
Abstract
Team reflexivity, the extent to which teams collectively reflect upon and adapt their working methods and functioning, has been shown to be an important predictor of team outcomes, notably innovation. As described in the current article, the authors developed and tested a team-level contingency model of team reflexivity, work demands, and innovation. They argue that highly reflexive teams will be more innovative than teams low in reflexivity when facing a demanding work environment. A field study of 98 primary health care teams in the United Kingdom corroborated their predictions: Team reflexivity was positively related to team innovation, and team reflexivity and work demands interacted such that high levels of both predicted higher levels of team innovation. Furthermore, an interaction between team reflexivity, quality of physical work environment (PWE), and team innovation showed that poor PWE coupled with high team reflexivity was associated with higher levels of team innovation. These results are discussed in the context of the need for team reflexivity and team innovation among teams at work facing high levels of work demands.
There is general agreement that, in demanding environments and in challenging times, teams and organizations have to be innovative in order to maintain or enhance effectiveness (De Dreu, 2002; West & Anderson, 1996). A small but growing body of research suggests that team reflexivity—that is, conscious reflection on team functioning—may be an important process in enhancing team innovation, the development and implementation of more effective processes or procedures (for a review, see Widmer, Schippers, & West, 2009). However, a recent review by Moreland and McMinn (2010) indicated that the relationship between reflexivity and performance indicators is often mixed, and they concluded that reflexivity can have positive consequences but often only under specific conditions. Some research has suggested contingencies of the reflexivity–performance relationship, indicating under what conditions team reflexivity may be especially helpful. For instance, a longitudinal study among 73 student teams showed that low-performing teams benefited more from reflexivity in terms of both learning and improved final performance than did initially high-performing teams (Schippers, Homan, & van Knippenberg, in press). This study indicated that reflexivity may be particularly valuable when things are not going well for the team. Indeed, in challenging times there is a need for organizations and teams to respond with innovation rather than passivity (Boone, Van Olffen, Van Witteloostuijn, & De Brabander, 2004).
Discovering what combinations of factors prompt team innovation is hugely important for teams and organizations. Reflexivity may be one such key factor because it promotes awareness of the objectives, strategies, processes, and environments of teams. This awareness may lead to the identification of discrepancies between current and ideal factors in the team’s domain (cf. Kahneman, 1973; Locke & Latham, 1990; Schippers, Den Hartog, Koopman, & van Knippenberg, 2008; Schippers et al., in press), prompting arousal and action such as innovation to reduce the discrepancies (e.g., Cyert & March, 1963; Locke, Cartledge, & Knerr, 1970; Locke & Latham, 2002). Here, we identify two of the most salient factors influencing a team’s functioning: work demands and the physical work environment (PWE). High levels of work demands, we propose, will focus the awareness created by reflexivity upon a specific, important aspect of the team environment. Reflexivity with a specific focus on high work demands will present teams with clarity, agreement, and a specific challenge about the need for innovation, making it more likely that targeted innovation will result. Similarly, working in a low-quality PWE encourages a specific focus on the external environment as a domain for reflexivity and therefore innovation. Under such conditions, teams have the potential to benefit significantly from their reflexive processes. In relatively benign and nonchallenging team environments, reflexivity may not play a role in prompting team innovation (cf. Schippers et al., in press; Sitkin, 1992). In short, reflexivity will likely be focused rather than diffuse when there is a clear environmental constraint or demand.
Specifically, we propose that to understand team-level innovation we need to explore whether the team context (e.g., the demands of the team environment) moderates the relationship between team processes (such as team reflexivity) on the one hand and team innovation on the other hand. Our study explores how teams can effectively influence their work environment, responding to Bamberger’s (2008) call to study the role of context (see also Shalley, Zhou, & Oldham, 2004). Our study also extends work demands research by examining demands at the team level. More generally, our study adds to the emerging knowledge about team-level factors that influence creativity and innovation in the workplace.
In the following section, we outline the theory and review research on work demands, team reflexivity, and innovation. We subsequently argue why work demands and team reflexivity would be expected to interact to predict innovation.
Literature Review and Hypotheses
Innovation
Following prior research, we define innovation as “the intentional introduction and application within a job, work team or organization of ideas, processes, products or procedures which are new to that job, work team or organization and which are designed to benefit the job, the work team or the organization” (West & Farr, 1990: 9). Innovation subsumes creativity—the generation of new ideas—but, in addition, includes the implementation of the ideas (West, 2002; West, Hirst, Richter, & Shipton, 2004) and is seen as an important factor in organizational effectiveness and survival (Agrell & Gustafson, 1996; Anderson, De Dreu, & Nijstad, 2004; Hirst, van Knippenberg, & Zhou, 2009; West et al., 2004). We augment this definition by suggesting that innovations also should be judged on the basis of whether they prove effective in practice.
Team-level innovation at work is often engendered by problems and challenges that arise in the pursuit of work goals, and as such we focus on team innovation as an outcome resulting from teams developing and implementing novel and useful solutions to challenges and problems encountered in the workplace (Drucker, 1985; Hirst et al., 2009). Innovative behavior consists of three behavioral tasks: idea generation, idea promotion, and idea realization (Scott & Bruce, 1994); the latter usually requires teams to implement the ideas for innovation that they have developed (West, 2002). A recent review of team-level innovation by Hülsheger, Anderson, and Salgado (2009) points to inconsistent findings that characterize the field and argues for contingency models. Furthermore, their review identifies two key flaws in past research that we aim to address in the current study: (a) Researchers have relied on self-ratings when measuring team innovation, leading to an overestimation of effect sizes, and (b) there are many contradictory findings, suggesting unknown moderating effects in addition to simple direct effects (Hülsheger et al., 2009).
