
Abstract
Third-party accreditations and certifications can provide legitimacy or signal trustworthiness about an organization and its products or services, and with very little exception, the vast majority of research on these labels focuses on their benefits. Yet the value of becoming accredited may change dramatically over time. Little research, if any, has examined the processes through which this occurs. Here, I develop theory about three mechanisms that could each tarnish the value of accreditation and reduce its performance impact. First, “quality patching” occurs when organizations are penalized if they seek accreditation shortly after problems occur, as observers believe such pursuits reflect superficial impression-management efforts. Second, “legitimacy dilution” occurs when the value of third-party accreditations becomes diluted as third parties certify more and more businesses. Finally, “stigma transfer” occurs when a newly accredited organization experiences spillover from quality problems at other accredited organizations. Empirical tests provide support for quality patching and legitimacy dilution but not for stigma transfer. Results suggest that organizations gaining new accreditations under some circumstances may benefit much less than organizations that gain those same accreditations under different circumstances.
Keywords
One of the primary challenges facing many businesses involves convincing consumers that they can deliver consistent, reliable, and high-quality products and services, and this challenge is compounded when those products and services, or the underlying organizations, are difficult for outsiders to evaluate (Rhee & Valdez, 2009; Rindova, Petkova, & Kotha, 2007; Rindova, Williamson, Petkova, & Sever, 2005). Various solutions to this ubiquitous challenge have been proposed, examined through academic research, and used by businesses in practice (e.g., Barney & Hansen, 1994; Benjamin & Podolny, 1999). Of these solutions, third-party accreditations, certifications, or other similar labels are particularly appealing signals given that they represent the views of potentially objective external parties rather than those of the organization’s own members (Podolny, 1994; Polidoro, 2013; Rao, 1994).
In this context, third-party accreditations refers to certifications or assurances by third parties, such as industry trade groups or regulatory associations, that a business conforms to certain quality standards or follows specific socially acceptable practices or guidelines (Barnett & King, 2008; Graffin & Ward, 2010; Harbaugh, Maxwell, & Roussillon, 2011; King, Lenox, & Terlaak, 2005). The use of these certifications has increased during recent years, making them an important topic for scholarly research as well as managerial practice (Graffin & Ward, 2010; Harbaugh et al., 2011; Polidoro, 2013; Wijen, 2014). And with very little exception, the vast majority of academic research on these labels within strategic management, organization theory, and other related fields seems to suggest that accreditation tends to benefit the receiving organizations (e.g., King et al., 2005; Polidoro, 2013; Rao, 1994; Sine, David, & Mitsuhashi, 2007).
According to extant theory, this occurs because third-party accreditations can provide an organization with legitimacy; that is, they can signal congruence between an organization’s values and those of external stakeholders or otherwise communicate trustworthiness about an organization and its products or services (Dowling & Pfeffer, 1975; Meyer & Rowan, 1977). This information is particularly useful when consumers or other external groups have limited direct information about an organization’s activities (Barney & Hansen, 1994; Graffin & Ward, 2010). Indeed, research consistently shows that these accreditations can improve organizational performance or provide other advantages, as external parties who face uncertainty could use this information to determine whether and how to interact with particular organizations within the field (Barnett & King, 2008; Barney & Hansen, 1994; Polidoro, 2013; Rao, 1994). Although organizations may not necessarily conform to the spirit of these accreditations in practice (Wijen, 2014), there appears to be little doubt that being accredited can boost organizational legitimacy and performance or, at the very least, that it could do no harm (Graffin & Ward, 2010; Polidoro, 2013; Rao, 1994).
Yet, in practice, newly accredited organizations are unlikely to universally benefit through the accreditation process. Instead, the value of becoming accredited likely fluctuates over time. For instance, external parties may use knowledge regarding the performance of accredited organizations to facilitate their underlying evaluations of organizations that newly receive those designations (Graffin & Ward, 2010; Harbaugh et al., 2011; Montiel, Husted & Christmann, 2012). If so, external parties that believe a specific accreditation might not accurately reflect organizational quality are less likely to use an organization’s accreditation to inform their behaviors, and the signal value of that accreditation, along with its benefit to organizational performance, are likely diminished. Despite the dynamic nature of this process, most research on organizational accreditation presumes that becoming accredited tends to consistently benefit organizations. In contrast, little work, if any, examines whether and how an accreditation might instead become tarnished, such as through negative actions by currently accredited or potentially accreditable organizations (Harbaugh et al., 2011; Waguespack & Sorenson, 2011). Yet, some evidence suggests the importance of this understudied process. For instance, Harbaugh et al. (2011) argue that consumers face greater uncertainty regarding the benefits of certification when multiple certification standards exist in a particular setting. Similarly, consumers and other external parties likely incorporate a wide variety of other information into their evaluations of the certification process, and these evaluations can certainly affect organizations that pursue and successfully obtain those certifications.
In this article, I develop theory about three distinct but related processes that could each tarnish the value of third-party accreditation and ultimately reduce the performance benefits of such designations. First, I describe the notion of “quality patching,” whereby organizations are penalized if they seek accreditation shortly after quality problems occur, as external observers infer that such pursuits merely represent an instrumental or superficial attempt to patch the organization’s problems or repair its image. Second, I consider the possibility of “legitimacy dilution,” whereby the legitimacy conferred by third-party accreditations becomes diluted as third-party organizations certify more and more businesses. Finally, I examine the process of “stigma transfer,” whereby newly accredited organizations experience a spillover penalty when quality problems occur at other organizations with the same accreditation. In each case, I propose that the theorized condition will reduce the performance benefits of new accreditation, in effect by negatively moderating the direct relationship between new accreditation and organizational performance.
I test related hypotheses on a panel of home health care agencies operating in the state of California from 2004 through 2013. Home health agencies (HHAs) are agencies that provide or contract to perform health care services for elderly, disabled, or other chronically ill populations within patients’ homes and residences. This is an appropriate setting in which to study accreditation because HHA quality is difficult for consumers to directly evaluate, partly because reliable information about HHA performance is scant and also partly due to the fact that HHAs typically serve marginalized or homebound populations with limited access to information about care alternatives. Given these challenges, HHAs can voluntarily obtain third-party quality accreditations and communicate these credentials to the market. In this context, I am able to examine the performance impact of these accreditations while controlling for several important alternative explanations and confounding factors.
Below, I discuss the study’s theoretical framework, beginning with a review of the direct relationship between accreditation and organizational performance, and then I forward each of the study’s moderating hypotheses. Following the theory, I describe the study’s empirical setting, methods, and results. I conclude with a discussion of the study’s implications for research on third-party certifications, organizational legitimacy and reputation, and related areas.
Theory and Hypotheses
Third-Party Accreditation and Organizational Performance
Third-party certifications, accreditations, and other similar designations refer to assurances or endorsements provided by influential or well recognized third-party agencies regarding particular organizations within a given domain (Graffin & Ward, 2010; Polidoro, 2013; Rao, 1994). For example, organizations within certain industries can be certified by industry associations, trade groups, or other entities as conforming to specific fair trade practices, sustainable harvesting or fishing standards, clean emissions thresholds, or other guidelines and standards, and certified businesses can communicate these certifications to other organizations or the general public through their marketing and promotion efforts (Sine et al., 2007; Waguespack & Sorenson, 2011; Yeung, Lo, & Cheng, 2011).
In some cases, these designations accurately reflect the certified organizations’ underlying practices or quality, and third-party agencies may require inspections or other due diligence by organizations in order to preserve the integrity of their accreditation process. In other cases, however, accreditation may be a less reliable predictor of organizational quality. For instance, third-party inspections may be infrequent or incomplete, or organizations may pay for desirable treatment, and evidence indicates that the certification process can sometimes be coopted (Waguespack & Sorenson, 2011).
