moisture, and permeability to radon); the concentration of radon in the soil; the difference in pressure between inside and outside of the considered building or location, between the soil and the atmosphere surrounding the building, and between the soil and the lower rooms of the building; the area of building in contact with the ground; and the air tightness of the outer shell of the building, including the presence of cracks, pipe ducts, cable ducts, etc., especially in the floors and foundations of the building. The transfer of radon within buildings also depends on several factors:
the circulation of air in the building depending on ventilation and air conditioning; the meteorological and seasonal parameters, mainly the temperature difference between outside and inside air; the floor level and the size of the rooms; and the lifestyle choices, such as opening doors and windows, and the working habits of the building occupants. Building materials have variable levels of uranium and thorium. Radon can be released from these materials into the surrounding air. The activity released depends on the rate of radon production and the porosity of the material. For ordinary building materials, the volumetric rate of ingress is between 0.05 and 50 Bq (m3 h)−1 and the corresponding concentration is between 0.03 and 30 Bq m−3 (for an average rate of air renewal of 0.7 h−1). Situations do exist where the concentration of radon can reach 1000 Bq m−3 (e.g. in the case of concrete containing a high concentration of radium). However, in the majority of cases, this source of radon is of secondary importance compared with radon infiltration from the soil (EC, 1999). Radon concentration in ground water varies considerably, and can be relatively high despite the poor solubility of radon in water. Values range from a few to several tens of thousand Bq l−1 (Skeppström and Olofsson, 2007). Relatively high radon concentrations have been observed for some private wells, boreholes, and springs. If the water containing radon is used for a domestic supply, the radon can degas into indoor air causing elevated levels. Radon levels in most public supplies are generally relatively low due to the decrease in radon by decay or degassing during transfer. Whatever the source of radon (soil, building materials, or water), the concentration in buildings can vary over several orders of magnitude ranging from 10 to 70,000 Bq m−3 according to UNSCEAR (2009). The world average indoor value is approximately 40 Bq m−3. Pathways of indoor radon.

2.3. Risks of radon
Traditionally, the assessment of risks of radon exposure has been based on epidemiological studies, mainly involving the follow-up of underground uranium miners. This approach allowed the calculation of relative risk per level of exposure, expressed in working level months (WLM), J h m−3, or Bq h m−3. In Publication 65 (ICRP, 1993), a dose conversion convention was defined, based on a direct comparison of the detriment per unit exposure to radon and its progeny with the total detriment per unit effective dose. The former was determined from miner epidemiology, and the latter was mainly determined from epidemiological studies of Japanese atomic bomb survivors exposed largely to gamma rays. This comparison allowed the calculation of effective dose per unit exposure, expressed in mSv per WLM or mSv per Bq h m−3, and the derivation of action levels expressed in Bq m−3. For all other radionuclides, effective dose is calculated using reference biokinetic and dosimetric models with specified radiation and tissue weighting factors. In Publication 115 (ICRP, 2010), the Commission stated its intention to include radon with other radionuclides in future calculations of dose coefficients.
2.3.1. Epidemiological evidence
In its Handbook on Indoor Radon (WHO, 2009), WHO evaluated the health effects of radon exposure in dwellings and drew the following conclusions.
Epidemiological studies confirm that radon in homes increases the risk of lung cancer in the general population. Other health effects of radon have not been demonstrated consistently. The proportion of all lung cancers linked to radon is estimated to lie between 3% and 14%, depending on the average radon concentration in the country and the method of calculation. Radon is the second most important cause of lung cancer after smoking in many countries. Radon is much more likely to cause lung cancer in people who smoke, or who have smoked in the past, than in lifelong non-smokers. However, it is the primary cause of lung cancer among people who have never smoked. There is no known threshold concentration below which radon exposure presents no risk. Even low concentrations of radon can result in a small increase in the risk of lung cancer. In Publication 115 (ICRP, 2010) on the risk of lung cancer associated with exposure to radon and its progeny, the Commission made a thorough review and analysis of the epidemiology of radon for both workers (underground miners) and the general population. Its main conclusions were as follows.
There is strong evidence from cohort studies of underground miners and from case–control studies of residential radon exposures that radon and its progeny can cause lung cancer. For solid tumours other than lung cancer and leukaemia, there is, to date, no convincing or consistent evidence of any excess risk associated with exposure to radon and its progeny. Appropriate comparisons of estimates of the risk of lung cancer from miner studies and from indoor studies show good consistency. Three pooled residential case–control studies (in Europe, North America, and China) gave similar results. After correcting for random uncertainties in the radon activity concentration measurements, the European pooled residential case–control study reported an excess relative risk of 16% (95% confidence intervals: 5–32%) The cumulative risk of lung cancer up to 75 years of age is estimated for lifelong non-smokers as 0.4%, 0.5%, and 0.7% for radon activity concentrations of 0, 100, and 400 Bq m−3, respectively. The cumulative risks of lung cancer by 75 years of age for lifelong smokers are close to 10%, 12%, and 16% for radon activity concentrations of 0, 100, and 400 Bq m−3, respectively (Darby et al., 2005, 2006). Cigarette smoking remains the most important cause of lung cancer. Based upon a review of epidemiological studies of underground miners, including studies with relatively low levels of exposure, a detriment-adjusted nominal risk coefficient of 5 × 10−4 per WLM (0.14 per J h m−3) is adopted for the lung detriment per unit exposure. This value was derived from recent studies considering exposure during adulthood, and is close to twice the value calculated in Publication 65 (ICRP, 1993). As a result of this review, the Commission recommended, in its Statement on Radon, a detriment-adjusted nominal risk coefficient for a population of all ages (mixed adult population of non-smokers and smokers) of 8 × 10−10 per Bq h m−3 for exposure to radon-222 gas in equilibrium with its progeny (ICRP, 2010). The Commission’s findings are consistent with other comprehensive estimates, including that submitted to the United Nations General Assembly by UNSCEAR (2009).
2.3.2. Dosimetric approach
Equivalent and effective doses, following inhalation of radon progeny, can be calculated with the ICRP reference biokinetic and dosimetric models including the Human Respiratory Tract Model (ICRP, 1993, 2014a), the Human Alimentary Tract Model (ICRP, 2006a), and the systemic biokinetic models for polonium, lead, and bismuth (ICRP, 2014b). A systemic biokinetic model for radon gas has also been developed so that effective doses arising from the inhalation of radon gas can be calculated (ICRP, 2014b). Radon-222 decays to form one atom of non-gaseous polonium-218. In turn, this atom decays into other radionuclides as shown in Fig. 1.1. Short-lived radon decay products (polonium-218, lead-214, and bismuth-214) exist in air as unattached radionuclides, and attached to aerosol particles with the unattached fraction depending on local conditions. They can be removed by deposition on surfaces and ventilation. As radon is an inert gas, nearly all of the radon that is inhaled is subsequently exhaled. However, a large proportion of inhaled radon progeny deposits in the airways of the lungs. Due to their short half-lives, dose is delivered to the lung tissues before clearance can take place, either by absorption into blood or by particle transport to the alimentary tract. Two of these short-lived progeny, polonium-218 and polonium-214, emit alpha particles, the deposited energy of which dominates the dose to the lung. In contrast, doses to systemic organs and gastrointestinal tract regions are low. As a consequence, the equivalent dose to the lung contributes more than 95% of the effective dose following inhalation of radon progeny. The effective dose from the inhalation of radon gas alone is typically less than 10% of that from inhaled radon progeny. Doses depend mainly on the concentration of radon progeny, the duration of exposure, the breathing rate, and the aerosol properties, including the activity size distribution of the radon progeny aerosol and the unattached fraction. If the exposure is characterised by radon gas measurements, a value for the equilibrium factor, F, is required to estimate the concentration of radon progeny in air. For radiological protection purposes, most of the parameters in the dosimetric models, such as breathing rate, correspond to values for Reference Worker or Reference Person. For the dosimetric model considered by the Commission (ICRP, 2014b), two occupational exposure situations have been considered: a mine and a generic indoor workplace. The calculated dosimetric coefficients for these two situations do not distinguish between smokers and non-smokers. This approach is considered appropriate for radiological protection purposes. For dwellings, the dose coefficient has been calculated to be 13 mSv per WLM (Marsh and Bailey, 2013). With this dose coefficient and exposure parameters of F = 0.4 and occupancy of 7000 h year−1, an annual average radon concentration of 300 Bq m−3 corresponds to a dose within, but towards the upper end of, the 1–20-mSv range of reference levels for existing exposure situations. For comparison, a radon concentration of 300 Bq m−3 in homes corresponds to an annual dose of approximately 10 mSv using the epidemiologically derived dose conversion convention (see Para. 27), applying the revised nominal risk coefficient in Publication 115 (ICRP, 2010) and Marsh et al. (2010). A dose coefficient of 11 mSv per WLM has been obtained for exposures in mines using the dosimetric approach, essentially the same as obtained by the dose conversion convention.