Team Reflexivity and Innovation
Team reflexivity is defined as the extent to which group members overtly reflect upon and communicate about the group’s objectives, strategies (e.g., decision making), and processes and make changes accordingly (West, 2000). In the taxonomy of team processes proposed by Marks, Mathieu, and Zaccaro (2001), reflexivity can be seen as a transition process referring to actions that teams execute between performance episodes. These have a dual focus, namely, reflecting on and interpreting accomplishments so far and preparing for future action (LePine, Piccolo, Jackson, Mathieu, & Saul, 2008).
By reflecting on work processes, teams may innovate because this reflection spurs further reflection on ways in which they can work more effectively. Indeed, research into idea generation in groups has shown that this process is much more efficient if teams (a) carefully process the ideas exchanged in the group (i.e., attention) and (b) take the opportunity to reflect on ideas produced during the exchange (i.e., incubation; Paulus & Yang, 2000). The study by Paulus and Yang (2000) suggests that, under the right conditions, the idea exchange process in groups may be an important means for enhancing creativity and innovation in organizations. These conditions—attention and incubation—are at the heart of team reflexivity.
Teams that engage in such deep processing (i.e., that are highly reflexive) will also develop more innovations (ideas for new and improved ways of doing things or new products and services) than nonreflexive teams do (De Dreu, Nijstad, & van Knippenberg, 2008; Hülsheger et al., 2009; Wong, Tjosvold, & Su, 2007). Reflexive teams will also reflect critically on ideas, drop those that are less promising, and choose to implement the better bets (cf. De Dreu, 2002). Prior research has indeed established a direct link between team reflexivity and innovation (Carter & West, 1998; Tjosvold, Tang, & West, 2004). In their research among 100 work teams in China, Tjosvold et al. (2004) found that teams that reflected on their tasks were more innovative, and a study among BBC TV production teams showed a positive relation between team reflexivity and external management ratings of creativity (Carter & West, 1998). Thus we hypothesize:
Hypothesis 1: Team reflexivity is positively related to team innovation.
Team Reflexivity and Work Demands
Work demands, such as having to work fast and hard and cope with a high qualitative workload, can be seen as psychological stressors (LePine, Podsakoff, & LePine, 2005). How individuals and teams respond to such psychological stressors is important for their well-being and their effectiveness (Perrewé & Zellars, 1999). At the individual level of analysis there is evidence to suggest that innovation as a response to stressors is an effective and often-used stress coping strategy (Bunce & West, 1994). We propose that the same is likely to be true at the team level but that reflexivity is especially likely to lead to high levels of innovation when stressors, in the form of work demands, confront team members. In such situations, reflexivity gives the team the self-awareness necessary for recognition of work demands and an appreciation of the team’s capacity to respond to these demands by introducing new and improved ways of working.
We propose that the extent to which team reflexivity enables or stimulates innovation may be contingent upon the objective team-level workload. Thus, both team reflexivity and team innovation may be needed and helpful, particularly when the level of team demands is high (West, 2002). The process of identifying demands and their consequences raises the awareness of team members about the gap between their ideal and current circumstances. Thus, a health care team may identify a high workload (many patients) as a demand that affects the team’s ability to provide high-quality patient care. Awareness of a gap between the current and desired situation is likely to lead to arousal and discussions about how the gap can be closed (cf. Kahneman, 1973; Locke & Latham, 1990; West, 2002), in this case the need to deal with a high quantity of patients while aiming to provide high-quality care.
High workload levels can produce diverse responses, one of which is innovation—developing new and improved ways of doing things. We do not theorize here about the range of possible responses, which can be very wide (e.g., working harder or faster, reappraising the environment, seeking help, faking good performance). Rather, our focus is on teams innovating in order to cope with work demands (cf. Janssen, 2000; West, 1989).
We propose that a critical factor determining whether an innovative response is elicited is the extent to which the team is aware of the pressures or difficulties it faces; team reflexivity is the theoretical concept that most usefully articulates this awareness. Awareness of the need for team innovation seems crucial. By reflecting on their work context and by discussing how their working methods can be improved to ensure an effective response to that context, teams will develop a deeper understanding of the problem at hand and will be better able to fashion effective ways of dealing with demands (cf. De Dreu et al., 2008). We propose that team reflection produces a general innovation orientation in the face of demands, rather than a work-faster or hide reaction. Reflection provides the shared cognitive space within which action possibilities can be considered by team members. Such shared cognitive space, in the context of preparedness for action spurred by demands (necessity to act), creates the opportunity for innovation (Bunce & West, 1994; Janssen, 2000; West, 1989). In other words, work demands and team reflexivity will interact to predict team innovation, such that high levels of both will be associated with high levels of team innovation.
In the context of the study we describe below, when health care teams have many cases to handle, resulting in a high workload (i.e., patient-to-doctor ratio), team innovation might well be needed to develop new and improved ways of working to provide high-quality patient care in the context of a high workload. Thus, we expect an interaction between reflexivity and the patient-to-doctor ratio, such that when team reflexivity is high, combined with a high patient-to-doctor ratio, then team innovation will be higher.
Hypothesis 2: The relationship between team reflexivity and team innovation will be moderated by team-level workload, such that teams with a high workload and a high level of team reflexivity will innovate more.
Physical Work Environment
Another salient demand health care teams face on a daily basis is the PWE they occupy, since this affects their performance by enabling or inhibiting their ability to provide health care to their patients. Factors in the PWE include spaciousness, quality of the working area, facilities, and general condition of the building. Traditionally, this is the domain of environmental psychology, which considers the relationships between people and their physical environment (for a review, see Sundstrom, Bell, Busby, & Asmus, 1996). The majority of studies are devoted to the link between the PWE and job satisfaction and performance (e.g., Lee & Brand, 2005; Peters & O’Connor, 1980). Several studies have also examined the effect of the working environment on workers’ moods (Brief & Weiss, 2002) and behaviors (Wickhorst & Geroy, 2006). The PWE can create demands and stressors, for example, as a result of working in a confined space or with old equipment or in an impoverished work environment in general (Elsbach & Pratt, 2007; Peters & O’Connor, 1980; Sevdalis, Arora, Undre, & Vincent, 2009; Sundstrom et al., 1996; Sutherland & Cooper, 1988; Villanova & Roman, 1993).