Regardless of whether accreditation is an accurate reflection of organizational quality, the crucial point identified by much prior research is that people and parties who interact with organizations often believe that it is an accurate reflection (Montiel et al., 2012; Polidoro, 2013; Yeung et al., 2011). According to Rao (1994: 32), accreditations and certifications “provide extrinsic criteria of fitness and reduce the ambiguity caused by the lack of standards and the absence of complete knowledge,” and as a result, they “enable organizations to score favorably in relation to their rivals, induce them to devote resources to visible criteria of performance, stratify organizations, and generate status orderings of organizations that determine their access to resources.” This sentiment is echoed by many other studies of the certification process and through findings such as the possibility that accreditation boosts organizational legitimacy (Graffin & Ward, 2010; Rao, 1994), attracts potential exchange partners and lowers the uncertainty of transacting with the organization (King et al., 2005; Montiel et al., 2012), facilitates new ventures or market entry (Sine et al., 2007), and protects against competitive threats by uncertified rivals (Polidoro, 2013) and even that gaining accreditation may lead to increases in executive compensation (Yeung et al., 2011).
While a variety of theoretical processes have been forwarded, the central mechanism underlying these and many other similar findings involves signaling (Rao, 1994). External parties who wish to interact with organizations tend to have expectations regarding what they want to gain through these interactions (Graffin & Ward, 2010). However, the ultimate outcome of these interactions is difficult to anticipate in advance, and when combined with information asymmetries, such as their limited knowledge about the organization’s internal practices, these external parties tend to face uncertainty about their potential interactions with particular organizations (Graffin & Ward, 2010; Polidoro, 2013). More specifically, while considerable research suggests that external observers may obtain information about organizational quality directly through observation of an organization’s performance or use of its goods and services (Rhee & Valdez, 2009), or indirectly through statements from or communication with other parties that have interacted with the organization (Rindova et al., 2005), these evaluations are often imperfect or incomplete since external observers cannot directly observe the underlying, internal organizational routines and practices that generated these external performances. Accordingly, organizations that gain prominent or respected third-party certifications can reduce this uncertainty by using these labels to signal their commitment to specific practices or standards that are valued by potential exchange partners.
Evidence clearly suggests the importance of these credentials to exchange partners within institutional channels, such as among competitors or with suppliers and distributors (Sine et al., 2007; Zuckerman, 1999), as well as outside of these institutional channels, such as with consumers or other end users (Harbaugh et al., 2011). Indeed, large institutional exchange partners may be expected by third parties, such as owners or stockholders, to primarily associate with well-established, accredited organizations. Thus, accreditation is known to provide tangible organizational benefits through this channel (Montiel et al., 2012; Sine et al., 2007). However, consumers or other large and diffuse groups of end users often lack this external pressure to associate singularly with accredited organizations; furthermore, some research suggests that they may face greater uncertainty when evaluating these accreditations and their relationship with organizational quality (e.g., Harbaugh et al., 2011). For these reasons, these external audiences, in particular, are sensitive to the information that particular accreditations provide about organizations with these designations.
Much prior work in this domain has found that the direct effect of accreditation on organizational performance is generally positive, meaning that being accredited leads to an increase in organizational performance (Graffin & Ward, 2010; Polidoro, 2013; Rao, 1994). However, despite compelling arguments regarding the benefits of organizational accreditation, the predicted relationship between accreditation and performance is likely far from universal. In particular, when certain events or new information tarnishes the perceived value of those accreditations, external audiences may be less inclined to view organizational accreditation as a positive attribute. This decouples the relationship between accreditation and organizational performance, as audiences may even withdraw support or resources from some accredited organizations. Below, I develop theory regarding this evaluative process, and I forward hypotheses regarding how several related factors may moderate the direct relationship between accreditation and organizational performance.
The Signaling Quality of Third-Party Accreditations
While external parties, such as customers, end users, and other transaction partners, can use accreditations to infer the quality of particular organizations, the value of those accreditations—and, therefore, their ultimate impact on organizations—may change through this process. Specifically, external parties that believe a specific accreditation does not accurately reflect organizational quality are less likely to use that accreditation to inform their behaviors, and the signal value of becoming accredited, along with its benefit to organizational performance (as predicted above), is likely to be diminished. Three processes, in particular, could lead to this outcome.
First, unaccredited organizations that pursue and successfully obtain new accreditation shortly after quality problems have occurred may experience diminished benefits to that new accreditation, as external observers infer that the accreditation itself is a less reliable predictor of the organization’s potential future performance. Second, external observers might discount commonplace accreditations as fairly nondistinctive, and previously unaccredited organizations that subsequently obtain those accreditations may experience weaker benefits as a result. Finally, newly accredited organizations may suffer following prior wrongdoings by other accredited firms. While the last process is similar to arguments in the research on categorical spillover, as negative perceptions are transferring across organizations within a particular category (e.g., Hudson, 2008; Piazza & Perretti, 2015), it is important to note that the effect theorized here is sequential in nature. This means that the judgments may arise immediately following wrongdoing at accredited firms but are retained and subsequently projected onto organizations that obtain the accreditation in the future. Consequently, in contrast to arguments regarding categorical spillover, changes in the accreditation’s value serve as a repository for this effect to persist over time and affect organizations that obtain accreditation after wrongdoing has occurred. Each of these three theoretical processes is discussed in greater detail below.
Quality patching
As described above, accreditations serve to assure external parties that particular expectations about the organization, such as the quality of its goods and services or its orientation toward social issues, are less likely to be violated than at unaccredited organizations (Graffin & Ward, 2010; Rao, 1994). Organizations that pursue accreditation shortly after these expectations are violated, however, risk the possibility that the move could backfire, as external observers may infer that such pursuits merely represent an instrumental or superficial attempt to patch the organization’s problems or repair its image following the quality lapse (Elsbach, 2003; Suchman, 1995).
Crucially, though, any events or occurrences that serve to violate expectations regarding the quality of an organization’s goods or services must be visible to relevant external parties outside of the organization. Any problems that are known about only within the organization, despite their potential importance, would fail to engender changes in how external observers perceive the value or meaningfulness of the organization’s accreditation. Research in this area supports the notion that either event frequency or magnitude may each affect external visibility (Haunschild & Sullivan, 2002; Homsma, Van Dyck, De Gilder, Koopman, & Elfring, 2009; Madsen & Desai, 2010). Specifically, when few problems with an organization’s products or services exist, or when problems are relatively minor, few external observers are likely to notice or pay attention to these issues. However, when the volume or severity of these problems increase, they become much more likely to garner external attention (Hoffman & Ocasio, 2001).
Accordingly, when a few quality problems have occurred or when quality problems are relatively minor, observers may ignore or fail to notice the events, presume that they are not an accurate reflection of the organization’s underlying quality, or assume that the problems were minor and their causes have been corrected. However, an increase in the magnitude or frequency of these events raises their salience, attracts greater external attention, and suggests that the underlying organizational problems may be more deeply rooted and difficult to correct (March, Sproull, & Tamuz, 1991; Ramanujam & Goodman, 2003). In these cases, unaccredited organizations that pursue a new accreditation may appear motivated by the desire to manage their external image or may seem to be using the signal instrumentally in order to artificially improve their legitimacy, especially given that the underlying problems are presumed to be relatively enduring (Elsbach, 2003). In these cases, the value of the accreditation to the organization is likely to be diminished; since organizations in this situation successfully become accredited following recent quality problems, external observers likely infer that the accreditation itself will be a less reliable indicator of high quality in the future as well. Collectively, this reduces the signal quality of accreditation and diminishes its benefits to the organization. Therefore, I predict that greater quality problems (referring specifically to increases either in frequency or magnitude) at the focal organization will reduce (i.e., negatively moderate) the direct relationship between new accreditation and organizational performance.