2.4. Challenges of managing radon exposure
Control of indoor radon exposure poses many challenges to be addressed by a national radon protection strategy, particularly in terms of public health and responsibilities.
2.4.1. Public health considerations
People are exposed to radon as members of the public in dwellings or as workers in workplaces. They are also exposed to radon in mixed-use buildings as members of the public or as workers. As individuals move between many places in a typical day, a radon protection strategy should ideally provide consistency in the management of the different locations in a given area, and should also provide an integrated approach despite the fact that the time of occupancy varies from one location to another. According to WHO, indoor radon exposure poses a significant public health hazard (WHO, 2009) due to the estimated radon-attributable lung cancer death rates in comparison with other cancers. People spend much of their time indoors, primarily at home. From a public health perspective, as domestic exposure to radon is the most important, a radon protection strategy has to focus primarily on exposure in dwellings rather than in public spaces and workplaces, where premises are under formal management and regulation is more appropriate. Although there are no epidemiological studies of domestic exposure of children to radon, they are generally assumed to be more sensitive to radiation than adults. However, in line with its integrated approach, and given that risk accumulates throughout life, the Commission does not recommend the use of specific indicators and advice for children. Nevertheless, the significant presence of children in a building should be an argument for strengthening awareness and implementing both preventive and mitigating actions as a priority. From a public health perspective, radon reduction is a long-term objective. Prevention of radon exposure is most relevant in new buildings. The implementation of preventive measures in new and renovated buildings provides a good partial solution, with cost-effectiveness increasing with experience and application of building codes (STUK, 2008). This also helps to develop awareness amongst professionals involved in the construction sector. Remediation in existing buildings is also often appropriate in buildings with high radon concentrations. In such situations, there may be a primary source of radon ingress, and radon levels can often be reduced by a factor exceeding 10. There is a large distribution of individual radon exposures, and the evidence of risk of lung cancer exists at levels of long-term average radon concentration below 200 Bq m−3 (ICRP, 2010). As a consequence, the aim should be to reduce both the overall risk for the population and, for the sake of equity, the highest individual exposures to levels that are as low as reasonably achievable. However, the total elimination of radon exposure is not feasible. Radon exposure is not the only source of risk for the population. The radon protection strategy should be properly scaled, with other health hazards and priorities identified in the country taken into account. Furthermore, comparison and integration between the radon protection strategy and other public health policies, such as non-smoking and indoor air quality policies, should be sought in order to avoid inconsistencies and achieve better effectiveness. Considering the ubiquity of radon exposure, and the multiplicity and diversity of situations and decision makers, a straightforward, realistic, and integrated radon protection strategy, addressing most situations with the same approach, is appropriate. It must be supported and implemented on a long-term, potentially permanent basis, and involve all the relevant stakeholders.
2.4.2. Responsibilities of stakeholders
The national radon protection strategy also has to address many challenges in terms of responsibilities, notably the responsibility of the individual householder towards the occupants, of the builder or the seller of a property towards the buyer, of the landlord towards the tenant, of the employer towards the employee, and, generally speaking, of the responsible person for any building towards its users. As radon exposure is mainly a domestic issue, the success of a radon protection strategy depends, to a large extent, on the decisions taken by individuals to reduce the risk in their home, when relevant (self-help protection). Clear awareness among the general population about the risk associated with radon is required, particularly in radon-prone areas, to help individuals in taking their responsibilities. It has to be recognised that, at present, apart from some countries with established radon policies, this awareness is often poor and should be increased. Improvements can be achieved through the development of action plans that describe the risks of radon and the actions that are needed to address it. The provision of a good infrastructure and support for information, measurement, and remediation are prerequisites. The level of enforcement of actions that are warranted is closely related to the degree of legal responsibility for the situation. The owner of a house may have such responsibilities if the house is rented or sold. An employer has a legal responsibility for the health and safety of the employees. The manager of a school (or the local authority) may have a legal responsibility for the health of the pupils as well as the staff. The same consideration may apply to other public buildings and workplaces. The requirements related to such responsibilities should be commensurate with the wider public health policy in the country. The issue of responsibility clearly shows the need for a graded approach in defining and implementing a radon protection strategy. Such a graded approach should be based on both ambition and realism.
3. ICRP System of Radiological Protection Against Radon Exposure
The Commission’s system of radiological protection is described in Publication 103
1
At the time of writing of the present publication, the Commission was revising the glossary in Publication 103 because of some imperfections and inconsistencies with the text, so this publication refers to the text of Publication 103 rather than to its glossary.
Indoor radon exposure is controllable as the pathways from the source to the exposed individuals can be largely controlled or influenced. Outdoor radon concentrations at ground level can be high, but the radon gas is normally diluted through dispersion into the atmosphere, so concentrations in the ambient air are generally rather low, up to a few tens of Bq m−3 (UNSCEAR, 2009), apart from some limited areas with very high exhalation of radon. As neither the source nor the pathways can reasonably be controlled, the Commission considers that human exposure to outdoor radon is not reasonably amenable to control, except in cases where very high outdoor concentrations arise from a source enhanced by human activities.
3.1. Exposure situations and categories of exposure
3.1.1. Types of exposure situations
An exposure situation is the process that includes a natural or man-made radiation source and the transfer of radiation through various pathways leading to the exposure of individuals. The recommendations in Publication 103 (ICRP, 2007) organise radiological protection according to three types of exposure situations: planned exposure situations, emergency exposure situations, and existing exposure situations. Planned exposure situations are situations resulting from the deliberate introduction and operation of sources. Exposures can be anticipated and fully controlled. Emergency exposure situations are situations resulting from the loss of control of the source, and urgent action is necessary in order to avoid or reduce undesirable consequences. They also include exposures resulting from a malicious act or from any other unexpected situation. Existing exposure situations are situations where the source already exists when a decision is taken to control the related exposure. They include exposures from natural radiation sources as well as exposures from past events, accidents, and practices. Characterisation of the pattern of exposures in these situations is prerequisite to their control. Radon exposure situations have the characteristics of existing exposure situations as the source is unmodified concentrations of ubiquitous natural activity in the earth’s crust. Human activities can create or modify pathways, increasing indoor radon concentrations compared with outdoor background levels. These pathways can be modified by preventive and mitigating actions. The source itself, however, cannot be modified and already exists when a decision of control has to be taken. Radon in dwellings and workplaces are given as examples of existing exposure situations in Publication 103 (ICRP, 2007, Para. 284). Exposure to radon in uranium mining is often managed in the same way as a planned exposure situation, because uranium mining is part of the nuclear fuel cycle and also because workers are occupationally exposed to other radiation sources as well as radon, such as external exposure to gamma radiation, and inhalation or ingestion of dust. It is for national authorities to decide which other radon exposure situations involving workers are to be regarded from the outset as planned exposure situations. Radon is not likely to give rise to an emergency exposure situation despite the fact that the discovery of very high concentrations in a place can require the prompt implementation of protective actions, particularly when the exposure affects other occupants for whom the decision maker for a property has a duty of care. The philosophy of Publication 103 (ICRP, 2007) compared with Publication 60 (ICRP, 1991) is to recommend a consistent approach for the management of all types of exposure situations. This approach is based on application of the optimisation process below appropriate dose restrictions (i.e. dose constraints or reference levels).
