
Abstract
Improvements in conforming radiation fields to tumours in radiotherapy have increased the potential for successful treatment of cancer. However, achieving successful delivery requires the patient to be positioned on the treatment couch accurately. X-ray imaging using on-board imaging systems incorporated into linacs is performed to verify patient positioning, frequently at every treatment fraction. The x-ray imaging exposes normal tissues surrounding the tumour and carries a risk of inducing second cancers. The reductions in high-dose treatment margins achieved with image-guided radiation therapy (IGRT) must be balanced against harm from additional imaging doses. ICRP Task Group 116 has been set up to prepare guidance on radiological protection aspects of IGRT. The task group has undertaken a survey of imaging practices in radiotherapy in nine countries across the world. This has shown that kilovoltage (kV) cone beam computed tomography (CT) is used widely, and the level of use increases with the Human Development Index for the country. The survey has shown that there is limited awareness of the doses from imaging in radiotherapy centres, a lack of expertise in diagnostic imaging, and limited recording of patient doses. This has informed the task group in the development of guidance.
Keywords
BACKGROUND
The use of image-guided radiation therapy (IGRT) has increased in recent decades to take advantage of improvements in shaping radiation fields from linear accelerators (linacs) to tumour target volumes (Mundt and Roeske, 2011). This has been brought about by a number of technological developments including the introduction of multi-leaf collimators, consisting of motorised high-density tungsten alloy leaves to conform the irradiation field to the shape of the tumour target, and improved flexibility in the delivery of radiation from different directions and angles. As a result, linacs operating under the control of a computer are able to conform radiation fields more effectively to tumour targets while sparing normal tissue surrounding the target volume, enhancing the potential effectiveness of treatments and improving clinical outcomes (De Neve et al., 2012). In order to take advantage of these improvements in treatment delivery, the patient needs to be positioned with mm accuracy, and imaging is essential to ensure success. Imaging is used both for producing the initial plan and verifying that the patient is in the correct position on the treatment couch so that the planned dose distributions will be delivered precisely to the intended tissues. Since radiation therapy treatments are generally delivered in fractions, imaging may be required at each fraction to verify patient position. However, imaging with ionising radiations will give an additional dose to normal tissues, adjacent to the tumour, and thus carry a risk of inducing second cancers, as well as increasing doses to organs at risk lying within the region of the treatment.
ICRP set up Task Group 116 (TG116) to review the radiological protection aspects of imaging in radiation therapy and prepare guidance on IGRT in 2020. Although there was information in the literature on the use of IGRT in Europe, North America, and other Western countries, there were many parts of the world for which little data were available. The ICRP mentorship programme had just been set up, and applicants for TG116 came from a broad range of countries, so the task group used the opportunity to set up a survey that could collect information on imaging practices in radiotherapy for the mentees’ countries.
METHODS
Applications were received from candidates in nine countries, two from each of Europe, America (North and South), Asia, and Africa and one from Australia. A questionnaire on radiotherapy and imaging practices was designed, including 130 items of data. Mentees were asked to contact a selection of radiotherapy centres in their country and were provided with a link that they could send to the representative at each centre, through which the representative could register to take part in the survey. The questionnaire was completed online using SurveyMonkey®, and a close liaison between mentees and radiotherapy centres allowed clarification of issues in the interpretation of data. Data were collected for 3½ months starting in late summer 2020, and a total of 97 completed questionnaires across the nine countries were included in the final data analysis. The number of centres in the survey from higher-income countries only represented a few percent of the total in the country, but over 20% of radiotherapy centres took part in five middle- and lower-income countries. The Human Development Index (HDI) as defined by the United Nations Development Programme was used in making comparisons between countries to bring out differences relating to the level of development (UN, 2023). The HDI combines measures of the index of life expectancy, education, and per capita income. Values move towards 1.0 as the level of development rises with countries surveyed having values between 0.7 and 0.95.