As with workload, several reactions to a challenging PWE are possible. Employees may complain about the quality of the work environment, adapt to the impoverished environment by accepting the limitations, or reflect and respond innovatively to their difficult circumstances and try to make the best of them (cf. Elsbach & Pratt, 2007; Vashdi, Bamberger, Erez, & Weiss-Meilik, 2007). However, if teams reflect on the physical environment and make changes, this may help the teams perform more effectively. Research among surgical teams has shown that a reflexivity intervention helped teams question taken-for-granted assumptions, such as the suitability of the room layout for an operation. Consequently, those teams made adjustments to the physical layout of the operating room in order to avoid communication problems with the head surgeon due to a blocked line of sight (Vashdi et al., 2007). Similarly, members of a highly reflexive health care team may respond to the fact that they have a small waiting area with a limited number of seats for patients by developing a smart and effective appointment system that minimizes the number of people waiting to see a doctor or nurse. Alternatively, they may encourage a greater use of clinics for small groups of patients with common ailments so that they are seen together outside of normal surgery hours.
We thus expect an interaction between reflexivity and quality of PWE on team innovation, such that under conditions of high team reflexivity, combined with low-quality PWE, team innovation will be higher. In contrast, when the quality of the PWE is high, the level of reflexivity will be unrelated to the level of innovation.
Hypothesis 3: The relationship between team reflexivity and team innovation will be moderated by quality of PWE, such that high team reflexivity is more strongly related to team innovation when the quality of the PWE is low rather than high.
Method
Data and Sample
Data were collected from 1,156 members of 98 primary health care teams (PHCTs) across 19 health authorities in the English National Health Service. The health authorities chosen were located across a range of geographical areas of England to ensure a representative sample of PHCTs. These teams, known as general practices, consist of health care professionals providing primary services to patients in the community, led by one or more general practitioners (GPs, or family doctors), and typically include a practice manager, nurses, health visitors, administrators, and sometimes other professionals such as psychologists, physiotherapists, and midwives. The mean team size was 21.4 (SD = 11.1).
We chose a sample with high variance on job demands, since in general many work demand studies failed to find the hypothesized relationships as a result of sampling within the same profession or organization, resulting in limited variance in work demands (Oldham & Hackman, 2005). We therefore concluded that it was important either to sample from different organizations or to choose work demands that all the teams have to deal with, while providing sufficient variance between the teams to be able to observe the expected relationships (Oldham & Hackman, 2005). The health care teams in the current study are high on autonomy, since they make decisions about most changes themselves, and have similar types of demands. Besides, autonomy is an important antecedent to creative or innovative performance (Amabile, 1983, 1996).
Procedure
The study was part of a larger data-gathering effort providing three large samples of health care teams throughout the United Kingdom, and the data collection procedure was similar to that described by Fay, Borrill, Amir, Haward, and West (2006); Stewart (2006); and West et al. (2003). In each team, the practice manager or another senior administrator completed a short questionnaire identifying the names and occupations of team members as well as information such as frequency of meetings and information about the local population. When these were returned, questionnaires were mailed to each team member, with a reply-paid envelope so that the questionnaires could be returned to the research team directly. In total, 2,096 questionnaires were sent out, so the 1,156 returned represents a 55% response rate.
Response rates within teams varied from 21% to 100%, with a mean of 58%. Of the respondents, 85% were female; 15% were doctors (ranging from 0% to 50% within teams); 14% practice-employed nurses (0% to 60%); 23% trust-employed nurses (health visitors, district nurses, midwives; 0% to 67%); 34% administrative staff (0% to 86%); 7% managers (0% to 33%); and 4% professions allied to medicine (0% to 31%). The numbers of patients for which teams were responsible ranged from 1,500 to 21,850, with a mean of 6,902. Teams were fairly stable over time: On average, half of the team had been together for at least 63 months. Mean total working hours was 335 hours per week. Twenty percent of teams were located in cities, 65% in other urban areas, 6% in areas described as both urban and rural, and the remaining 8% were in rural locations.
Measures
Team reflexivity
Team reflexivity was measured with an 8-item measure (Carter & West, 1998; see also Schippers, Den Hartog, & Koopman, 2007). Example items are “We regularly discuss whether the team is working effectively” and “In this team we modify our objectives in light of changing circumstances” (1 = strongly disagree, 7 = strongly agree). Cronbach’s alpha was .82.
Work demands
Our study focuses on PHCTs, teams that are the first port of call for patients seeking health care in the United Kingdom. Two work demands that such health care teams report as particularly pressing and stressful are the objective workload in terms of patient-to-doctor ratio and the quality of the physical work environment, such as the quality of the waiting area for patients, the amount of space, and the comfort of the premises. These two job demands have a high level of variation between the teams, besides being important to all teams. It is therefore these demands we focus upon.
The objective workload of a PHCT depends largely on the number of patients seen and the number of GPs available to complete tasks. 1 Patient-to-doctor ratio as a measure of objective workload is a clear and objective measure that is widely accepted as a good indicator of work demands by those working in this context. Patient-to-doctor ratio was calculated as the size of the practice list divided by the number of full-time-equivalent GPs (see Groenewegen & Hutten, 1991, for a similar measure of objective workload). Objective workload correlates .32 (p < .01) with total hours worked in the team, indicating that a higher workload does result in more working hours for the team. 2
To measure quality of the PWE, the manager of each practice (who was also a team member) was asked to rate the quality of his or her practice PWE on a scale of 1 (very poor) to 5 (excellent), incorporating spaciousness, facilities, quality of public waiting areas, and general condition of the practice buildings. Team managers were the most relevant people to do these ratings, as they were most familiar with the strengths and limitations of their environment. PWE refers to a single latent construct, which is the quality of the environment the team works in; it is the overall sense of physical adequacy as a whole that determines whether or not the GPs can perform the work they need to do. To check the construct validity of this measure, we asked senior managers with organizational responsibility for the teams to nominate 20 teams they felt were housed in either poor, moderate, or good premises. We then surveyed the practice managers of those 20 teams, who were asked to rate their premises on a 1-to-5 scale. The premises nominated as good received a mean rating of 4.9, premises nominated as moderate received a mean rating of 4.0, and premises nominated as poor received a mean rating of 2.8 (overall SD = 0.96). Organizational experts described premises of good quality as having easy physical access, plenty of space, open style of design, and good lighting. In contrast, premises of poor quality were described as having a lack of space, poor physical access, being poorly decorated or poorly lit, and very old (and old looking). These results indicate that the construct validity of the quality of PWE operationalization is acceptable.
