
Abstract
A content analysis of two complementary and alternative medicine (CAM) streaming shows on Netflix is presented. This qualitative analysis of the two interview-style shows reveals the influence of political beliefs in support of CAM and wellness lifestyles. Subjects in both television shows used the language of neoliberalism to describe their desires for and qualms with existing healthcare. The advantage of CAM and wellness lifestyles originated from its comparative emphasis on personal choice and market solutions to standard medicine. Finally, it is discussed how these political undercurrents can be leveraged to improve the outcome of education campaigns.
Personal Reflexive Statement
When I first began my research on vaccine hesitancy, I entered asking the same question many researchers pose: “why don’t people get the vaccines that are good for them.” As I sorted through the literature, I grew dissatisfied with Sociology’s and Public Health’s disengagement with Neoliberalism in all its forms. I believe that to understand vaccine hesitancy fully, we must examine “violently” the contours of Neoliberalism and its impacts on our relationship with Medicine.
A Content Analysis of Alternative Medicine and Wellness Programs on Netflix: The Construction of Medicine under Neoliberalism
Users of complementary and alternative medicine (CAM) grew from roughly 29% to 40% of Americans between 1999 and 2007 (Barnes, Bloom, and Nahin 2008). This growth continued to increase dramatically over the next 10 years, and by 2017 approximately 80% of American women used some form of alternative medicine. 1 Loosely defined as any treatment or product not taught as part of the core medical school curriculum, the scale of CAM is vast and underappreciated (Eisenberg et al. 1993). This market has boomed since the 1990s, mushrooming into a 17-billion-dollar market (Mikulic 2020), with a secondary industry preaching a life of general health and well-being worth roughly 1.5 trillion dollars to support its more narrowly defined parent (Callaghan et al. 2021). Taken together, these industries represent an astounding seven percent of the national GDP. Comparatively, the United States spends roughly 18% of its GDP ($3.8 trillion) on standard healthcare (CMMS Staff 2020).
Despite multivitamins and supplementation increasingly becoming recommended by physicians and public health officials, the nearly fifty-billion-dollar vitamin industry exists in a liminal space. Although (over)supplementation is seen as beneficial by the medical community in some instances (Waggoner 2017), the use of mega-vitamins by the alternative health and wellness communities (henceforth collectively called “healthists”) as a “prevent-all” has made the medical community approach supplementation cautiously (Crawford 1980; Eisenberg et al. 1993). The coalescence of these factors has led to the “health” industry (healthist, vitamins, and standard healthcare) comprising a staggering twenty-five percent of the national GDP today.
Some scholars have placed the origins of such a large market and consistent exponential growth in social dissatisfaction with medical care (Astin 1998) and increasingly adversarial relationships between patients and doctors (Defibaugh 2019). To the average patient, this is not the case, however, with alternative medicine being seen as an augment to allopathic medical treatments (such as to reduce side effects) (Johnson et al. 2018). Additional research suggests that cancer patients use alternative medicine to make their treatment closer to what “fits” their belief of what healthcare “should be” rather than reject it completely (Astin 1998).
However, relatively little research exists aiming to show how these perceptions of medicine are constructed. Likewise, the literature examining how consumers process and reconcile their qualms with the medical industry needs to be made more robust. Research on CAM users has relied mainly on marketing discourses: which demographic is more likely to use a specific treatment, how can education campaigns (often treated like marketing campaigns) shift voluntary purchasing habits, etc. Some scholars have attempted to bridge this gap, examining how the political economy influences our understanding of and relationship to healthcare (Hallin, Brandt, and Briggs 2013). Emphasizing, among other things, personal responsibility, lax government regulations, and consumer spending, neoliberalism has been a potent force in redefining the roles of citizens, the government, and the market (Harvey 2011). Esposito and Perez (2014) argue that this political and economic project has carried over into medicine, leading patients and healthcare providers to treat health with this hyper-individualist market logic. Faced with institutional retreat, patients are held responsible for their health management and increasingly expected to decide on complex treatments (Armstrong 2005; Conrad and Potter 2000). Though illuminating, this line of work has risked economism, with ideological and cultural shifts merely a consequence of economic changes.
Building on this research, I analyze two recent healthist “television” shows that aired directly to Netflix in 2020 as a microcosm for the healthism industry. The Goop Lab with Gwyneth Paltrow (hereafter called “Goop”) was announced in 2019 (Iannucci 2020) and released in January 2020, while UnWell was released in August 2020 and similarly filmed in 2019 (Horton 2020). I begin with a brief history of modern medicine, arguing that the neoliberal restructuring of medicine has fundamentally altered how patients, practitioners, policymakers, and others relate to medical institutions. I go on to emphasize the importance of media in constructing our beliefs. Next, I use Gramsci’s theories of hegemony and common sense to contextualize existing literature on CAM, neoliberalism, and medical consumption. Through my analysis of Goop and UnWell, I found five main themes: otherization, idyllic health, patient autonomy, frustration and disenchantment, personal responsibility, and legitimate medicine. These results provide critical insights into healthism’s goal of making active consumerism the cornerstone of healthcare. Through the shows’ interviews with patients, practitioners, and researchers, both Goop and UnWell present undisputed “facts” regarding standard medicine, CAM, and how a person can control their health. I recommend ways researchers and policymakers can reconceptualize how medicine is understood, related to, and interacted with. This reconceptualization can steady a wavering effort to combat misinformation and distrust effectively.