3.1.2. Categories of exposures
The Commission distinguishes between three categories of exposure: medical exposure, occupational exposure, and public exposure. Occupational exposure is radiation exposure of workers incurred as a result of their work. However, because of the ubiquity of radiation, the direct application of this definition to radiation would mean that all workers should be subject to a regime of radiological protection. The Commission therefore limits its use of ‘occupational exposures’ to radiation exposures incurred at work as a result of situations that can reasonably be regarded as being the responsibility of the operating management (ICRP, 2007, para. 178). In most workplaces, radon exposures are adventitious (i.e. they are not caused by, or associated with, the nature of the work undertaken, but arise simply through workers and others being present in the employer’s premises). Publication 65 (ICRP, 1993, Para. 86) indicates that ‘workers who are not regarded as being occupationally exposed to radiation are usually treated in the same way as members of the public’. This is still valid, considering that the health and safety of the workers continue to be the responsibility of their employer. In other words, in general workplaces where radon exposure is adventitious, radon is not managed by controlling individual exposures, but by controlling the building or location in order to ensure the overall protection of its occupants. In cases where radon exposure is concomitant with exposure in a planned exposure situation (e.g. radon exposure in a nuclear facility or in a hospital radiology department), the Commission recommends a pragmatic approach. Radon exposures of workers should only be part of their overall occupational exposure if this is necessary within the specific graded approach for workplaces, as described in Section 3.3.5. The Commission’s approach to the management of radon exposure is also directly related to the type of location. Publication 65 (ICRP, 1993) makes a distinction between the approach to protection in dwellings and the approach to protection in workplaces. Considering that a given individual typically moves from place to place, in dwellings, workplaces, and mixed-use buildings, in the same area, the Commission now recommends an integrated and graded approach to protection in all buildings using the requirements for public exposure. In addition, the Commission considers that it is appropriate to apply its occupational exposure requirements in some workplaces that are identified on the basis of either the reference level, as a quantitative criterion, or a list of activities or facilities, as qualitative criteria (see Section 3.3.5). Due to this new approach, the Commission no longer uses the term ‘entry point’, introduced in Publication 103 (ICRP, 2007, Para. 298), to describe the concentration above which occupational protection requirements apply to radon exposure in workplaces.
3.2. Justification of protection strategies
In the ICRP system of protection, the principle of justification is one of the two source-related fundamental principles (ICRP, 2007, Para. 203). In application of this principle, any decision that alters the radiation exposure situation should do more good than harm. This means that by introducing a new radiation source, by reducing existing exposure, or by reducing the risk of potential exposure, one should achieve sufficient individual or societal benefit to offset the detriment caused. Radon exposure can be controlled mainly by actions that modify the pathways of exposure, and not normally by direct action on the source. In these circumstances, the principle of justification is applied in making the decision regarding whether or not a protection strategy against radon exposure is implemented. Such a decision, which will always present some disadvantages, should be justified in the sense that it should do more good than harm (ICRP, 2007, Para. 207). The responsibility for judging the justification of radon protection strategies to ensure an overall benefit to the society falls on governments or national authorities. The characterisation of the situation, such as the assessment of radon concentrations and the identification of radon-prone areas, as well as considerations about public health priorities and social and economic factors, are necessary for national authorities to determine whether or not a radon protection strategy is justified in a country. The Commission considers that there are many arguments which provide broad justification of the implementation of national radon protection strategies. These include:
radon is a significant source of radiation exposure, and is the second cause of lung cancer in the general population after smoking; radon exposure can be controlled, as feasible techniques exist to prevent and mitigate high indoor radon concentrations; and a radon protection strategy can have positive consequences on other public health policies such as indoor air quality and non-smoking policies. Reducing the radon concentration contributes to mitigate the health effects of tobacco. Although radon is much more likely to cause lung cancer in people who are smokers, or who have smoked in the past, than in lifelong non-smokers, the evidence suggests that it is the primary cause of lung cancer among people who have never smoked (WHO, 2009). The excess relative risk is comparable for smokers and non-smokers. In practice, it would be difficult to address the radon issue separately or differently for smokers, non-smokers, passive smokers, or past smokers. For example, smoking can be restricted inside a building, but it would not be practical to limit a person’s access to a building based on their individual smoking status. In the workplace context, discrimination between smokers and non-smokers would cause ethical and social problems, which are not in the competence of the Commission. The Commission’s recommendations for the management of radon exposure do not differentiate between smokers and non-smokers.
3.3. Optimisation of protection
Optimisation of protection is the second fundamental principle of radiological protection, and is central to the system of protection. It is source-related, in common with the principle of justification, and applies to planned, emergency, and existing exposure situations. According to the principle of optimisation, the likelihood of incurring exposures, the number of people exposed, and the magnitude of their individual doses should all be kept as low as reasonably achievable, taking economic and societal factors into account. This means that the level of protection should be the best possible under the prevailing circumstances, maximising the margin of benefit over harm. In order to avoid severely inequitable outcomes of this optimisation procedure, there should be restrictions on the doses or risks to individuals from a particular source (dose or risk constraints and reference levels) (ICRP, 2007, Paras 203 and 211). Implementation of the optimisation principle of protection is a process that is at the heart of a successful radiological protection programme. It must be framed carefully to consider the relevant attributes of the exposure situation. Furthermore, it should include, as appropriate to the exposure situation, the involvement of the relevant stakeholders. The Commission considers these two elements to be important components of the optimisation process (ICRP, 2006b, Para. 23).
3.3.1. Reference level
In Publication 65 (ICRP, 1993), the Commission considered that some remedial measures against radon in dwellings were almost always justified above a continued annual effective dose of 10 mSv. The Commission also considered that it is logical to adopt an action level for intervention in workplaces at the same level of effective dose as the action level for dwellings. Given that, for simple remedial measures, a somewhat lower figure could be considered, the Commission recommended using a range of approximately 3–10 mSv as a basis for adopting action levels for intervention in dwellings or workplaces. An action level was defined as the annual mean concentration of radon at which intervention is recommended to reduce the exposure in a dwelling or a workplace. In Publication 103 (ICRP, 2007), the Commission abandoned the concept of an action level, and instead introduced the concept of a reference level in conjunction with the optimisation principle. The reference level represents, in emergency and existing controllable exposure situations, the level below which the goal is to reduce all doses to a level that is as low as reasonably achievable, taking economic and societal factors into account. The reference level is also the level above which it is judged to be inappropriate to allow exposures to occur. The consequence of using the concept of reference level instead of the concept of action level is that optimisation should be applied as appropriate above and below the reference level, and not only above. It must be kept in mind that reference levels do not represent a demarcation between ‘safe’ and ‘dangerous’, or reflect a qualitative change in the associated health risks for individuals. According to Publication 103 (ICRP, 2007), the chosen value for a reference level depends upon the prevailing circumstances of the exposure situation under consideration (ICRP, 2007, Para. 234). In order to provide guidance for selecting appropriate values, the Commission has defined a dose scale (ICRP, 2007, Table 5) reflecting the fact that, within a continuum of risk (linear non-threshold assumption), the risk that someone is willing to accept depends on the exposure circumstances. This scale is divided into three bands reflecting greater or lesser need for action, which is dependent upon the characteristics of the exposure situation: controllability of the source; individual or societal benefit from the situation; and requirements with regard to information, training, and dosimetric or medical surveillance. Numerically speaking, the three bands for acute or annual doses are: <1 mSv, 1–20 mSv, and 20–100 mSv. According to Publication 103 (ICRP, 2007), reference levels for existing exposure situations should typically be set in the 1–20-mSv band. This applies when individuals receive direct benefits from the exposure situation, and when exposures may be controlled at source or, alternatively, by action in the exposure pathways, so that general information should be, where possible, made available to enable individuals to reduce their doses. Radon exposure cannot normally be controlled at the source (apart from a few exceptions), but can be controlled through many pathways by preventive and mitigating actions, which are not disproportionately disruptive. People generally receive an obvious direct benefit from being indoors. Thus, there is a benefit from continuing to use or live in a building rather than moving to another building or even another area. In Publication 103 (ICRP, 2007), the Commission retained the upper value of 10 mSv of effective dose, adopted in Publication 65 (ICRP, 1993), for the individual reference level. This value, which is in the middle of the 1–20-mSv band, is consistent with the rationale provided in Publication 103 (ICRP, 2007, Table 5). For the sake of continuity and practicality, the Commission continues to recommend a reference level of the order of 10 mSv year−1. The Commission also recommends the use of a derived reference level given in terms of an indoor radon concentration (in Bq m−3), which is a measurable quantity.