Team innovations
Team innovations were measured in two steps, following West and Anderson (1996): (1) asking respondents to list team innovations and (2) having domain-relevant experts rate these innovations. In the first step, we asked respondents to write descriptions of the major changes or innovations introduced by the teams in their work in the previous 12 months. These innovations could relate to, but were not limited to, working practices, innovation in health care, improved services for patients, changes in administrative systems, and improving aspects of the premises. The question was stated as follows: “Please describe below the major changes the team has introduced in its work in the last 12 months (these may be changes in working practices, innovation in healthcare, improved services for patients, changes in administrative systems, or improving aspects of the premises).” For each team, the list of innovations team members reported introducing was produced, and these lists were used as the inputs for external ratings of team innovation. An innovation was included in the list only if two or more team members independently described it in their accounts of team innovation. Two researchers independently produced these lists from team member accounts, and the final list for each team was made up of only those innovations that appeared in each researcher’s cataloguing.
The final lists of innovations contained 1,223 examples of the introduction of new and improved ways of doing things within the teams; the maximum number of innovations reported was 29, and the minimum was 1. The overall mean was 12.5 innovations per team. Examples of team innovations ranged in innovativeness from not very innovative, such as the introduction of regular weekly team meetings and the reorganization of patient records, to (very) innovative, such as the introduction of a completely new clinic.
In the second step, three experts in primary health care rated these descriptions of team innovations. Domain-relevant raters were chosen who were experienced practitioners and who had worked in professional roles that provided a broad overview of primary health care. This approach is based on Amabile’s (1983) rationale for using “domain-relevant experts” to judge creative products. This procedure involved the experts giving a summary rating for each team rather than for each innovation separately.
Team innovations were rated using a 5-point scale on four dimensions (following West & Anderson, 1996): magnitude, how great would be the consequences of the changes introduced; radicalness, to what extent the status quo would change as a consequence; novelty, how new in general the changes were; and impact, to what extent changes would improve PHCT effectiveness. A mean value of the ratings was used (after standardizing the four separate ratings) to give an overall measure of team innovation: Cronbach’s alpha was .91. A mean overall score was calculated by combining the ratings from the external raters. Interrater reliability was calculated using the intraclass correlation coefficient (ICC)(3, 1) and ICC(3, k) form of ICC(1) and ICC(2) (Shrout & Fleiss, 1979) for each dimension. These values were .63 and .84, respectively, the latter falling above Klein et al.’s (2000) suggestion of .80 for good ICC(2) values.
As we did not receive ratings for 1 team, the analyses are performed on 97 teams. In Table 1, we report the intercorrelations between the number of innovations per team and the four dimensions of innovation.
Means, Standard Deviations, and Intercorrelations
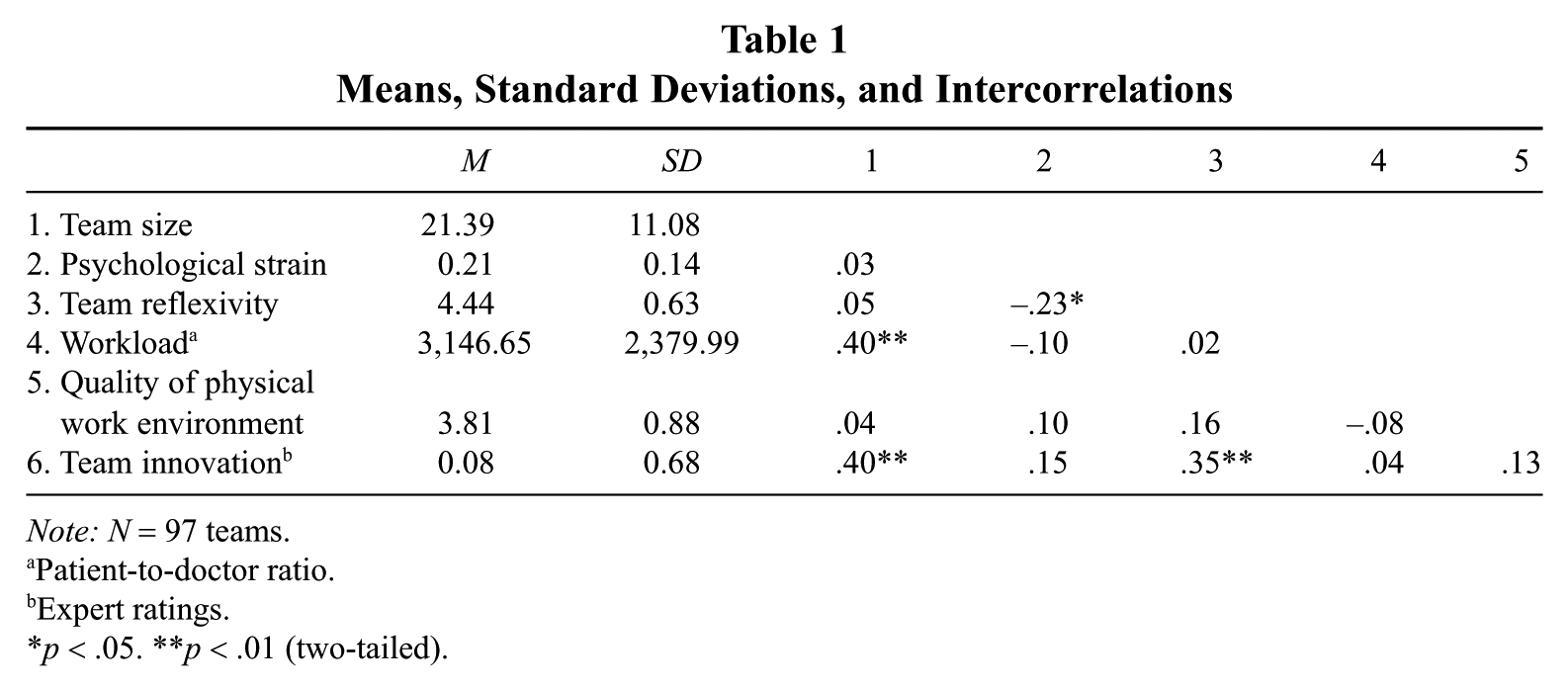
Note: N = 97 teams.
