
Abstract
Comprehensive support for the everyday life of people in reconstruction areas around the Fukushima Daiichi nuclear power station should include access to specialists. This prompted the original development and recent user satisfaction survey of the ‘Mimamoru Health Application’ (MHApp), a digital tool connecting people to specialists and their expertise. To improve MHApp user satisfaction, user data from April 2021 to January 2023 were collected and analysed. Participants included affected populations (evacuees and returnees), unaffected residents, and local healthcare workers living in Fukushima Prefecture. Data included MHApp's system usability on a 0–100 scale [system usability scale (SUS)], user background characteristics, and free-text comments about using MHApp. In total, 47 participants joined this study. The number of days participants used MHApp was 17.3 ± 14.7 (mean ± SD). The SUS mean ± SD was 57.4 ± 13.2. Age-specific SUS scores were higher among users 20–40 years old than among users 50 + years old (p = 0.03). These results, along with free-text comments, suggest that improving the visualisation of various data and addressing the needs of users aged 50 years and older were key to better usability of MHApp.
INTRODUCTION
For the everyday life of people in reconstruction areas around the Fukushima Daiichi nuclear power station (FDNPS), radiation protection and health issues require specific support from specialists (Ito et al., 2023; Schneider et al., 2019). Recent publications have described the importance of supporting returnees during the recovery phase after a nuclear disaster (ICRP, 2020; Liutsko et al., 2023). To support not only returnees to former evacuation areas around the FDNPS but also those who remain evacuees, we have developed the ‘Mimamoru Health Application’ (MHApp) as a digital tool to facilitate effective communication between local healthcare workers and these affected populations (Ohba et al., 2020). ‘Mimamoru’ means ‘support from a distance’ in Japanese. This digital tool includes functions to record radiation exposure (external and internal exposures) and health status (BMI, blood pressure, body temperature, daily physical activity, sleep, and diary notes), as shown in Fig. 1 (Nakano et al., 2022; Ohba et al., 2021a). These items were decided based on a previous survey of needs (Ohba et al., 2021b).
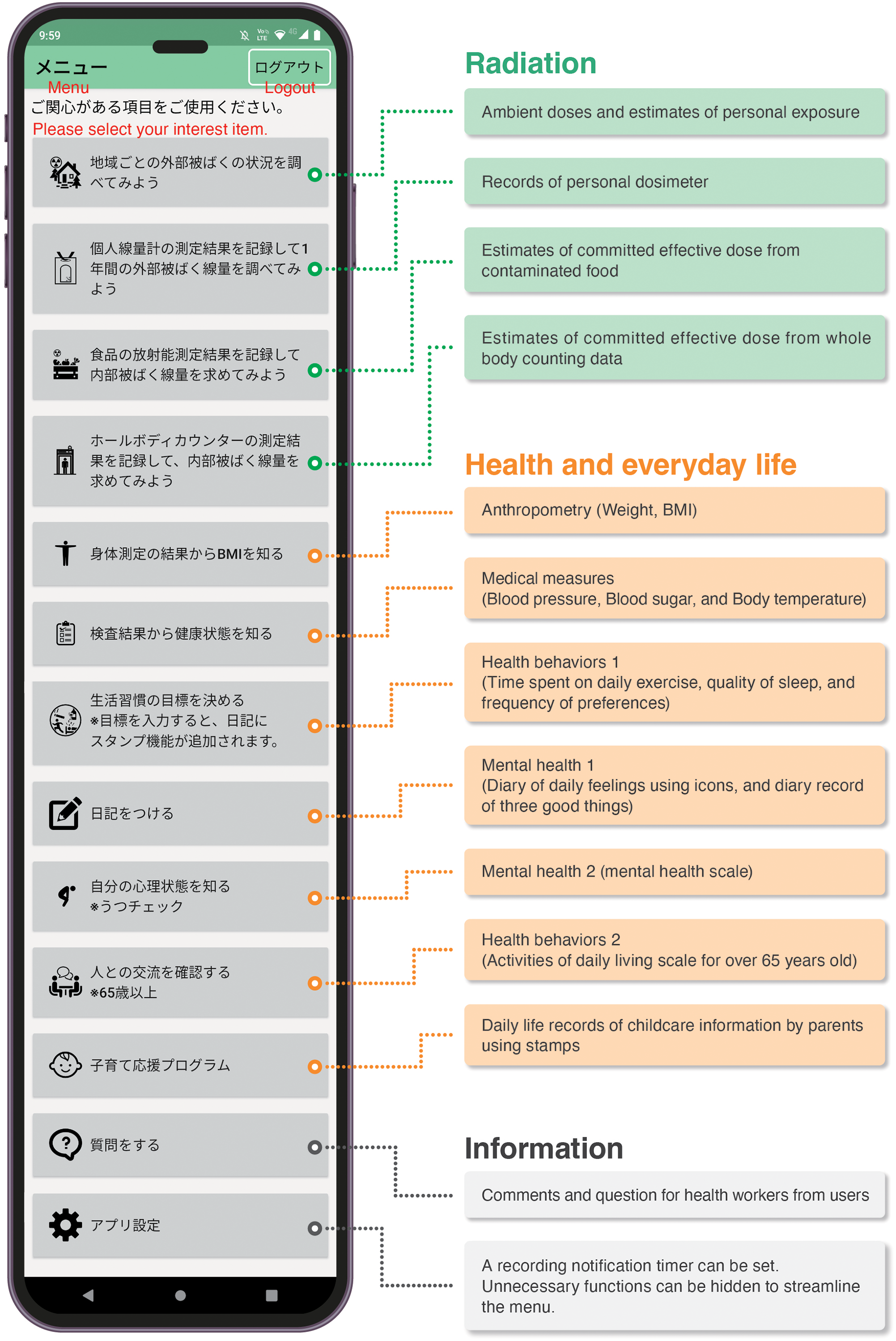