Theory
Neoliberalism
Like all institutions, medicine’s ideological narratives interact with the political economy (today, neoliberalism) to define goals and methods to achieve them (Althusser 2014). This has become clear as our wider social, political, and economic existence has been restructured to cement neoliberalism’s hegemony. Despite often being taken as self-evident, beliefs are neither neutral positions nor their production. The neoliberal, ideological definition of a “good” citizen as independent of the state inherently relies on those reliant on the state becoming deviant (Fording, Schram, and Soss 2009). “Good” citizenry is therefore constructed to exclude those relying on governmental assistance for healthcare, disability services, and other social services. This fundamental “common sense” of the world that we develop through ideology is described in detail by Gramsci (Gramsci 1992). Such “common sense” relies on commonly accepted “facts” that we use to navigate and explain life. For example, people “know” that a profit motive sullies drug development and efficacy (Navarro 2007). These “facts” are dynamic, changing with the politics and economics of our life, being more of a truth than a fact (Gramsci 1992). Simply put, our socially common assumptions are built on, and change with, our collective existence. Moreover, this wide-ranging common sense allows for self-identification, which can often be mistaken for personal, experiential knowledge (“I am x, so I do y.”).
Gaining steam in the 1980s, neoliberalism became fully entrenched in America, Canada, and Western Europe and began making inroads globally by the late 1990s (Harvey 2011). An all-encompassing economic and political project that minimizes the government’s role in daily and economic life, regulatory and social “reforms” coincided with reshaping societal-level beliefs around individual responsibility, personal choice, and market-based freedom. The neoliberal project has also attempted the ultimate goal of the market: “things which until then had been communicated, but never exchanged, given, but never sold, acquired, but never bought – virtue, love, conscience – all at last enter into commerce” (Marx 1992). This transformation did not leave the medical system unscathed, with regulations mandating patient decision-making (informed consent), reducing development regulations, and generally fostering a market-based healthcare system (Fisher and Ronald 2008; Navarro 1994). Concurrent technological changes transforming medicalization into biomedicalization quickly merged with the personal responsibility narrative to develop a unique social understanding of medicine (Clarke et al. 2003). Where non-compliance with medical treatments was previously pathologically deviant, the biologically individualized commodification of the body places the moral onus of health onto the individual (Crawford 1980; Zola 1972). Similarly, the allowance of pharmaceutical advertisements in 1997 has given rise to an advertising industry that often suggests that to remain healthy, patients are obligated to actively seek the most “up-to-date” treatment in the marketplace rather than rely on their physician (Murray et al. 2004). With the proliferation of smart devices to monitor personal health metrics, the market has become the primary locale to attain health (Esposito and Perez 2014).
This centrality of a market-based patient cannot be understated. With medical treatments falling victim to the “commodification of everything,” consumer education is increasingly seen as the only guarantor of health. Despite the occasional doctor-patient disagreements, this decision-making and self-education remain the fundamental method of empowerment, transforming patients into experts and democratizing treatments from breast cancer to heart disease (Armstrong 2005; Busfield 2010; Defibaugh 2019). Indeed, vaccine-hesitant parents have framed themselves as empowered, self-educated, and moral parents, implicitly framing those who follow the complete schedule as “lazy” parents (Reich 2016).
Building on the consumer-patient’s development, a plethora of health-recommendation media and technology have developed. Medical television shows—Dr. Oz, The Doctors, etc.—sprung up relatively early; wellness shows/segments and websites have provided direct access to patient-mediated education (e.g., WebMD) and alternative treatments and their supporters (Betsch et al. 2012). The last decade or so has seen the rapid development of biomedical technologies breaking into this healthism market. With fitness trackers providing by-the-minute updates on your “heart health,” sleep habits, and fertility, and DNA tests giving biological reasons for why you might be heavier than you want (and the best ways/products available to counteract your natural “ill-health”).
This marketization of healthcare has led physicians to “lose control” of medicalization, with corporate and consumer demand driving (bio)medicalization and over-prescription more frequently than before (Bell and Figert 2012; Conrad 2007). As patients have increasingly become experts of their own health, treatments have increasingly catered towards their desires—though this has been shaped significantly by corporate pharmaceuticals (Moynihan and Henry 2006). As biomedicine and consumerism have become entrenched, self-directed treatments are seen as the natural course, with personalized cures or maintenance schedules the ideal. Ultimately, this has resulted in increased pharmaceuticalization, with consumer-patients seeing prescribed treatments as unique, individualized treatments to a unique, individual problem; even when the treatment is in response to a larger social problem (Lakoff 2004; Pescosolido et al. 2010).
