
Abstract
Errors are a recurring fact of organizational life and can potentially yield either adverse or positive consequences. Organizational researchers and practitioners alike have become increasingly interested in understanding the causes of errors and the coping strategies that foster organizational success. Although we have learned much about errors in specific research areas across specific organizational contexts, we know little about how multifaceted forces in organizations, especially when they contradict each other, might affect the pathways of errors in organizations. This review strives to integrate the literature on errors, not only by summarizing conceptual foundations and empirical findings, but also by discussing discrepancies, inconsistencies, and opportunities for research synthesis via level of analysis, temporal dynamism, and priority lenses. At the core of this integrative review is a call for future research to explain how to reduce the underlying causes and negative consequences of errors while promoting positive outcomes and learning benefits in organizations. We close this review by offering suggestions that help develop an integrative, rather than isolated, investigation of errors in organizations.
Introduction
Errors in organizations are essentially unintended and potentially avoidable deviations from organizationally specified goals and standards that can yield either adverse or positive organizational consequences (Frese & Keith, 2015; Hofmann & Frese, 2011). Examples include medical errors like those responsible for thousands of deaths in U.S. hospitals each year; coordination errors, such as the one that resulted in the loss of the $125-million Mars Climate Orbiter; or the numerous mistakes that led to subsequent innovations at 3M. Errors are a recurring fact of organizational life and thus merit study in their own right as an important phenomenon of growing theoretical and managerial significance (Goodman et al., 2011; Hofmann & Frese, 2011).
Despite recent advances in our knowledge regarding errors in organizations (see Frese & Keith, 2015; Goodman et al., 2011; Hofmann & Frese, 2011), different lines of error research have largely progressed in isolation from each other. Moreover, insights from distinct approaches to error in a variety of organizational settings, although considered complementary, sometimes raise inconsistent or competing views that have yet to be reconciled. For instance, whereas error prevention approaches view errors as negative and seek to avoid them at all costs, error management approaches consider errors to be opportunities for learning and innovation and opt to manage and learn from them (see Frese & Keith, 2015, for a review). As another example: on one hand, nurses need to apply short-term remedies for errors to proceed with their duties; on the other, these quick fixes present intractable threats to the so-called second-order problem solving that helps remove the root causes of these errors (Tucker & Edmondson, 2003).
Given that various lines of research have suggested different defense mechanisms related to error, each focusing on a singular view, organizational scholars are calling for a more integrative approach to errors that explores new common grounds of competing views (Goodman et al., 2011; Hofmann & Frese, 2011). In response to this lacuna, we conduct an integrative review of the error literature and suggest future research that transcends the limits of specific approaches and bridges diverse disciplinary backgrounds. We not only acknowledge the interplay between opposing forces and foci affecting error pathways in organizations, but also suggest potential syntheses between these oppositions to stimulate integrative studies.
We review research insights in the error literature according to three fundamental dimensions identified by organizational scholars: level of analysis, temporal dynamism, and priority. Cast in the context of errors, the level-of-analysis dimension refers to the degree to which errors are attributed to individual (e.g., an individual employee) or collective actors (such as a team, a unit, or a system). Temporal dynamism refers to the degree to which organizational emphasis is placed before, during, and after an error occurs; time lags and dynamic properties of the error chain; and the timing of error responses. The priority dimension refers to the tension between prioritizing error elimination and other conflicting demands (e.g., errors vs. innovation) simultaneously. We focus on these three dimensions because the error literatures have suggested them to be building blocks in organizational research in general and applicable to the error context (Goodman et al., 2011). From the managerial viewpoint, level of analysis, temporal, and priority aspects are critical because they reflect the primary dimensions of organizational incentives, culture, resource distribution, and performance strategy.
We begin the review by defining its scope and search methods and proceed to review error research from the level of analysis, temporal, and priority perspectives, paying particular attention to opportunities for future research. We then discuss how to integrate insights into a more comprehensive model and suggest future research directions and managerial practice.
Definitional Issues and Scope of Review
The definition of errors used in this review is consistent with current error literature and refers to action-based errors rather than errors in judgment and decision making (i.e., cognitive biases and heuristics; Frese & Keith, 2015; Hofmann & Frese, 2011). We distinguish error from the concepts of violation, failure, and risk. Violations differ from errors in that they involve a conscious intention to break a rule or to be nonconforming to a standard (Reason, 1990), while errors referred to in this review are unintended behaviors (Frese & Keith, 2015). Failures refer to negative or undesired organizational outcomes that might be caused by a combination of errors, violations, risks, and chance factors (Frese & Keith, 2015; Hofmann & Frese, 2011). However, not all errors lead to failure—when detected and corrected immediately, some errors can generate positive outcomes such as learning or innovation. Errors are also distinguished from risks. Whereas risks refer to the possibility of suffering, harm, loss, or danger and often reside in the environment, errors refer to acts committed by humans or through the interaction of individuals with the environment in an unpredictable way (Frese & Keith, 2015).
Error-related topics have been covered extensively in literatures on quality control, failure, high reliability organizations (HROs), accidents, risk, active learning, and more. Given the breadth of topics, we limit our focus to research explicitly centered on error phenomena whose definition is consistent with ours. We consolidate conceptual work and empirical research on errors into the following areas (see Figure S1 in the Supplementary Materials): error taxonomy, latent errors, error training (avoidance vs. management), error orientation, error reporting, learning from errors, and error culture (aversion vs. management). Although we refer to relevant literatures (e.g., quality management, failures, and HROs) throughout our review, we do not emphasize them as our primary focus.
To identify theoretical and empirical papers for this review, we performed a keyword search in databases (e.g., Business Source Complete, ISI Web of Science, PsycINFO, ProQuest, and EBSCO) and in top management, organizational behavior, and applied psychology journals (following the ISI Web of Science [2014] Journal Citation Report). Our key search words included “error(s),” “mistake(s),” “latent error(s),” “error taxonomy,” “error training,” “error management,” “learning from error(s),” “error orientation,” “error culture,” “individual error(s),” “team error(s),” “organizational error(s),” and “system error(s).” We also manually checked our reference list against a recent meta-analysis (Keith & Frese, 2008) and other review papers (Frese & Keith, 2015; Goodman et al., 2011; Hofmann & Frese, 2011). Considering the target audience and space constraints, we included a total of 65 articles published in the last 25 years (see Table S1 in the Supplementary Materials for a detailed summary of each article).
Below we review error research via the lenses of level of analysis, temporal dynamism, and priority. The relationships described in the next three sections are summarized in Figure 1.

Models That Organize the Error Research Literature
Reviewing Error Literature via the Lens of Level of Analysis
A fundamental issue in error literature is the determination of error origin by level of analysis. Errors in organizations can be classified as individual or collective errors. Individual errors are broadly defined as those that are caused by the individual’s actions alone without any participation by other individuals (Sasou & Reason, 1999). Collective errors are those attributed to the actions of multiple persons within an organizational entity (e.g., a team, unit, department, or the entire organization) or nested between such entities, caused by collective conditions (Goodman et al., 2011). Within the domain of collective errors, we distinguish errors occurring in groups and teams (including units) from those occurring in organizations or systems. Team errors refer to those that occur when team members engage in collaborative and interdependent work, “most commonly a breakdown in internal team processes” (Bell & Kozlowski, 2011: 119). Organizational and system errors occur when “multiple elements – groups, tasks, knowledge, external conditions – converge in unpredicted or unprecedented ways” (MacPhail & Edmondson, 2011: 187-188). Next, we summarize the error literature by examining individual, team, and organizational and system errors according to their antecedents across different levels (see the “Level of Analysis” diagram in Figure 1).
Errors That Occur at the Individual Level
Here we review error literature from an individual perspective and divide our review into individual characteristics and multilevel factors that impact the occurrence of individual errors.