3.3.2. Derived reference level for radon
In its Statement on Radon (ICRP, 2010), the Commission reduced the derived reference level for radon gas in dwellings from 600 Bq m−3 [published in the 2007 Recommendations (ICRP, 2007)] to 300 Bq m−3, based on epidemiological considerations. The Commission continues to recommend 300 Bq m−3 as the upper value of the derived reference level for radon gas in dwellings. While there is no unique annual dose associated with 300 Bq m−3, it is clear that the vast majority of annual doses that would be incurred by this level of radon lie within the range (1–20 mSv year−1) that the Commission has identified as appropriate for relevant existing exposure situations. In its Handbook on Indoor Radon, WHO stated that a national reference level for dwellings of 100 Bq m−3 is justified from a public health perspective, but recognised that this level cannot be implemented in many countries (WHO, 2009). The value of 300 Bq m−3 is already introduced in standards such as the International Basic Safety Standards (IAEA, FAO, ILO, OECD/NEA, PAHO, UNEP, WHO, 2011) and the European Basic Safety Standards (EURATOM, 2014) that were revised recently. As stated in Publication 103 (ICRP, 2007, Para. 295), it is the responsibility of the appropriate national authorities, as with any other controllable radiation source, to establish their own national derived reference levels, taking the prevailing economic and societal circumstances into account, and to apply the process of optimisation of protection in their country. The Commission strongly encourages these authorities to set a national derived reference level that is as low as reasonably achievable in the range of 100–300 Bq m−3. It is important to note that derived reference levels relate to the annual mean concentration of radon in a building or location. Moreover, although the absolute risk of lung cancer arising from radon exposure is significantly greater in smokers than non-smokers, the Commission’s recommendations for protection against radon do not distinguish between smokers and non-smokers. As individuals move from place to place in the same area, a radon protection strategy should be developed by national authorities, and implemented in a consistent and integrated manner in the various locations. As a consequence, the Commission recommends, a priori, use of the same derived reference level in dwellings and in mixed-use buildings (e.g. schools, hospitals, shops, cinemas) that have access for both members of the public and workers, and, by extension, in workplaces without public access when radon exposure is not considered as occupational (e.g. office buildings, typical workshops).
3.3.3. Optimisation process
According to Publication 101, Part 2 (ICRP, 2006b, Para. 22), ‘to provide the best protection under the prevailing circumstances (in normal, emergency, or existing controllable situations), the process of optimisation below a dose restriction must be implemented through an ongoing, cyclical process (called the optimisation process) that involves evaluation of the exposure situation to identify the need for action (framing of the process); identification of the possible protective options to keep the exposure as low as reasonably achievable; selection of the best option under the prevailing circumstances; implementation of the selected option through an effective optimisation programme; and regular review of the exposure situation to evaluate if the prevailing circumstances call for the implementation of corrective protective actions’. In relation to optimisation, the Commission considers that distinction should be made between prevention, which aims to maintain the expected exposure at a level that is as low as reasonably achievable under the prevailing circumstances, and mitigation, which aims to reduce the residual dose to a level that is as low as reasonably achievable (see Fig. 3.1). For radon exposure, prevention focuses on the implementation of building codes in order to avoid high indoor radon concentrations in new buildings, while mitigation focuses on the reduction of high radon concentrations in existing buildings through the use of techniques such as managed ventilation. The objective of the optimisation process is to reduce the overall risk to the general population and, for the sake of equity, the individual risk to the most exposed individuals, i.e. those in the upper-end of the distribution of individual exposures (see Fig. 3.2). In both cases, the process includes the management of buildings or location, and should result in radon concentrations in ambient indoor air that are as low as reasonably achievable below the national derived reference level. In a given building, after successful implementation of management actions, the only ongoing requirements would be to perform routine inspection and maintenance of the mitigation system, and periodic monitoring to ensure that radon levels remain low. The aim to significantly reduce the risks of radon to the general population has a time frame of several decades rather than several years. Optimisation of protection from radon exposures in buildings and locations can be determined using standard optimisation techniques, including cost–benefit analysis and multi-attribute techniques. All relevant attributes, such as technical, economic, societal, and ethical, must be taken into account, with due consideration to the issue of equity, particularly for very high ongoing exposures. Thus, comparisons can be made between the financial costs associated with the estimated number of cases of lung cancer that are likely attributable to radon at different levels of exposure, the selection of preventive and protective actions for a given population, and the costs of those actions to reduce radon exposures (HPA, 2009; WHO, 2009). Such analyses can be used to inform decisions on the cost-effectiveness of measures to reduce radon levels in existing properties and new buildings. Implementation of the optimisation principle. ALARA is as low as reasonably achievable, taking economic and societal circumstances into account. Use of a reference level in an existing exposure situation, and evolution of the distribution of individual exposures with time as a result of the optimisation process.