RESULTS
Practices in the use of image guidance in radiotherapy
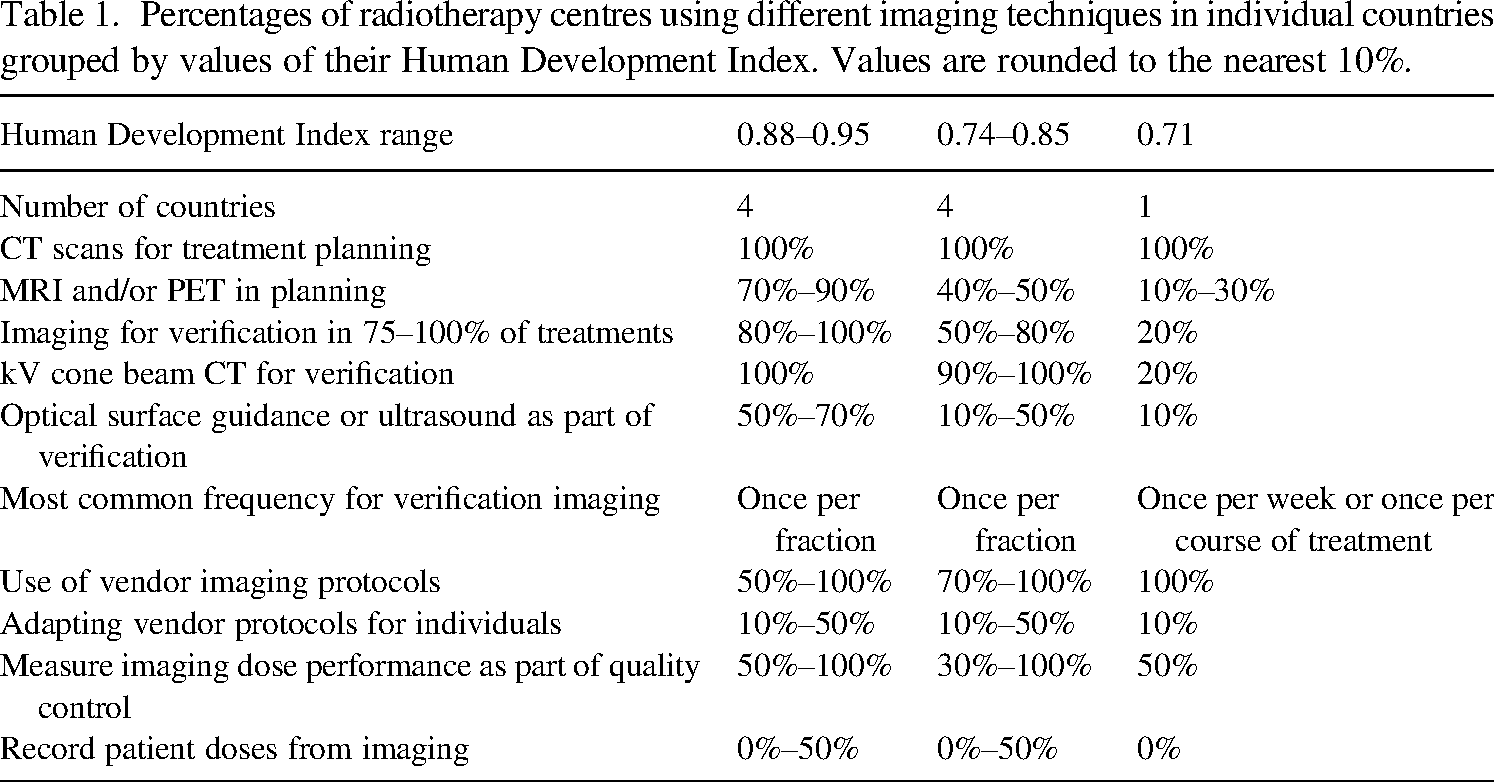
A full report on the findings of the survey has been published in Martin et al. (2021), and this article reports the main findings that are summarised in Table 1 and considers the implications for developing guidance by the task group. Centres in all the countries surveyed used computed tomography (CT) for treatment planning with the use of magnetic resonance imaging (MRI) or positron emission tomography (PET) in the planning process in countries with higher HDI values. Imaging carried out immediately prior to each treatment for verification of patient position was used for 75%–100% of treatments in most countries with higher HDI values, but the proportion declined with HDI (Table 1). Verification imaging requires fields covering the area surrounding the tumour to encompass bony or fiducial markers to confirm alignment, so more normal tissues are irradiated than by the treatment beams. Most centres used kilovoltage (kV) imaging systems incorporated into the linear accelerator. These comprise an x-ray tube and image detector plate that can record either planar kV images or can rotate around the patient to produce cone beam CT (CBCT) images, in a similar form to the CT planning images. Most centres had at least one linac with kV imaging, apart from in the country with the lowest HDI, which only had kV imaging facilities attached to 2 out of 17 linacs. Other centres in the country relied on the use of MV therapy sources with electronic portal imaging devices for verification, but the contrast obtained from MV imaging is poor, and doses are higher, so they are less satisfactory for imaging. Some non-ionising imaging devices, namely, optical surface guidance or ultrasound, were used for patient position verification, primarily in countries with higher HDIs (Table 1), and there were MRI systems incorporated into linacs in 10%–25% of centres in some countries. In the countries with higher HDI values, half of the centres imaged at every fraction, while others used alternative options such as the first three fractions followed by weekly imaging. The frequencies varied with the treatment site to some extent and would be carried out according to set protocols, but they tended to follow similar patterns for most types of treatment within each country. Generally, the proportion of centres using imaging at every fraction declined with the HDI of the country, and the frequency may be chosen to match the standard of care and resources available. Centres in the country with an HDI of 0.71 that did not have kV CBCT only imaged either once per week or once during the course of treatment for most types of tumour. When centres acquired kV CBCT systems, the frequency of imaging generally increased.