Individual characteristics and individual errors
A large, active stream of error research studies the relationships between individual characteristics, particularly in terms of error training and individual differences in traits and expertise, and the occurrence of individual errors. One determinant line of work focuses on the role of error training—either error management training (EMT) or error avoidance/prevention training (EAT)—in reducing individual errors and improving individual learning. The thoughtful work of Frese and Keith (2015; Keith & Frese, 2008) thoroughly summarizes and reviews research insights in this area. We will not repeat their findings and conclusions; instead, we will highlight and contrast some fundamental differences in the assumptions and reasoning related to the respective training methods, because they result in incongruent findings that deserve further attention. Specifically, EAT emphasizes error-free performance, views errors as negative events that should be avoided at all costs, and suggests providing trainees with specified instructions. In contrast, EMT considers errors to be valuable feedback for learning and encourages trainees to make errors and learn from them (Chillarege, Nordstrom, & Williams, 2003; Frese et al., 1991; van Dyck, van Hooft, de Gilder, & Liesveld, 2010). Moreover, a large body of evidence shows that EMT is more effective than EAT in helping trainees improve future task performance, deal with errors, and learn from them, especially when trainees perform tasks that involve developing new solutions and dealing with frequent error occurrence (Keith & Frese, 2005; van Dyck et al., 2010). A meta-analysis has indeed confirmed that, while it may initially worsen, the performance of EMT trainees does improve over time (Keith & Frese, 2008).
Recent research shows that not all individuals benefit equally from EMT and suggests that individual traits play a moderating role in the relationship between EMT and individual errors (or performance outcomes). For example, Loh, Andrews, Hesketh, and Griffin (2013) conducted an experiment on software training. They found that individuals who are open to experience performed better in the EMT condition than in the EAT condition; individuals who are less open to experience were more afraid to err and performed better in the EAT condition than in the EMT condition. Individuals open to experience tend to be adventurous and are not afraid to explore and make errors; also, they tend to ask more questions and request more assistance during training (Gully, Payne, Koles, & Whiteman, 2002). In another experiment, Heimbeck, Frese, Sonnentag, and Keith (2003) found that individuals with a high performance prove goal orientation (e.g., having a proactive attitude towards task performance) performed better in the EAT condition than individuals with a low prove goal orientation. Similarly, individuals with a high avoidance goal orientation, who are anxious about erring and failing and prefer to evade negative judgments of performance and disapproval, benefited more from EAT than individuals with a low avoidance goal orientation. In addition, individuals with low prove or low avoidance orientations performed better in the EMT condition than in the EAT condition. Individual expertise has also been shown to influence the occurrence of individual errors. For example, Prümper, Zapf, Brodbeck, and Frese (1992) showed that novices (i.e., individuals with limited knowledge and work experience) tend to make more knowledge errors (those due to lack of relevant knowledge) than experts (i.e., individuals with specialized knowledge and rich work experience). However, this trend is reversed with respect to habit errors, defined as “a correct action [that] is performed in a wrong situation” (Zapf, Brodbeck, Frese, Peters, & Prümper, 1992: 317), because experts increasingly rely on routinized actions with limited attention. This finding is interesting and counterintuitive because it challenges the belief that experts make fewer errors than novices and suggests that different actors commit different types of errors.
Multilevel characteristics and individual errors
A central tenet of error literature is the call for using a multilevel perspective to examine how antecedents across different levels can simultaneously influence individual errors (Goodman et al., 2011). Hunter, Tate, Dzieweczynski, and Bedell-Avers (2011) developed a multilevel framework of leader errors and identified several key error antecedents across the individual (e.g., dispositions and individual differences, cognitive bias, expertise and experience, emotion), team (e.g., team climate, groupthink, personalized charismatic relationships, group stress), and organizational (e.g., communication and organization structure, error management culture) levels. This conceptual framework directs our attention to the fact that antecedents across levels may also interact with each other to influence the occurrence and reoccurrence of leader error.
Despite its theoretical appeal, the multilevel investigation of individual errors has been rare. As a notable exception, Naveh, Katz-Navon, and Stern (2015) investigated how a team learning climate (i.e., the shared belief that encourages individual members within a team to learn through exploration and experimentation) interacted with individual characteristics to influence individual errors. The authors showed that whereas individuals who are more open to experiences commit fewer errors when working in a team that does not emphasize such a learning climate, those team members who are less open to experiences commit fewer errors when working in a high learning climate. Interestingly, this finding contradicts the conclusion of the EMT research reviewed above. According to the latter, individuals who are open to experiences should be placed in an environment that emphasizes learning. Combining these findings suggests an interesting interplay between individual traits and environmental constraints: whereas certain individual traits seem desirable for error-free performance in some working conditions, they may work exactly against reliable performance in a different environment; or, individuals with certain traits may seem prone to error in some task environment, while these same traits may help eliminate errors in other environments.
Errors That Occur at the Team Level
We next review research on the influence of team features and conditions on team errors and then proceed to examine the role of multilevel characteristics in team errors.
Team characteristics and team errors
A few studies have investigated the relationship between a team climate and team error rates (e.g., Edmondson, 1996; Fruhen & Keith, 2014). Edmondson (1996) studied a team climate of psychological safety and found a positive association between psychological safety, characterized by open communication about errors, and the rate of errors reported at the unit level. This work highlights the psychological barriers that deter individuals from talking about their own errors and prevent teams and organizations from learning (Edmondson & Lei, 2014). Some studies have investigated safety climate as an important antecedent of team error rates (Hofmann & Mark, 2006) and accident rates (Hofmann & Stetzer, 1996). In particular, Hofmann and Mark (2006) found that a safety climate, characterized by adherence to safety protocols, open communication, and constructive responses to errors, actually reduced medication errors made by nurses, especially when dealing with more complex cases. Similarly, Leroy and colleagues (2012) showed that the relationship between team priority of safety and number of errors was stronger for higher levels of team psychological safety, suggesting that adherence to safety procedures reflects a genuine concern for safety when employees feel safe enough to speak up about errors.
Bell and Kozlowski (2011) proposed numerous factors that can influence error prevention and error management processes in teams. Their theoretical work drew attention to the roles of team characteristics (e.g., member diversity or team complexity that demands coordinated individual performance), team climate (e.g., psychological safety), and team interventions (e.g., training, technology, and automation) in error management in team contexts. Subsequent work extended this framework and investigated how team design and team configuration (i.e., the specific proportions of members with diverse dispositional traits, skills, error attitudes, and emotions in a collective entity; Miron-Spektor, Erez, & Naveh, 2011) help teams avoid and manage errors. In this direction, Chang and Mark (2011) examined the relationship between nurse mix or team configuration (i.e., the number of highly trained registered nurses within a team) and the rate of team errors in 279 nursing teams in 146 randomly selected American hospitals. They found that team learning climate had a negative association with medication errors and that learning climate moderated the relationship between nurse mix and medication errors. In poor learning climates, nursing units staffed with fewer RNs reported more errors than those with more RNs; however, this was not the case in average or good learning climates. This contradictory influence of teams’ convergent and divergent configurations on team errors suggests that, although team configuration can improve certain team performance outcomes such as innovation (Miron-Spektor et al., 2011) and error elimination (Chang & Mark, 2011), it may also increase the total number of error occurrences as well as the incidence of specific error types, because different experts with different characteristics commit different types of errors.
Sieweke and Zhao (2015) advanced current error research by examining team coordination errors within the dynamic and interdependent interactions of team members. Using panel data on NBA teams, the authors found that team familiarity has a U-shaped relationship with team coordination errors and that team-specific leader experience has a moderating effect on this relationship. In particular, the U-shape is less pronounced in teams led by leaders with high levels of team-specific experience. These findings highlight a potential contradiction between the advantages of prior leadership experience and the results of transferring such experience to unique team contexts. That is, prior leadership experience enables a team leader to successfully coordinate team actions by detecting suboptimal routines and introducing new or improved practices. However, an experienced leader who joins a new team may approach coordination in a way that is incompatible with the team’s existing practices, thus creating coordination problems that result in team coordination errors.
