
Abstract
Maternal mortality in the United States of America is a human rights issue. This study gathered perspectives from Black women community members and from duty bearers in four fields (academic, special interest, government, and media) on barriers to maternal health in Indiana. Semi-structured interviews and an editing (data-based) analytic strategy revealed six themes regarding barriers to maternal health: lack of continuous, quality health care coverage; racism and implicit bias; trauma and lack of mental health services; lack of instrumental and emotional support systems; insufficient knowledge for self-advocacy; and lack of data transparency and reliability. Participants raised several strategies to address barriers, including continuous high-quality health care coverage, implicit bias training, mental health services, doulas, and grassroots-university partnerships. We discuss these barriers and solutions using a human rights-based approach to health (HRBA). These findings present a blueprint for duty bearers in Indiana to increase women’s ability to claim their right to health.
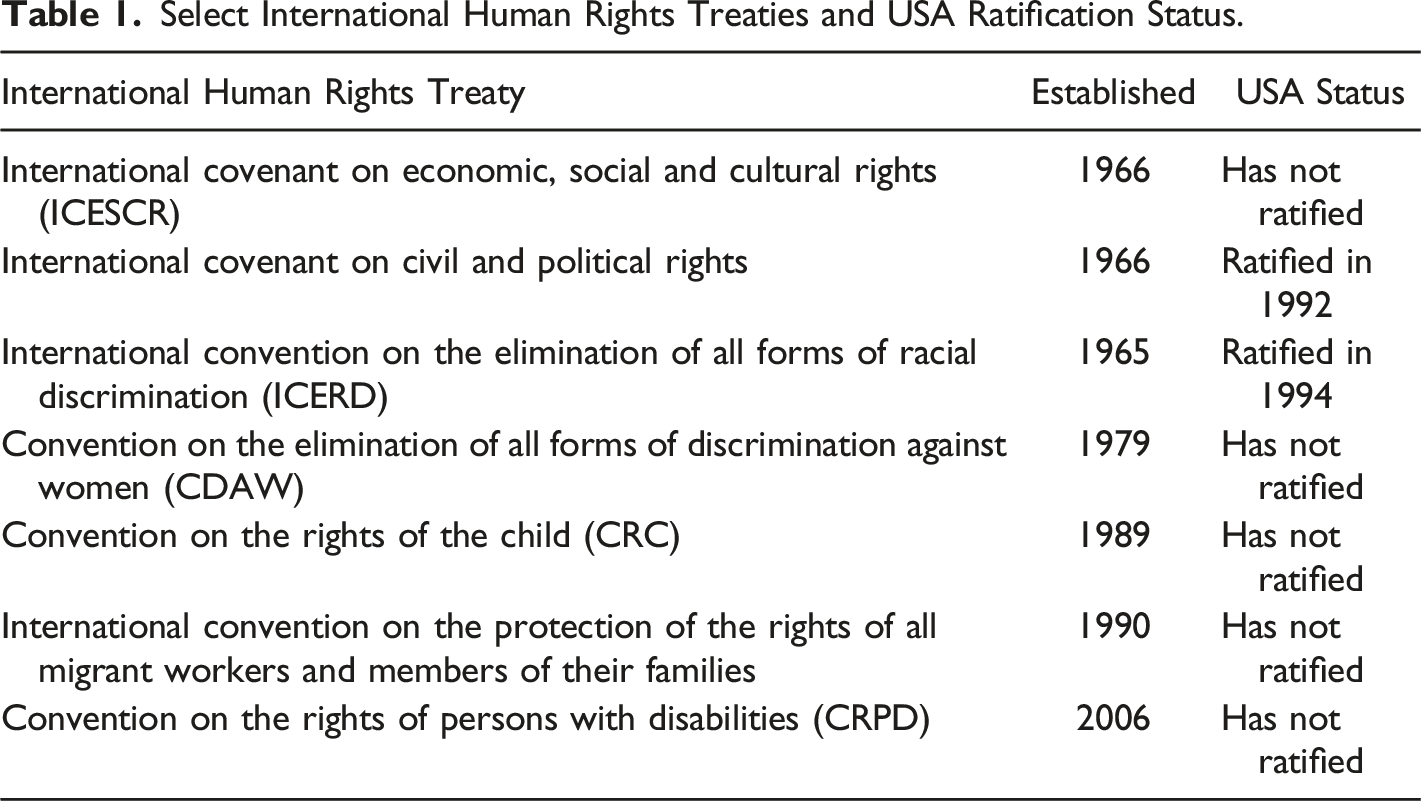
Personal Reflexive Statement
As a public health practitioner, I have seen the failings of our health systems firsthand and hoped to capture them in my research. As a White, middle-class, college-educated woman, my childbirth experiences were much different than the interviewed community members; I didn’t have to worry about how the healthcare system will perceive me based on the color of my skin. While I have always known that there are women who don’t have a support system, this research brought the realities home in a new way. During and after each pregnancy, I had family members and friends providing meals, house cleaning, and opportunities for respite. As I listened to the community members and the experiences that the participants reflected on, it gave me great pause. During one interview, I needed to take in the heaviness of the moment and utilize empathy and my professional experience and training in trauma-informed care to respond appropriately. Most concerning, perhaps, is that the United States has not signed and ratified all the UN conventions supporting human rights. Like so many things, women and children bear the burden of human right infractions and policy failures. However, the resiliency of the community women is inspiring and the consensus about what needs to change to improve the health and well-being of new mothers is heartening. My co-authors and I remain committed to transforming policy to support human rights.
Introduction
Despite being one of the wealthiest countries in the world, the United States of America (USA) has a Maternal Mortality Ratio (MMR) of 19 deaths per 100,000 live births and ranks 50th of all countries for maternal mortality (World Health Organization 2022). Pregnancy-related deaths have increased at such an alarming rate that researchers are classifying the increase as a human rights issue and are urging policymakers to place women’s health at the center of policy making (Duncan 2014; Small et al. 2017). Duty-bearers, or institutions that bear responsibility to “develop the capacity, the resources and the political will to fulfill their commitments to human rights” (United Nations Population Fund 2021:para. 10), can best promote public health by simultaneously advocating for the promotion of public health and protection of human rights (Georgetown Institute for Women, Peace, and Security 2020; Mann 2006). This study is grounded in a Human Rights Based Approach (HRBA), and recognizes that women’s health needs to be,“…understood and addressed within the economic, social and cultural context of individual women’s lives” (Gruskin et al. 2008:591). It explores the barriers to women, and especially Black women, claiming their rights to health and the barriers of duty-bearers in their efforts to develop the capacity, resources, and political will to make the claiming of these rights possible.
Select International Human Rights Treaties and USA Ratification Status.
While research reveals the major medical causes of maternal mortality (Collier and Molina 2019), more recent studies examined social determinants of (i.e. environmental, social, and economic conditions that surround) poor maternal health outcomes (Crear-Perry et al. 2021; Gadson, Eloho, and Mehta 2017; Shah, Kershaw, and Khan 2021). A recent review of literature on the social determinants of maternal mortality offered strong evidence of the role of race and ethnicity, insurance, and education in maternal deaths, but noted “a lack of diversity in the social determinants of health and maternal outcomes literature, including the type of determinants studied, type of study design, and exploration of potential mechanism that underlie the observed association” (Wang et al. 2020:911). This study takes aims squarely at some of these gaps.
Variations among states’ MMRs suggest that state demographics and state-level policies influence maternal health outcomes. Although many states report a decreasing number of maternal deaths, Indiana’s MMR continues to increase, similar to southeastern states like Georgia, Mississippi, and Louisiana (Moaddab et al. 2016). In 2018, Indiana reported an MMR of 41.4 per 100,000 live births for White women, and 53.4 per 100,000 live births for African American women (Indiana State Department of Health 2018). This MMR is on a par with Vietnam, Mongolia, and El Salvador (WHO et al. 2019), countries with far fewer resources to address these health outcomes.