Patient-to-doctor ratio.
Expert ratings.
p < .05. **p < .01 (two-tailed).
Control variables
Team size was added as a control variable since this variable has been shown to influence innovation. Although research in the area of teams has shown that team size sometimes negatively relates to team outcomes because of process loss (e.g., Paulus, Leggett-Dugosh, Dzindolet, Coskun, & Putman, 2002), a recent meta-analysis on team innovation indicated that larger teams are in general more innovative (Hülsheger et al., 2009). Larger teams may simply have more resources, such as money, energy, and skills, enabling them to complete difficult tasks in complex and uncertain environments and to be more innovative (cf. Fay et al., 2006; Stewart, 2006; West et al., 2003). As our sample included teams covering very different sizes of populations, there was larger variation in team size than in many studies, and therefore its inclusion as a control variable was particularly important.
Psychological strain is the extent to which people feel they cannot cope effectively with the demands they are facing in their work and is a psychological state manifested in a subjective feeling in response to the stressors in the environment (cf. Leiter & Maslach, 1988). Despite our focus on objective workload, it is important that we do not discard this more subjective element of work pressure. Some research has also linked stressors and psychological strain to innovation (Bunce & West, 1994). In their research among 333 health care professionals, Bunce and West (1994) noted that 32% of these workers showed innovative coping responses in reaction to occupational stress and strain, that is, by changing workplace factors in an innovative way.
Psychological strain was measured as an individual-level variable, using the General Health Questionnaire (GHQ) 12-item measure (Goldberg & Hilliera 1979; validated by Banks et al., 1980). An example of an item is “Have you recently lost much sleep over worries?” (1 = not at all, 4 = much more than usual). We used the “caseness” measure developed and validated by Hardy, Shapiro, Haynes, and Rick (1999), which examines how many of the 12 items respondents give one of the two highest responses (3 or 4). If a respondent answers in such a way to four or more of the items, Hardy et al. (1999) demonstrated via interviews with clinicians that they would benefit from a clinical intervention, thus representing clinical caseness, a dichotomous measure of whether or not individuals were suffering from psychological strain. Team-level psychological strain was operationalized as the proportion of team members who satisfied this criterion, a configural model of aggregation following an additive rather than a consensus model (Chan, 1998), as this reflects the extent to which the team was composed of members who felt an unreasonable level of strain; this is an accepted way to operationalize psychological strain using the GHQ at the team and organizational levels (e.g., Hardy et al., 1999; Haward et al., 2003; Wall et al., 1997).
Other control variables included location of the practice, differences in age, gender, percentage of GPs, and team tenure. Location of the practice, urban versus rural, was created by collapsing city and urban into the new variable urban and collapsing urban/rural and rural into a rural variable. Adding location as a control variable also did not change our pattern of results. Differences in age and gender were limited between groups, and controlling for them did not change our pattern of results. We therefore proceeded to test our hypotheses with size and psychological strain as control variables in order to preserve degrees of freedom and to minimize the chances for a Type I error.
Results
Table 1 shows the means, standard deviations, and intercorrelations of all variables used in this article. The relationship between team size and team innovation was substantial and significant (r = .40, p < .01). This variable was therefore included as a control variable in all subsequent analyses. Also, a negative and significant relationship between the reflexivity and proportion of team members suffering from psychological strain can be observed, indicating that if the level of reflexivity is higher, the level of strain within the team is lower. Urban/rural location was negatively related to team size (r = −.26, p < .05; not shown in the table), indicating that urban teams were generally smaller than rural teams. This can be explained by the fact that in cities there are more opportunities for what are called “single-handed GPs,” that is, doctors setting up practices by themselves to cover a relatively small area of the city. This would not make sense in rural areas, as the geographical spread covered by the teams has to be larger (e.g., covering several villages); otherwise, there would not be coverage of some parts. Finally, as expected, the relationship between reflexivity and innovation was significant (r = .35, p < .01).
Data Aggregation
Our theory and measurement are aimed at the team level of analysis. We therefore computed rwg(j) (Bliese, 2000; James, Demaree, & Wolf, 1984, 1993), ICC(1), and ICC(2) (Bliese, 2000) to determine whether aggregation to the group level was appropriate. A value of .70 or above is suggested as “good” with respect to within-group interrater agreement (James et al., 1993) and “satisfactory” with respect to ICC(2) (Bliese, 2000). Therefore, rwg(j) had a good average of .83 for reflexivity, and ICC(2) was satisfactory at .70. The value of ICC(1) was .17. Psychological strain was measured individually but, as indicated above, we used the caseness measure (Hardy et al., 1999).
Hypothesis Testing
Prior to analyses, all continuous variables were mean centered (Aiken & West, 1991). The hypotheses suggest two interactions, and we tested whether each added unique variance by testing them in one model. Table 2 reports the series of regression models to test both the main effect of reflexivity on team innovation and the hypothesized moderator effects. In each regression analysis, team size and psychological strain were entered as the first step. As can be seen from the table, there is a significant, positive relationship between team size and team innovation, as suggested by earlier research (Hülsheger et al., 2009). In line with Hypothesis 1, there is a significant, positive relationship between team reflexivity and team innovation (β = .35, p < .01). Thus, teams whose members report greater levels of reflexivity are adjudged to be more innovative by independent raters.