Orientalism and Otherization
Modes of thought can exist in an altered form centuries after their introduction (Poulantzas 1978). Perhaps the most pervasive “facts” haunting us are, as Edward Said called it, our beliefs of “The Orient” (Said 1978). By examining how European colonial powers portray “The Orient,” Said observes that “The Orient” is nothing but an imaginary geographic area unique to each colonial experience—perceptions of “the east” are different in Britain, France, and Germany. This imaginary is based on real or invented difference and can flatten everyone in the “orient” into a single homogenous culture and people. The Thief of Bagdad just as much portrays British ideas of West Asia as it represents American ideas about East Asia (Said 1978). “They” are different from us: while “we” are honorable, “they” are conniving; while “we” are brave, “they” are cowardly; while “we” are progressive, “they” stuck in the muck of feudalism; while “we” favor the individual, “they” are a single collective consciousness. Indeed, we see these ideas continue into today. China is regularly depicted as a collective under the control of a single man: Xi says jump, and the entire country asks how high (Buckley 2022). Similarly, the global south is “known” as a den of copyright thievery. Of the countries labeled by the United States government as “threats to intellectual property,” only one is a “Western” nation (USTR Staff 2022).
Stuart Hall rightly expands on this untethered relationship, describing “orientalism” as a subcategory within the colonial process of “othering” its subjects (I will use this term going forward) (Hall 2018). As we will see, the colonies and semi-colonies in Africa, South America, South and South-East Asia, and Oceania are equally exoticized. Common sense, however, is not cohesive (Gramsci 1992). Instead, “facts” can be vague, contradict, compete, supersede, or replicate each other. The “West” at times is portrayed as deficient compared to the “Rest,” but the “West” “was always in a position of strength” (Said 1978). We will see this manifest in the exotification of “eastern medicine” as inherently humanistic because, condescendingly, those cultures are not linked to the materialism of capitalism.
It is beyond the scope of this paper to provide an in-depth analysis of orientalism in the media. It must be noted, however, that orientalist tropes are maintained in altered forms. Japan is portrayed as technologically and economically advanced but culturally backward. China is seen as an economic and military threat unequal to the US; China has only become a competitor by falling victim to its cultural backwardness. “The media … [is] one place [where] … ideas are articulated, worked on, transformed, and elaborated” (Hall 2021b). Indeed, as “the media’s main sphere of operations is the production and transformation of ideologies,” television, film, literature, radio, etc., are both reflections of our existing social and political norms (ideology) and significant influencers of it (Hall 2021b).
Otherization as an Assistant
It is important to note that otherization is a competitor to neoliberalism’s hegemony. Otherization and orientalism are devoid of political-economic analysis. Stuart Hall attempted to link these when describing the colonial origins of otherization but did not fully touch on this. The absence of political economy has been criticized as making the theory deficient, but it remains useful when narrowly applied to folklore and ideas of difference (Amil 2021; Hall 2021a). As with other common beliefs, otherization augments the hegemonic project and its direct ideological beliefs. Individual freedom is a tenant of capitalist ideology, with otherization depicting “other” cultures as deficient because they disregard this “right.” Likewise, political-economic projects like socialism are condemned for suppressing market-imposed freedom. 2 Importantly, we have seen orientalist tropes fall victim to commodification rather than eke out a set of practices and ideas that are “sacred,” so to speak. Asian femininity, healing practices, and philosophies have been packaged and sold as wellness tactics (Cheng 2019). As we will see, a corpus of Buddhist and Hindu religious texts (tantra) are turned into a way to purchase better sex.
Methods
This study aims to elucidate ideas of medicine, wellness, alternative medicine, and personal health through self-narration in the interviews. The stories (and treatments) highlighted by the producers and the ways the interviewees describe them are reflections of such preexisting ideas rather than endeavors of re-creation. I will address discussions as ideological, refraining from delving into the efficacy or “correctness” of standard treatments, alternative treatments, and wellness lifestyles shown. As political and economic shifts shape culture, factual argumentation is relatively ineffectual. Indeed, we have seen vaccine-hesitant parents double down on their decisions, even after agreeing with the hard numbers (Sobo 2015).
Although the majority of public health discourse analysis has been done through the frame of the news, such research provides adequate groundwork for analyzing healthist television. For example, a content analysis was used to examine how images and behaviors are used in magazines to stigmatize obesity (Gollust, Eboh, and Barry 2012). In addition, talking points have been used to identify the ideological shape of obesity discussions (Kim and Anne Willis 2007). Another study compared the depiction of seven diseases in the media to identify bias (Armstrong, Carpenter, and Hojnacki 2006). Similar to these, an analysis of newspaper coverage of stay-at-home mothers has demonstrated how motherhood is romanticized within a neoliberal framework (Orgad and De Benedictis 2015). Likewise, textbooks have been analyzed to examine how neoliberal ideology is furthered in textbooks (Babaii and Sheikhi 2018). With these examples and our brief discussion of orientalism, we can see that “the media … [is] one place [where] … ideas are articulated, worked on, transformed, and elaborated” (Hall 2021b).