Multilevel characteristics and team errors
An increasing number of theoretical works and qualitative studies suggest that team errors occur as a result of the joint effect of antecedences across individual and team levels. For example, Sasou and Reason (1999) analyzed 67 events within the nuclear, aviation, and shipping industries in order to develop a taxonomy of team errors. They suggested that individual antecedents (e.g., high stress; excessive fatigue; and deficiencies in knowledge, skills, and experience) may interact with team antecedents (e.g., deficiencies in communication, team excessive authority gradient, and team excessive professional courtesy) to affect team errors. A similar view can be found in the work of Bell and Kozlowski (2011). Yet exactly how multilevel forces work in concert to create the conditions leading to and inhibiting team errors remains unclear. On one hand, individual and team antecedents may work in the same direction to increase or reduce team errors. On the other, these antecedents can have the exact opposite effect on team errors, with individual antecedents reducing team errors and team antecedents increasing them, or vice versa. For example, specialization and expertise may help individuals commit fewer errors, yet the existence of a high level of task interdependence and specialization in a wide range of domains in a team makes coordination more challenging and may lead to coordination errors.
Errors That Occur at Organizational and System Levels
Research on organizational and system errors highlights the importance and complexity of the highly interdependent dimensions of the work context (e.g., teams, tasks, technology, culture). The boundaries of an organization and a system may overlap to some extent, but errors occurring within an organization differ from those occurring within a system, considering the specific contexts and antecedents of errors relevant to each level. We thus organize this section by reviewing research on organizational and system errors separately.
Errors that occur at the organizational level
One particularly prominent factor in discussions about errors at the organizational level is organizational culture, specifically error management culture (EMC). Van Dyck, Frese, Baer, and Sonnentag (2005) conceptualized EMC as norms and common practices that encourage error detection, communication, analysis, and quick correction (see our expanded explanation in the Temporal Lens section). Research in this stream suggests that EMC is pivotal in reducing negative error consequences (e.g., faulty products, negative publicity, lost human lives) and promoting positive error consequences, including learning and innovation (van Dyck et al., 2005). Recent theoretical work also emphasizes the critical role of safety culture in reducing errors at the organizational level. In particular, Vogus, Sutcliffe, and Weick (2010) developed a theoretical framework explaining how patient safety is produced and sustained through a safety culture. Relatedly, Singer and Vogus (2013) applied and extended a theoretical model of safety culture in healthcare organizations aimed at eliminating errors; they concluded that interventions too often fail to eliminate errors because they fail to develop a safety culture.
Organizational scholars have also developed insights on learning from errors at the organizational level. Edmondson and Lei (2014) suggested that in order to learn from errors, leaders must create an organizational environment of psychological safety that fosters open reporting, active questioning, and frequent sharing of insights and concerns; they must empower learning as a way of identifying, analyzing, and removing hazards that threaten learning and performance. Haunschild and Sullivan (2002) used a panel data of accidents and incidents experienced by U.S. commercial airlines to show that heterogeneity in the causes of errors generally works better for specialist airlines. Generalist airlines (i.e., those possessing large resource space and offering a broad range of products and service), however, learn from outside factors such as the experience of others and general improvements in technology. Moreover, Anderson, Ramanujam, Hensel, and Sirio (2010) examined the hypothesized benefits of interorganizational data sharing, wherein hospitals participate in a regional reporting system for medication errors. Interestingly, this study found that interorganizational error reporting systems increased error reporting rates but not necessarily the rate of corrective actions. This suggests that error reporting or information sharing may not always yield actual learning and improvement and that organizations should analyze reported errors and make improvements (Naveh & Katz-Navon, 2014).
The multilevel nature of errors that occur at the system level
An important line of error studies focuses on system errors, which occur due to complex, unpredictable interplays between a set of interrelated elements—tasks, technology, external conditions—at the boundaries or intersections of different entities such as teams, units, and the entire organization (Carroll, 1998; Leveson, 2002; MacPhail & Edmondson, 2011; Reason, 1990). Early research in this domain focused on high-risk industries, notably Perrow’s normal accident theory (1984). According to Perrow, system errors are caused by interdependent actions and multiple interacting elements that become chained together and are extremely vulnerable to “normal accidents” that are virtually inevitable. As such, more complex and tighter coupling systems are likely to have a higher rate of errors because the potential interactions between interdependent actions and elements in such systems cannot be thoroughly planned, understood, anticipated, and guarded against. Recent HRO and resilience research suggest the opposite, positing that system errors can be avoided consistently through individual and collective vigilance that helps create robust yet flexible processes (Weick & Sutcliffe, 2007). In particular, system resilience can be cultivated by expanding people’s general knowledge and technical capabilities, their behavioral repertoires and skills to improvise, and social and relational networks that can help compensate for any losses (Weick & Sutcliffe, 2007). For example, based on an in-depth study of two nuclear power plants, Marcus and Nichols (1999) found that organizations operating closer to the border of safety respond to warning signs in a resilient rather than anticipatory way; and that these organizations rely on after-the-fact intervention, rather than preparation, foresight, and the provision of countermeasures, to overcome unexpected problems and limitations.
The different points of view of the two schools notwithstanding, they both emphasize a holistic approach to errors that integrates engineering and social systems theory. To this end, the recent multidisciplinary theory of Human Systems Integration (HSI; Durso, Boehm-Davis, & Lee, 2015) offers promising directions for integrating human considerations and psychological factors (e.g., individual differences in traits, personnel, training, safety, organizational culture) with and across all system and situational elements (e.g., equipment, environment, ergonomics) to ensure overall performance by complex systems. A central tenet of the HSI approach is its focus on the multilevel feature of complex systems—that is, every system “is viewed as a system of systems” (Durso et al., 2015: 6). As such, HSI theory highlights that it is not sufficient to examine items independently—one must go beyond a focus on individual workers, tools, tasks, or environments. Extending these ideas into the error context, this implies that different system components, taken separately, may be harmless to performance, but together they can trigger a cascade of errors and organizational malfunctions and breakdowns when they become increasingly sophisticated and interconnected with each other.
Much of the research on system errors focuses on the large-scale, catastrophic errors that blindside organizational systems. Nevertheless, the insights derived from this research have important implications for all organizations that experience smaller-scale, recurring errors, which may not cost lives but can affect product quality, market shares, legitimacy, and reputation. Coping with system errors thus requires a better understanding of the mechanisms that unify all phases and aspects of human considerations and system elements across levels. Research on system errors also suggests some profound relationships between the influences of certain organizational activities (e.g., adherence to rules and policies, error management, specification of individual responsibilities) required to eliminate errors at one level and their possible opposite effect on error occurrence on another. From a top-down perspective, the activities to defend against system-level errors may not be effective at the individual level. For example, EMC, often deemed helpful in reducing system errors, may overly encourage error commission and learning (from errors). Consequently, individuals living in an EMC environment may become less vigilant and mindful at their tasks and are prone to make more errors because they become too comfortable with making errors and reporting them, without engaging in deep learning to achieve reliable performance (Edmondson & Lei, 2014). In another instance, strict structures and organizational design may promote adherence to rules, possibly reducing certain types of errors. But overly emphasizing adherence to rules may restrict the individuals’ focus of attention to dominant tasks such that they do not notice peripheral error cues, or increase their tendency to use well-learned practices, making them too rigid or inflexible to adapt to change (Staw, Sandelands, & Dutton, 1981). From a bottom-up perspective, we would expect a similar pattern in which error strategies targeted at the team or lower level may not work at the system level, because localized best practices at lower levels may be harmful at global levels, as exemplified by the saying “can’t see the forest for the trees.” For instance, clearly specified individual responsibilities can be effective for holding individuals accountable for their error-free performance. However, without an overarching coordination theme, these responsibilities may become diffused on the verge of boundaries of interconnected systems, letting errors fall through the cracks.