In response to these outcomes, Indiana’s legislature established and funded a Maternal Mortality Review Committee in 2018. This committee reviewed all 2018 maternal deaths with a goal of identifying statewide trends and providing recommendations. The MMRC’s first report, published in December 2020, deemed 87% of the pregnancy-associated deaths reviewed preventable and identified substance use disorder as the top contributor to maternal deaths, with 36.5% of maternal deaths caused by accidental overdose (Indiana State Department of Health 2020). In 2021-22, journalists at the Indianapolis Star published the results of their investigative report on maternal mortality, sharing women’s stories and pointing to the closure of rural hospitals, preeclampsia, health issues and the failure to take the concerns of Black women seriously, substance use, and mental health challenges (IndyStar Staff 2021). Our analysis adds to these efforts to understand barriers to maternal health.
Methods
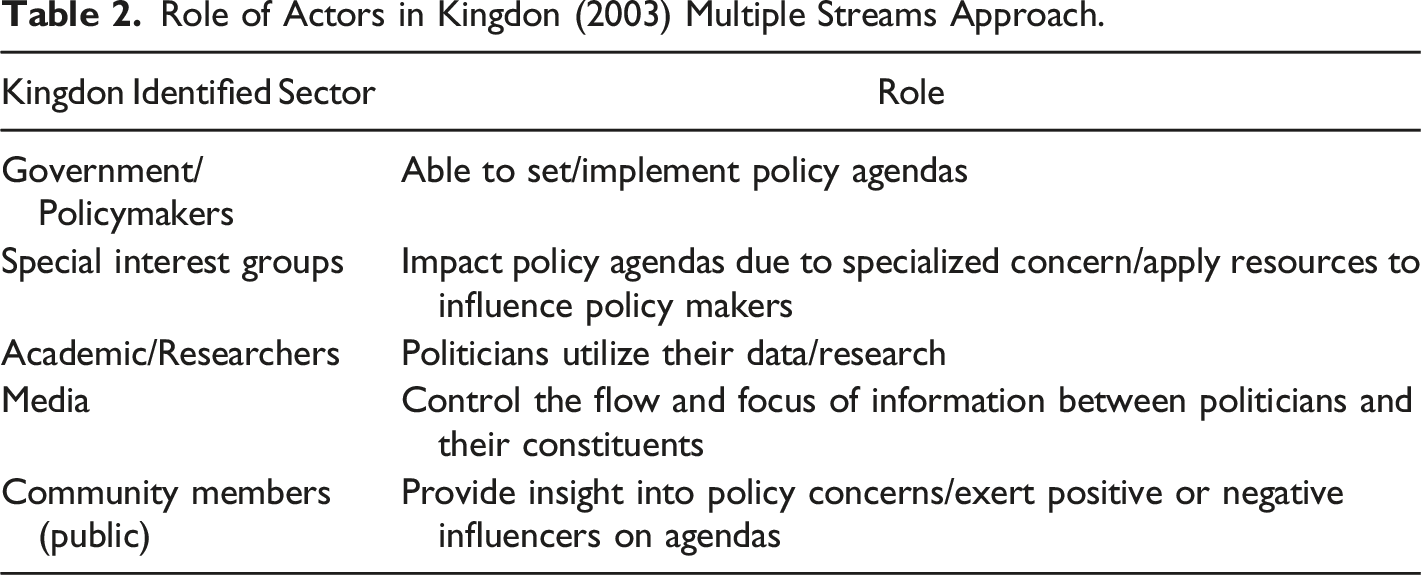
A human rights perspective “is concerned first with identifying the effects of social, economic, and political relations on women's health and then with promoting "interventions" aimed at transforming the