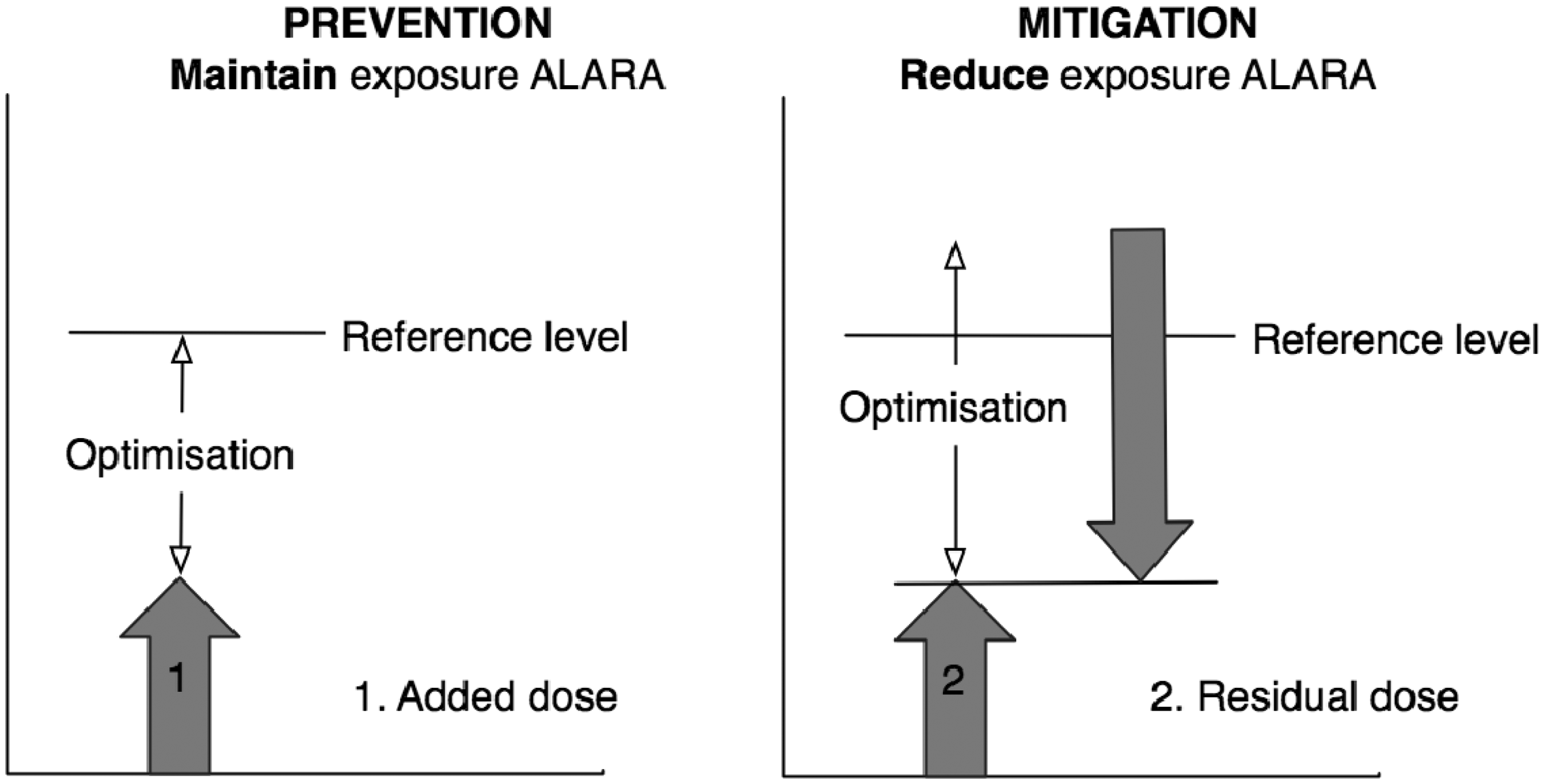
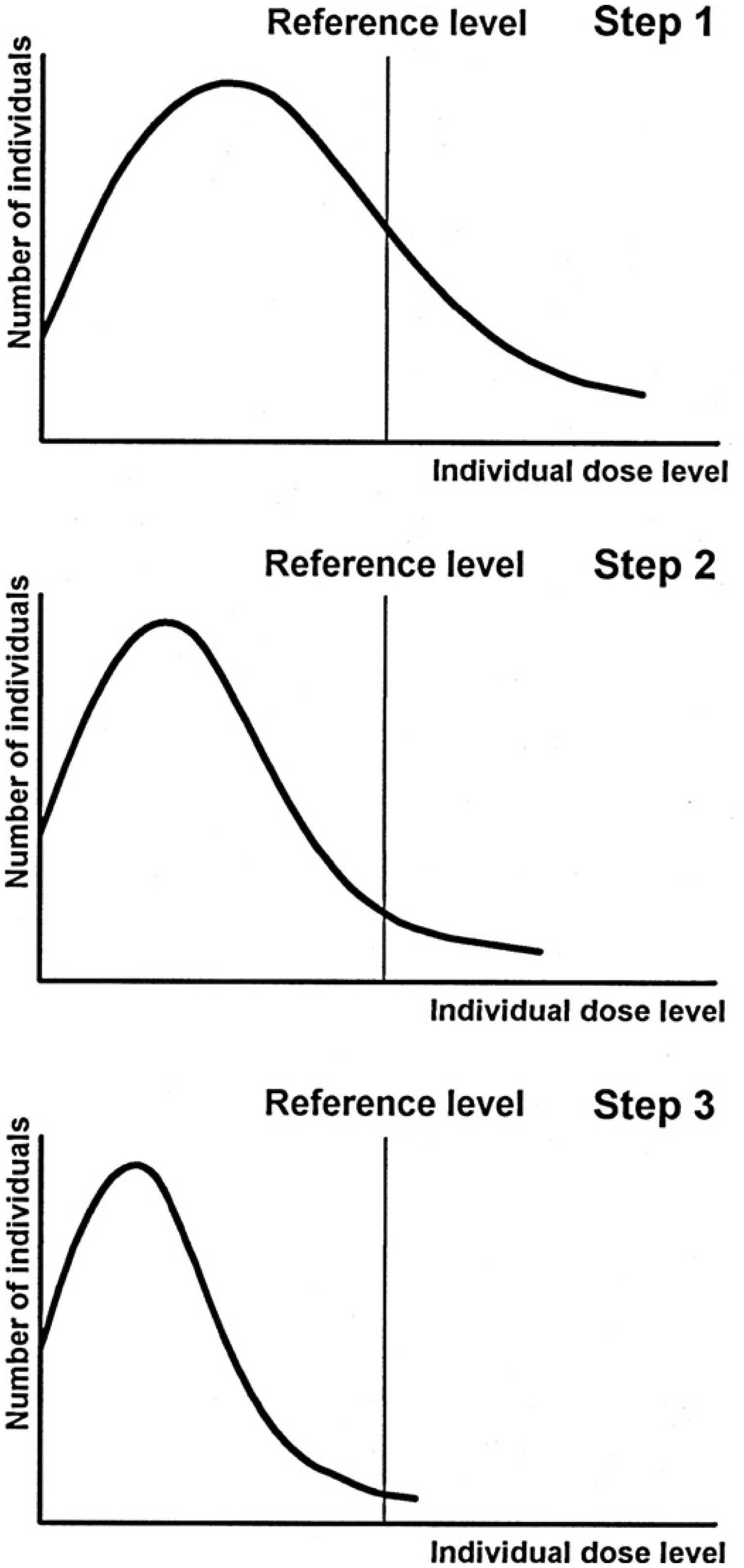
3.3.4. National derived reference level
As stated previously, it is the responsibility of the appropriate national authorities, as for any other controllable radiation sources, to establish their own national derived reference levels in terms of indoor radon concentration (in Bq m−3), taking the prevailing economic and societal circumstances into account, and to apply the process of optimisation of protection in their country. As stated in Section 3.3.2, the Commission strongly encourages national authorities to set a national derived reference level that is as low as reasonably achievable in the range of 100–300 Bq m−3. The first step is to characterise the exposure situation of individuals and the general population in the country, as well as other relevant economic and societal criteria, and the practicability of mitigating or preventing the exposure. The appropriate value for the derived reference level may then be established by a process of generic optimisation that considers national or regional attributes and preferences, together, where appropriate, with consideration of international guidance and good practice elsewhere. Many factors such as mean radon concentration and radon distribution, number of existing homes with high radon levels, etc. should be taken into consideration. When a national derived reference level has been established, preventive and mitigating actions should be undertaken to help achieve a substantial reduction in radon exposures, as required. It is not sufficient to adopt marginal improvements with the aim of reducing radon concentrations to a value just below the national derived reference level. The national derived reference level should also be applied at the design stage of any new building, whatever its purpose. The value of the national derived reference level for radon exposure should be reviewed periodically to ensure that it remains appropriate.