Future Research Directions From the Level-of-Analysis Perspective
One notable research opportunity concerns how to match the right individual traits to environmental requirements, given that certain individual traits may become more error-prone or error-suppressing in specific environments. Second, future research can particularly benefit from exploring how team configuration (e.g., novices vs. experts, open vs. conservative members) influences error processes and outcomes. Third, at the collective level (e.g., team, organization, and system), we encourage scholars to develop new models and insights that systematically explore the complex interplay between distinct forces across different levels, given that the steps necessary to eliminate errors at one level of analysis may differ from, or even conflict with, those required at other levels. Therefore, a key research question is to examine how multilevel antecedents interact to create conflicting and synergistic forces that facilitate and inhibit errors.
Finally, we suggest future research should improve the precision of error attribution (or origin) to the right level of analysis, because error phenomena may be far more complicated than it appears. Consider several nurses in different hospital units who separately failed to verify the medicine doses administrated to patients; as a result, patients were harmed. On the surface, these instances could be considered to be individual errors because they concern separate actions by individuals. Yet they might well be a collective error caused by certain shared conditions in the hospital (e.g., lack of medication verification monitoring, or extreme time pressure for turnaround time). Therefore, one step forward is to map out the boundary conditions that are tied to individual versus collective errors, and then identify the specific processes through which errors shift between a lower level (e.g., individual, team) and a higher level (e.g., organization, system). Hence, we urge future research to examine the linkage question of how errors and consequences at one level affect those at another level (see Table 1 for a summary).
Summary of Research Findings, Gaps, and Opportunities, and Related Future Research Directions

Review of Error Literature via the Temporal Dynamism Lens
We now review error literature via the temporal dynamism lens, with a particular focus on processes, dynamic properties, and timing issues (see the Temporal diagram in Figure 1).
An Event Time Frame: Before, During, and After the Occurrence of an Error
A significant portion of error research divides the error-coping process into three distinctive phases: before, during, and after the occurrence of an error (Frese et al., 1991; Goodman et al., 2011). To avoid repeating the conclusions in recent work in this domain, we focus on assessing inconsistent or even competing views according to different event phases.
The “before” phase refers to a time when no error occurs or when the occurrence of an error and its adverse outcomes has not been noticed. During this phase, organizational actors often use prevention strategies to defend against errors, which include planning, standardized operating procedures (e.g., manufacturing protocols, aviation check lists), reinforcing institutional or professional rules and norms (e.g., hand washing in hospitals), and technological advancement or automation. Ample evidence in operational management research (Detert, Schroeder, & Mauriel, 2000) and error management strategies supports this prevention paradigm.
Yet the prevention approach has several limitations, such as the inability to remove or predict all errors, or the inflexibility it imposes (see Frese & Keith, 2015, for explanations). Frese et al. (1991) introduced error management as an add-on strategy to block negative consequences and prevent the same error from happening again (van Dyck et al., 2005). The error management process comprises three phases: error detection, reporting, and recovery (i.e., error correction and learning from errors) (Frese & Keith, 2015). Whereas detection, reporting, and correction activities emphasize real-time interventions at the “during” phase (i.e., the short phase when errors occur and threaten to produce adverse outcomes, but have not yet done so; Goodman et al., 2011), learning activities largely occur “after” the error situation is under control.
Error detection refers to the realization that an error has occurred, whether or not its cause and nature are understood (Sellen, 1994; Zapf et al., 1992). Yet error detection remains a challenge for various reasons. Individuals anticipate errors and understand organizational goals differently (Rybowiak, Garst, Frese, & Batinic, 1999; Sellen, 1994); the level of complexity of a task affects error detection (Frese et al., 1991; Hofmann & Frese, 2011); and delayed or ambiguous performance feedback blurs error signals (Blatt, Christianson, Sutcliffe, & Rosenthal, 2006). Team- or system-level factors (e.g., task interdependence, diffused knowledge structure) also make error detection harder (Bell & Kozlowski, 2011) because teams or systems may develop habitual routines and repeatedly exhibit similar behavioral patterns in any situation without mindfully selecting suitable strategies over alternative options.
Managing errors in real time often requires that identified errors be reported timely so that remedy steps can be taken before harm occurs (Zhao & Olivera, 2006). Yet covering up errors—rather than reporting and openly discussing them—is a more natural tendency in organizations (Nembhard & Edmondson, 2006). In the case of their own errors, if individuals perceive that such errors involve more potential risks and costs (e.g., job loss, embarrassment) than benefits, they will be more likely to hide them (Zhao & Olivera, 2006). People are also reluctant to report errors due to social concerns such as a low status in the organizational hierarchy or relational concerns (Bienefeld & Grote, 2012; Blatt et al., 2006; Fruhen & Keith, 2014; Nembhard & Edmondson, 2006).
During the “after” phase, error management shifts attention to positive outcomes associated with errors, such as learning and innovation (Frese & Keith, 2015; Goodman et al., 2011). For learning to occur, organizational actors are expected to conduct after-error analyses (Vashdi, Bamberger, & Erez, 2013), reflect on the root causes of previous errors (Tucker & Edmondson, 2003), and deliberately experiment with new things (Homsma, van Dyck, de Gilder, Koopman, & Elfring, 2009). Whereas extant work points to cognitive, motivational, and behavioral pathways to achieve learning benefits, Frese and Keith (2015) highlight how emotions such as anxiety, anger, shame, and guilt are related to errors (also see Zhao, 2011; Zhao & Olivera, 2006). In particular, some EMT research explicitly instructs participants to reduce negative emotions (Keith & Frese, 2005), switching from a (self-)blaming mindset to a learning-oriented one (see Keith & Frese, 2008).
Overall, prevention and management approaches suggest somewhat contradictory views. First, whereas error prevention views errors as highly negative and emphasizes precaution, error management focuses on real-time actions to reduce the adverse consequences of errors and highlights errors as opportunities for learning and innovation. As such, error prevention works by emphasizing routines, standardization, and control, while error management encourages adaptation, flexibility, and improvisation. Although scholars consider the two approaches to be complementary rather than contradicting (Frese et al., 1991; Frese & Keith, 2015), their integration is rare, and little research has focused on how to achieve it. One notable exception is a study by Hofmann and Mark (2006). In conceptualizing safety climate as both adherence to safety protocols and constructive responses to errors, the authors implicitly adopted a complementary view, with the former mirroring error prevention and the latter mirroring error management. Their study supports the notion that a complementary approach can have positive effects on errors. In a similar vein, using panel data from 21 administrative units in hospitals, Aron, Dutta, Janakiraman, and Pathak (2011) found that continuous incremental growth in three types of automation (i.e., sensing, controlling, and monitoring) reduces procedural and interpretative error rates. More interestingly, automated error prevention functions and quality management training, both part of an error management perspective, are complementary because they amplify each other’s positive effects on error reduction.
Time Lags and Dynamic Properties of the Error Chain
Emerging research has begun considering the role of time lags and dynamic properties of system complexity in error responses and outcomes. Reason (1990) coined the concept of latent errors, defined as events, activities, or conditions “whose adverse consequences may lie dormant within the system for a long time, only becoming evident when they combine with other factors to breach the system’s defenses” (p. 173). Compared to the conceptualization of active errors, latent errors emphasize some unique aspects of errors. First, latent errors and their (often) damaging consequences may be hidden for an unknown period of time until enabling conditions trigger them (Ramanujam & Goodman, 2003). Second, whereas many nonlatent errors are committed by employees at the “sharp end” of organizations (e.g., nurses, software developers), latent errors often occur within the organizational and managerial spheres (Reason, 1990, 2005).