Hypothesis 1: Quality problems negatively moderate the direct positive relationship between new accreditation and performance, such that new accreditation leads to a lower increase in performance at organizations with greater quality problems than at organizations with lesser quality problems.
Legitimacy dilution
One of the crucial attributes of certifications and accreditations, and of signals more generally, is that external observers believe (whether accurate or not) that the designations help to distinguish organizations that are likely to meet expectations from those that are not (King et al., 2005; Polidoro, 2013; Rao, 1994). When relatively few organizations within a domain receive these designations, external observers are likely to presume that third-party accrediting agencies use fairly stringent and rigorous standards to evaluate organizations and that new accreditation is awarded only to the select few organizations that meet relatively high expectations (Rao, 1994). However, as more and more organizations receive accreditation, external observers may relax these assumptions. Specifically, when customers, suppliers, or other outside parties survey the organizational field and notice that many of the organizations that they could interact with have a particular designation, the designation itself becomes less useful as a tool to distinguish between organizations, and its meaningfulness as a signal of organizational quality within the field is accordingly diminished.
It is important to briefly consider an alternative possibility, that having more accredited organizations throughout the field will raise the visibility and perceived value of new accreditation rather than dilute its impact. Indeed, some research in this area may suggest that having more accredited organizations within a field will increase the visibility of that designation and lead observers to notice it more reliably (Hoffman & Ocasio, 2001; Ocasio, 1997). Yet, in relatively established or mature industries, this is an unlikely possibility since accreditation agencies and standards may already be fairly visible or connote value even when few organizations are accredited. In addition, even if the designation certainly becomes more salient as more firms become accredited, its perceived relationship with organizational quality does not necessarily improve. Accreditations, certifications, and other designations that are intended to serve as quality symbols tend to gain legitimacy and connote value through their limited and discretionary use (Polidoro, 2013), in contrast with other institutional symbols or artifacts that may benefit through prevalence or ubiquity (Tolbert & Zucker, 1983). Therefore, an increase in accreditations throughout the field will likely dilute the legitimacy of that particular designation, reduce its signal quality, and diminish its benefit to organizational performance. Accordingly, I predict that the number of other organizations with a particular accreditation will reduce, or negatively moderate, the direct relationship between becoming newly accredited and organizational performance at a focal organization.
Hypothesis 2: The number of other organizations with accreditation will negatively moderate the direct positive relationship between new accreditation and performance, such that new accreditation leads to a lower increase in performance when many other organizations have the accreditation than when few other organizations have the accreditation.
Stigma transfer
Hudson (2008) raises the possibility that discrete problematic events or episodes can generate negative judgments about an organization or its actions. Organizations can typically recover from these “event stigmas,” in contrast to other more stable forms of stigma that may arise due to an organization’s core attributes (Hudson, 2008: 253). Nonetheless, considerable research recognizes that the negative judgments that arise from these events may transfer across organizations following these problematic events (Hudson, 2008; Jonsson, Greve, & Fujiwara-Greve, 2009; Yu, Sengul, & Lester, 2008). This occurs when external audiences generalize from an affected organization to other organizations with similar structures, practices, or other attributes, using these generalizations to infer the likelihood that the other organizations may create or experience similar events (Jonsson et al., 2009; Yu et al., 2008). For instance, following wrongdoing or negative performance at an accredited organization, external observers may infer that other accredited organizations are likely to suffer similar fates. For brevity, I refer to the spillover of negative judgments under these event-driven circumstances as “stigma transfer.”
These negative judgments may transfer to newly accredited organizations following negative events at other accredited organizations. Following these events, external observers may infer that the accreditation itself has lost signal quality, and they may retain that judgment in connection with the accreditation itself, applying it to previously unaccredited organizations that subsequently pursue and receive the new designation. This is a sequential process; judgments do not spill over immediately across organizations within a particular accreditation category; rather, the accreditation itself serves as a repository, over time, of judgments regarding the likely performance of organizations that may obtain the designation in the future (Rao, 1994).
Consequently, when a quality problem arises at an accredited organization, the event violates observers’ assumptions that the event should not have occurred given the organization’s accreditation status (Rhee & Haunschild, 2006). While occasional problems may be missed, an increase in the frequency or magnitude of quality problems at accredited organizations makes the issue even more salient and difficult to ignore. Given that external audiences use accreditations as signals to infer organizational quality, as described above, poor quality at accredited organizations likely tarnishes the accreditation and diminishes its signal value. Simultaneously, as noted by research on event stigmas (Durand & Vergne, 2015; Gephart, 1993; Hudson, 2008), this situation also gives rise to negative external judgments about an organization. Given that the perceived relationship between the organization’s quality and its accreditation status has been challenged (since the accreditation was previously presumed to reflect its quality), these negative judgments likely transfer readily to other organizations that newly obtain the same accreditation status in the future, even if they have not directly experienced quality problems themselves (Harbaugh et al., 2011; Yeung et al., 2011). Therefore, organizations that newly obtain a particular accreditation may experience a penalty when quality problems have already occurred at many other organizations with the same accreditation status, and the benefit of new accreditation to the focal organization’s performance will likely be diminished. Accordingly, I predict that the number of quality problems at other accredited organizations will reduce, or negatively moderate, the direct relationship between new accreditation and performance at a focal organization.
Hypothesis 3: The number of quality problems at other accredited organizations will negatively moderate the direct positive relationship between new accreditation and performance, such that new accreditation leads to a lower increase in performance when many quality problems arise at other accredited organizations than when few quality problems arise at other accredited organizations.
Methods
Setting and Data
These hypotheses are tested on a panel of HHAs operating in the state of California from 2004 through 2013. Data were collected through California’s Office of Statewide Health Planning and Development (OSHPD). Analyses are conducted at the HHA-year (i.e., organization-year) level, and the study sample contains a total of 8,472 observations spread across an average of 847 organizations per year. Out of this group, 386 organizations became newly accredited (i.e., had a value of one on the newly accredited variable, described further below) at some point during the study period.
HHAs are organizations that provide or contract to perform health care services for elderly, disabled, or other chronically ill populations, typically within patients’ homes and residences. Given a significant rise in this demographic population, as well as the relative cost-effectiveness of home health services compared to inpatient hospitalizations, HHAs represent an integral component of health care delivery systems, and their use has been steadily increasing (U.S. General Accounting Office, 1997, 2004).
HHA quality is difficult for consumers to discern, and the industry is wrought with quality problems and other lapses. Under some conditions, no prior health care knowledge or experience is required to establish or own an HHA. In some anecdotal cases, pawn shop owners and taxicab drivers have been allowed to open HHAs and bill the federal government for rendered services (U.S. General Accounting Office, 1997). Although these and other similar cases may not necessarily lead to substandard care since HHA owners can contract with other health care providers to perform their services, they are indicative of broader, more systemic, and well-recognized quality problems within the industry, since federal standards for quality of care and other organizational processes are often poorly enforced in this setting (U.S. General Accounting Office, 1997, 2002, 2004).
More generally, any particular HHA’s underlying quality is difficult to directly ascertain, partly because reliable information about HHA performance is scant and also partly due to the fact that HHAs typically serve marginalized or elderly, homebound populations with limited access to information about care alternatives or quality differences among various HHAs in their local marketplace (U.S. General Accounting Office, 1997). Given these challenges, HHAs can obtain third-party quality accreditations through organizations such as the Joint Commission (JCAHO), the Community Health Accreditation Program (CHAP), the Accreditation Commission for Health Care (ACHC), or other third-party agencies (U.S. General Accounting Office, 1997, 2002). Once obtained, accredited HHAs often display these designations visibly on their websites and through other marketing materials since their accredited status distinguishes them within the marketplace. As a few examples, accreditations from JCAHO are visibly displayed on the webpages for some agencies (http://www.salushomecare.com/orange-county/, accessed on June 5, 2016), as are accreditations from ACHC (https://www.maximhomecare.com/achc/, accessed on June 5, 2016). Interestingly, accreditation serves as such a prominent visible signal in this setting that one agency, accredited through CHAP as well as other smaller accrediting bodies, has chosen to use the term accredited directly within its corporate name (https://accreditednursing.com/, accessed on June 5, 2016).