3.3.5. Graded approach
The Commission now recommends that a graded approach should be applied for the control of radon exposures. In such an approach, the radon protection strategy should start with a programme aimed at encouraging relevant decision makers to promote self-help protective actions, such as measurement and, if needed, remediation. This process can be implemented through information, advice, incentives, practical assistance and, where necessary, more formal requirements. The level of enforcement of these various actions should be dependent upon the degree of legal responsibility for the situation, and the level of ambition of the national radon protection strategy. The radon protection strategy should include a programme of actions including provision of general information on radon behaviour and risk, campaigns aiming to increase awareness among the targeted public, campaigns of concentration measurements, and organisation of technical or financial support for measurements and remediation actions (see Section 4). These actions may be implemented preferentially in certain areas, such as radon-prone areas, and in buildings that are heavily occupied. This might include buildings that are occupied by many people, or those that have occupants who are present, often residentially, for a high proportion of the time. In situations involving legal responsibilities (e.g. employer/employee, landlord/tenant, builder/buyer, seller/buyer, public building with high occupancy), some mandatory provisions may be required. Mandatory provisions, commensurate with the degree and type of responsibility, may be more appropriate than incentive-based provisions if an assessment indicates that they would be more effective under the prevailing circumstances. Such provisions could be to ensure good traceability, record keeping, and compliance with the derived reference level. A radon protection strategy should ensure that requirements are commensurate with the means available to the responsible persons or organisations, and that the benefit in terms of risk reduction outweighs the disadvantages. For example, requirements should not deter people from initial radon measurements, result in reduced property value, or involve excessive procedures. Where a building has high radon concentrations, the response should include the involvement of, and communication with, relevant stakeholders, such as the building users. In cases of non-compliance with the reference level, the consequences should also be adapted to the situation. For example, the consequences for those responsible for the dwellings could be to provide the result of the measurement (e.g. to an authority or the buyer) or the obligation to undertake remediation. In most workplaces, radon exposures of workers are adventitious and are more related to the location than the work activity. Such exposures are not considered as occupational, as defined by the Commission. These considerations are without prejudice to the legal responsibility of the employer towards its employees. Workplaces in this category include most mixed-use buildings, such as schools, hospitals, post offices, jails, shops, cinemas, office buildings, and general workshops. In all workplaces where radon exposure is regarded as being adventitious and not considered as occupational, the first step of the graded approach consists of managing the working location using the national derived reference level (300 Bq m−3 or less) and implementing the optimisation process. The legal responsibility of the employer towards its employees is exercised by applying the regulatory requirements, consensus standards, or other standards that may be laid down for the control of radon exposure in buildings as part of implementation of the national radon strategy. The relationship between a measured radon concentration and effective dose depends upon several parameters including the equilibrium factor, the time of exposure, etc. that can vary greatly between locations. Therefore, if the derived reference level is exceeded in a workplace, this does not necessarily mean that the dose reference level, representing annual doses of approximately 10 mSv, would be exceeded. Consequently, in workplaces, if difficulties are encountered in keeping indoor radon concentrations below the derived reference level, the radon protection strategy should provide, as a second step of the graded approach, the possibility to undertake further investigation using a more realistic approach. This means making an assessment of radon exposure, taking the actual parameters of the exposure situation into account (e.g. actual time of occupancy, measurements of radon progeny). Doses calculated in this way should be compared with the dose reference level of 10 mSv year−1 to decide on the need for, and type of, further action. At this stage, the aim is still to ensure the overall protection of the users of the building, rather than to control doses to specific individuals. In workplaces where, despite all reasonable efforts to reduce radon exposure, individual doses persist above 10 mSv year−1, the workers should be considered as occupationally exposed and their exposure should be managed using the relevant radiological protection requirements established for occupational exposure: identification of the exposed workers, information, training, dose monitoring (in doses or potential alpha energy concentration) and recording, and health surveillance. In any case, the individual doses should not exceed the upper value of the 1–20-mSv band for the setting of reference levels in existing exposure situations. This is the third step of the graded approach. In some specific types of workplaces, national authorities may decide that exposure of workers to radon should be considered as occupational regardless of being above or below a reference level, because the workers are inevitably and substantially exposed to radon, and their exposure to radon is more intimately or obviously related to their work activities. A list of such workplaces or work activities (e.g. mines and other underground workplaces, thermal spas) should be established nationally. In workplaces where radon exposure of workers is considered to be occupational, the Commission recommends that the relevant locations should be identified. This might be parts of a building, individual buildings, or parts of a site. Within these locations, the employer should meet the relevant occupational exposure requirements and apply the optimisation principle. If the national authorities decide that a radon exposure situation should be regarded as a planned exposure situation, the dose restriction is likely to be ensured through an occupational dose limit (see Section 3.4). In the view of the Commission, the decision regarding whether or not exposure of workers to radon is considered as occupational should be made by the national authorities.
3.4. Application of dose limits
According to Publication 103 (ICRP, 2007, Para. 203), the principle of application of dose limits is the third fundamental principle of the ICRP system. It is individual-related and only applies for planned exposure situations. It means that the total dose to any individual from regulated sources in planned exposure situations, other than medical exposure of patients, should not exceed the appropriate limits recommended by the Commission. For the sake of consistency, dose limits should apply in radon exposure situations that national authorities have decided, from the outset, are planned exposure situations, typically when workers are considered as occupationally exposed. The dose limit recommended by the Commission for occupational exposure is expressed as an effective dose of 20 mSv year−1, averaged over defined 5-year periods (100 mSv in 5 years), with the further provision that the effective dose should not exceed 50 mSv in any single year (ICRP, 2007, Para. 244).
3.5. Summary
Fig. 3.3 shows the general approach now recommended for the management of various radon exposure situations. General approach for the management of radon exposure. ALARA is as low as reasonably achievable, taking economic and societal circumstances into account. *Workplaces where, from the outset, radon exposure is considered as occupational by national authorities.

4. Implementation of Protection Strategies
4.1. National action plan
A national radon action plan should be established by national authorities with the involvement of relevant stakeholders. The objective is to reduce the collective risk of the population and the individual risk to indoor radon exposures by implementing the optimisation principle. The action plan should establish a framework with a clear infrastructure, determine priorities and responsibilities, and describe the successive steps to deal with radon in the country. Depending on the exposure conditions, it should identify the various stakeholders, notably those who are exposed and those who should provide support or take action. In addition, the action plan should address ethical issues – particularly those associated with responsibilities – and provide information, guidance, support, and conditions for sustainability. The national radon action plan should, as far as possible, be integrated in a manner consistent with other strategies concerning buildings, such as indoor air quality or energy saving, in order to develop synergies and avoid contradictions. Implementation of the national radon action plan needs cooperation between national, regional, and local authorities competent in different domains (i.e. radiological protection, public health, labour, land planning, housing, building construction, etc.), different professional disciplines (i.e. architects and other building professionals, radiological protection professionals, public health inspectors, medical professionals, etc.), different types of supporting organisations (i.e. experts, supporting agencies, associations, etc.), and different responsible individuals or institutions. The action plan may contain both incentive-based and mandatory provisions. Given that responsibility for taking action against radon will often fall on individuals who cannot be expected to perform a detailed optimisation exercise, the action plan should provide appropriate information and support to those individuals to be able to address the radon issue themselves through self-help protective actions, such as self-measurement or access to appropriate measurement services, proper use of buildings, and simple remediation techniques. A national radon survey should be conducted, using recognised radon measurement devices and protocols, to determine the radon concentration distribution that is representative of radon exposure of the population of a country. The two key objectives of a national radon survey should be:
to estimate the average exposure of the population to indoor radon and the distribution of exposures, which can be best achieved by a population-weighted survey in representative selected homes in which long-term radon measurements are performed; and to identify areas where significantly high indoor radon concentrations are more likely to be found (i.e. radon-prone areas). Screening for these areas can be best achieved coupled with long-term radon measurements in selected homes. Radon maps can be used as a tool to optimise the search for homes and other buildings with high radon concentrations, and to identify areas for special preventive actions during the planning and construction of new buildings. However, estimates resulting from these surveys should be verified by ongoing measurements in selected buildings in suspected radon-prone areas. Radon-prone areas can be identified indirectly by using radon gas concentrations in soil (provided that there are established transfer factors correlating radon concentrations in homes to radon gas concentrations in soil beneath the foundations of a building), or directly by using indoor radon measurements. Geological information can be used as part of this process. However, various definitions of a radon-prone area exist in different countries. It could be defined using administrative or other established geographical divisions, and be based on different criteria such as the average concentration (i.e. arithmetic mean value, median value for a geometric distribution), the proportion of buildings exceeding the derived reference level, and the probability of exceeding that level. The definition of a radon-prone area should be specified in the national radon action plan. Even in confirmed radon-prone areas, the distribution of radon concentrations in buildings is often quite wide, and values can be low in most of them. Conversely, even in areas not classified as radon-prone areas, buildings with high radon concentrations can be found, albeit with a lower probability. Therefore, as well as identifying radon-prone areas, some efforts should also go into the identification of building characteristics that can be associated with higher radon concentrations. The national radon action plan may comprise mandatory provisions, especially in the case of legal responsibilities. For example, measurements, communication of the results, record keeping, and compliance with the derived reference level may be imposed. However, the national radon action plan should also include incentive-based and supportive measures, such as organising measurement campaigns, and inclusion of radon protection in housing improvement programmes, with financial support or fiscal measures where appropriate. Such measures should be repeated regularly. In the national action plan, consideration should be given to any building with public access, with priority given to those with extended public occupancy such as schools, kindergartens, care institutions, hospitals, and jails. People present in these buildings often have no choice but to use them, and can spend a significant part of their time inside, although it may be a temporary situation. They may not be aware that they are exposed to elevated concentrations of radon, and they are not in a position to reduce the exposure levels themselves. For buildings used by both members of the public and workers, the derived reference level should be the level used for dwellings. The use of different reference levels within the same enclosed location is not recommended. Furthermore, preventive and mitigating actions should be implemented in order to achieve compliance with the derived reference level. Monitoring, as well as record keeping, of radon concentrations may be required. Relevant information should be provided to members of the public using the building and staff working inside the building. Appropriate support should be provided to people responsible for this type of building in order to ensure that they are able to fulfil their responsibilities and obligations. The national action plan can provide a graded approach applicable to buildings with public access, such as workplaces under the control of the national authorities (see Section 3.3.5).