Results of Regression Analyses for Hypothesis Tests With Dependent Variable Team Innovation (expert ratings)
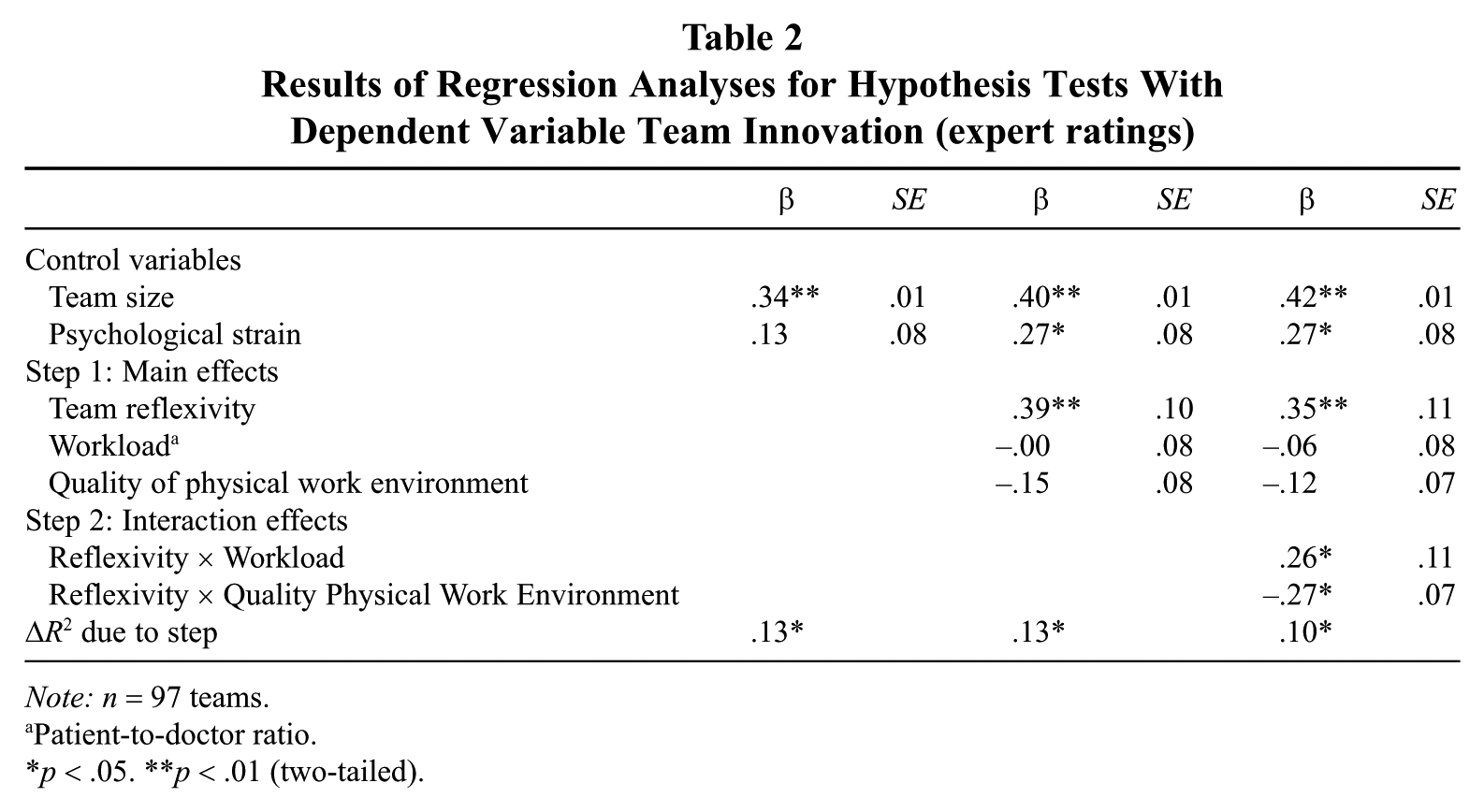
Note: n = 97 teams.
Patient-to-doctor ratio.
p < .05. **p < .01 (two-tailed).
Hypothesis 2 predicted an interaction between reflexivity, objective workload, and team innovation, such that teams with a high workload in terms of patient-to-doctor ratio, that were also more reflexive, were more innovative. The results show that this interaction term also is significant (β = .26, p = .03) and explains unique variance over and above the second interaction term. 3 This effect is shown in Figure 1. It appears that when workload is low, there is no significant relationship between objective workload and team innovation (simple slope test: t = 0.73, p = .47); however, when workload is high, the relationship is significant and positive (t = 4.67, p < .001). Thus, given the significance of the interaction effect, and the results of the simple slopes tests, there is support for Hypothesis 2. When looking at the overall pattern of the interaction, teams with a high workload and low reflexivity differ most from the other teams in terms of innovation (i.e., these teams seem to be especially low on innovation). We explore this further below.