Ramanujam and Goodman (2003, 2011) used the collapse of Barings Investment Bank to illuminate latent errors. They showed that organizational antecedents such as profitability goals can cause latent errors and that the frequency, variety, and severity of latent errors also increase the chances of adverse organizational consequences (see also Soane, Nicholson, & Audia, 1998). Barings’ collapse highlighted a basic premise concerning latent errors: whereas they seldom produce adverse consequences by themselves, over time they steeply accelerate the creation of new latent errors and create conditions that make such consequences more likely. This point is also demonstrated in the investigation of a Mid-Western Hospital (MWH) incident (Ramanujam & Goodman, 2011), where five different nurses administrated an overdose of heparin to six infants in the same unit over a weekend, which subsequently caused the deaths of three infants and the injury of three others. Although the latent errors of no verification at a particular moment did not incur adverse consequences immediately, they led to adverse outcomes when another error triggered the chain reaction of the latent errors. Reason (1990, 2005) echoed a similar point, suggesting that latent errors are transmitted along various organizational pathways to create the local conditions (e.g., high work load, poor communication, conflicting goals, etc.) that increase the commission of errors and violations.
The key temporal aspect of time lags and latent errors prompts us to consider some critical inconsistences in current error research. For example, latent errors are difficult to detect long before major (crisis) events occur, because consequences associated with these errors are delayed or hidden in organizational systems, or because organizations have limited resources for precaution efforts to defend against these errors. But when latent errors become more obvious, it may be too late to enact effective responses to mitigate them. As another example, to cope with latent errors, it seems logical for organizations to be readily prepared with extremely high levels of vigilance and monitoring (Grote, 2009; Weick & Sutcliffe, 2007). Yet doing so, especially when making the incorrect diagnosis of a latent error, not only taxes organizational resources and incurs additional costs but also translates into interruptions or breakdowns that can create additional latent errors in the system (Ramanujam, 2003). Furthermore, when latent errors are successfully reduced by vigilance and quality control, this positive situation may ironically create an illusion that the system is safe and error-free. Yet the moment monitoring and quality personnel are dismissed and vigilance reduced, latent errors are fed back into the system.
Organizational change is another key temporal aspect associated with latent errors. For example, Ramanujam (2003) showed that discontinuous change (i.e., infrequent, goal-directed shifts in technology, structure, and top management) increases latent errors and that this increase varies with the level of risk. Goodman and Ramanujam (2012) also found that formal, planned, and goal-directed change was positively related to the frequency of latent errors. These studies point to the contradictory influences of discontinuous changes on organizations: although these changes can bring positive outcomes for organizations, they generate uncertainties and complexity, interrupt stability, and reduce vigilance, ultimately yielding more latent errors.
Dynamic Properties of Error Responses and Feedback Loops
Error situations are also characterized by feedback loops and interruptions that are not intentionally planned. Feedback loops refer to changes in one variable or condition that lead to changes in another variable or condition, which in turn directly affect the first variable or condition (Ramanujam & Goodman, 2003, 2011). In the context of errors, feedback loops can be either error amplifying (i.e., positive feedback loops) or error corrective (i.e., negative feedback loops). Ramanujam and Goodman (2003, 2011) suggest that error-amplifying processes often manifest as mislearning of deviation-induced behaviors, escalation of commitment, and reduced attention to and vigilance of increasing latent errors, as we observed in the Barings Bank case (Soane et al., 1998). By contrast, negative feedback loops help organizations diagnose problems, correct mistakes, and improve performance. For example, Edmondson’s work consistently shows that learning organizations, characterized by a willingness to identify, report, discuss, and remedy failures will have fewer latent errors (Edmondson, 1996; Tucker & Edmondson, 2003). In another example, Christianson, Farkas, Sutcliffe, and Weick (2009) suggest a paradigm shift from “learning from” the rare event to “learning through” it as a powerful error-corrective mechanism. Using the case study of the B&O Railroad Museum, the authors show that the museum was able to establish error-corrective mechanisms and gain richer responses to a series of interruptions. Moreover, error-amplifying and error-corrective feedback loops can also interact to change task environments and accelerate the occurrence of (latent) errors. Ramanujam and Goodman (2011) use a mining example to demonstrate this point. One error-corrective mechanism in mining is to have a variety of people, including regulators and inspectors, check the gas levels in multiple locations at multiple times. When a peer minor does no gas-level checks and no consequences occur, others continue this practice, assuming monitoring and corrective actions are not necessary. Over time, such amplification processes become more predominant, and latent or active errors accumulate at an even faster rate.
The dynamic interplay between error-amplification processes, the state of the surrounding environment, and organizational responses was further explored by Rudolph and Repenning (2002) in a system-dynamic model. Although the authors examined interruptions rather than errors, they explicitly discussed the dynamic properties of a system environment fraught with survival-threating errors. In particular, Rudolph and Repenning found that stress induced from an overaccumulation of interruptions can shift an organizational system from a resilient, self-regulating regime to a fragile, self-escalating regime that amplifies them. Moreover, counterintuitively, adhering to preexisting routines instead of implementing alternative responses may be the best way to prevent the overaccumulation of pending interruptions.
The dynamic nature of changing environments fraught with (latent) errors and interruptions highlights the different emphases on dealing with the coexistence of positive and negative feedback loops when an ongoing stream of (latent) errors accumulates. To remove positive, error-amplifying feedback loops and stop the accumulation of (latent) errors, organizations need to reinforce monitoring, control, and rules. However, as error situations evolve, organizations need to reframe and unlearn established rules and routines.
Timing of Error Responses
The timing of error responses often has dramatic effects on organizational performance and outcomes. For example, to prevent catastrophe, the sooner organizational entities suspect a (latent) error, the higher their chances to detect it (Allwood, 1984), and vice versa (Reason, 1990). Also, as stress and anxiety run high and time ticks by toward potential disastrous outcomes, individuals tend to remain silent or postpone error reporting (Zhao & Olivera, 2006). In fact, Uribe, Schweikhart, Pathak, and Marsh (2002) identify the time and extra work needed to document an error and report it as the top two barriers for physicians and nurses to do the latter. Similarly, Tucker, Edmondson, and Spear (2002) find that lack of time and access to key people prevent nurses from reporting errors and problems.
Once errors are clearly declared, organizational actors must formulate interpretations and correction choices quickly, because errors evolve rapidly and their actions also change the situation. However, organizational actors face certain dilemmas. First, too slow or too fast error responses can generate more errors. Second, whereas short-term quick fixes remove the problems at hand, they cannot remove root causes that may bring about more errors. Regarding the first dilemma, a simulation study by Rudolph, Morrison, and Carroll (2009) illustrates how different rates of taking action generate qualitatively different dynamics. For example, doing nothing or holding an erroneous diagnosis clearly makes the error situation deteriorate over time. Yet either acting slowly when unsure or generating alternatives too quickly can make it difficult to collect enough supporting information to confirm a diagnosis and resolve the crisis. Similarly, in two experiments, Brumby, Cox, Back, and Gould (2013) showed that a high (rather than a low) time-cost penalty associated with errors and idle time before resuming the primary task effectively reduces participants’ error rates after task resumption. Together, organizational actors need to find a balancing act for pacing actions: focusing on solving problems and improving error situations rapidly, while taking time to generate alternatives before task resumption.