The mobile phone screen of MHApp's function list and description of the functions.
Digital tools such as MHApp need to be properly evaluated for usability. We chose the system usability scale (SUS, scale range 0–100) to assess MHApp (Kortum and Bangor, 2013), aiming to make it as user-friendly as possible. This study analysed usability survey data to guide potential improvements, with the ultimate aim of better connecting local healthcare workers to affected populations through MHApp.
This article covers data collected between April 2021 and January 2023. Participants included affected populations (evacuees and returnees) living in municipalities around FDNPS, unaffected residents, and local healthcare workers living in Fukushima Prefecture. We asked about MHApp's usability and collected user background characteristics such as residential area, gender, age, living conditions, and education level. Among the three geographic areas of Fukushima Prefecture, we anticipated more interest in radiation exposure in coastal Hamadori, where FDNPS is located, than in central Nakadori or inland Aizu. The prior work of Kortum and Bangor allowed us to compare MHApp on a system usability scale (SUS, range 0–100) with PC software, internet browsers, web-based services, and familiar electronic devices used in everyday life. Their SUS survey was conducted between 2010 and 2011 on 1058 participants in the USA, including university undergraduate students (499 participants, aged 18–22 years) and adults (559 online participants, aged 18–72 years). The gender ratio in this survey was 42% male and 58% female (Kortum and Bangor, 2013).
We also calculated the frequency with which participants used each function of MHApp. As the number of days that each participant used MHApp varied, we calculated usage data per month for comparisons. Participants also provided their opinions about MHApp, including positive aspects and points for improvement, in the free-text description section of the questionnaire. Herein, we report representative items written by several participants, selected and translated by the first author (T.O.).
The t-test was applied to the data, using JMP14.3 software (JMP Statistical Discovery LLC, Cary, NC, USA), with statistical significance set at 5%. This study was approved by the Ethics Committee of Fukushima Medical University (approval #2022–069), which is guided by local policy, national law, and the World Medical Association Declaration of Helsinki.