These accreditations are voluntary and require that the certified HHA meet quality standards that are typically more stringent than those established by the federal government; in fact, HHAs with certain types of accreditation status are exempt from federal monitoring and enforcement, as the accrediting agency’s standards and oversight are typically thought to be sufficient (U.S. General Accounting Office, 1997). Yet, even in these cases, HHAs with accreditation may underperform, which in extreme cases could lead to loss of accreditation status, loss of access to Medicare reimbursement, or other significant business challenges (U.S. General Accounting Office, 2002, 2004). Therefore, this is an appropriate setting in which to examine accreditation, its impact on organizational performance, and how this relationship may be influenced by quality patching, legitimacy dilution, and stigma transfer. The specific variables used by this study are described below.
Measures
Patient referral percentage
Each of the study’s hypotheses examines the relationship between predictors and organizational performance outcomes. Organizational performance is difficult to study in health care settings and particularly in the HHA context. Typical measures of performance, such as financial performance and organizational survival, are valuable but coarse indicators since different facilities may be compensated or reimbursed at very different rates for the same procedures based on whether they treat patients with private insurance, those who self-pay, or those who are insured through Medicare (and in the case of California, those insured through Medi-Cal, an additional state-run insurance program).
While financial measures are certainly useful if these and other caveats can be addressed, a more direct metric is available in this setting. Notably, accreditations and certifications provide information to the market regarding the desirability of interacting with particular organizations (Graffin & Ward, 2010; Rao, 1994). Accreditation, in this context, is intended to induce external parties toward a particular HHA (U.S. General Accounting Office, 1997, 2004). This may occur directly, such as when potential patients research HHAs and choose one on their own, or it may occur indirectly, such as when family and friends refer a consumer to a particular HHA or when the patient is referred or transferred through institutional channels, such as by hospitals, physician referrals, or other HHAs. While each of these channels is essential to an agency’s admissions and viability, the present project focuses on noninstitutional referrals and admissions, such as when a patient directly selects a particular HHA or is referred to it by family and friends, rather than institutional referrals through health care channels.
This focus is beneficial in the present context. Although physicians and other health care providers may be fairly knowledgeable about HHA accreditations and their significance, hospitals and other institutional referral sources often have long-term agreements or other arrangements with specific HHAs, which limits their flexibility to refer patients across all agencies within their geographic area; indeed, some health care organizations own or operate particular HHAs, which further limits their referral flexibility (e.g., Publication of the OIG Compliance Program Guidance for Home Health Agencies, 1998). Conversely, accreditation status may be more informative to consumers within noninstitutional channels, since patients as well as their family and friends often have greater flexibility than institutional providers when selecting an HHA.
For these reasons, an increase in an HHA’s admissions through self-referral or referral by family or friends, when other relevant factors are controlled, may signal that agency’s increased attractiveness to the market, and the agency’s accreditation status is certainly one notable factor in this consumer decision-making process. Conversely, when these external parties believe the value of an organization’s accreditation has been diminished, a drop in admissions from these sources would provide a sensitive indicator of the organization’s more limited desirability. Therefore, I estimate performance outcomes through the percentage of an HHA’s patients who are referred to the HHA through noninstitutional channels, such as by family, friends, or self-referrals (i.e., by patients themselves). While many HHAs have established relationships with institutional providers, such as hospitals or nursing homes, and tend to receive most of their patients through those channels, HHAs may also receive a sizable number of patients through self-referrals or referrals by family or friends. Furthermore, as discussed above, this channel is likely much more sensitive to new information about accreditations and organizational quality. Thus, this focus was essential within the present context. This dependent variable was scaled by 100 to facilitate interpretation of the study’s results.
Newly accredited
Accreditation is measured through a dichotomous indicator that is set to 1 if the focal HHA has changed from being unaccredited (by any agency) to becoming newly accredited, within the year prior to the observation, by any one or more of the three main accrediting bodies within this industry (JCAHO, CHAP, or ACHC) and is set to 0 otherwise. Although this treatment absorbs an extra period of observations (accreditation status in the period t − 2 is used to determine whether an agency’s accreditation in the period t − 1 is new rather than ongoing), the approach is crucial to ensure that any variation in this variable reflects recent changes in accreditation status within agency rather than static differences in accreditation across agencies. This variable’s direct relationship with performance (patient referrals) is controlled in the analyses below, and the moderating influence of the following three variables on this direct relationship is respectively examined to test each of the study’s hypotheses.
Patients lacking medical progress
As with financial performance, organizational quality is also difficult to study in health care settings. In these settings, quality measures are often grouped into two categories. First, process-based measures of quality address whether health care providers have adequate policies and procedures in place to prevent or mitigate adverse patient outcomes (LaPar et al., 2012; State of California Office of Statewide Health Planning and Development, 2013). These metrics are useful indicators of an organization’s approach but may not necessarily reflect ultimate quality outcomes, because some facilities with adequate procedures may treat sicker patients than others or because the procedures themselves are implemented inconsistently (Jiang, Lockee, & Fraser, 2012; Tucker, Nembhard, & Edmondson, 2007). Therefore, a second category of quality measures examines ultimate patient outcomes, such as the prevalence of iatrogenic (i.e., health care–induced) errors or overall patient mortality rates (Birkmeyer et al., 2002; Birkmeyer, Stukel, Siewers, Goodney, Wennberg, & Lucas, 2003).
As objective indicators of organizational quality, patient outcomes are a very indirect proxy since they can reflect differences in patients’ underlying health conditions rather than differences in quality among facilities. For this reason, studies of health care quality that rely on patient indicators often attempt to control for underlying patient differences (Birkmeyer et al., 2003; LaPar et al., 2012; State of California Office of Statewide Health Planning and Development, 2013). Despite this weakness, patient quality measures provide one important set of metrics in this and other settings since they account for the ultimate outcomes of relevant organizational processes.
In this setting, patients who are discharged from HHAs because they lack medical progress (many of whom may be transferred to hospitals or other acute care settings for more intensive care), or patients who die while under the care of an HHA, provide visible and salient information to family, friends, and other external audiences. This information, along with other relevant quality indicators, are disseminated through websites such as Medicare’s Home Health Compare (www.medicare.gov/homehealthcompare) as well as through other state and federal communication efforts (such as, in the case of the California HHAs in this study, the efforts of the California HealthCare Foundation and its quality comparison website, http://www.calqualitycare.org). While some patient deaths may not objectively reflect inadequate treatment, a large volume of deaths or discharges due to lack of progress at a particular facility may be subjectively interpreted as a cause for concern or attributed (whether correctly or incorrectly) to the facility’s treatment approach (Birkmeyer et al., 2002, 2003; LaPar et al., 2012; Li, Carlisle, Young, & Amsterdam, 2008).
Therefore, I proxy for quality problems through the percentage of an agency’s patients who die or are discharged due to lack of progress during the year. This approach directly controls for the HHA’s operating scale, since larger agencies may naturally discharge more patients for these reasons. I also control for several patient characteristics in order to address underlying differences in patient populations among HHAs. These and other controls are described further below. The interaction between this measure of quality problems and the HHA’s accreditation status is used to test the relevant hypothesis about this moderating relationship. As with accreditation status, this measure of quality problems (as well as the other predictors described below) is measured in the period t − 1, prior to measurement of the study’s outcome variable.