Extreme time pressure also heightens the dilemma between employees’ heroic problem-solving actions and the need to remove root causes in order to improve the organizational system over time. In a series of studies with hospital nurses, Tucker and Edmondson (2003) found that nurses often implement a short-term fix for the overwhelming majority of medical errors and failures. Ironically, while these quick fixes seem to work well and even create the gratification of overcoming problems without outside help, they can preclude performance improvement over time by impeding operational and structural changes that would prevent the same errors and failures from happening again.
Future Research Directions From the Temporal Perspective
Additional research is needed to address the three temporal aspects—event time frame, lags and feedback loops, and timing of error responses. First, organizational scholars should take a complementary view and investigate whether and how error prevention and error management can be integrated and work in concert to generate desirable performance outcomes. Second, given the lagged effects of error situations, a fruitful research direction is to explore the conditions that accelerate or delay the identification of latent errors and prolong or shorten the recovery window of coping with them. Third, future research should also take a systematic, dynamic approach to studying the role of feedback loops or reciprocal relationships between different foci or forces over time. For example, a learning climate may initially reduce error occurrence within a team and is thus welcomed and emphasized. Yet over time, reduced error rates may create a complacent mindset within the team, which in turn harms team performance. Fourth, we also encourage scholars to explore the role of the timing and duration of error responses in the error chain. For example, how would a combination of acting fast to control the situation and taking time to learn play out in affecting performance and learning over time, especially when the task environment is constantly fraught with time pressure, uncertainty, and ambiguity? What are the boundary conditions that allow for both short- and long-term performance benefits? Understanding these questions moves beyond conceptual models and predictions that use one particular temporal aspect—be it the event time frame, time lags and feedback loops, or timing issues. To this end, we encourage organizational scholars to embrace and leverage the unique temporal aspects of errors and error responses to develop more integrative theoretical models and new insights regarding the relationships between different temporal aspects of errors and performance outcomes. We summarize our key points in Table 1.
Review of Error Literature via the Priority Lens
Errors have significant implications for organizational performance but are not the only priority in organizational life. For example, error coping strategies, especially error prevention, get the highest priority in HROs such as nuclear power plants, the aviation industry, and healthcare, because errors in these fields may have serious and even catastrophic consequences. However, even in these HROs, errors are not the only organizational priority because organizational success depends on many other important priorities, such as learning, financial performance, and reputation (Carroll, 1998). Eubanks and Mumford (2010) examined leaders’ behaviors to demonstrate the influence of different priorities on errors. According to their study, in the face of time pressure, leaders are pressed to focus on a particular aspect of the task at hand without paying adequate attention to other important aspects, which results in errors. Organizational scholars have thus recognized the prevalence of contradictory demands and the coexistence of different priorities, and they acknowledge that findings from a single-priority literature do not always apply to the multiple priorities situations. As such, scholars have begun to explore how different priorities are integrated, or at least do not interfere with each other, to affect error occurrence and consequences. We summarize this stream of research as it relates to the following three areas (see the Priority diagram in Figure 1).
Safety and Active Learning
The active learning theory posits that most learning must occur “online” during the participants’ task performance process (Bell & Kozlowski, 2008). Whereas active learning requires exploration and experimentation, risk taking, and tolerance for errors, employee or customer safety emphasizes zero tolerance for errors and control and requires planning, procedures, and rules. Thus, while active learning entails clear advantages, including with regard to error elimination, it also bears the cost of errors that are a natural by-product of it.
An emphasis on safety does not necessarily allow learning to occur; some learning strategies, such as experimentation, are in direct conflict with the safety goal (Katz-Navon, Naveh, & Stern, 2009). For example, medical residents are usually the frontline providers of inpatient medical care and play a complex role in taking tremendous responsibility while being novices they must still learn and master their professional skills. Therefore, it is understandable that residents need to learn actively by doing and by making more errors. However, at the core of high-quality medicine, they must keep patients safe and eliminate medical treatment errors. Katz-Navon et al. (2009) analyzed this dilemma, showing that when both priority of safety and active learning climate were high, the number of errors committed by resident physicians was higher, as compared to a situation where priority of safety was high and active learning climate was low. These results suggest that although organizations tend to encourage active learning and priority of safety at the same time, this is not an optimal combination for minimizing errors because a tension exists between the two.
Error Management and Innovation
Innovation refers to the generation of creative solutions, which are also useful, implementable, reliable, and free of errors (Miron-Spektor et al., 2011). Frese and Keith (2015) claim that error management and innovation are complimentary. That is, error management and innovation both encourage and are encouraged by values of open communications and idea generation (Frese & Keith, 2015). First, innovation is inherently susceptible to errors and even increases the occurrence of errors by generating new breakthrough ideas, encouraging openness to different ways of thinking, breaking existing paradigms, taking risks, implementing trial-and-error methods, and promoting tolerance for errors (Miron-Spektor et al., 2011). For example, new technologies can create new types of errors in the processes of exploration and experimentation (Hammond & Farr, 2011). However, when error management is a priority, efforts to control the potential damage of errors, reduce the potential for error cascades, and prevent future instances of similar errors are emphasized (van Dyck et al., 2005). As such, errors are made in an environment of open communication, which is assumed to enable quick error detection, damage control, and effective error handling.
Second, a complementary perspective also suggests that innovation may eliminate errors. For example, although automation may not always reduce all types of errors (Bainbridge, 1982), innovation characterized by error prevention functions (e.g., recording and monitoring of actions) does have a great impact on the medical staff’s behavior related to the reduction of medical errors (Aron et al., 2011). Specifically, automation of core error-prevention functions increases the benefits of training clinical and nonclinical staff members in quality management procedures. Technology enhances the positive effects of quality management training pertaining to the reduction of medical errors. In this respect, Naveh and Erez (2004) show in a longitudinal study that prioritizing both quality and innovation reduces the cost of poor quality dramatically. Note that this study does not assess errors specifically as a quality measurement. However, according to research on quality management, errors are an inherent part of quality (Miron-Spektor et al., 2011). Therefore, Naveh and Erez’s findings (2004) shed light on the relationship between innovation and error reduction. That is, the implementation of opposing management practices, such as a combination of the ISO 9001 quality management standard and teamwork, may enable both innovation and quality.
Third, errors can lead to innovation and exploration because they are important for scientific discovery. A surprising and unexpected result associated with errors may often be the starting point for innovation and new discoveries when learning and no blaming are emphasized. Studies on quality management also provide examples of a complementary approach in which error prevention and corrective responses to errors lead to continuous improvement and incremental innovations (e.g., Detert et al., 2000; Naveh & Erez, 2004).
Finally, an error-free priority may also harm innovation, because organizations are discouraged from taking risks and exploring new ideas through trial-and-error methods when zero-error performance is emphasized. Using data from 41 teams in an R&D company, Miron-Spektor and colleagues (2011) found that the inclusion of creative and conformist members in a team enhanced the team’s radical innovation, whereas the inclusion of attentive-to-detail members hindered it. The authors explained the results by suggesting that creative members might introduce task conflict and discourage team adherence to standards; in contrast, attentive-to-detail members often enhance team adherence to standards and assist in error prevention.
Thus, there is a tension between error management and innovation. Whereas innovation is inherently susceptible to error and even increases the occurrence of errors, a complementary perspective suggests that innovation may eliminate errors. The tension resulting from the priority assigned to error elimination and to other organizational goals may contribute to the elimination of errors, but it may also increase error occurrence.