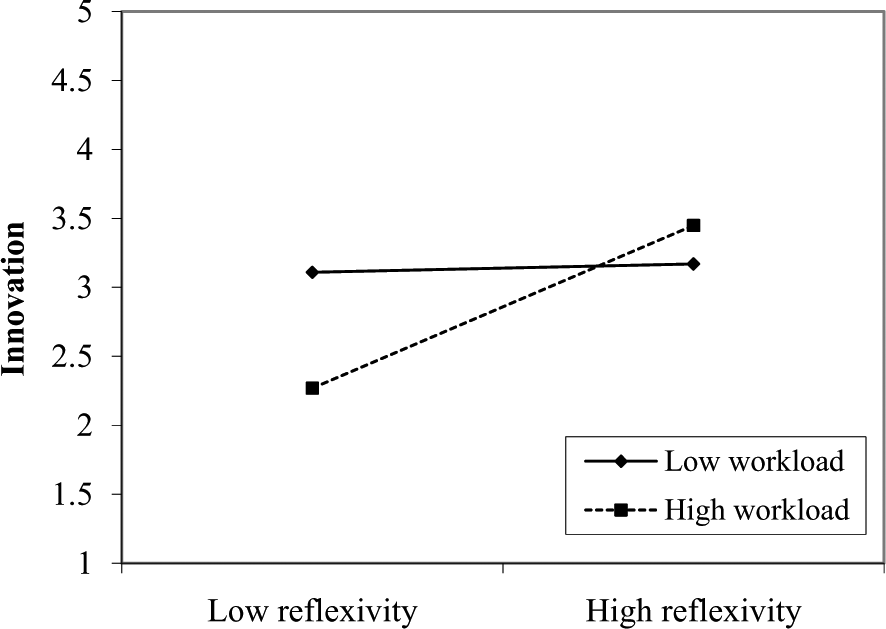
Moderating Effect of Workload on the Reflexivity–Innovation Relationship
Our third hypothesis predicted a moderating effect of team reflexivity on the relation between quality of PWE and team innovation. Supporting our hypothesis, the interaction term between reflexivity and quality of PWE is indeed significant (β = −.27, p = .03), and the nature of this effect is shown in Figure 2. It can be seen that where quality of PWE is high, there is little relationship between reflexivity and team innovation (simple slope test: t = 1.79, p = .08); however, when the quality of the PWE environment is low, the relationship is strong and positive (t = 4.56, p < .001). It is particularly noteworthy how similar this effect is to that for objective workload, despite there being no significant correlation between the two moderating variables. Thus, Hypothesis 3 is fully supported. Note, however, that the overall pattern of the interaction suggests that teams with a combination of low-quality PWE and high reflexivity differ most in terms of innovation from the other teams (i.e., these teams are most innovative).
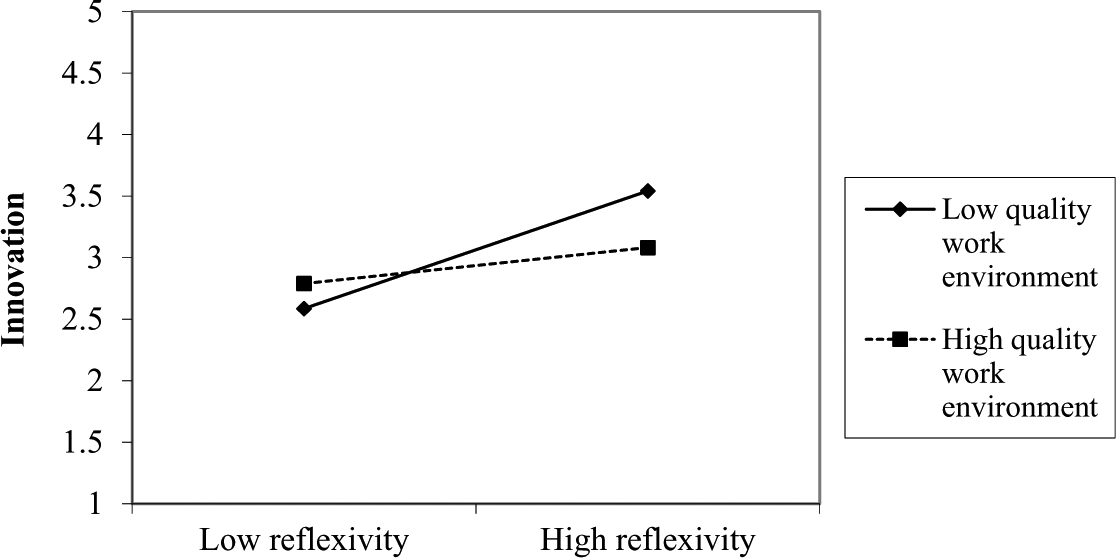
Moderating Effect of Quality of Physical Work Environment on the Reflexivity–Innovation Relationship
Interestingly, although not hypothesized, psychological strain was positively related to team innovation but only when the other variables are taken into account (β = .27, p < .05). When entered in the regression only with team size, the effect is nonsignificant (β = .13, ns). This seems to suggest a suppression effect, a situation in which the magnitude of the effect becomes larger when a third variable is included in the regression equation (MacKinnon, Krull, & Lockwood, 2000; Shrout & Bolger, 2002). When adding reflexivity and strain in one step, the positive effect of psychological strain was enlarged and became significant (increase in beta from .13, ns, to .27, p < .05), possibly because for two teams of a given reflexivity level, the one with greater levels of strain would be more innovative, but otherwise this association may be obscured by the variation due to reflexivity.
Discussion
Team reflexivity has been shown to be important for team effectiveness and performance, but research investigating the boundary conditions of team reflexivity has been scarce (for exceptions, see De Dreu, 2002, 2007). Because reflexivity is an energy-consuming activity, we feel that it is important to illuminate the situations under which reflexivity is cost-effective. We adopted a team-level contingency approach to test predictions about the combined effect of team reflexivity and work demands on team innovation. In support of our conceptual analysis, we found that the relationship between team reflexivity and team innovation was contingent upon team-level work demands. For teams with a demanding environment (i.e., high workload or adverse PWE), team reflexivity was associated with the development of new and improved ways of working.
While we hypothesized that teams with a combination of high workload and high reflexivity have the greatest opportunities for innovation, and slope tests indeed show that the largest effect of reflexivity can be found for those teams with high workloads, the pattern of the interaction essentially shows that teams that have a high workload and are low in reflexivity do worse than other teams in terms of innovation and that the other teams are relatively similar in innovation. This suggests several different potential mechanisms. One could argue, for instance, that high workload blocks teams from being innovative, but being reflexive helps teams to overcome this barrier. Another possibility is that reflexivity is a proxy for good team communication and that teams that do not communicate well suffer when overloaded. 4 A third explanation could be that teams low on reflexivity and high on work demands may avoid problems associated with this high workload, or use work-arounds, rather than dealing directly with them (Tucker, Edmondson, & Spear, 2002).