laws, institutions, and structures that deny women's rights and well-being” (Yamin 1997:169). Accordingly, we used the Kingdon (2003) multiple streams approach to identify study participants because this approach encourages researchers to seek out the types of actors needed to influence policy. The alignment of these actors can create an optimal policy window to advance change (Figure 1). Table 2 outlines these actors and their role in promoting policy change. Kingdon Framework for Policy Change. Legend: This schematic displays the elements that need to align to create an optimal policy window for social change. Note that key to the framework is the voice of a diverse set of actors who identify social problem and solution strategies. Role of Actors in Kingdon (2003) Multiple Streams Approach.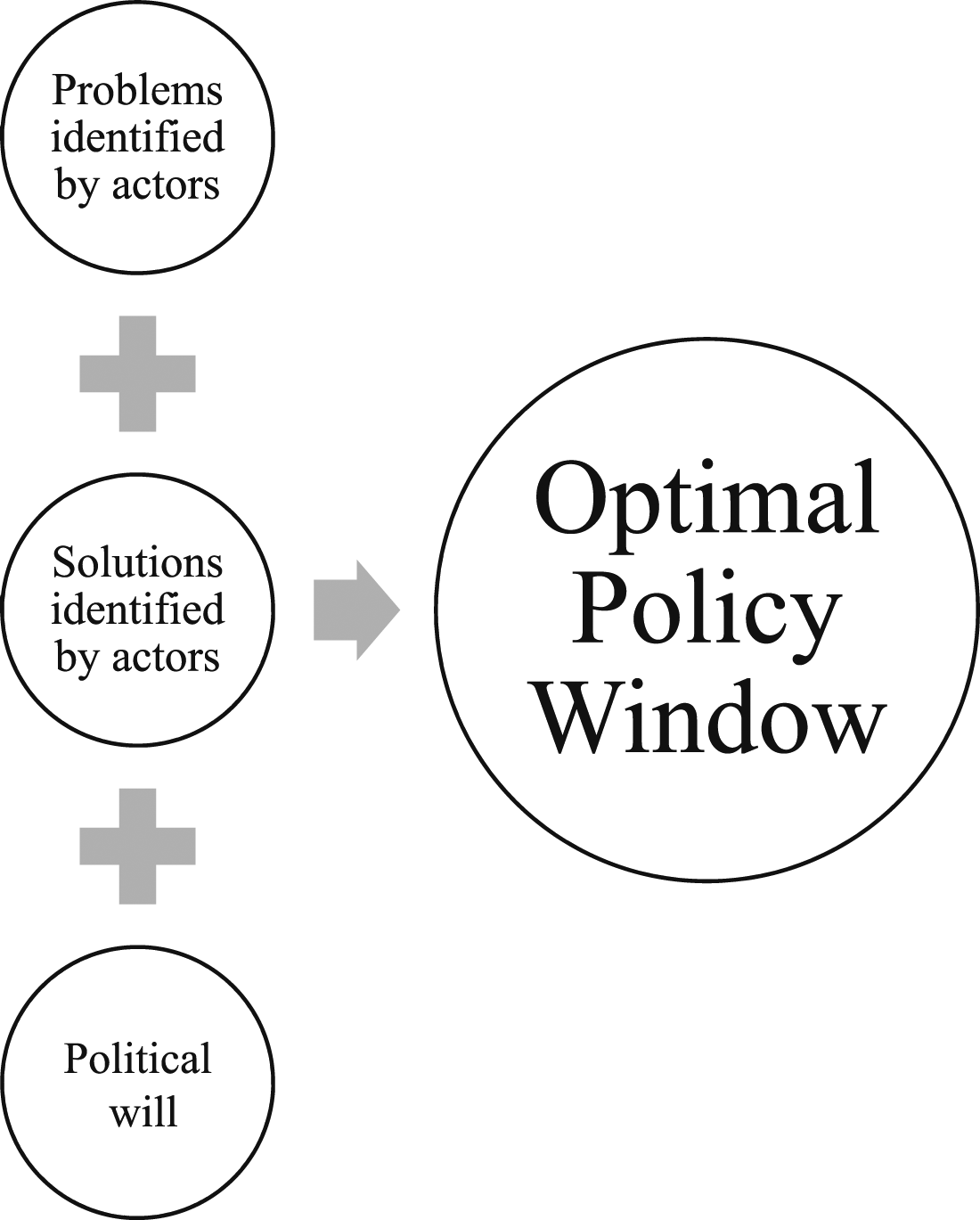
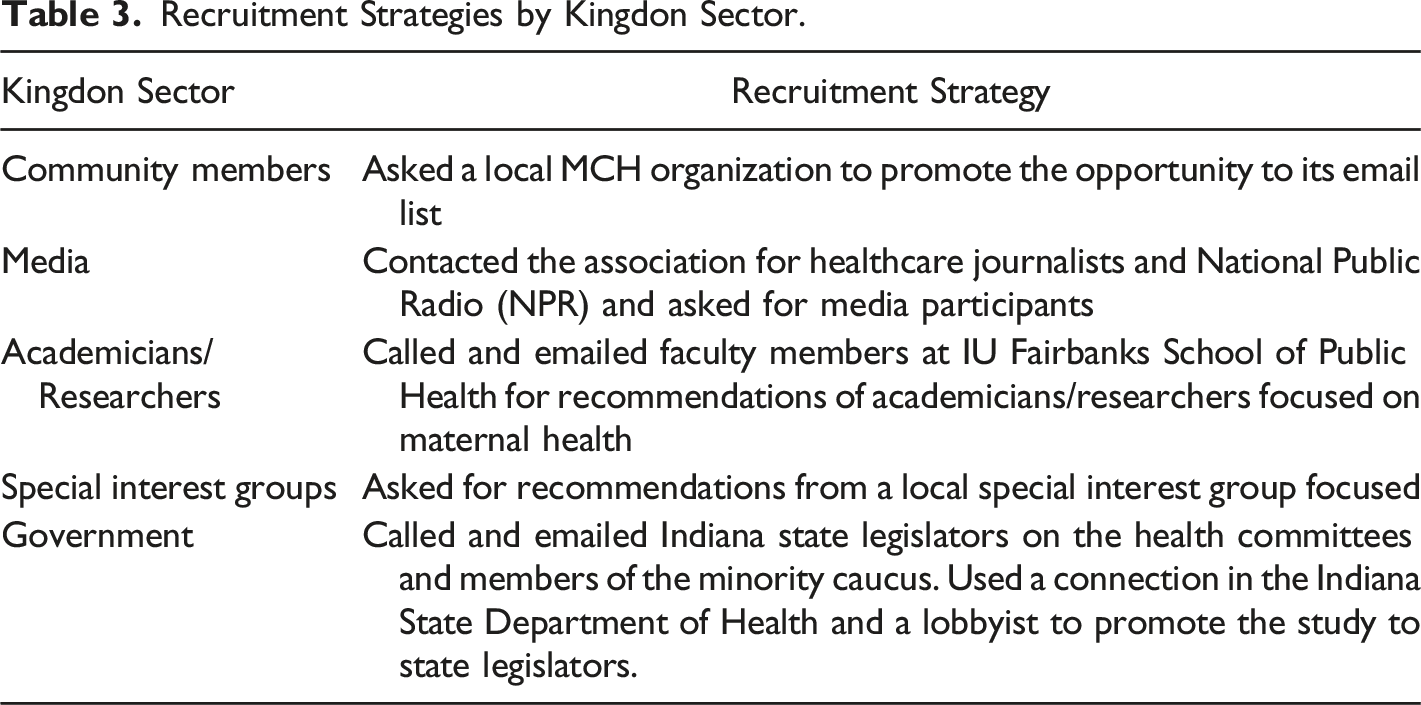
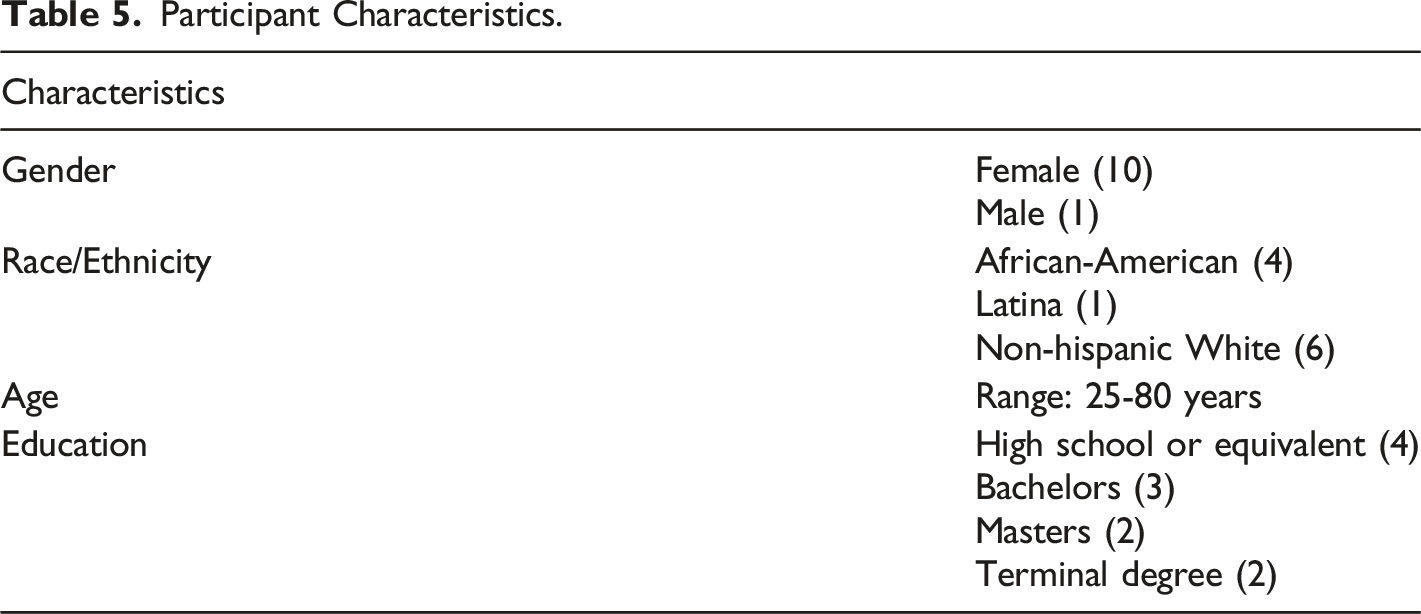
Reflecting the goal of empowering the women whose human rights are most likely to be violated, we included Black women who were enrolled in Medicaid during at least one pregnancy. Then, reflecting Kingdon, we included legislators, professionals in special interest groups, OB/GYN physician/researchers, and members of the media.