Formal and Informal Error Coping Strategies
Tension may also exist between formal error coping strategies and informal messages from top and middle managers. Formal error strategies refer to a fixed set of rules, procedures, and structures for coordinating and controlling activities in response to errors, while informal strategies consist of the implicit norms, values, and beliefs that underlie error-related behaviors. Exploring the interplay between formal and informal error strategies is important to explain organizational outcomes (Katz-Navon, Naveh, & Stern, 2005). Formal error-coping strategies and informal signals of managers’ priorities complete each other when there is alignment between the enacted and espoused priorities and when there is a large extent of congruence, rather than misalignment, between managers’ words and deeds. In other words, managers’ messages and rhetoric without actual implementation may be perceived as an empty declaration of intentions. Or, formal action plans without management support will probably not be fully executed (Naveh & Katz-Navon, 2014). Given the priority assigned to learning and innovation, informal signals that fully support the priority status of error elimination are not ensured in all cases. Several studies demonstrate the consequences of misalignment between formal and informal error-coping strategies for error occurrence. Katz-Navon et al. (2005) observe that the conflict between a low safety priority and extensive formal managerial safety practices is expressed in high error rates as employees receive conflicting messages about the importance of safety within the unit. Similarly, Leroy et al. (2012) find that when head nurses’ words and actions align, when they practice what they preach, this signals to nurses that their concern for treatment errors is genuine and that it is safe to admit treatment errors. In sum, organizational priorities other than error elimination, such as active learning and innovation, may weaken the informal message about the importance of error-free performance. Counterintuitively, managers who invest less, rather than more, in formal error practices may resolve the message inconsistency, and consequently reduce the occurrence of errors.
Future Research Directions From the Priority Perspective
More research is needed to examine how different priorities are coupled with each other to affect error occurrence and consequences, because many important questions remain unanswered. For example, what are the mechanisms (e.g., mediators) by which different priorities promote or inhibit error occurrence? What are the conditions (e.g., moderators) that enhance or attenuate the conflicting influence of different priorities on error occurrences and outcomes? More specifically, what is the relationship between error management and innovation? And between learning and errors? Furthermore, current research largely focuses on the impact of dual priorities (e.g., error prevention versus management, safety versus active learning, routine versus nonroutine operations) on error occurrence and organizational outcomes. Yet it could be fruitful to consider a multiplicity of priorities (e.g., safety versus active learning versus cost reduction) in organizations. Needless to say, a research endeavor in this direction presents a host of challenging theoretical and empirical issues. For example, what overarching theories can integrate a disparate set of organizational priorities? Should we reduce or embrace tensions arising from these priorities in order to achieve desirable performance outcomes? In this respect, the paradox paradigm (Smith & Lewis, 2011), which has yet to be discussed in the error context, may provide a helpful framework. According to this paradigm, embracing tensions and finding ways to “live with” them may be one, or the only, solution if competing priorities never go away. In a more exploratory note, it seems plausible to find a dynamic equilibrium in the coexistence and coplay of different, sometimes competing, priorities as these move in and out of the center stage of organizational life.
Discussion: An Integrative View of Error Research
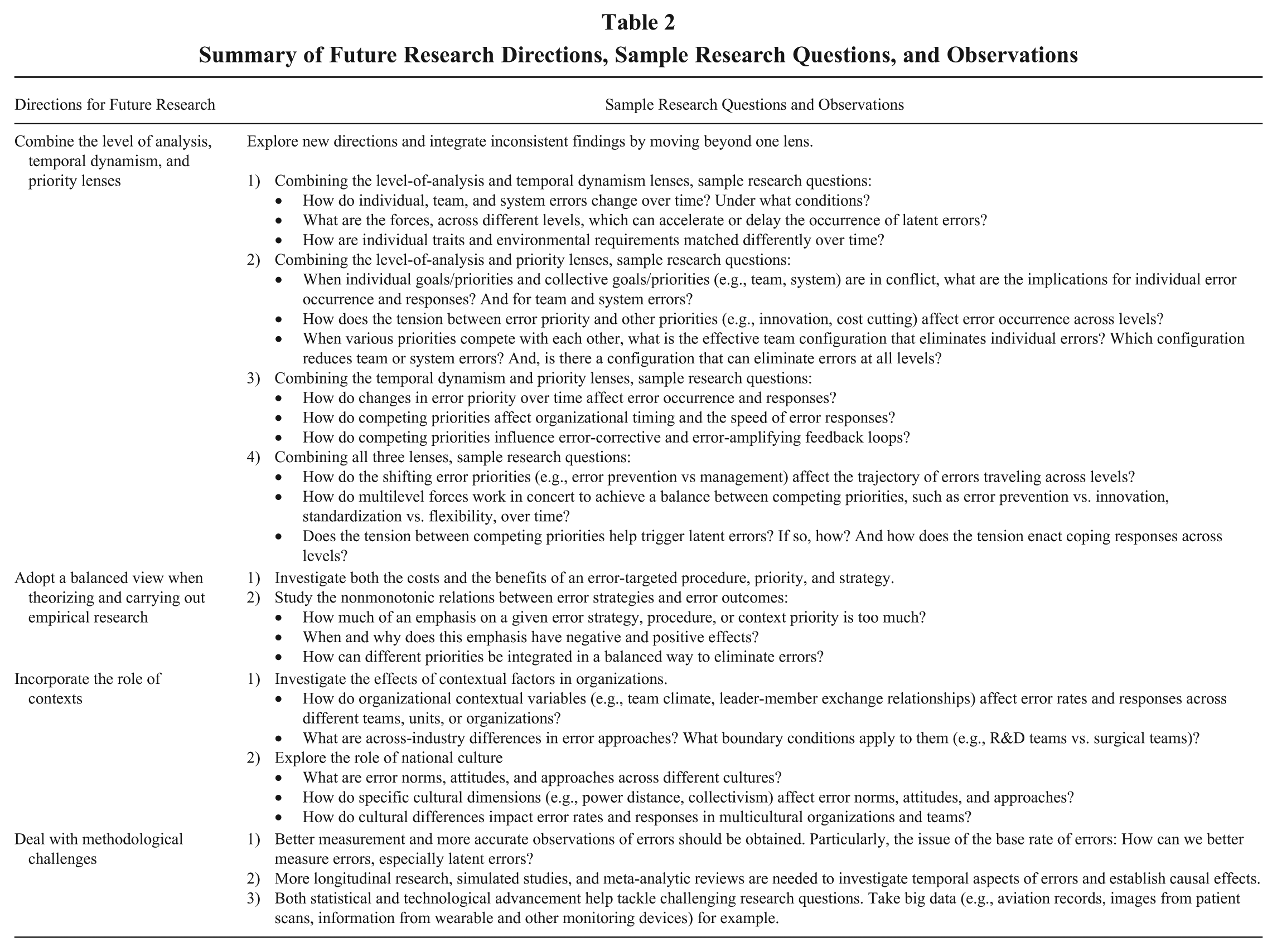
Three observations stand out from our review according to each specific lens (see Table 1). First, a large portion of error research refers solely to antecedents at one level of analysis, with sparse attention to a multilevel approach. Moreover, a recurrent pattern in the literature shows that certain error strategies implemented at one level may have a different impact on errors occurring at another level. Second, error research has primarily adopted a static, rather than dynamic or temporal, approach, masking the opportunities for exploring inconsistencies and contradictions. Third, errors are not the only priority in organizational life, and an emphasis on error elimination may be a double-edged sword for organizations. As a result, each line of error research looks at a particular aspect of errors through a certain lens, leaving considerable room for a more integrative framework that can better capture the complexity of error phenomena and explain inconsistent research findings (see Figure S2 for the cross-categorization of included articles). To integrate the research insights and observations, we highlight below four key research needs that would significantly advance theory and research (summarized in Table 2).