Both Goop and UnWell began as 6-episode series in 2020. Neither has been renewed for a second season though Goop received a spin-off series on sexual health. The spin-off was released after coding was completed for this study. These shows were chosen for four reasons: 1) Netflix produced both. Netflix is available in 190 of the 195 countries in the world, making these shows widely available (Netflix Staff 2022). Netflix has a membership of 220 million globally with roughly 73 million US subscribers (Ruby 2022). It is projected that an additional 30 million people in the US access the service on another person’s account (i.e., “out of household password sharing”) (Malik 2022). All considered, roughly one-third of Americans utilize Netflix; 2) Both shows use a similar documentary format; both feature well-established creative teams and hosts. Goop features Academy Award-winning actress-turned-businesswoman Gwyneth Paltrow. YouGov has found that 89% of Americans have heard of Paltrow, and only 19% hold an unfavorable opinion of her (YouGov Staff 2021). The “executive in charge” of UnWell, Stuart Fero, has won multiple Emmys for his documentarian work, both independent and on the investigative journalism program Frontline (IMDb Staff 2022); 4) UnWell and Goop (the show and the company) have been accused of platforming junk science and opportunistic snake oil salesmen (Albert and Block 2020; Bradley 2020). 3 Though Netflix does not generally release viewership numbers, it would not be unreasonable to assume several million people watched each show based on the notoriety of Paltrow and the controversy of the shows.
UnWell and Goop differed slightly in that UnWell interviewed new participants each episode while Goop had a fixed rotation of participants. Likewise, while Goop made use of the Goop corporate office staff, asking workers to undergo treatment and be interviewed before, during, and after treatment, UnWell changed locations each episode. 4 In addition to Goop staff, unaffiliated patients were interviewed after treatment. Some were interviewed after they had been undergoing treatment for several years, while others only took a treatment once. Practitioners were interviewed in similar circumstances, with one or two practitioners serving as the primary “medical” resource throughout the episode. 5 Other practitioners were interviewed during the episode to provide further insight on how a treatment functioned or how additional benefits might be gleaned from it. Often practitioners urged viewers to exercise caution when electing to use a particular treatment or to consult a doctor before use—both shows displayed similar disclaimers at the start of each episode. Persons who were not patients or practitioners were interviewed to provide insight into patients' experiences. For example, the mother of someone undergoing treatment was interviewed. Finally, researchers testing a treatment in a clinical setting were interviewed on the clinical implications.
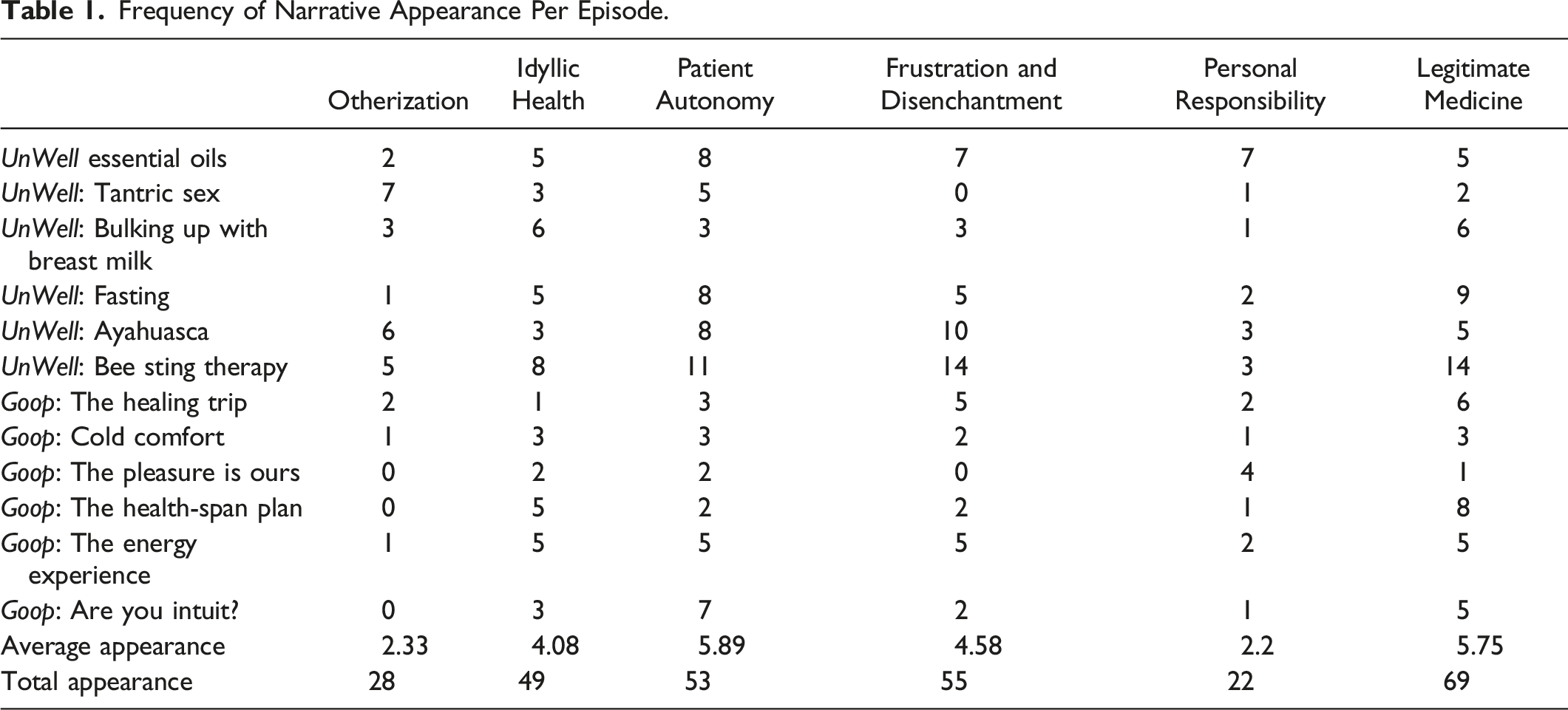
Though Goop and UnWell both follow an interview format, I do not have access to the questions or the full response transcripts. Instead, I am limited to the answers provided in the show. As a result, I treat the subtitles provided by Netflix as an “official” transcript. Five main themes/codes were chosen in line with previous research suggesting the five themes can provide quality information before running the risk of repetition and oversaturation (Kim and Anne Willis 2007; Lawrence 2016). Secondary coding was done to denote how the main five were discussed (Saguy and Almeling 2008). Themes were adapted into codes after watching each episode once. These codes were verified and modified on a second re-watch where data was not collected. Episodes were re-watched five times after this creation process to ensure accurate coding and data collection. Certain sections were watched additional times during the analysis.