4.2. Prevention
A radon protection strategy should include preventive actions to control future radon exposure. Regardless of the indoor location, the category of individuals present, and the type of exposure situation, it is possible to address radon exposure by considering the issue of radon exposure during the planning, design, and construction phases of a building. Preventive actions are implemented through land planning and building codes for new buildings, and for renovation of old buildings.
4.2.1. Regional and local land planning
The potential for any building to have a high indoor radon concentration is highly variable, notably due to the large variation in geological conditions. This variability should be taken into account during regional and local land-planning processes, at least in radon-prone areas. Local radon maps may be established on the basis of geological data, radon measurements in the soil, or indoor radon measurements in existing buildings (see Section 4.1). They should be complemented by data on radon concentrations in buildings, in water supplies from drilled wells, etc. Local radon maps and appropriate data should be made available for relevant local, regional, and national authorities; building professionals; home builders; and the general population to help them in planning, constructing, and renovating buildings. Land planning might be mandatory, for which a radon map remains a useful tool, but it cannot be considered to give definitive results. It is not possible to predict the radon concentration in a given building before construction. Further investigation, such as measurements in soil, might be useful. However, as the radon concentration in a building is dependent on many factors, only a measurement in the finished and occupied building is able to provide a relevant result. A radon map should not result in areas where buildings are forbidden because of radon concentrations, except in very exceptional cases.
4.2.2. Building regulations and codes
National, regional, and/or local authorities should consider the implementation of building regulations or building codes that require radon prevention measures for homes and buildings under construction or major renovations. Implementing radon prevention measures during the design and construction of a building is considered to be the most cost-effective way to protect the overall population. If implemented correctly, such measures will, over time, reduce the national average level of radon, and decrease the number of new buildings with radon concentrations above or close to the national derived reference level. Ensuring compliance with building regulations and codes is important. Quality assurance programmes should be implemented at the level of professionals or at a regulatory level, as appropriate. It is important to note that these building regulations and codes alone cannot guarantee that radon levels in new buildings will be below the derived reference level. Therefore, building owners and managers should be made aware that the only way of knowing the radon situation of the building is through measurement. If necessary, postconstruction radon mitigation approaches should be considered.
4.3. Mitigation
A national radon protection strategy should also include mitigation actions for existing buildings or locations with enclosed spaces. The control of exposure should be ensured as far as possible through the management of the building (or location) and the conditions of its use, regardless of the category of individuals inside. The main steps are measurements and, when needed, protective actions.
4.3.1. Radon measurement techniques and protocols
Radon measurements in a given building or location should be targeted to produce a reliable estimate of the long-term radon exposure of the occupants, considering many factors such as the building occupancy, and the daily or seasonal variability of the concentration. Consistency and quality assurance among radon measurements are important prerequisites. Therefore, radon measurement protocols should be established, reviewed regularly, and updated as necessary. Standardised measurement methods have been developed (ISO, 2012a–g). Ideally, long-term measurements over a whole year, and therefore covering all seasons, are preferred over short-term estimates. However, shorter periods of a few weeks to months are often chosen as difficulties may arise when the period is too long, as detectors tend to be moved or forgotten. Reliable measurements should be representative of the average annual concentration, and seasonal adjustments may be used. The measurements should be accomplished at low to modest costs. Measurement devices should be easily available with clear instructions about their use. After mitigation, a measurement is needed in the same conditions as the initial measurement to test the effectiveness of the mitigation system. Measurements should be repeated periodically to ensure that the situation does not deteriorate. When using radon-222 progeny measurements in dwellings and general workplaces, conversion to the radon concentration is implemented by assuming a default generic equilibrium factor of 0.4 between indoor radon gas and its progeny, unless evidence shows otherwise.
4.3.2. Methods for mitigating radon exposure and their applicability in different situations
The main ways to achieve mitigation of radon exposure are to prevent radon inflow from entering occupied spaces, and to extract radon from indoor air using both passive and active techniques. The primary radon mitigation techniques aim to reduce convection and diffusion radon intake from the soil under the building, and focus on the following actions:
re-inforce the air tightness of the shell of the building (e.g. sealing radon entry routes); and reverse the air pressure differences between the indoor occupied space and the outdoor soil through different soil depressurisation techniques (e.g. reducing the pressure in the soil beneath the building, installing a radon sump system, applying an overpressure in the cellar, etc.). Reduction of the indoor radon concentration by dilution with outside air is another mitigation technique used in dwellings. Mitigation is achievable by passive or active means that manage the ventilation of occupied spaces. In heating or cooling an indoor environment, balanced ventilation may be used. Balanced exhaust ventilation neither pressurises nor depressurises the indoor air condition in relation to the pressure of air in soil and outdoors. This ventilation technique dilutes radon after it has entered the building. Fan-powered ventilation can dilute indoor radon after it enters the building, and can reduce pressure differences between the soil and the occupied space. Some of these solutions are not suitable for all types of building, nor are they suitable for all levels of radon. In several cases, a combination of these techniques provides the greatest reduction in radon concentration. For buildings where an artesian borehole serves as the water supply source, this water may be a potential source of radon. When water degasses radon into the room atmosphere (especially during water spraying), significant short-term exposures may occur. Techniques for mitigating the entry of radon into ambient air from water principally involve degassing the water prior to its use, or water filtration on beds of active charcoal. Detailed guides presenting the different mitigation techniques, developed by national or international bodies, are available (WHO, 2009).