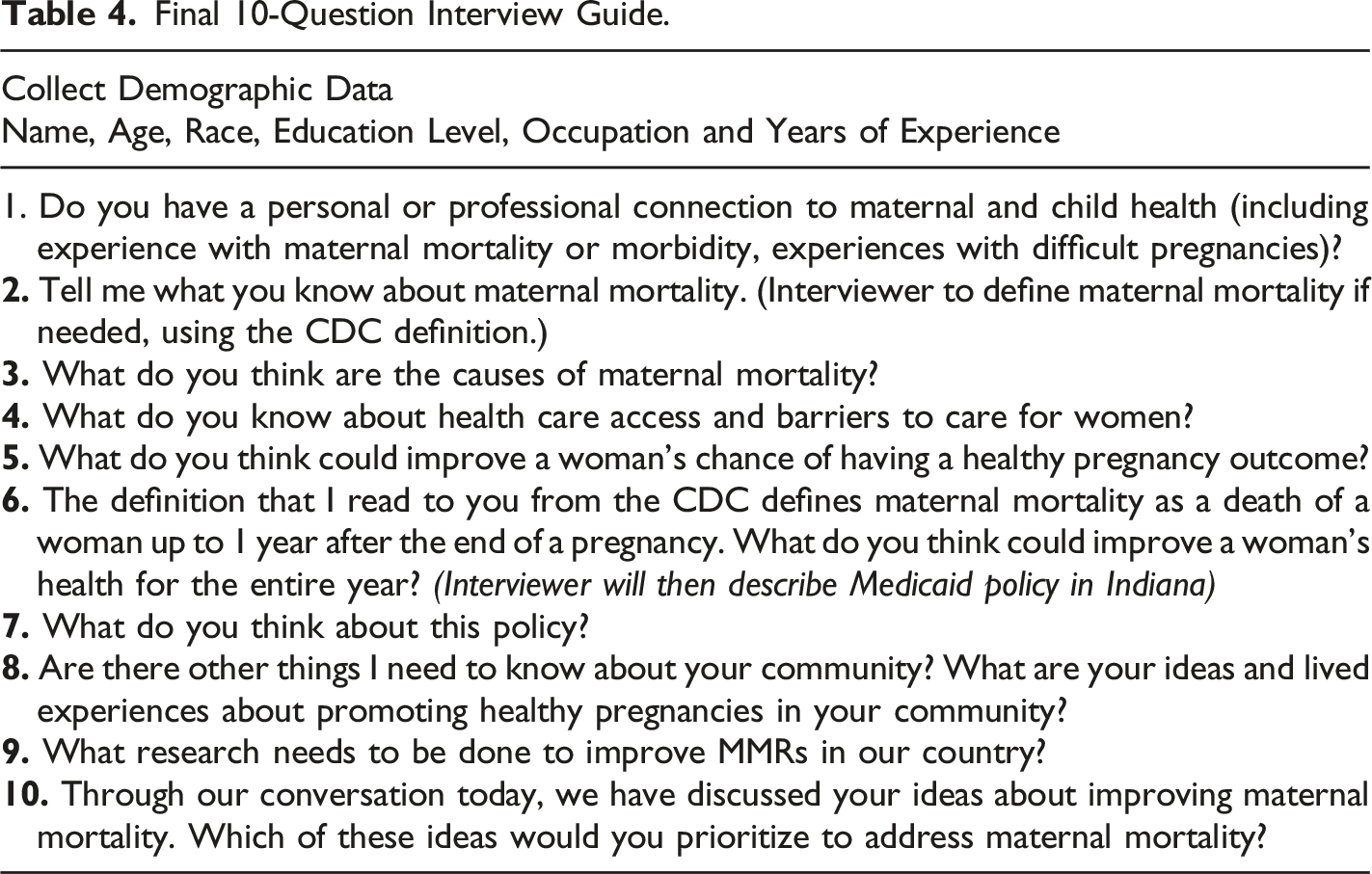
A narrative approach was used to collect data because it is an inclusive, ethical research method for promoting individual, community, and societal-level change (Biehl and Petryna 2013); specifically, this study relied on semi-structured hour-long interviews in which participants were invited to share perspectives and personal stories to inform our understanding of barriers to health. To develop the interview guide, a convenience sample of consultants from each Kingdon sector was asked to provide feedback on the initial draft protocol, which contained four prompts around factors contributing to health during pregnancy and the postpartum period, loss of Medicaid coverage at 60 days postpartum, insurance coverage in general, and ways to improve women’s health. A doctoral candidate developed the original four prompts based on a review of literature and was advised by her doctoral committee to test them and incorporate feedback from sector consultants prior to initiating the study.
Recruitment Strategies by Kingdon Sector.
Analysis
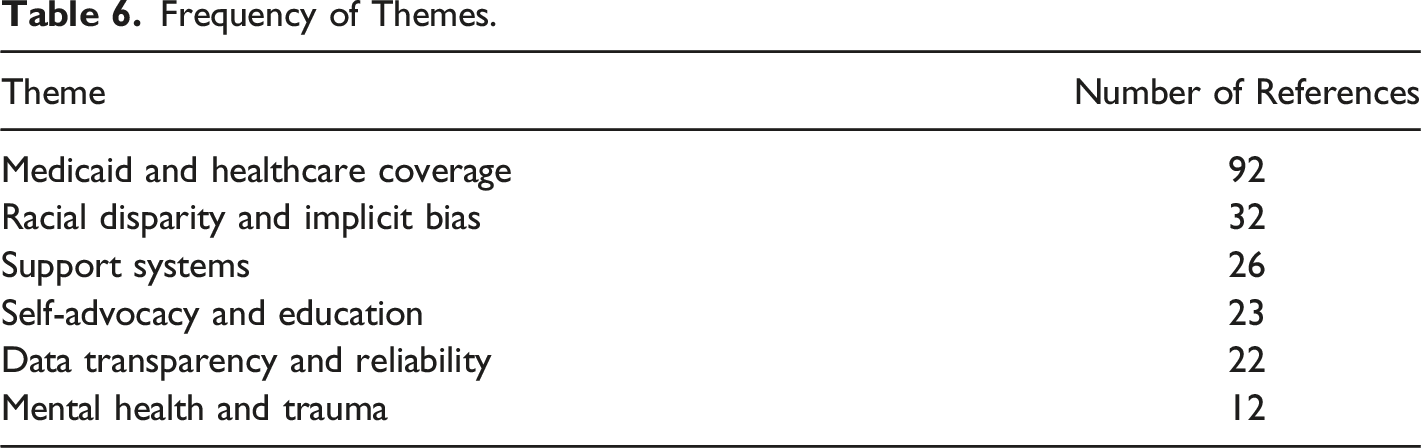
Data analysis techniques aligned with an editing (data-based) strategy, in which the researcher identified words/phrases in the text, that formed the basis for data-developed coded categories (Crabtree and Miller 1999). These were used to reorganize the text and search for the frequency of themes associated with the coded categories (Crabtree and Miller 1999; Malterud 2001). Two researchers used NVivo content analysis software (Wong 2008) to code data sets for themes. The two sets were compared for consistency and agreement of findings, and differences were resolved through dialogue to reach agreement. The codes were then combined into one Excel spreadsheet to find the frequency of references to themes. Because in a Kingdon framework, the alignment of diverse actors is seen as important to moving action forward during a “policy window,” we prioritized presenting the six themes where consensus across all or, in the case of one theme, most sectors emerged. To promote transparency, we have included participants’ quotations (in a different font) throughout our presentation of the findings.
Results
Final 10-Question Interview Guide.
Participants
Participant Characteristics.
Themes
Frequency of Themes.
Theme 1: Lack of continuous, quality health care coverage
Across sectors, participants articulated a belief that continuous and robust health care coverage for new mothers would yield benefits in terms of health, financial well-being, and/or return on investment. Many participants discussed the impact of losing health care coverage, especially Medicaid coverage, on new mothers. In particular, the loss of Medicaid at 60 days post-partum had serious consequences for women’s health, and, in turn, their children’s well-being. One community member, describing her experience seeking postpartum care, drew connections between health care coverage to the financial well-being of her household, her own health, and her ability to care for her child: So, after having my son, I developed mastitis really bad. But you know, your insurance cuts off at a certain time...even now I'm still receiving bills from me continuing to go see certain specialists that I had to see, you know, because it's something I had to have. It was awful. But my insurance didn't cover it, you know? I had no other option but to continue to see doctors and rack up bills. So, if I could continue to have like, the proper health care, so I can take care of myself the way that I need to take care of myself, so you know, that I can take care of my son now would have been like, awesome.