RESULTS
In total, 47 participants joined this study. The simple duration of each participant's MHApp use was recorded in days, which averaged 17.3 ± 14.7 (mean ± SD). During this time, the frequency of function-specific usage was highest for the functions recording daily physical activity and sleep.
The SUS mean ± SD was 57.4 ± 13.2, close to that of Microsoft EXCEL® (SUS 56.5 ± 18.6), as shown in Fig. 2. The SUS scores were not significantly different between MHApp and Microsoft EXCEL® by t-test.
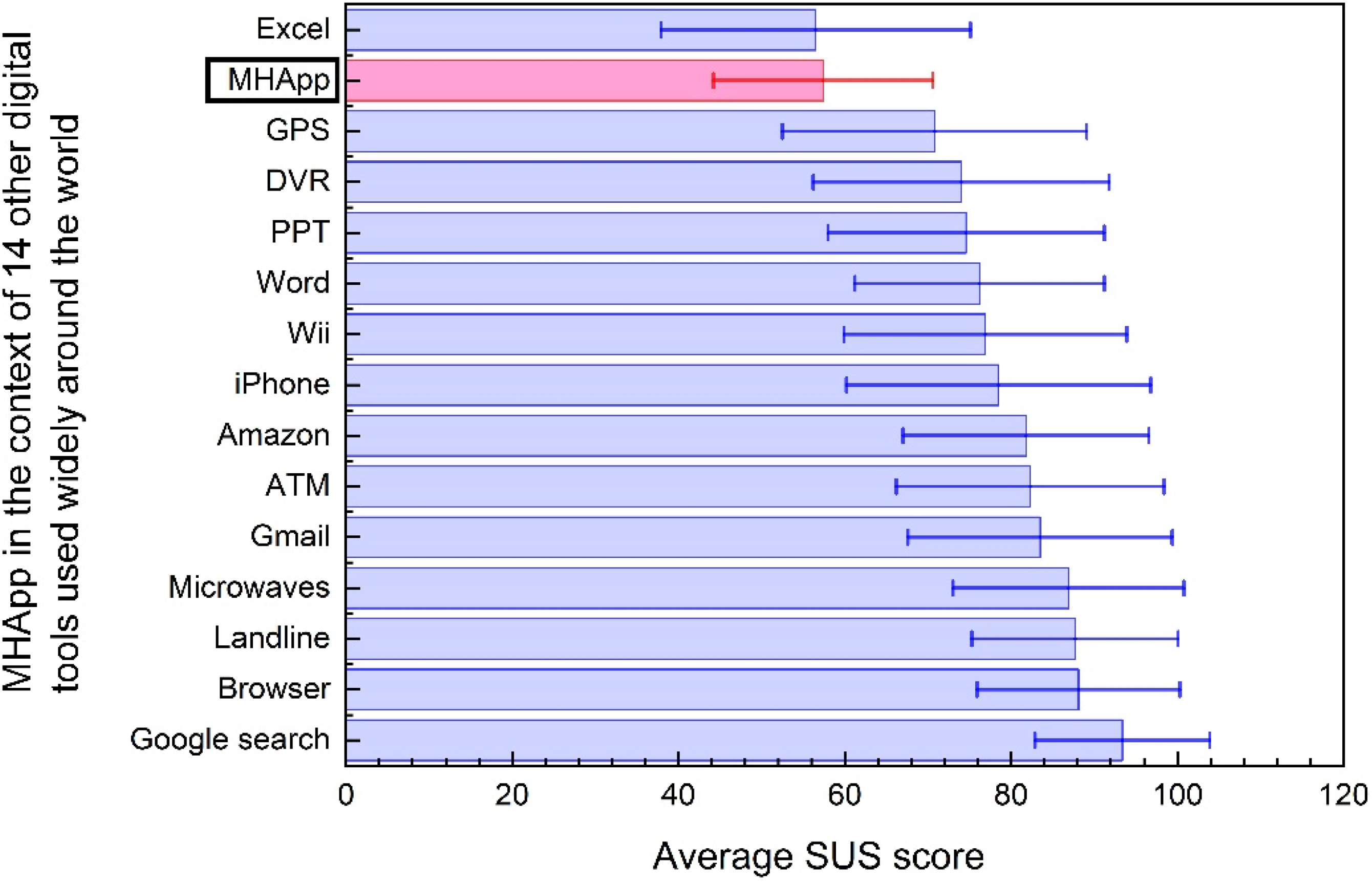
A comparison of MHApp with 14 other digital tools known around the world. The SUS scores (mean ± SD) shown for these digital tools are as previously reported (Kortum and Bangor, 2013). SUS, system usability scale; GPS, global positioning system; DVR, digital video recorder; PPT, PowerPoint®; ATM, automated teller machine; MHApp, Mimamoru Health Application; Wii®, a Nintendo television game system; iPhone®, an Apple mobile phone.