Other agencies with accreditation
The number of other HHAs with accreditation is measured through a count of the number of other accredited HHAs within the state. Specifically, this refers to the number of other HHAs (not including the focal agency) that possess an active accreditation for all or any part of the year (again, this measure—along with other predictors—is lagged by one period). While the industry’s state-level regulator, OSHPD, consolidates and reports accreditation status and other information for HHAs across the state, preliminary tests of a more localized count measure (at the level of the local health service area, a geographic designation that reflects the distribution of health care resources around population centers) yielded similar results. This variable was scaled by hundreds (100s) to facilitate interpretation. The interaction between this variable and the HHA’s accreditation status is used to test the relevant moderating hypothesis.
Deaths at other agencies with accreditation
To measure the number of quality problems at other accredited organizations, I construct a count of the number of patient deaths (in hundreds) at other accredited HHAs throughout the state. In preliminary tests, this measure was constructed as a percentage (of patients served across the industry) rather than as a count. Although results were identical across these approaches, the percentage measure was highly correlated (r = −0.92) with the variable tracking other agencies with accreditation, and a simpler count version of this metric was employed in the final analyses in order to alleviate this source of collinearity. Importantly, the patients lacking medical progress variable, described above, includes patient deaths as well as discharges of patients who lack medical progress, since both outcomes reflect agency quality. However, the current variable, which is used to test for stigma transfer across facilities, includes only patient deaths (and excludes discharges due to lack of progress) because agencies with a large volume of patient deaths may be much more visible across the field—and may receive greater attention and scrutiny from the media, regulators, and other parties—than agencies with a large volume of patients who lack medical progress. Nonetheless, preliminary tests that incorporated the latter cases into this variable yielded similar results, with no hypothesis tests affected. Again, the interaction between this variable and the HHA’s accreditation status is used to test the relevant moderating hypothesis.
Control variables
Industry characteristics and prior research suggest a number of relevant controls. First, I control for each HHA’s age, in years, to address the influence of age-related inertia on performance outcomes (Hannan & Freeman, 1984). I include a control for the number of patients served by the HHA during the year in order to address the effects of operating scale. Next, several controls are included to address differences between HHAs that may attract patients with more difficult conditions, as well as other underlying differences between patient populations across HHAs. Specifically, I include a variable that measures the percentage of an HHA’s patients who have been diagnosed with HIV, another variable for the percentage who have been diagnosed with Alzheimer’s disease, and a third variable for the percentage of patients above 90 years of age. Each of these factors has been identified as key characteristics associated with overall patient health quality within this particular patient population (U.S. General Accounting Office, 2002). I also include a dichotomous control that is set to 1 if the HHA’s chief administrator left or was replaced during the year, since administrator turnover may independently affect performance outcomes (Eldenburg, Hermalin, Weisbach, & Wosinska, 2004).
Next, several additional variables were necessary to independently control for differences across organizations that could independently affect accreditation, quality, and other constructs outside of the study’s hypothesized relationships. First, a dichotomous variable is included to track whether the focal HHA is a sole agency, that is, an independent outlet without any additional branches. Sole agencies within this industry are typically smaller and subject to less external oversight or scrutiny; thus, less information about organizational quality is available externally. This may independently affect their likelihood of accreditation as well as the relationships among patient referrals and each of the study’s predictors. Relatedly, I also include a dichotomous indicator that is set to 1 if the focal HHA is owned by a local (i.e., within-state) parent organization, since these arrangements allow for closer scrutiny over organizational quality and performance outcomes.
Next, I include several geographic controls that are closely correlated with HHA quality in this context (U.S. General Accounting Office, 1997, 2002). A dichotomous indicator measures whether the agency is located in a rural area. Specifically, this variable is set to 1 when the agency’s local medical service study area, or MSSA (a geographic unit of analysis used within the state for health care policy and assessment), has a population density of fewer than 250 persons per square mile. This characteristic is known to influence health care availability and outcomes within the home health context (U.S. General Accounting Office, 2002). Similarly, I also include a dichotomous control that is set to 1 if the state regulator has identified a documented shortage of primary care physicians or other essential health care personnel within the focal agency’s MSSA. In addition, I include a variable tracking the percentage of total population within agency’s local MSSA that live below the federal poverty level, since this geographic characteristic is also associated with lower health care access and poorer outcomes within this context.
I also include additional controls for relevant organizational attributes. First, I include a variable that is set to 1 if the focal HHA has a pharmacist on staff. Although rare, agencies with staff pharmacists generally provide more advanced care to the elderly populations typically served in the home health context. These patient populations often take a broad range of medications and are therefore at a high risk for adverse drug interactions or other pharmacological problems. At the same time, given their limited mobility or other impairments, many HHA patients are often unable to access pharmacists or seek similar guidance outside of the home. Thus, HHAs with pharmacists on staff may be able to more effectively monitor drug interactions or provide other patient care advantages, and they may receive more patient referrals as a result of their quality-oriented advantages. Second, I also include a categorical control for the HHA’s ownership structure (for-profit corporation, for-profit partnership, nonprofit, or government owned) since this characteristic is also known to be associated with organizational quality and performance in this and other health care contexts (U.S. General Accounting Office, 1997, 2002).
Finally, I control for time period by including fixed effects for the observation year, to address the influence of factors that change over time across the industry. All controls and predictor variables were lagged by 1 year to reduce the possibility of reverse causality.
Analysis
I estimate models on the pooled data set with an observation for each HHA in each year it operated between 2004 and 2013 (with observations from 2004 used to calculate lagged variables for the initial period). I use organization fixed effects to control for stable differences across panel members over time. In addition, using ordinary least squares regression (OLS) to conduct estimations with panel data may yield biased estimates since repeated observations for the same panel members are pooled over time (Baltagi & Wu, 1999). In the present case, Wooldridge tests indicated the presence of autocorrelation in the error residuals from each estimated model (Drukker, 2003; Wooldridge, 2002). For this reason, I use fixed-effects linear regression (with AR[1] disturbances) to estimate the study’s models (using the xtregar command in Stata/SE v13). The first observation of each panel is automatically dropped by the estimator in order to condition out the fixed effects. Thus, the estimation sample size reported in Table 2 differs from the sample size reported in Table 1 (8,472 sample size − 1,707 groups = 6,765 estimation sample size).