In contrast to past research, our study did not view the team’s physical environment as a given but as a variable of considerable interest in understanding team innovation (cf. Elsbach & Pratt, 2007; Vashdi et al., 2007). The interaction showed that the teams with a combination of low-quality PWE and high level of reflexivity were most innovative, and the slope analyses indeed showed the largest effect for the low-quality PWE line.
Although not hypothesized, we found a suppression effect for the control variable psychological strain, with strain more positively related to innovation when reflexivity was added to the equation. This is probably due to the fact that, when the proportion of team members experiencing high levels of strain increases, there is a greater sense of urgency to innovate as a coping response (Bunce & West, 1994).
Our study contributes further to the innovation literature by demonstrating that team reflexivity is an important variable in predicting team innovation and that this relationship is moderated by the team’s context (cf. Bamberger, 2008; West, 2002; West, Sacramento, & Fay, 2006). A strength of the current study is the fact that we used field data including a large number of intact teams, where the main dependent variable, team innovation, was based on blind ratings from domain-relevant experts from outside the teams (Amabile, 1983). By showing that the positive effects of reflexivity are contingent upon team demands and working environment, our study develops and extends team reflexivity theory (Moreland & McMinn, 2010; Schippers et al., 2007; West, 1996; Widmer et al., 2009).
Theoretical Implications
This study showed that the work environment has a contingent influence on team innovation; our findings show that teams can actively adapt to the work environment by being reflexive and innovative. Second, we showed that work demands may operate at the team level of analysis and that teams do respond to adverse working conditions, in the form of high work demands and an impoverished PWE, through team innovation as one of a number of potentially adaptive responses. Third, the study adds to our understanding of theory regarding the relationship between team reflexivity and innovation in illuminating the role of work demands, such as workload and PWE, suggesting the value of a targeted use of reflexivity in conditions of high workload and/or impoverished PWE rather than in conditions of low workload and high-quality PWE. In doing so, we have built on, and expanded, the literature on how teams can influence their working conditions.
Managerial Implications
Past research has shown that team reflexivity is positively related to team performance (e.g., Schippers et al., 2008; Schippers, Den Hartog, Koopman, & Wienk, 2003; West, 1996). The same holds for the team innovation–performance relationship (Amabile, 1988). However, reflexivity and team innovation may be time consuming, and especially for teams that do not have a demanding work environment, it is questionable whether the investment is always worth the payoff (cf. Bunderson & Sutcliffe, 2003). The present findings suggest that a targeted use of reflexivity and team innovation may be effective particularly when teams face high levels of work demands, such as a high workload or low-quality PWE. An important management implication could thus be that teams facing adverse working conditions in the form of high demands should be trained to be reflexive in order to become more innovative. Research has shown that a transformational leader can play an important role in engendering a shared vision and reflexivity within a team (Schippers et al., 2008). In this respect, the present findings speak to a contingency approach to leadership (Fiedler, 1978), as leaders should adjust their focus on reflexivity depending on whether the working conditions of the team are satisfying or not. Managers should be cautious about encouraging teams in low-work-demand situations to be reflexive.
Limitations and Directions for Future Research
While an obvious strength of our study is that we tested our hypotheses in a field setting using independent ratings of our key variables—working conditions and team innovation—we should recognize that only experimental studies speak to the causality implied in our research model. Nonetheless, future research could use field-experimental research designs to establish whether high levels of team reflexivity interact with high work demands to produce higher levels of team innovation.
A similar limitation is that while we have evidence about the core process involved—team reflexivity—we do not know about the content of this process. That is, we do not know for sure if and how often reflexive sessions took place, what was discussed in the teams when they reflected, and how these discussions led to team innovations. While such evidence is not a prerequisite for testing our hypotheses, such information would be helpful in further developing our analysis, as it may point to possible contingencies of reflexivity in relation to innovation. Also, research investigating the effect of reflexivity on other group process measures (focus on performance, monitoring, etc.) and on noninnovative performance (e.g., efficiency or compliance) could be helpful in this respect. Moreover, it would be useful to examine these processes in teams of different sizes; the teams we studied were extremely variable in size, and the processes used by some of the larger teams may not be typical of smaller teams, even though they all had a strong self-concept of being a team.
In addition, because workload is measured as the number of patients per GP, it is not clear that it captures the availability of slack time for reflection. It is possible that teams with a high workload might also be required to adopt team-based meetings and conferences to manage the workload and that it is those processes that lead to reflection. In teams with a smaller number of patients per GP, it may be possible to work more independently, and thus there are fewer opportunities for team-based reflection. Future research could use more fine-grained analyses such as interviews and reports from team meetings to add to our understanding of how and when team reflexivity occurs within the team.
A final limitation relates to the innovation measure. We cannot exclude reverse causality in the sense that previous successful innovation may well lead to changes in group processes such as team reflexivity. Future research could longitudinally examine the effect on innovation in order to explore the question of causal direction.
Conclusion
The relation between team reflexivity and team innovation is important for team functioning, and our analysis has shown that reflexivity is especially needed and helpful when work demands are high. Teams often face the challenge of dealing with demands stemming from the work environment that are not always mitigated effectively simply by working harder or sticking to previous work practices and routines. Our study directly addresses this challenge by identifying ways in which teams learn to work “smarter.” Our results suggest that it is possible to make the best of adverse working conditions by reflecting and innovating.
Footnotes
Acknowledgements
This article was accepted under the editorship of Deborah E. Rupp. We wish to thank Jeff LePine and Sebastian Stegmann for their useful comments on earlier versions of this article. An earlier, abbreviated version of this article was published in the Academy of Management Best Paper Proceedings of the 2010 annual conference.