This community member shared that the loss of health care coverage created financial strain and damaged her credit score. At the same time, by suggesting that better health coverage would have allowed her “to take care of myself the way I need to,” this community member also indirectly linked coverage with care-seeking behaviors. Other participants made even more explicit links between coverage and women seeking care. For example, one physician/researcher said, “They lose access to their health care, and then they don't know what to do or where to go,” while a special interest group participant stated, “everyone pretty much knows that if you don't have health insurance, you're not going to go to the doctor.”
Individuals felt this was problematic because postpartum health care needs can surface months after delivery. A physician/researcher participant, commenting on the loss of coverage, noted, “…that is the worst thing for women because a lot of pregnancy-related deaths happen outside of that window.” Similarly, one of the special interest participants pointed out that “postpartum depression doesn't always hit right after you have the baby...” in discussing the need for extended coverage. Other participants noted that more stable coverage might also lead to improved health prior to conception as well.
With such broad consensus that expanded coverage would promote maternal health, why wasn’t there political will to provide continuous coverage? The two legislators provided insight here, saying that the state tended to prioritize economic development and: …we don't put much effort into public health. And so, I think that is an area where we need to improve. A lot of other highly developed countries [have] national health care. And we have the Affordable Care Act, but it could be a lot better…we're gonna have to follow that up with where we put our money. The budget always shows our priorities…we have such a social safety net with a lot of holes.
Spending priorities also surfaced in the other legislator’s discussion of the state’s decision not to fund expanded coverage. She stated, “it would be dollars and cents well spent” and went on to say, “I think it’s like 52% of all of our births in the state of Indiana, are Medicaid. And so, we're, we're already paying a bill, so I think that's where a lot of people don't like to talk about is what it's costing us.”
Even as legislators seemed very focused on discussing costs and benefits, other participants pushed back against this kind of thinking. “What's the price tag you put on the death of a young woman?” one physician asked. Despite expressed frustration with an “actuarial price tag,” this same physician and other participants were able to name a variety of significant costs associated with not providing more comprehensive health care coverage, including the long-term consequences for child development after losing a mother.
Theme 2: Racism and implicit bias
Participants across domains were quick to articulate structural racism and interpersonal biases as barriers to quality care. One of the community members took aim squarely at the role of bias, extending it beyond race and gender, in effect laying out an intersectional theory of “four checks” in health care settings: My personal belief is that there are three factors that will get you less preferential treatment - if you are a woman, if you are poor, and if you are Black. Four actually - if you're overweight, that counts too. If you have any of those four checks, you're not going to get the same kind of treatment as if you don't, and [my sister] had all four checks. And so, she comes in talking about how she's in pain and her back hurts and her stomach hurts…and they told her that they thought she was exaggerating and sent her home. She went into the hospital like three times. And then she lost her child.
This community member described a trauma compounded by bias, lack of understanding, resources, and support. In her view, anyone with one of the four “checks” will be treated poorly or disregarded, and she drew in an intersectional overlap of factors.
While not all participants saw as many factors, there was broad consensus that race and gender were key factors in health care access, in how women were treated, and/or in how they felt about interacting with the health care system. In one government/policy maker’s words, “…we need to be sure that all pregnant women have access, regardless of their race or not. I think there are racial disparities here.” One of the medical professionals, speaking about her own pregnancy, said she “just felt more vulnerable as a Black woman in the health care system.” She also described her wedding ring as part of a “protective shell,” suggesting potential fifth “check” against unmarried women.
Concerns about bias motivated women to make a variety of efforts to navigate around it. One community member sought out a Black doctor for her care, hoping that this would result in a change in the kinds of information she was given. She ultimately ended up disappointed: “Now if it was to happen again. I would not use a Black doctor. I didn't gain anything from it.” This same community member talked about how other women she knew made similar calculations about navigating a system they perceived as having racist providers, setting up a dynamic where women were accepting less resources to avoid what they perceived as biased providers: I have friends that are White that prefer not to have their babies in [a wealthy suburban town] because they have mixed babies, and they say that you know, that they're racist. That's totally, you know, I haven't experienced it. All I know is I don't want to be at [a downtown hospital] because you just aren’t going to get people and the resources that, you know, I need.
Some participants outright disagreed with the idea of the existence of four or five “checks.” One member of the media said, “I don't think that I think it's worse if you're poor. I think it's worse if you're a woman of color.” Similarly, the physician who spoke about her own pregnancy experiences shared her belief that “socio-economic factors don't protect you from these horrible outcomes.” She further stated: We can't say that like going to prenatal visits is what's going to protect you or, you know, being more health literate - granted that everyone should have health literacy - but we see Black women dying that had college degrees and advocated for themselves.
Like the idea of navigating to avoid bias, this physician seems to search for protective factors that would reduce bias, like attending prenatal appointments or greater health care literacy. Still, both “solutions” put the onus on women to avoid bias rather than reducing or eliminating it.
Regarding solutions, this same physician/researcher worried that applying the label “racism” would make addressing the challenge of bias more difficult: “…it's so hard, because I think that as soon as you hear the word racism, people get really defensive. If we call it ‘-ism,’ it kind of disassociated from anything we can do and have power over.” In a similar vein, one of the special interest group members felt that “bias” was too abstract or big to address concretely. “…we talk a lot about implicit bias, but we seem to talk about it as a sound bite at a very broad level, and we say there's implicit bias that I don't hear a lot of drilling down to specifics. What exactly is happening there?”
Participants did crave solutions that didn’t put the onus on women. One physician wanted someone to “come up with some implicit bias and medical racism training that we can start and measure” that is “interactive and gets people really connecting it to like their everyday life.” While ideas differed about how best to address them and how many “isms” to include, the role of racism and bias in health care clearly constituted a barrier most participants quickly identified.
Theme 3: Trauma and lack of mental health services
Community members spoke about their own trauma and the trauma of other women they knew. Alarmingly, these traumas appeared to exist in a space with little support, communication, or empowerment. In one community member’s words: So, yeah, they put me under, and I didn’t realize it. And then I wake up and it's the next day, and I wasn't allowed to see my son for 24 hours. And he was in the NICU, so we weren’t even in the same room. Again, I wasn't allowed to see him so I didn't meet my own child for a day. And I went through a long period of depression, and just very much confusion because I didn't have, like, some type of closure or something, like oh there's my baby. But I was pregnant and then I wasn't, and for a while, it felt like I still was, and I had to go through, “Is this my child? I feel like I'm still pregnant.” It was it was a really tough, really tough time. Yeah, really hard.
In this community member’s history, her mother had lost infants, and her sister had recently experienced infant mortality. Her family history of these experiences, combined with her own experience of an emergency c-section, left her struggling with sense-making and dealing with long-term depression. She was adamant that this would be her only child because she would not go through this type of experience again and felt very isolated.
Feelings of isolation and inability to make sense of what had happened were also expressed by a media participant, who noted the failure of health systems to provide mental health supports to women in the wake of trauma: [My sister] has a lot of scars, and a lot of, you know…physical scars and emotional scars. And, but the what the reaction was really kind of like, “Oh, that never happens to anybody you were the absolute only person that this has ever happened to…you’re a unicorn, you’re a freak” …. And, and for her the problem with that was that there was a real sort of silencing of her experience as a result, it was…there wasn't anybody. They didn't put her in touch with anybody to talk to. There wasn't anything that she could do about it.
When discussing the lack of systems for women to have all their health needs addressed, in addition to case management, several participants noted the concept of “self-medication” through substance use. One physician/researcher participant indicated frustration when making a behavioral health referral, noting: “the problem then becomes finding a provider." A community member expressed her concerns around mental health and substance abuse, which she then correlated to needing an integrated system to also address support systems: …health, mental health, and substance abuse is connected. You know, I think a lot of services are like one tract. So like, if you think about, like, a collective approach, like somebody that can help with mental health and drug use at the same time, like it could be a one stop shop, it could address like, homelessness and parenting and like, just working in more of a collective way, because I wanted my [friend] to go to rehab, but then she got to rehab and she's still homeless, she ends up on the street falling back into bad bad behaviors. We need to look at the whole solution and come up with problems that are attacking it from all angles.