Summary of Future Research Directions, Sample Research Questions, and Observations
Directions for Future Research
First, combine the level of analysis, temporal dynamism, and priority lenses
Researchers should begin to make inroads into combining different lenses to complement existing models based on a specific lens. Pursuing this issue suggests considering additive, interactional, or both additive and interactional relations between lenses. We highlight below four key combinations of different lenses that, if adopted, can significantly advance our understanding of errors in organizations. First, significant opportunities exist in combining the level of analysis and temporal dynamism lenses. This suggests the value of recognizing the temporal dynamics inherent in the error occurrence and coping processes across levels, and the ways in which organizational actors across levels move back and forth between different error response mode over time (see sample research questions in Table 2). This multilevel, dynamism-oriented approach enables scholars to better unpack the complex, time-based relationships between the change in error antecedents across levels (e.g., individual training, error climate, system procedures) and subsequent organizational outcomes across levels (e.g., individual performance, team errors, organizational learning). Second, our understanding of errors could be deepened by considering both the level of analysis and priority lenses. Here, the research goal is to trace the interplay between multilevel forces, with different interests and priorities, and organizational responses across levels to error occurrence and learning. More theoretical development and empirical investigation are needed to understand the factors that influence reliability-innovation, or error prevention-management, routines-flexibilities trade-offs that are inherent in complex organizational life. Third, combining temporal dynamism and the priority lenses opens up many research questions and points to hypotheses worth testing. For example, the ebb and flow of error priority and other competing priorities is likely to play an important role in explaining error occurrence and related responses over time. More fundamentally, as discussed previously, when organizational actors face tensions between competing priorities, we have yet to know how to achieve a balancing act to reach desirable performance outcomes. Finally, it would be most challenging yet intriguing to combine all three lenses to synthesize the extensive research literature. This combination may sharpen the conceptualization of errors in organizations and help us systematically address the “what” (i.e., nature, origins, antecedents, consequences), “how” (new relationships, dynamic processes, feedback loops), “where” (new boundary conditions, contingencies), and/or “why” (new causal logics) of preventing, managing, and learning from error in organizations (see Table 2).
Second, adopt a balanced view when theorizing and carrying out empirical research
Existing inconsistencies in current research challenge us to rethink our research conclusions concerning error processes and coping strategies. We thus encourage scholars to take a balanced view regarding inconsistencies, and to consider both the costs and the benefits of an error-targeted procedure, priority, and strategy. For example, it is possible that the benefits of adhering to rules to achieve an error-free performance may come at the cost of adaptability and creativity. It is also possible that a learning climate may backfire when employees blame “the system” for any errors they commit without taking personal responsibility. Moreover, adopting a balanced view and offering possible explanations for inconsistencies and tensions may challenge the implicit assumption that the relationship between error strategies and error outcomes is linear. Organizational scholars have indeed discovered that, at high levels, the positive effects of certain error procedures, priorities, and practices turn negative (Katz-Navon et al., 2005; Sieweke & Zhao, 2015). Future investigations should become attentive to the nonmonotonic effects associated with error phenomena: is the relationship between error antecedents and error outcomes quadratic, or inverse, or logarithmic? More specifically, we have yet to answer important questions such as, How much of an emphasis on a given error strategy (e.g., error prevention, management), procedure (e.g., automation), or context priority (e.g., safety, learning) is too much? When and why does this emphasis have positive effects and negative effects?
Third, incorporate the role of contexts
By “context” we refer to a set of relatively stable features of a setting that shape the processes, responses, and outcomes of errors (Goodman et al., 2011). Contextual factors can set the pace and priority of error-related actions and performance activities. Future research should examine how a variety of organizational contextual variables (e.g., team climate, leader-member exchange relationships) affect error rates and responses across different teams, units, or organizations. Researchers should also synthesize knowledge from multiple industrial (e.g., reliability- or innovation-driven industries) and environmental (e.g., competition intensity, task complexity) contexts so that we can understand variations in error occurrence and responses not just across individuals and work groups, but also across organizations, industries, and geographical locations. For example, 23 of the 51 empirical studies included in this review were conducted in high-risk industries or HROs. Applying the findings from one setting (e.g., aviation, healthcare) to other settings (e.g., high technology, banking) requires researchers to work hard on identifying the nature and mechanisms underlying the error processes that hold true across contexts and exploring the boundary conditions in which these processes are particularly powerful. Moreover, cross-cultural comparisons of error antecedents, processes, and outcomes, and the underlying mechanisms explaining these effects, warrant attention (Gelfand, Frese, & Salmon, 2011). Cultural factors become even more critical as we seek to understand how error strategies unfold in an ever-growing global context. For example, there is more tolerance for error making and more emphasis on creativity and entrepreneurship in Israel compared to countries like Germany, where adherence to rules, standards, and procedures is highly valued. In another example, the Fukushima disaster suggests that in collectivistic cultures with high power distance, reflexive obedience, reluctance to question authority, and “sticking with the program” are the main factors leading to catastrophe. Many questions need to be explored: across different cultures, how are errors perceived, positively or negatively, in the workplace, and how do error responses vary? How do cultural differences impact error rates and responses in multicultural organizations and teams?
Finally, deal with methodological challenges
First, studying errors requires developing better measures and obtaining more accurate observations of errors. Given that most studies examine errors that have actually occurred, more research should test the base rate of errors (e.g., how many actual errors we observe and measure), paying particular attention to latent errors (e.g., how can we better study and measure them). Second, researchers should build a better alignment between theory and method to understand the processes and changes related to errors over time and thus to assess causality. The temporal-focused research approach can enable error scholars to test key predictions about how key dynamics of error situations evolve over time, and also to begin specifying the causal links and feedback loops that are central to theories about the relationship between errors and, to highlight just two examples, safety or innovation. Although reciprocal models filled with feedback loops are extremely challenging to test in real time, we encourage researchers to make efforts in this direction by using a longitudinal and dynamic design. For example, simulated studies are a feasible means to try this dynamic approach. Meta-analytic reviews also provide a quantitative foundation for some of the most forceful conclusions and recommendations. Third, exciting methodological and technological developments offer error researchers interesting and powerful tools to understand error phenomena, explore related intervention strategies, and assess the latter’s effectiveness. For example, large-scale integration and analysis of “big data” (e.g., aviation records, images from patient scans, information from wearable and other monitoring devices) can boost the generation of high-quality evidence concerning errors and their remedies and address the methodological limitations previously mentioned (e.g., reciprocal models, longitudinal effects).
Implications for Management Practice
Our review has important value for organizations and the actors within them. Consider the example of healthcare providers who engage in patients’ safety assurance and error elimination activities such as following clinical guidelines and accreditation standards for evidence-based medicine, improving the willingness to report, using technology to eliminate errors, and implementing data-sharing systems. Moreover, the healthcare industry strives to learn from HRO industries (e.g., aviation, nuclear power plant). However, based on the current review, managers may come to realize that the inconsistencies or tensions between different error strategies are inherent in the system, and that implementing the above-mentioned practices would not always be optimal. Instead, a balanced view of errors and an integrative approach to them are required. As a first step, managers should integrate error-defense activities across the individual, team, and system levels. For example, they should provide individual employees with skill training to achieve error-free performance and strengthen the learning climate. Second, managers need to pay attention to the temporal aspect of errors. For example, they may alter specific error-defense strategies before, during, and after error occurrences, or consider the performance implications of latent errors. Third, managers need to be aware of inherent tensions between error-related and other organizational priorities. For instance, while the R&D team aims at designing a sophisticated prototype that is error-free and may require a long period of development, the team needs to cope with the time and resource constraints to bring the prototype to the market.
Summary and Conclusion
This review offers an integrative framework for error theory that indicates how this phenomenon is central to certain inconsistencies or even tensions in organizational practices, and how we may reconcile them. We suggest that there is value in examining differences and controversies across investigations to address unanswered questions and identify new research directions. We hope that our work suggests ways to understand the current state of error research and sets challenging directions for future research that will uncover the complexity of errors.
Footnotes
Acknowledgements
We thank Fred Oswald for his encouragement and guidance throughout the development of this article. We are grateful to John Carroll, Gudela Grote, David Hofmann, Alfred Marcus, and two anonymous reviewers for their insightful comments and feedback.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.