4.4. Building materials
Building materials are generally of minor importance for radon exposure, but there can be special cases with a radon-222 source that cannot be neglected. Further, the thorium concentration in building materials (concrete, bricks, etc.) is usually the only source of radon-220 in indoor air. Hence, the control of thorium concentrations in building materials used for surface dressing (plaster, etc.) of walls, ceilings, and floors can decrease the probability of elevated radon-220 levels in buildings. To prevent and optimise the impact from building materials, materials with low levels of radium-226 and thorium-232 should be preferred. A benchmark system has been established (i.e. radioactive concentration index) in order to characterise the risk associated with gamma radiation emitted by specific building materials, and to specify the conditions of their use (EC, 1999). In general, if building materials are controlled with regard to gamma radiation, radon exhalation does not cause indoor radon concentrations that are significant in comparison with the derived reference level. The use of building materials emitting high quantities of radon-220 or radon-222 would require justification.
4.5. Protection of workers
In workplaces where workers’ exposure to radon is not considered as occupational, workers are treated in the same way as members of the public for radiological protection purposes. However, when workplaces are not accessible by the public (or when public access is for a very limited period of time), some specific or complementary provisions may be established within the optimisation process as part of application of the graded approach to protection. Such provisions may be:
specific measurement protocols (e.g. measurement when and where the workers are present); specific use of the derived reference level according to the actual exposure parameters, such as time of occupancy or equilibrium factor, keeping the value of 10 mSv year−1 as the dose reference level; arrangement of working conditions (e.g. by limiting the time of occupancy in some premises); and requirements concerning implementation of measurements, communication of the results, record keeping, and compliance with the reference level. External expertise may be needed to implement such specific provisions, as well as supervision of the national authorities. In workplaces where exposure of workers to radon is considered as occupational, the operating management and the national authorities will need to determine which requirements need to be met. The requirements generally relevant for radon exposure are:
setting an appropriate reference level, expressed as effective dose, radon concentration, or potential alpha energy concentration, taking the time of occupancy into account; determination of the working areas concerned; although the classification of controlled or supervised areas does not fit well, it remains important to determine the area in which occupational exposure may occur, and to control, as appropriate, access to such areas; adequate information, instruction, and training of workers; use of personal protective equipment in some exceptional cases; monitoring of exposures through individual monitoring, collective monitoring, or, if inappropriate, inadequate, or unfeasible, inferred from monitoring of the workplace; recording of exposures; provision of health surveillance for workers; promotion of the radiological protection culture; and compliance with the reference level. This can involve area workplace monitoring combined with tracking time in specific work locations. Personal radon monitors can also be used either as a group average or on an individual basis. In any case, a dose of 20 mSv year−1 should not be exceeded.
4.6. Protection of workers against radon in the uranium mining industry
National authorities may decide to manage some occupational exposures to radon as planned exposure situations from the outset. This is typically the case for the uranium mining industry. Factors that influence this choice include the levels of exposure to other sources in the mine, including external exposure to gamma radiation, and inhalation or ingestion of radioactive dusts. The long-lived radioactive dust can be uranium ore during the mining and initial stages of milling, and/or the refined uranium product, often a uranium oxide powder. In addition, there can be potential exposures to other uranium decay series radionuclides, depending upon the process. In uranium mines, radon progeny may be the dominant source of radiation exposure. Protection of workers against exposures to radon in the uranium and thorium mining industries are regarded as being the responsibility of the operating management. According to the ICRP system, exposures in a planned exposure situation should be controlled by the optimisation process using dose constraints, as well as with application of dose limits. Ideally, a dose constraint should be determined at the design stage of an operation. The nature of radioactive ore-bearing deposits is highly variable, implying that a variety of mining methods and approaches are needed to extract the resource successfully. As a result, dose constraints as well as the result of the optimisation process will vary between mines, and, in some cases, will vary over time at the same installation as the physical conditions change. The principles used to control occupational exposures to radon and radon progeny in a uranium mine are similar to those used in other workplaces in planned exposure situations. This starts with careful design of the workplace, and use of appropriate engineering controls to limit and control radon exposures. In some cases, the potential for highly variable and/or high exposures to radon and its progeny is elevated in uranium mines because of the relative strength of the source term and other physical constraints (e.g. underground work). In these cases, additional attention needs to be paid to the details of the monitoring programme, to ensure that it assesses workplace conditions and worker doses adequately. Strategies such as real-time monitors and personal dosimeters should be considered in situations with high and variable radon concentrations. Conversely, in situations with low and stable concentrations of radon and its progeny, periodic workplace monitoring may be sufficient. In general, the active ventilation of workplaces means that the concentration of radon gas, together with approximations of equilibrium conditions, cannot be relied upon to assess exposures to radon progeny. As a consequence, measurements of radon progeny concentration (i.e. potential alpha energy concentration) should be used. Converting exposures to radon progeny into doses requires the use of dose conversion factors. In the past (ICRP, 1993), the dose conversion factors for radon progeny were based on epidemiological studies. The Commission is now proposing to calculate effective dose coefficients following exposure to radon progeny using ICRP reference biokinetic and dosimetric models with specified radiation and tissue weighting factors (ICRP, 2010). These dose coefficients will replace the dose conversion convention based on epidemiology.
4.7. Stakeholder interactions
The first step in securing support of a national radon strategy is the development of awareness, which appears to be very weak in many countries. Easily available information about radon, how it can be trapped inside enclosed spaces, related risks, and how to identify and mitigate high concentrations should be disseminated to the general population, notably through elected representatives, civil servants in administrative divisions, home owners, landlords, employers, children at school, etc. Training professionals (e.g. builders, architects, radiological protection professionals, employers, trade unions, workers) in radon issues will help to ensure that recommended preventive and mitigating measures are correctly designed, planned, and installed. Training programmes for professionals should be an integral part of the national radon action plan, so that householders or property owners subjected to radon concentrations above or close to the derived reference level can access a radon prevention and mitigation infrastructure. Appropriate information and training should also be provided to other concerned professionals (e.g. health, real estate). As the synergy between radon and smoking has been demonstrated in the assessment of the risk of lung cancer, a link between public health programmes for radon reduction and non-smoking policies is warranted, at least in terms of warning. National radon action plans should include provisions for information about the cost and the effectiveness of both preventive and mitigating actions. Data should be gathered regularly at different levels (i.e. local, regional, national), and made available to the various stakeholders.
5. Conclusions
The purpose of this report is to provide updated guidance on radiological protection against radon exposure, considering evolution of the system of radiological protection (ICRP, 2006b, 2007), updated knowledge about health risks due to radon exposure (UNSCEAR, 2009; WHO, 2009; ICRP, 2010), and experience gained by many countries and international organisations over recent years. In previous recommendations on the same subject (ICRP, 1993, 2007), the Commission recommended a strategy based on the distinction between protection approaches for dwellings and for workplaces. The Commission now recommends an integrated approach for protection against radon exposure in all buildings, whatever their purpose and the status of their occupants. The strategy of protection in buildings, implemented through a national action plan, is based on application of the optimisation principle below a derived reference level set in terms of the concentration in air. The Commission encourages national authorities to set a derived reference level that is as low as reasonably achievable in the range of 100–300 Bq m−3, taking the prevailing economic and societal circumstances into account. The aim of this new approach, graded according to the exposure situation, is to cover all buildings from a public health perspective (dwellings, mixed-use buildings, and general workplaces), at least in radon-prone areas. The Commission emphasises the role of preventive actions, mainly through building codes, in all types of buildings. This report provides guidance for the management of specific radon exposure situations in which workers are considered as occupationally exposed. It covers exposure situations when compliance with the reference level cannot be achieved, or they are included in a national list of activities or facilities established by the national authorities. The strategy of protection is then based on application of the optimisation principle and the relevant requirements for occupational exposure. The occupational dose limit should apply when the national authorities consider that the radon exposure situation should be managed as a planned exposure situation. By recommending a straightforward, integrated, and graded approach for most radon exposure situations, the Commission anticipates a reduction in exposure to radon, which is by far the main source of public exposure worldwide.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.