Frequency of Narrative Appearance Per Episode.
Total Narrative Frequency & Total Frequency of the Positive/Negative Inflection.
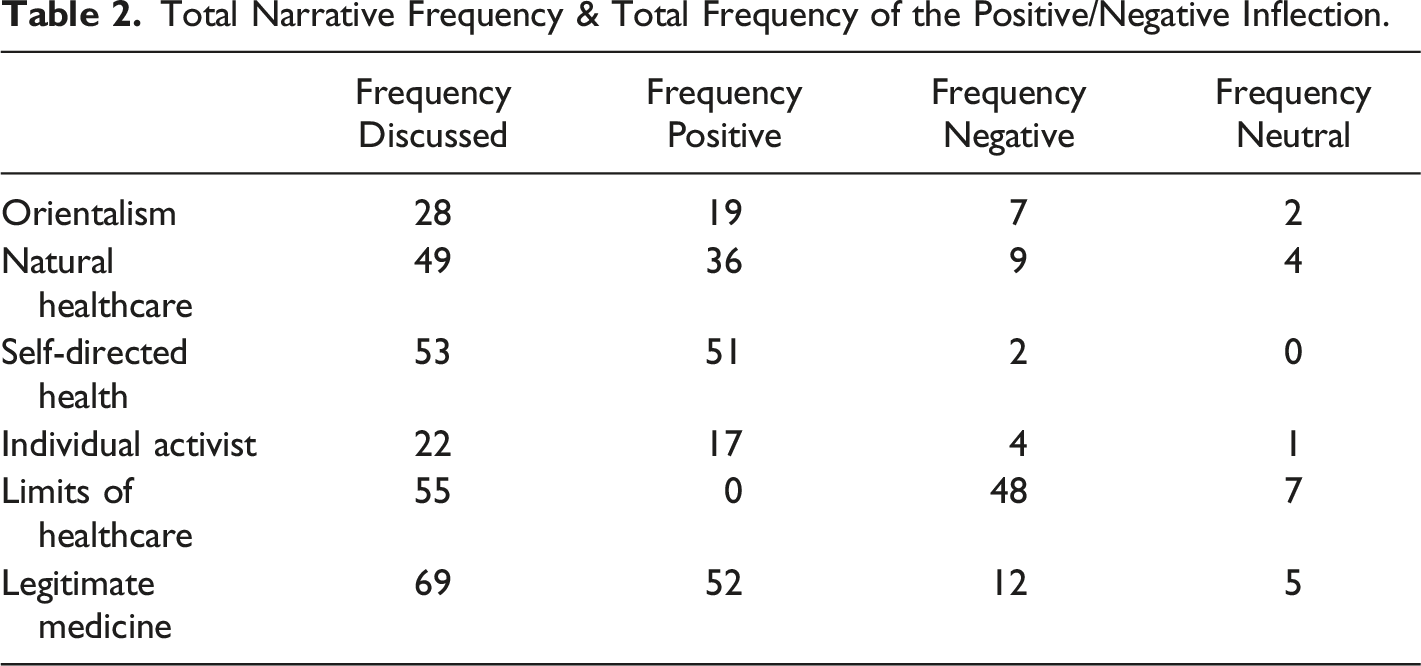
Otherization as a code followed Stuart Hall’s concept of “otherization,” which itself was an expansion of Edward Said’s Orientalism. A “collections of dreams, images, and vocabularies,” Orientalism (and therefore otherization) is vague in its strictness (Said 1978). “Other” (i.e., “non-Western”) cultures are collapsed into a larger non-western one where archaic beliefs, ignorance of science, and a rejection of “progressive social norms” abound (Hall 2018). Importantly, as we will see soon, this othering can be contradictory in a way that cedes credit to Other forms of knowledge without demoting Western supremacy (Said 1978). The other codes were more straightforward.