Descriptive Statistics and Correlations
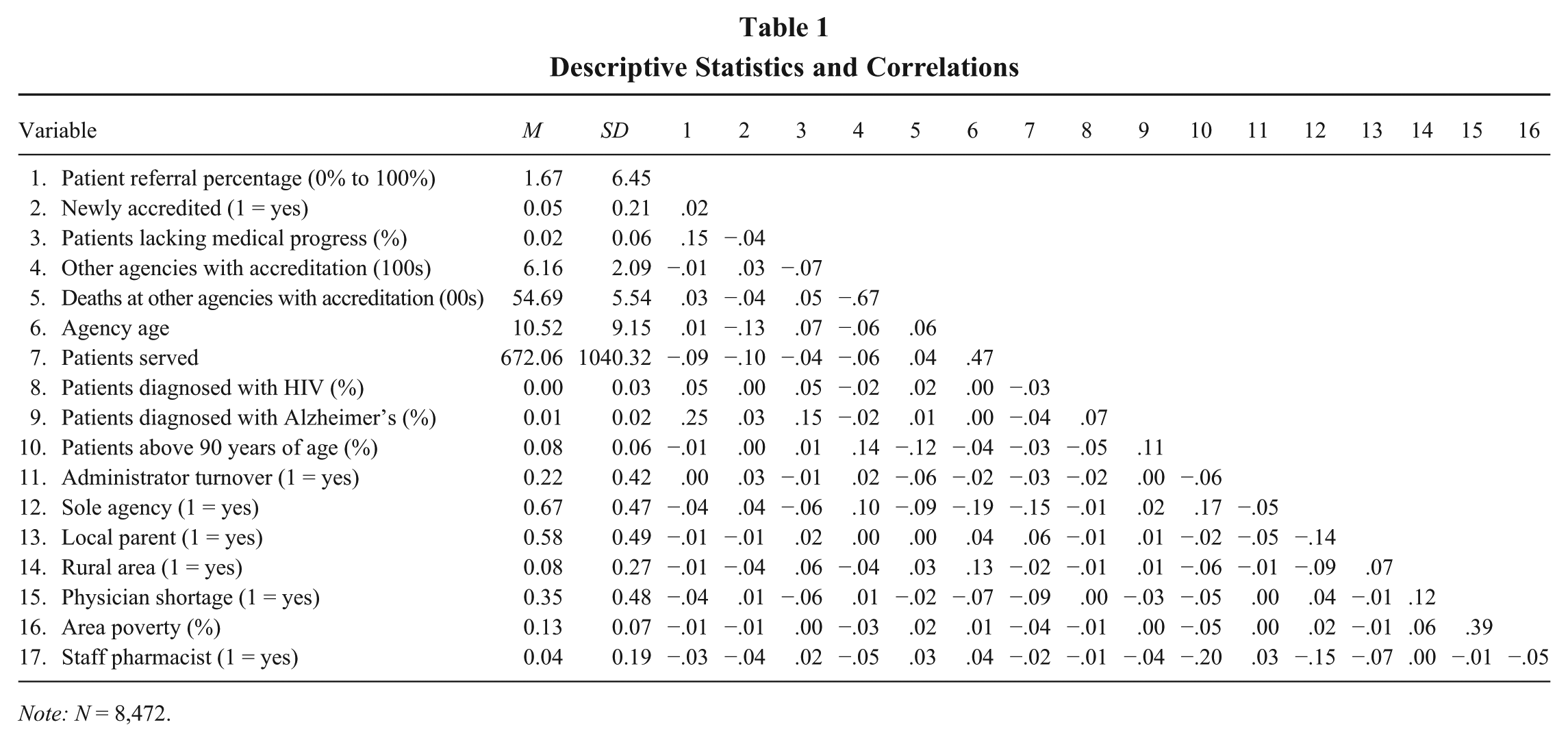
Note: N = 8,472.
Results
Table 1 presents descriptive statistics and correlations among the study’s variables. The variables for year and ownership structure were omitted from this display given that they are categorical in nature. Nonetheless, it is important to note that high correlations existed among the categorical year control (if treated continuously) and the variables respectively measuring other agencies with accreditation and deaths at other accredited agencies. In the final analyses, year is included as a categorical rather than continuous control, which reduces the direct overlap among these predictors. Nonetheless, the issue was more directly examined by omitting the year control entirely from preliminary regressions that otherwise replicated each of the study’s analyses. The results of each hypothesis test were unchanged in each case, suggesting that inclusion or exclusion of the year control does not affect tests of the study’s hypotheses. Final models continue to include year effects given the necessity to control for systematic changes affecting firms across this industry over time.
A moderate negative correlation exists between the measure of other agencies with accreditation and the measure of deaths at other accredited agencies (r = −0.67). Although these variables reflect distinct theoretical constructs, the correlation perhaps reflects the possibility that an increase in the number of accredited HHAs throughout the field could have led to more substantial oversight and external visibility that, in turn, suppressed quality problems. Alternatively, the overlap could signify patient sorting within the industry, to the extent that less sick patients may have tended to select accredited agencies given their greater visibility and prevalence. Regardless of the reason, the correlation could make the variables’ respective effects difficult to distinguish. For that reason, hypothesis tests are interpreted across models that do not simultaneously include both of these variables and their respective interactions. However, crucially, a nested model including both of the variables and their interactions is also presented, and results in that model are similar.
Table 2 presents models estimating the HHA patient referral percentage. Model 1 includes only controls. Model 2 introduces the main effect of new accreditation. Although the coefficient estimate of this variable is positive, it is not significant in this and several later models. However, the coefficient estimate becomes significant and positive in Model 6 (and again in the final model) upon inclusion of the interaction with others with accreditation.
Fixed-Effects Linear Regression Models (With AR[1] Disturbances) of Patient Referral Percentage

Note: N = 6,765; standard errors in parentheses. For-profit corporate is used as the omitted category from the categorical ownership variable.
p < .05.
p < .01.
p < .001.
Importantly, the lack of strong significance on the newly accredited variable across many models may be surprising given the support for a positive relationship between accreditation and performance in this literature (as reviewed above). However, this pattern of results is still consistent with general evidence in this literature for several reasons. First, the current study theorizes and estimates the effect of new accreditation, rather than an organization’s overall accreditation status, since the newly accredited variable equals 1 only in cases where the organization has obtained a new accreditation within the past year. This is a relatively rare event; furthermore, it may take time for the effects of accreditation to materialize, meaning that this variable’s effect on performance may naturally be weaker than the effect of an organization’s overall accreditation status. Second, and more fundamentally, the pattern of results across models indicate that the coefficient estimate of this newly accredited variable is positive and significant when the interaction with others with accreditation is also included. This effectively indicates that the direct effect of new accreditation on performance is predicted to be positive when few other HHAs are accredited but that the effect of new accreditation becomes less positive (and ultimately turns negative, as seen in the relevant figure below) during periods when more other agencies become accredited.
Collectively, this suggests that the direct effect of new accreditation (on performance) across other models may be confounded, as the positive effect of accreditation when few other agencies are accredited may be washed out by the negative effect when many other agencies are accredited. This could lead to the lack of significance for the newly accredited variable’s coefficient across other models.
Model 3 in Table 2 includes the main effect of patients lacking medical progress, and Model 4 adds its interaction with the newly accredited variable. The interaction term’s coefficient estimate is negative and significant. Despite the lack of significance for the main effect of newly accredited in this model, this negative coefficient on the interaction term provides support for Hypothesis 1 (also see the discussion below regarding findings in the study’s full model, where the coefficient estimate for newly accredited is positive and significant). Model 5 removes these variables and instead introduces the main effect of others with accreditation, and Model 6 includes its interaction. That interaction estimate is also negative and significant, providing support for Hypothesis 2. Model 7 removes these and includes the main effect of deaths at others with accreditation, and Model 8 introduces its interaction with the accreditation variable. The latter interaction term is not significant, despite the prediction in Hypothesis 3. Thus, Hypothesis 3 is not supported through this analysis.
In the study’s final model (Model 9), which includes all prior variables and their respective interactions, the effect of new accreditation when all other moderators are held at zero is positive and significant (as seen through the coefficient estimate for the newly accredited variable in this model). However, the negative and significant estimate on the interaction with patients lacking medical progress suggests that as a greater percentage of an agency’s patients lack medical progress, the effect of new accreditation on performance becomes less positive (and indeed ultimately turns negative, as shown by Figure 1). Similarly, the estimate for the interaction with others with accreditation is also negative and significant in this model, suggesting that the effect of new accreditation becomes less positive (and also ultimately turns negative, as shown by Figure 2) as more other agencies become accredited. However, again, the interaction with deaths at others with accreditation is not significant in this model. In each case, the pattern of results in the final model is consistent with findings from the study’s earlier models.