Percentages of radiotherapy centres using different imaging techniques in individual countries grouped by values of their Human Development Index. Values are rounded to the nearest 10%.
Percentages of radiotherapy centres using different imaging techniques in individual countries grouped by values of their Human Development Index. Values are rounded to the nearest 10%.
Imaging undertaken for verification is carried out using protocols with standard settings. These are generally provided by the equipment vendor, and since the primary aim is simply to ensure the image quality is sufficient for verification of patient position, efforts put into optimisation of radiological protection may be limited. Radiotherapy centres in all parts of the world used vendor protocols, and those undertaking optimisation were in the minority, even in countries with higher HDI values (Table 1). When considering optimisation of radiological protection, a knowledge of dose levels is needed to provide an assessment of potential harm from the exposure and enable any dose reductions achieved through optimisation to be evaluated. However, although 50% of the radiotherapy centres in European countries recorded patient doses, only 10% or less did in most other parts of the world. Moreover, this was independent of the country’s HDI. In addition, only 50%–60% of the centres in the two countries in the 0.88–0.95 HDI bracket outside Europe carried out measurements of dose performance for the imaging equipment.
DISCUSSION AND IMPLICATIONS FOR THE TASK GROUP
The survey of imaging in radiotherapy showed that centres throughout the world are using image guidance. Most centres in high-income countries have kV imaging systems attached to their linacs, and cone beam CT is the predominant mode in which it is used. Imaging protocols supplied by the vendor are used in most centres with limited adjustment for optimisation. Most centres use imaging at every fraction, and the cumulative dose from repeated exposures over a whole treatment course may give a significant dose to normal tissues surrounding the tumour target. Results suggest that more guidance on the frequency of imaging and optimisation techniques is required, particularly for paediatric exposures. The same vendor protocols are usually used at each fraction throughout the treatment of a patient, and further adaptation of exposure factors to optimise radiological protection may be possible as exposures are repeated.