Here trauma, mental health, and substance abuse are also linked to instrumental support, a theme discussed below. A physician/researcher also linked these back to health care coverage, suggesting that failure to address mental health needs arising from trauma constituted abandonment: “We need a much better [and] can do a much better job of not just sort of abandoning women in this country, based on insurance or what have you after the baby is born.” In other words, trauma and mental health connected with other barriers.
Theme 4: Lack of instrumental and emotional support systems
Participants described the need for both instrumental and emotional support. This theme intersected with both access to health care and the bias theme, as the lack of instrumental and/or emotional support either promoted or constrained access to quality care within the system. More specifically, lack of support systems contributed to situations wherein community members did not understand their diagnoses when hospitalized and/or when receiving services for perinatal care. For example, one community member stated: …if a woman doesn't truly feel comfortable with her healthcare provider, or the nurses who handle her, she's less likely to be honest, she's less likely to answer questions or ask questions. I had a major panic attack because I didn't have any support system, and the next thing you know I’m no longer pregnant [following c-section], and I'm back in my room.
All three community members discussed not understanding diagnoses while pregnant, and two discussed still not understanding the diagnosis and cause for hospitalization related to postpartum incidents.
Lack of appropriate support also discouraged healthy behaviors. One of the community members indicated frustration at not feeling supported when she was trying to self-advocate and linked the themes of support and racism. She had taken breastfeeding classes, educated herself on the importance of breastfeeding, and did not want her infant to receive formula in the hospital. She was discouraged because she expected the hospital and healthcare providers to support her desire to breastfeed her infant yet, she noted, “… my breastfeeding journey was never supported.” She wondered if the hospital did not support her because she was African American, and professionals assumed “…[my] community doesn’t have that dedication.” She eventually received support from a community-based home visiting nurse program, but her experience speaks to the role of bias and timing in the provision of needed support.
Community members also noted that the need for support goes beyond the hospital and includes supports like good jobs, transportation, and child care. “These are all necessary things that people act like it's a luxury. It is a luxury. But it shouldn’t be and it’s really not fair,” one community member noted. She went on to explain: At this moment don't have a car, I don't have a job, those are two major things. So, if I have an emergency. I either have to call an ambulance to take on that $2,000 cost, or I have to wait for somebody to come take me to the hospital. That's not a great plan either way. I've had to cancel multiple appointments because I just couldn't get there. And on one occasion I actually did make it to my son's appointment, I had to beg someone for a ride.
One of the physician/researchers concurred that a lack of supports plays an important role in deterring healthy choices, especially in nutrition and physical activity; “Those things are hard choices to make…when you’ve got a baby who’s crying…or you may need to go back to work.”
A physician/researcher in his/her acknowledgement of the need for these types of supports, added that different supports might be needed in different contexts: I think that really unpacking what are the major contributing factors to women in different areas of [State], because it may be all about social determinants and racism and poverty and things like that, in [an urban setting], my hypothesis would be that out in one of the counties outside of [another urban setting], it may be the fact that it's a two-hour drive to get to a hospital, or even a doctor.
Differentiation of supports to suit contexts must also include culturally responsive approaches, one of the legislators noted. Participants across all sectors also spoke about doulas as a potential source of emotional and instrumental support. One of the community members shared that she is seeking, “certification to become a doula so that I can help other women like me” and one of the policymakers mentioned her work at the state level to fund doulas for women who need additional support during the prenatal and postpartum period.
Theme 5: Insufficient knowledge and ability to self-advocate
The power dynamics between women and their health care providers, as well as between women and government, surfaced repeatedly. Community members expressed a strong need for more knowledge for women to “get out of their comfort zone and just be empowered to speak up for themselves and advocate for themselves.” Similarly, a physician/researcher wanted patients “to feel empowered enough to bring things up that they're concerned about, especially things that could potentially be life threatening” while a media professional wondered how to “empower patients to be able to have their voices heard” and suggested coaching patients as one potential strategy.
The community members offered clear examples of feeling disempowered, especially through lack of knowledge. One community member shared her experience of loss, expressing both disbelief and a fear that medical professionals had done something wrong: The doctors was looking at me and the nurses was looking at me like somebody slapped them...like they had never seen anything like this. And so, I kept asking, you know what caused this, nobody could tell me to this day. I still don't know what caused this. And so, then they just they kept me overnight and they did some procedure. I still have no idea what the procedure is. So, I know in that experience, like, I asked them a question. They would explain a little bit, but I didn't get it but I didn't push further to say, “can you explain it again? Right, can you break it down?” Because, like I said still to this day, I don't know what caused that. They didn't explain to me what caused it.
Despite the urging of family to consider a legal remedy to uncover whether something had been done wrong, she did not challenge the health care providers, nor even come to a full understanding of what happened. More information and empowerment may not have changed the loss in this case but may have mitigated the trauma and forced improvement in treatment of similarly situated women.
One of the physician/researchers acknowledged that failure to communicate might be widespread and inhibited women’s ability to better advocate for themselves and their babies, suggesting: ...as a culture in medicine, we don't explain well enough to our patients, what we're doing, we don't partner with them as effectively as we should. And some of that is by virtue of just lack of time, you know, trying to see a lot of patients and a little bit of time. And so a more efficient way to address the medical needs but also make sure that patients feel that they are getting the education they need so that, you know, if there is an emergency if something goes wrong, they're aware that something is not right as well.
Her comments also suggested a tension, however, because while she saw patient education as a tool to increase self-advocacy, she also felt it shouldn’t be the “patient’s responsibility to make sure that they’re not ignored.”
Even so, there were times when women used knowledge to do just that. For one of the community members, self-advocacy meant knowing what kind of treatment they didn’t want to put up with and how to maneuver around it, she connected awareness of what superior care looks like to empowerment. When Medicaid assigned her to a particular clinic, she fought to go somewhere else. “I've been exposed to better health care. So that was, like, not acceptable for me,” she explained. Meanwhile, however, she observed that her friends tolerated treatment she would not accept and theorized that lack of exposure to better care made them more accepting of poor treatment: I have a friend that had a baby after I had a baby, and she gave birth at [local county hospital]. And they have like a waiting room full of pregnant women waiting to have their babies and it blew me [away]. “Why are you waiting out here?” “Like, oh, cuz I have to wait, you have to wait.”
The community member contrasted this with another hospital where, when in labor, “you're going to call ahead, you know, you're going to be greeted at the door, they're gonna have a wheelchair for you – you’re going to go up an elevator to your room.” She posited that the women who lacked this knowledge – and, therefore, the ability to demand something better - were “all from lower income.” “Yeah, she has no idea that that it's completely different a couple blocks down,” she concluded.
Finally, community members expressed an interest in opportunities to advocate not only for themselves, but for other women. They wanted duty-bearers to make sure “we continue to have people of the community…that are affected the most by these things at the table to strategize and come up with plans to make sustainable change. Make sure they always at the table.”
Theme 6: Lack of data transparency and reliability
While not all participants spoke to this barrier, media and government participants repeatedly raised concerns about data transparency and reliability. They expressed skepticism the current systems in the USA report a true picture of maternal mortality data, given reporting discrepancies, non-standardized death certificate reporting, and lack of reportable accountable quality measures by Medicaid providers. The media participants argued that even among the systems that are in place to monitor health data in the United States, the data are still lacking. As one media participant noted: When you think about that, and you think about the maternal data, right, so the CDC data, and they say, they know that it's not the best data, right, like, so, you know, there seems to be a big disconnect between these two large government systems, right, CDC and Medicaid being unable to, to kind of connect. They don't. But I think the big issue is really Medicaid.