As shown in Table 1, SUS scores did not differ significantly by the place of residence. Age-specific SUS scores were higher among users 20–40 years old than among users 50+ years old (t-test, p = 0.03, Table 1). We implemented a modification in 2021 to fix errors and operational bugs in MHApp, but did not change the visual interface at that time. Therefore, the SUS scores of MHApp did not show significant differences before and after this modification. In addition, there was no significant relationship between the frequencies of MHApp function-specific usage and SUS score.
Comparisons of SUS scores and background characteristics of 47 participants.
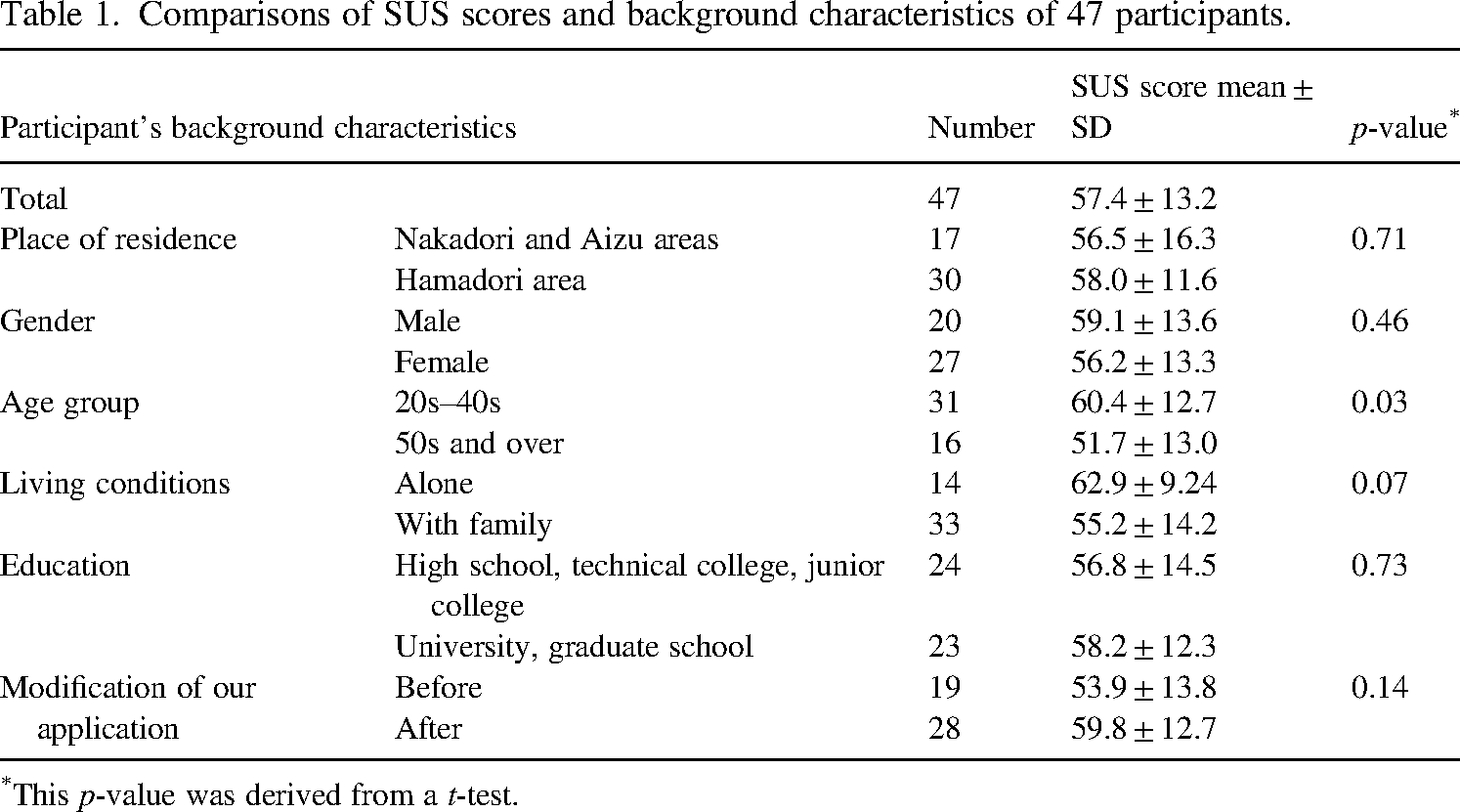
This p-value was derived from a t-test.
Among free-text descriptive comments, ‘Use of the diary helped me to know how happy I am every day’ was noteworthy. Comments such as ‘Medical measures and exercise records were good indicators of well-being’ and ‘It is good to be able to check radiation exposure doses’ were favourable points. A suggestion for improving the tool was, ‘I would like to see a visualisation of the radiation exposure levels’. Other improvements were suggested: (1) ‘It was time-consuming to enter IDs and passwords for the MHApp’. (2) ‘After I forgot to enter records, it felt like a hassle to enter them at a later date – better to have an input notification function’. (3) ‘I would like a system where I could receive information related to my daily life, such as notices from the municipality’.
This study will continue to collect data through March 2024 (the end of Japan's fiscal and academic year). Our preliminary analysis suggests that improving the visualisation of various data and addressing the needs of users aged 50 years and older were key to better usability of MHApp (especially, for health behaviours and mental health). These points are detailed as follows.