Moderation of Patients Lacking Progress on Effect of New Accreditation (Table 2, Model 4)

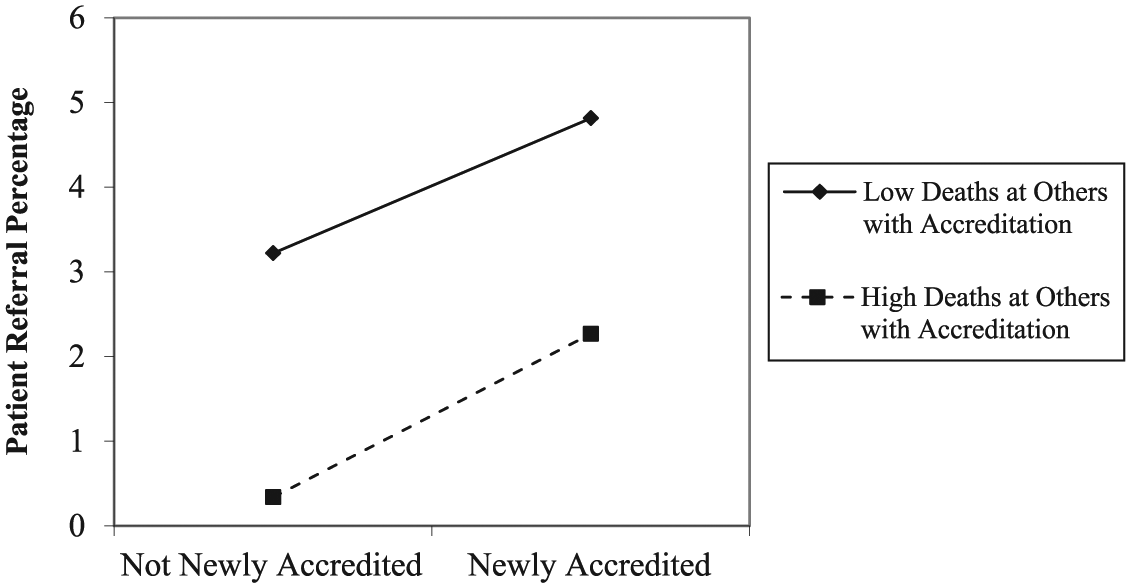
Moderation of Other Agencies With Accreditation on Effect of New Accreditation (Table 2, Model 6)
To aid in interpreting the study’s interaction effects, Figures 1 through 3 plot the respective interactions from the models in Table 2. Figure 1 plots the interaction between accreditation and patient deaths at the focal HHA. As seen in the figure, the relationship between accreditation and patient referrals becomes less positive (or more negative) as patient deaths increase (from one standard deviation below the mean to one standard deviation above it) at the focal HHA. Figure 2 plots the interaction with the number of other HHAs with accreditation, and the relationship between accreditation and referrals again becomes less positive (or more negative) as the moderator increases. Finally, Figure 3 plots the interaction with deaths at other accredited HHAs. Consistent with the results in Table 2, no moderating effect appears visible from this figure.
Moderation of Deaths at Other Agencies With Accreditation on Effect of New Accreditation (Table 2, Model 8)
Robustness Checks
Several robustness checks were warranted given various aspects of the manuscript’s empirical approach and findings. Some of these robustness checks, such as an effort to determine whether variables tracking the number of other accredited agencies as well as deaths at other accredited agencies should be accumulated across the state or on a more localized basis, were described above. However, other sets of supplemental analyses were also necessary and are discussed in more detail here.
First, the study’s primary analysis uses a measure of quality problems at the focal agency that is based on patient deaths as well as discharges due to lack of medical progress. In contrast, the measure of quality problems at other agencies is based only on patient deaths and does not include discharges due to lack of medical progress. This choice is driven by important considerations within the study’s empirical context. Specifically, information about recent patient deaths, as well as discharges due to lack of progress, can often be obtained through direct consultations with HHAs, as patients and their families may do prior to (or in the process of) selecting a particular agency. In contrast, when evaluating performance of the industry as a whole, patient deaths is a salient metric reported publicly through industry websites, but information about patients lacking medical progress elsewhere is much more difficult to ascertain without direct consultations with particular agencies (U.S. General Accounting Office, 1997, 2002). As a result, the latter information diffuses less readily across organizations and is therefore not included in the measure of problems at other agencies with accreditation. Nonetheless, a supplemental analysis was necessary in order to determine whether this empirical choice affected the study’s results. Accordingly, I replicated each of the study’s analyses using a measure of problems at other accredited agencies that not only included deaths elsewhere (as in the primary analyses) but also included patients lacking medical progress at these other agencies. Each of the models estimated through that approach yielded identical results to those in the primary analyses, with no hypothesis tests affected (as in the primary analysis, this specific measure’s interaction with the newly accredited variable was not significant). These models are not reported in this article in order to conserve space but are available upon request.
Second, it is also important to address one characteristic of the newly accredited variable. This variable is set to 1 during periods that an agency without accreditation receives new accreditation from any prominent accrediting body within the field. However, the variable is set to 0 for any number of reasons. For instance, an agency could operate without accreditation over the entire study window, and many agencies choose that approach given the high costs of accreditation and other considerations. Alternatively, though, an agency could receive a value of 0 on this variable because it was already newly accredited in a prior period or because it is constantly accredited over the entire study window. Effectively, the analyses compare the effects of new accreditation to those of multiple other accreditation statuses. This approach is necessary given the study’s empirical context, since agencies can (and some do) change accreditation status multiple times over the study period. Thus, for example, it would be less reasonable to exclude agencies from the analysis once they receive a new accreditation, since some of these agencies may subsequently drop the accreditation and later pursue another new accreditation from the same or an alternate accrediting agency. Comparably, agencies that are never accredited over the study window are still “at risk” of becoming accredited at any point; thus, excluding these agencies from the analyses would systematically limit the generalizability of the study’s findings.
However, one stricter test of the study’s analyses is certainly possible, and finding comparable results through this stricter test would enhance confidence in the study’s primary results. In particular, I conducted a supplemental analysis comparable to the study’s primary analyses except that this supplement excludes agencies that are always consistently accredited over the entire study period. While findings from this supplement certainly could not generalize to this subset of agencies, the approach is insightful because these agencies have the lowest likelihood of becoming newly accredited (since this would involve dropping an existing designation and waiting for at least a year before acquiring a new one). While this certainly occurs in practice, excluding these consistently accredited agencies from the analysis serves to test hypotheses only on agencies that are either newly accredited at any point or alternatively never accredited over the entire study window (thus, most closely “at risk” for becoming newly accredited).
Table 3 presents results of this supplemental analysis, which again is identical to the approach in the primary analyses except that the observations are restricted to exclude any agencies that are always accredited over the entire study window. To conserve space, Table 3 displays only models including interaction terms (Model 1 in Table 3 is comparable to Model 4 in Table 2, Model 2 is comparable to Model 6 in Table 2, and Models 3 and 4 are respectively comparable to Models 8 and 9 in Table 2). However, preliminary tests replicated all of the models in Table 2, with similar results in every case. As seen from the models in Table 3, findings are similar when excluding consistently accredited agencies, and no results of any hypothesis tests are affected. Collectively, the results of this supplemental analysis serve to provide greater confidence in the study’s primary results, suggesting that the primary results are not affected by the existence of consistently accredited agencies within this particular empirical context.
Fixed-Effects Linear Regression Models (With AR[1] Disturbances) of Patient Referral Percentage, Restricted to Agencies With Any Unaccredited Periods Within Observation Window

Note: N = 4,307; standard errors in parentheses. For-profit corporate is used as the omitted category from the categorical ownership variable.
p < .05.
p < .01.
p < .001.
Discussion
According to existing theory, third-party certifications can provide legitimacy or signal trustworthiness about an organization and its products or services, and consumers often rely heavily on these signals when more direct information is unavailable or unclear (Graffin & Ward, 2010; Rao, 1994; Sine et al., 2007). This study, however, suggests that the signals can become tarnished by negative information, such that accreditations obtained following quality problems may be less valuable, in terms of their impact on organizational performance, than accreditations obtained during other periods. In addition, the study provides evidence that the value of these accreditations is also diluted when more and more organizations pursue and obtain them (Harbaugh et al., 2011; Jonsson et al., 2009; Yu et al., 2008).