The participants spoke of the different insurance companies that administer Medicaid, and how this created barriers to data transparency. One media participant said, “The idea that the data…that information is not available to policymakers and researchers and reporters - but really policymakers and researchers even right, --- is shocking and wrong.”
Several participants spoke to the importance of using data to drive change. One media participant said, “Data transparency, I think that when the light of day is shown on things, it helps drive change. Nothing motivates people more than then when people know what you're doing.” Similarly, a legislator asked: “How can we improve a woman’s chances when we don’t have a clear understanding of the problem due to lack of data?” She went on to note that Medicaid is “one of the major payers for childbirth in this country” and added, “Policymakers should have data that allows them to know, what are we getting for our money's worth?”
Multiple participants also spoke to the need to study the issue more deeply and go “beyond numbers.” A special interest group member, flagging disparities for people of color, asked, “So, what's happening? To me that would be an excellent thing to drill down into.” Similarly, a media participant urged researchers and policymakers to take a deep dive into some of these reasons and some of the barriers to healthcare” adding, “that can probably be best done in a qualitative way, to be honest with you, instead of a quantitative.” One of the legislators spoke positively about the state’s new maternal mortality review committee, describing it as “critical” data collection mechanism to improving the state’s outcomes.
Concern over data collection, accuracy, and depth was deemed important by these participants to ensure that duty-bearers can fully understand causes of maternal mortality, can motivate change, and can ensure that remedies to ameliorate maternal mortality are sound. It is our hope that this research study begins to address their feedback.
Discussion
Interviews with Black women community members and duty-bearers revealed consensus around six barriers to maternal health in Indiana. These themes reveal the complex nature of the problem of maternal health and mortality, reinforcing the importance of examining social determinants of health and not merely the medical causes of poor health outcomes. They also speak to the importance of taking a more inclusive approach to defining health, and of establishing health as a right that duty-bearers are obliged to promote. Ultimately, they suggest that the USA has significant work to do to address the human rights of women and children.
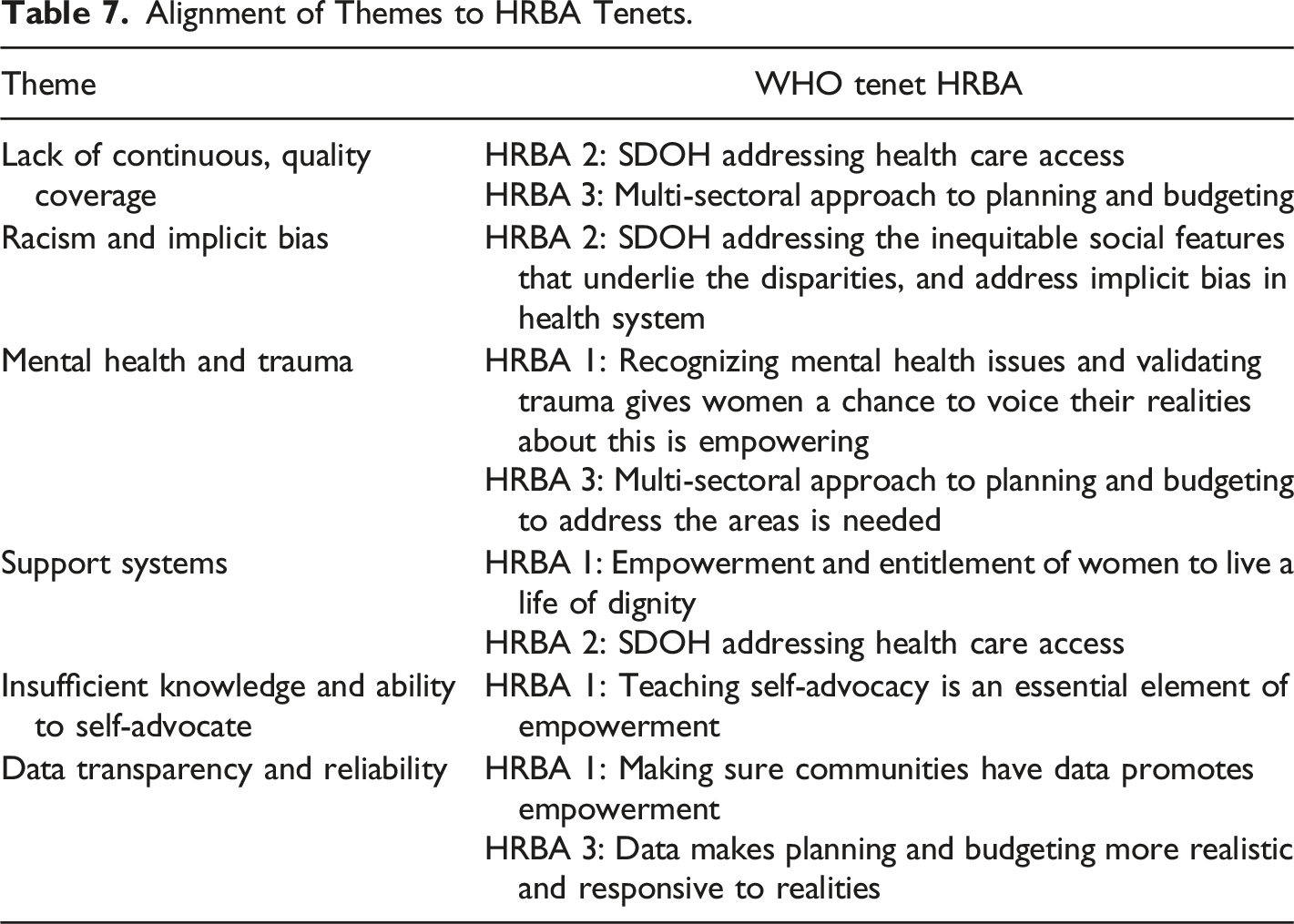
The counsel we received from this diverse range of individuals also helps us derive multilevel approaches to address this problem. We organize the remainder of our discussion around five of the solutions that emerged from participant interviews and how each fits within the existing literature, resolves barriers, and aligns with the WHO’s guiding tenets for applying a HRBA to maternal mortality (Office of the United Nations High Commissioner for Human Rights et al. 2015).
Make Health Care Affordable
Participants raised two important concepts about the consequences of the current state of health care coverage for women’s health: that it resulted in damage to the financial well-being women and their families and that it deterred care-seeking, impacting the mother’s health and her ability to care for her infant. The fact that so many Hoosiers have overdue medical debt supports the idea that gaps in health care coverage and/or insufficient coverage is resulting in serious financial harm. In December 2020, approximately one in five residents of Indiana had medical debt in collections, meaning that it is past due, and in communities of color in Indiana, that percentage rises to nearly one in three individuals (Urban Institute 2021). Women and households with children are also more likely to struggle with medical debt (Hamel et al. 2016). Past-due medical debt damages credit scores, which in turn can result in denial of access to housing, employment, credit, and insurance (Macey 2019).
Participants also shared that lack of coverage and/or the financial consequence of seeking care with poor or no coverage altered women’s care-seeking in ways that were detrimental to their health. Several studies support the notion that medical debt is a deterrent to seeking care (Herman, Rissi, and Walsh 2011; Kalousova and Burgard 2013). Medicaid expansion appears to have reduced the amount of medical debt held in the states with expansions (Kluender et al. 2021), however, further research on the intersection of insurance coverage, medical debt, and care-seeking, with particular attention to new mothers, is needed.
Seamless access to meaningful health care coverage that does not mire women in unaffordable debt is necessary to the achievement of women’s health as a human right. Efforts to expand meaningful insurance coverage touches all four HRBA tenets, in that such coverage empowers women to access their right to health and addresses social determinants. Given the obstacles, expanding coverage will require a multi-sectoral approach and due diligence in identifying, mitigating, and addressing barriers to implementation.