Romanticized health was marked when an ideal rooted in “natural” healthcare was invoked. Self-directed medicine and healthcare failures were coded when an explicit or implicit reference to the necessity of “taking the reins” from practitioners to achieve their desired outcome. Personal responsibility was made a different code to better identify feelings of a “moral imperative” to be healthy and stay healthy. This is distinct because personal responsibility takes the importance of the medical system and places it squarely on the patient’s lap, while the previous two are done out of necessity (Crawford 1980). Neoliberalism, anti-neoliberalism, and anti-capitalism were not used as codes. As we will see, these fundamental ideas (or reactions) influence how patients and practitioners process their relation to the world and medicine. Though the same can be argued about orientalism/otherization, it is possible to refrain from using such tropes or to recognize them and “own it.” For example, a clinic in UnWell, rather blatantly, uses almost every stereotype of indigeneity to create the right atmosphere for its customers. While themes were distinct and coded as such, they were deeply interlinked; otherization was often incorporated into conversations focusing on idyllic/romantic ideas of healthcare. While it is beyond the scope of this paper to discuss the contours of ideological construction and inter-reliance on ideas, beliefs, and folklore, it is worth acknowledging that the themes and codes described can inform the idea central to a discussion. (Gramsci 1992; Said 1978).
A tracking code was assigned to note who was the center of a discussion/interview (a patient, doctor, chiropractor, etc.). Additional demographic codes were also used to approximate the race, gender, and class position of speakers. It should be stressed that these demographic codes were done solely on appearance. It was impossible to code for class, race, or gender without using stereotypes and personal biases when there was no explicit self-identification. The codes are labeled as “x-presenting” to account for this overreliance on presentation. While this poses the risk of misgendering, racial profiling, and misrepresenting class approximating these identities helps develop a general understanding of the programs’ demographics and how identities are discussed within. For example, we can see that most treatment consumers are white-presenting.
Findings
Women made up roughly 67% of patients seeking the CAM covered in the shows. Several treatments were overwhelmingly gendered. For example, sixteen feminine-presenting people discussed their bee sting treatment (BST) while only one masculine-presenting person did; 11 of the 14 patients in UnWell’s fasting episode were men. There was a relatively even split between masculine-presenting (46%) and feminine-presenting (54%) practitioners. These discrepancies likely reflect broader gender norms and forms of misogyny unique to the medical system. Practitioners were overwhelmingly white, as were the patients: roughly 81% of practitioners and 80% of consumers were white-presenting. Anxiety and stress were the most common ailments being addressed. The CAM featured was also sought for its ability to help manage other interrelated mental issues like alienation or trauma. CAM as a total replacement for medical treatment was also common.
Otherization
An overt theme in all but two episodes, otherization collectivized non-western knowledge and cultural traditions into a single, ancient bloc of “history” removed from modern capitalism. For example, opening UnWell’s fasting episode, the disembodied voice stated: “every major religion has a tradition about fasting, from the Jews to the Jains, the Hindus, the Muslims.” In Goop’s “Energy Experience” episode, a clip of a bustling office was shown, with a voice-over of the episode’s featured practitioner (a masculine-presenting white person) softly stating that “in the western world, we value achievement over fulfillment.” Consequently, a practitioner opened a psilocybin session in Goop’s episode on mental health by saying: “indigenous people who have used [psilocybin] for years have really traditionally used them [to] cure … physical illnesses … [our illness is] that we do not have any connection with anything other than ourselves and the material world.”
Idyllic Health
A belief that there was an idyllic type of medicine could be returned to prevalent across both shows. This definition was relatively loose, based on a rough conception of “natural” health and healthcare. This understanding was linked heavily with the otherization of non-western cultures and the belief that pharmaceutical/surgical treatments can be too much.
The “traditional” bee sting treatment featured in UnWell was described by an acupuncturist as superior to an injectable because “a lot of [beneficial] volatile substances are lost” when bee venom is given via needle. In this episode, a nurse practitioner linked their interest in BST to desperation for “solutions that don’t include opiates.” Similarly, in Goop’s “Cold Comfort” episode, the featured practitioner, Wim Hof, implied that psychiatric medicine was ineffective at preventing his wife’s suicide because it was impersonal. Instead, the solution of cold-water therapy teaches a lifestyle that is “a great way of learning to adapt to stress” built out of natural strengthening rather than chemical management.
This view that alternative treatments and lifestyles could improve health by leveraging biology was echoed by patients of psychedelics, breast milk, and fasting. For example, in UnWell’s episode on breast milk treatment, several men and women described breast milk as the most natural dietary supplement for adults. Similarly, Goop depicted physician-managed diet and wellness plans as natural because they leveraged pre-existing biology to improve health.
Frustration and Disenchantment
These themes were present in all but the two episodes on sexual health. Many expressed frustration that standard medicine could not treat specific physical or mental ailments. This dissatisfaction came from personal experiences where medical treatment actively failed to improve their condition. A similar dissatisfaction centered on healthcare’s inability to treat mental health or realize that psychological issues need non-pharmaceutical treatment.