Despite the study’s findings regarding the effects of quality problems (at the focal organization) and accreditation frequencies (across other organizations) on the relationship between new accreditation and organizational performance, no support was found for stigma transfer through quality problems occurring at other accredited organizations. This is perhaps surprising, given some prior evidence of transfer through category affiliations in the literature (Jonsson et al., 2009; Yu et al., 2008). One reason that the present study may have been unable to detect this relationship could be that this study focuses on newly obtained accreditations. It is possible that stigma transfer occurs through categories that have been established for quite some time, such as through organizations that have been accredited on an ongoing basis, because such time allows consumers and other exchange partners to become familiar with the relevant organization’s membership within a particular category. This suggests the importance of future research that examines the time period over which an organization has maintained accreditation, both to determine whether the present study’s relationships are robust and, more importantly, to extend theory regarding the effects of category affiliation over time.
More generally, there may be several other reasons that the study was unable to detect a relationship in the case of stigma transfer. For instance, accreditations simply may not be a strong enough pathway or mechanism for the interorganizational diffusion of negative judgments following quality problems in this study’s setting, especially among audiences such as patients and families, who may fail to make strong interorganizational associations based on this category affiliation. This possibility suggests the importance of replicating the study in other contexts, where such category membership may be more salient across organizations. Collectively, such efforts could ultimately strengthen the suggestion that accreditations, certifications, and other third-party designations may serve as an additional pathway of interorganizational influence outside of more commonly studied channels, such as board interlocks and direct relationships between organizations (e.g., Davis, 1991; Haunschild & Beckman, 1998). This is important to work on interorganizational diffusion, given the possibility that resources, reputation, and even certain practices or innovations might flow between organizations not only based on their tangible relationships but also based on their orientation toward—and status with—prominent third-party agencies. For instance, future research could address questions such as whether and how particular practices or activities might spread through the connections that organizations have with these third-party agencies or within peer groups consisting of other organizations with the same accreditation status (Porac, Thomas, & Baden-Fuller, 2011).
In addition, the study’s findings also forward other implications for research on third-party certification (Barnett & King, 2008; Graffin & Ward, 2010; Rao, 1994) and for the literatures on organizational legitimacy and reputation (Elsbach, 2003; Polidoro, 2013; Rhee & Valdez, 2009; Suchman, 1995). For instance, the study suggests that third-party designations may not necessarily have a uniformly positive impact on organizations (Polidoro, 2013; Rao, 1994). Rather, these designations may reflect, and perhaps even reinforce, prior organizational events as well as external observers’ own perceptions and interpretations. Therefore, while they may confer greater legitimacy under some conditions, third-party certifications may at other times diminish an organization’s reputation or legitimacy (Elsbach, 2003; Hudson, 2008) and make it more difficult for organizations to recover from negative events (Rhee & Haunschild, 2006; Rhee & Valdez, 2009). Paradoxically, the very same third-party accreditations that managers might pursue in order to distance their organizations from a crisis may instead more directly associate them with it (Elsbach, 2003; Rhee & Haunschild, 2006; Suchman, 1995).
From a practical standpoint, the study’s findings suggest that organizations that newly obtain an accreditation following local quality problems, or during periods when that particular accreditation is extremely widespread, may benefit less through those accreditations than organizations that obtain those designations at other times. Nonetheless, there may be situations in which organizations must pursue those designations regardless of these challenges, such as when particular accreditations are increasingly expected or required of organizations doing business in a particular setting (Graffin & Ward, 2010; Polidoro, 2013). In these cases, organizations may benefit from distinguishing themselves positively from competitors in other ways as well (when legitimacy dilution occurs), such as through marketing campaigns or otherwise taking steps to communicate their genuine adherence to the desirable qualities represented through the accreditation (when quality patching is suspected).
Aside from its theoretical implications, this study contains a number of limitations that serve as opportunities for further research. As described above, assessing organizational quality and other performance measures is difficult in this study’s empirical setting. As one example, the measure of deaths at other accredited agencies was correlated with the variable tracking the number of other agencies with accreditation, and a percentage-based version of the former measure (constructed in a preliminary analysis, as reported above) was very highly correlated with the latter variable. This relationship can make the respective variables’ effects difficult to distinguish within this setting. In addition, although care was taken to control for a number of characteristics of HHAs and their patient populations, the chance that some other unaccounted factor might bias the study’s results certainly remains a possibility. Future research that replicates these analyses in other settings with more precise controls, and where industry-level quality is less correlated with other measures, certainly seems warranted.
Second, replication would also be advisable to determine whether the study’s findings generalize to other settings outside of the health care context. While health care, and home health in particular, represents an appropriate setting in which to examine the accreditation process and its implications, this is also a highly institutionalized context that is characterized by regulation through multiple agencies at the state and federal levels, stringent control and governance over key processes, and several other significant differences from nonhealth industries. Third-party accreditations and certifications are used in a wide variety of domains outside of health care, and replication of this study’s analyses in some of these other settings would certainly help to enhance the validity and generalizability of its findings (e.g., Graffin & Ward, 2010; Sine et al., 2007; Waguespack & Sorenson, 2011). As one example of the benefits to be gained, the current study examined one particular performance metric (patient referrals through self, family, or friends) that is salient only within this particular setting. Furthermore, even despite the importance of this metric within the setting, most patient referrals to HHAs tend to come through institutional channels, such as hospitals and nursing homes. Replicating the study in other contexts, and with a broader class of performance measures, would help to provide confidence in the study’s results.
In addition, generalizability of the study’s findings is also limited by an important theoretical boundary condition. The study’s theoretical arguments apply most directly to organizations that transition from being unaccredited to becoming newly accredited, since this status change conveys the most direct signal to the marketplace regarding a change in perceived organizational quality. Subsequent accreditations, at organizations that are already accredited by one agency but then receive additional accreditations from alternate agencies, likely convey marginally weaker signals given that they may reinforce but do not necessarily alter external perceptions about the organization. While the study’s theoretical arguments and empirical analyses focus on organizations that transition from an unaccredited to a newly accredited status, open questions involve whether and how processes such as quality patching, legitimacy dilution, and stigma transfer might affect organizations that receive new accreditations from multiple accrediting bodies, as well as how these organizations might compare with organizations that are newly accredited only by one particular accrediting body. In addition, future research would be wise to explore whether stigma might transfer across accreditations from different accrediting bodies or if this transfer is specific only to a particular type of accreditation.
Finally, this study raises a number of additional possibilities for future research, beyond those described above in connection with the study’s implications and limitations. For example, some research could examine whether third-party certifications intensify reputational differences among organizations, perhaps by improving the reputation of strong performers while disproportionately penalizing weak performers (Rhee & Haunschild, 2006). Alternatively, studies could determine whether certifications instead level the playing field, such as by facilitating the transfer of positive as well as negative goodwill among organizations. Research on these and other similar topics would broaden our understanding of how organizations obtain and manage their legitimacy and reputation, as well as how organizational crises influence this process (Elsbach, 2003; Montiel et al., 2012; Suchman, 1995).
In conclusion, this study tests whether an organization’s pursuit of third-party certification, often presumed to be a strong signal of quality, can become a liability through the organization’s own actions or through related events elsewhere in the field. Findings suggest that this may occur when relevant quality problems arise or when many other organizations already have accreditation status. This leads to the paradox that while third-party accreditations may appear attractive after a crisis or when they are quite common, they may actually reinforce effects of the crisis or otherwise be less beneficial than expected for the focal organization. Future research would be wise to examine this process in other settings and extend the theory to consider additional implications for organizational legitimacy and reputation.
Footnotes
Acknowledgements
This article was accepted under the editorship of Patrick M. Wright. I am grateful for feedback on earlier versions of this project from David Chandler, Peter Madsen, and participants at the 2015 annual conference on the Carnegie School of Organizational Learning. Jake Jabs Center for Entrepreneurship, University of Colorado, Denver, provided small research grant support to study author (Vinit Desai) for work on this project.