The survey highlighted that the awareness of doses from imaging, particularly the kV CBCT used by most centres, was limited. In the past doses from imaging have been regarded as insignificant in comparison with therapy doses, but with the increased frequency and the fact that they use larger fields and so irradiate more normal tissues, there is now a need to consider optimisation. Most medical physicists who work in radiotherapy do not have expertise in diagnostic imaging, which uses different dose quantities because of different dose distributions with tissue depth. Therefore, radiotherapy physicists need to be trained in diagnostic imaging or diagnostic medical physicists involved in assessments.
The dose quantity displayed by many CBCT systems is the CT dose index (CTDI), which is a quantity designed for measurement of narrow beam CT scanners. Although this can be evaluated for CBCT systems, it requires the use of the scanner with a CT phantom in a manner for which the scanner was not designed and in which it will not generally be used. Therefore, a more appropriate measurement technique that can readily be applied in radiotherapy clinics is required. Various methods have been proposed, such as adaptation of the CTDI technique (IEC, 2009) and measurement of cumulative dose from CBCT systems with a large phantom (AAPM, 2014), but neither technique is straightforward, and both require equipment that is not readily available in radiotherapy departments. Therefore, if proper assessments of patient dose are to be carried out, an alternative measurement technique needs to be developed using equipment that is readily available in radiotherapy centres and an alternative quantity used that can both be displayed on CBCT equipment and for which the calibration can be readily confirmed. The dose quantities mentioned earlier aimed to give a dose that had meaning in the general context of dosimetry, but for evaluating patient doses, a dose quantity is required that can be readily measured with tools available in a radiotherapy department (Abuhaimed et al., 2015). Such a quantity based on a similar method with standard equipment could be used for comparisons of dose between centres.
The next stage in achieving optimisation will be to carry out surveys using the dose quantity developed to evaluate doses for individual patients (ICRP, 2023). Information on patient doses from imaging in radiotherapy centres around the world is limited, and this needs to be expanded to start the process of optimisation. Methods for checking the dose performance of imaging equipment and recording of patient doses from imaging need to be introduced to raise awareness among radiotherapy staff. Once comparisons can be made between centres, then surveys can be carried out to identify centres where doses are higher, and optimisation is required, which is the approach that has been taken in diagnostic radiology.
CONCLUSIONS
A survey of imaging practice in radiotherapy centres from nine countries around the world has been carried out using the ICRP mentorship scheme. This has enabled countries from which it is often more difficult to obtain data to be included. Most middle- and high-income countries now use image guidance in radiotherapy and have kV cone beam CT systems installed on linacs. However, the country with the lowest HDI in the survey had very limited kV imaging facilities on their treatment machines. Thus, image guidance is now universal at the present time and is at the stage where it is likely to be taken on increasingly by other countries as they purchase new systems with kV imaging facilities in the coming years.
Apart from the need for general guidance relating to the application and frequency of imaging for different applications, the survey highlighted that little attention has been paid to doses from imaging in radiotherapy. For optimisation of radiological protection to be taken forward, medical physicists with imaging experience are needed in radiotherapy departments, or the involvement of diagnostic radiology physicists in the optimisation. However, the limited recording of doses may be partly due to the lack of a suitable agreed dose quantity that can be measured with the instruments and phantoms available within radiotherapy departments. The task group is therefore investigating dosimetry options utilising the physicists within different countries built up through the ICRP mentee programme.
Footnotes
ACKNOWLEDGEMENTS
The author acknowledges the work of members of ICRP Task Group 116, Tim Wood, Tomas Kron, Ung Ngie Min, Jenia Vassileva, Sebastien Gros, and William Small, who assisted in the organisation of the survey, and Mentees from TG116, Abdel-Hai Benali, Abdullah Abuhaimed, Hossam Ragab Shaaban, María Cristina Plazas d’Leon, Mario Djukelic, Sebastien Gros, and Yiannis Roussakis, who collected the data.