One of the central customers in the bee sting therapy episode, Kerri, described her experience of being “chronically ill and [having] seen so many doctors over the years” leading to “being misdiagnosed for most of my life,” including a misdiagnosis of depression causing the prescription of antidepressants at the age of 9. Ultimately, the experience “made [her] lose a lot of faith in western medicine.” UnWell’s ayahuasca episode featured two participants, Lance and Angela, who experienced traumatic life events and difficulty finding adequate psychiatric care. Lance described his usage as a last resort. Angela used ayahuasca because “if everything else has failed, what do you have to lose?”
Personal Responsibility
“Taking care of yourself” was how a person could find a long-term resolution for dissatisfaction. In episodes that directly dealt with systematic issues like sexism, respondents shied away from addressing the institution itself. For example, when discussing sexual wellness, Paltrow stated that “shame pervades our sexuality.” Rather than address misogyny in all its forms, these cultural norms can be offset by “[allowing women] to be able to take control” by purchasing sex toys and attending sexual-wellness classes. Likewise, frequent indictments of “western society” as materialistic and atomizing were met with calls to alter behaviors and personal outlooks. While lamenting that “people don’t slow down and connect,” the practitioner interviewed in Goop’s “Energy Experience” episode located the solution as inward facing rather than addressing the systematic causes of this disconnection. In the “Cold Comfort” episode, Wim Hof implied his wife’s suicide was caused by psychiatry’s dehumanization, arguing that her recovery was hindered by a reliance on prescription medication preventing self-reflection. Likewise, a practitioner declared that by “taking healing into your own hands,” any issues caused by medical misdiagnoses can be overcome.
Medical Legitimacy
The legitimacy of the medical field was challenged in tense and contradicting ways. Science and medicine were consistently looked to for legitimacy even if it was understood as limited or harmful. Degrees were frequently used as a source of medical legitimacy, often deceptively. In one case, a water fasting clinic featured in the episode advertised itself as fully staffed by doctors and offering medical supervision. Instead, the founder of the clinic had a Doctorate in Chiropractic (D.C.), while the supervising practitioner had a Doctorate in Naturopathy (N.D.), neither of which a layperson would consider a “doctor.” Scientific research was often used to provide “proof” that a treatment is effective. When research is fledgling or vague, it is often said that science is “just catching up” to non-western knowledge. Conversely, two mediums complained that science would not legitimate their work.
Summary of Themes
While distinct, each theme was relatively free-flowing and interconnected with one another. Otherization melded smoothly into idyllic and romanticized beliefs of health and wellness, while this romanticism played a distinct role in shaping the frustration interviewees in Goop and UnWell felt. Drawing on centuries of colonial narratives, the “factual” comparison between “the West and the Rest” was foundational in diagnosing the malaise of modern healthcare experiences and presenting an alternative to the current treatment plans. This contrast between a romanticized, humanistic world that cares about the whole person and a modern, sterile world often resulted in an interviewee attempting to overcome their frustration with the system by “reclaiming” their humanity through 1. A reclamation of the perceived “lost” lifestyle(s) through a neoliberal, personal responsibility narrative, and 2. Attempting to make their ideas and treatment plans mainstream through the market.
Within the wider “common sense” of neoliberalism, otherization, and romanticism, the alternative treatments and wellness lifestyles featured in Goop and UnWell were not and could not be inherently superior to Western medicine, despite having benefits not awarded by the traditional medicine (Said 1978). The benefits of these treatments were their adaptability to the individual, both as an empowering, customized treatment and an option when Western tactics fail. In all cases, interviewees ultimately saw the solution to their health issues and issues with the system by altering their healthcare consumption habits.
Discussion and Conclusion
In this study, I examined how patients, practitioners, and researchers understand medicine, health, alternative medicine, and wellness lifestyles. Using a content analysis of Goop UnWell, I found five predominant themes: otherization, idyllic health, patient autonomy, frustration and disenchantment, personal responsibility, and personal responsibility. Interviewees in both shows used the themes to describe and navigate their relationship with medicine, ideas of what “optimal” health looks like, and beliefs on how these goals can be achieved. These themes were often interconnected, with otherization linked to ideas of idyllic healthcare. Notably, there was consensus on what each of these themes means between each group, reflecting that common sense “facts” are often unconstrained by demographic categories (Gramsci 1992). Though alternative medicine and wellness were the center of focus, medical, scientific, and pseudo-scientific language—language which uses scientific-sounding jargon but has no basis in science—was central to maintaining the legitimacy of their actions when discussing treatments, ailments, and efficacy.
These results provide two main insights into the ultimate goals of healthism: first, with standard, institutionalized medicine insufficient for fulfilling healthcare, the integration of alternative health and wellness care provide a more comprehensive approach to health. Mental health was seen as a crucial part of physical health and worth pursuing in its own right, something seen as ignored by conventional healthcare. Medicine was “known” to be woefully incapable of addressing psycho-social maladies, primarily because it is fundamentally anchored to the corporeal realm; without direct, material observation, an association between an illness and a psychological state cannot be developed. Practitioners and patients alike believed that Other cultures offer a path to mental health and well-being through a reconnection with the self and a genuine human experience that medicine lost. As Derrida said, metaphysical (mental) health is based on the contrast between western values and Other cultures (Derrida 1995). Successful healthcare, which incorporates mental health, necessarily involves the assimilation of Other cultures and ideas.