Implement Implicit Bias Training
Both health and the ability to live a life of dignity are human rights that cannot be attained in a context with racism, sexism, or other forms of discrimination. Racism, or “the hierarchical categorization of social groups into races for the purpose of differential allocation of status, resources, and power to White individuals” was shown to affect the quality of health care services in both structural and interpersonal ways (Volpe et al. 2021:338); until structural racism and implicit bias are addressed in USA systems, such as health care, advancing health equity will be difficult (Bailey et al. 2017). Participants affirmed racism as a barrier, adding gender, income, weight, and marital status as characteristics affecting care. Research adds support to the notion of four of more “checks” influencing health outcomes. Foundationally, Crenshaw (1990) introduces the concept of intersectionality and suggests that a complete understanding of marginalization must take multiple, overlapping identities and the compounding of disadvantage into account. We observe that while many researchers examining maternal health are addressing racism and racial bias (e.g. Green et al, 2021; Saluja and Bryant, 2021; Scott, Britton, and McLemore 2019; Taylor 2020); we concur with Hall et al (2015:74) that “future studies should also expand the assessment of implicit bias…Bias can exist on multiple social dimensions, and patients with multiple minority identities may be particularly affected.”
Participants raised implicit bias training as a possible solution to these barriers. Research suggests that bias in health care settings contributes to poor health outcomes, including for women giving birth (Hall et al. 2015; Schnierle, Christian-Brathwaite, and Louisias 2019); however, much of this research focuses on race and not on the possible interplay of marginalized identities. The same is true in terms of interventions in Indiana; currently, one county has started facilitating curriculum from the Stanford University RaceWorks project for their Women Infants Children (WIC) offices. The training is focused on WIC staff increasing their own racial literacy to interact with and provide services to the individuals that seek assistance through WIC. While this is an example of the duty-bearer (a government service) addressing a barrier (racial bias) in a system, further multisectoral planning and budgeting to embed implicit bias training and training that includes but extends beyond race to examine other marginalized identities into health systems are needed. Extending beyond interventions that address interpersonal bias to those that address bias at the organizational and systems levels will also be necessary (Alson et al. 2021; Green et al. 2021; Taylor 2020).
Expand Mental Health and Addiction Services
With the long-lasting trauma associated with loss and maternal stress, it wasn’t surprising that mental health and substance use disorders also came up during the interviews. Providing non-punitive access for women to substance use treatment during pregnancy is evidence-based practice and endorsed and supported by the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists (ACOG) (Patrick et al. 2017). Substance use disorder and recovery treatment can take from months to years, depending on severity, and the National Institute on Drug Abuse indicates that “good outcomes are contingent on adequate treatment length” (National Institute on Drug Abuse 2020:para. 2).
Currently in Indiana if a health care provider identifies a substance use disorder, and the woman is not currently receiving substance abuse treatment, the provider must begin treatment, or refer the woman to treatment. While this aligns with evidence-based practice, with Medicaid coverage ending at 60 days postpartum, women can be without coverage for mental health services or treatment of substance use disorder. The full pursuit of the right to health must include avenues, provided by duty-bearers, for women to seek, access, and claim their right for necessary mental health and substance abuse treatment.
Increase Access to Doulas
Participants discussed doulas as a potential solution to addressing the lack of emotional and instrumental support systems for Indiana women. Doulas are trained professionals that provide continuous physical, emotional, and informational support to a mother before, during and shortly after childbirth to help her achieve a healthy, satisfying experience (DONA International 2021). As such, they support the HRBA tenet indicating that women are entitled to and should be empowered to live a life of dignity. Trained doulas also able to address social determinants of health by providing culturally competent care (Hardeman and Kozhimannil 2016), connecting women to mental health resources, including those for postpartum depression (McComish et al. 2013) and substance use disorder (Mosley and Lanning 2020), and supporting women in navigating the health care system (International Childbirth Education Association 2015).
Typically, Hoosier women contract privately with a doula to provide this support; however, Indiana recently approved legislation for women on Medicaid to have access to doula services. Unfortunately, even with the approved legislation, funding for doulas was stripped from the state budget (Safon et al. 2021). Using the Maternal Health Block Grant, Indiana has made limited doula services available for women on Medicaid through a partnership with a nonprofit agency (Platt and Kaye 2020). With reliance on grant funding for doulas, levels of coverage and availability vary and are not “firmly” funded (Safon et al. 2021).
Increase Grassroots-University Partnerships
Finally, participants raised qualitative inquiry, or more specifically, grassroots-university partnerships, as a solution. These are partnerships between academic institutions and community members designed to empower typically marginalized voices in ways that expand knowledge and lead to concrete action. Grassroots maternal and child health movements are rooted in changing issues at the community (Hoffman 2008; Marquam et al. 2020). Engaging communities at the grassroots level is important because the leaders engaged at this level have personal and community knowledge specific to their community (Marquam et al. 2020). Grassroots movements that are focused on Black women, and women from all marginalized groups, have been called upon as “the” way to address health inequities (Barlow and Johnson 2021).
Currently, Indiana has a Grassroots MCH Initiative (IUPUI Richard M. Fairbanks School of Public Health 2022), in which women from marginalized communities are supported as leaders and placed “at tables” where their voices can inform system change efforts (Turman and Swigonski 2021). This partnership addresses duty-bearers’ suggestion for more voice, transparency, and data, including qualitative data, to increase understanding of the challenges associated with maternal health. It also aligns with the HRBA tenets in that it empowers, addresses SDOH, invites community into planning and budgeting, and addresses barriers to implementation.
Strengths and Limitations
The strength of this study is that it applies a human rights approach to the challenge of addressing maternal mortality. The study centers the voices of women and draws from a group of interview respondents that was diverse in terms of the sectors and viewpoints they represented. The voices of community women adds a layer of authenticity and insight that is not always available or sought. Another strength of this study was the vetting of interview prompts with the different sectors prior to the final production of the interview guide and use of multiple researchers coding the data to reach agreement on key themes.
The main limitation of the study was the small sample of participants from each sector. Additional participants would undoubtedly have provided additional insights; however, the fact that five of the six themes emerged in all sectors suggests that these are robust findings. Furthermore, thinking of other duty-bearers from beyond the Kingdon framework and/or doing a deeper dive into the areas of agreement or tension within sectors may prove fruitful.
Conclusion
Alignment of Themes to HRBA Tenets.
There is no silver bullet when it comes to improving maternal health in Indiana, it must be the culmination of many activities. Affordable health care, implicit bias training, expanded mental health and addiction services, doulas, and grassroots-university partnerships emerged as potential solutions that align with a human rights-based approach to maternal health. Further study, including examination of the impact of lack of continuous health care coverage, intersectional disadvantage in health care systems, and differing needs for instrumental and emotional support based on place and social identities would also assist duty-bearers in their advocacy. These data can be used, within the context of a HRBA to maternal and child health, to change Indiana’s MMR. It is now the responsibility of duty-bearers to advocate for these changes to promote the human rights of women.
Key Findings
1. A human rights based approach to health is a useful framework to address maternal mortality. 2. Policies targeting actions to improve maternal mortality are best derived from the alignment of perspectives of diverse policy actors inside and outside of government, with a prioritization of community women’s voices guiding the process. 3. Our application of these principles resulted in five themes that should be considered when advancing policy to address maternal mortality in Indiana and the USA: Medicaid and healthcare coverage, racial disparity and implicit bias, support systems, self-advocacy and education, data transparency and reliability, and mental health and trauma. 4. Respondants’ provided five different solutions that align with the WHO’s guiding tenets for applying a HRBA to maternal mortality: make healthcare affordable, implement implicit bias training, expand mental health and addiction services, increase access to doulas, increase grassroots-university partnerships.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Riley Children’s Foundation to JE Turman, Jr.