First, improved usability will come from a more visually oriented interface. As shown by the SUS scores in Fig. 2, MHApp usability was similar to that of Microsoft EXCEL®, at the low end among rankings for general-purpose software and digital tools of everyday life. This could be due to visual difficulties in the MHApp interface. In particular, Fig. 1 shows the need for substantial scrolling to access all MHApp functions, which complicates how users reach the functions they want to use. Other improvements suggested in free-text comments include simplifying data entry and adding individualised information notification functions. Technically, easy solutions exist, but the security of personal information must be maintained (Liutsko et al., 2023). In short, we showed a need for balancing interface improvements and data security.
Second, the study suggested that methods to support active usage of MHApp should be prepared, especially for people aged 50 years and older. Indeed, our past research found that local healthcare workers questioned the adaptation of digital tools to older age groups (Nakano et al., 2021) and that support is needed for people with low eHealth literacy to use digital information tools (Yumiya et al., 2021). As seen from the free-text comments, MHApp not only checks radiation exposure doses, but also, using it contributes to healthy behaviours and mental health. It is therefore important that MHApp provides stress-free ways to record and reflect on health behaviours and mental health for people 50 years and older.
In conclusion, we are keen to strengthen support for radiation protection and health promotion in the recovery areas affected by the FDNPS accident, with digital tools such as MHApp that can be adopted and adapted around the world.
Footnotes
ACKNOWLEDGEMENTS
We heartily thank not only participants but also Dr. Hiroshi Yasuda (Hiroshima University) and Dr. Makiko Orita (Nagasaki University) for their support. This work was supported by a Ministry of the Environment grant, Research Project on the Health Effects of Radiation (JFY 2019-2021). This work was also supported by the Network-Type Joint Usage/Research Centre for Radiation Disaster Medical Science, Japan (JFY 2018–2023). The authors declare no conflicts of interest.