It was taken as a “fact” by patients, practitioners, and researchers in Goop and UnWell that medical treatments were impersonal and incompatible with the nuances of a person’s unique healthcare struggles. Discussions of empowerment and responsibility were rooted in common sense ideals of individual action based on individual context. Amplifying the metaphysical rigidity of medicine, the supposedly statistical strictness of scientific and medical research made interviewees feel dismissed outright by their physicians when seeking to incorporate new treatments or adapt existing treatment holes. In a way, this is not a baseless claim as the standard evidence-based medicine requires statistical significance and other measures of efficacy before it is incorporated into medical training and more comprehensive treatment plans—recall the definition of “alternative medicine” mentioned above is simply treatments not taught in medical school.
Though seen as numb to human needs, interviewees did not see medicine as fundamentally flawed. On the contrary, although western society and western medicine are unreasonably materialistic and rigid, the willingness to accept usefully (i.e., verifiable) science into the canon redeems the deficiencies. Indeed, this begrudging flexibility gave some hope to patients and practitioners while being a source of frustration that the alternative treatments would eventually become mainstream. Likewise, despite being depicted as the antipode of Western life, most interviewees believed that the treatments used by Other cultures are compatible with standard medicine or western society. We see this most clearly in research on CAM usage in cancer patients: patients often see CAM as compliments to an effective treatment to assist with side effects and pain (Ben-Arye et al. 2013; Johnson et al. 2018).
Here we see the second insight: alternative health and wellness can bring wider healthcare change through market forces. The market-as-reformer has been essential to the larger Fukuyama-esque “end of history” neoliberal common sense (Fukuyama 1989). With no alternative beyond the neoliberal market system, the market becomes the forum through which discontent is aired and mediated (Harvey 2011). For this reason, Other forms of knowledge were usable to Westerners featured despite fundamentally challenging Western life. This co-optation occurred by adopting treatments and lifestyles piecemeal, utilizing portions highlighting individual well-being and self-reflection while tossing collective (economic, political, and social) messages.
It is important to note that there are real undercurrents of anti-capitalist, anti-neoliberal ideologies throughout the interviews: beliefs that the profit motive undermines medical interests and Western “materiality” (i.e., economic life) is incompatible with personal fulfillment. A contradictory phenomenon of market-based solutions to (surface-level) challenges to Western life, and anti-neoliberal challenges have resulted in haphazard reforms within medicine. Instead, the knowledge that science is somewhat malleable and that there are no real alternatives beyond neoliberal political economy work to refocus these ideas of discontent into consumer goods and services. Indeed, we see the main benefit of the market is that while the medicine is limited and restrictive, the individual is free to maximize their health through educated purchases. While physicians, pharmaceutical companies, and insurance companies may limit outcomes, the only (theoretical) barrier in the market is you. For this reason, almost all patients interviewed were incredibly knowledgeable about their ailment and the benefits/drawbacks of the various treatments available for it. A similar phenomenon exists for vaccine-hesitant parents, with parents refusing or limiting vaccines having conducted more self-education on the subject than those complying with the scheduled (Attwell et al. 2017).
The political-economic discontent expressed in the episodes is firmly placed within the confines of healthcare and the market. Though patients and practitioners are usually seen as existing in “opposing teams,” there was relative unity in how patients, practitioners, and scientists diagnosed the “problems of healthcare.” Compounding beliefs of CAM’s potentially effective treatments, interviewees in Goop and UnWell often stated that health consumption tertiary to the regulations and practices of standard medicine improves their health. As Davies argues, under neoliberalism, medical care has increasingly been used to isolate social problems, turning them into issues of brain chemistry (Davies 2017). Indeed, as early as the late 1990s, anti-depressants were used in Argentina to manage dissatisfaction with the onset of neoliberalism (Lakoff 2004). Foucault and others argue that the state uses such political forms of medicalization to accumulate “power” (Foucault 1994; Foucault, Senellart, and Foucault 2010). This, however, assumes that power exists for power’s sake, insufficiently describing phenomena like healthism and standard medicine existing to complement each other (Ahmad 2008). Like Orientalism, a hegemonic knowledge exists regarding medicine within the hegemonic narrative of neoliberalism: a nesting doll of “facts.” Though medicine can have its deficiencies, in the final instance, it remains superior.
As researchers, we are confronted with a new issue: how do we examine the fragments of a political discontent movement obfuscated by individualist patient actions? This question has somewhat evaded researchers. When examining vaccine-hesitant parents, who often express distrust of corporations and the government, researchers often depoliticize their findings by simply explaining that hesitancy is caused by misinformation (Dubé et al. 2013). This search for empiricism has the accidental consequence of further distancing the scientific community from the wider populace by labeling political movements as irrational (Hall 2017). Though practitioners and patients desire to be adopted by the medical community and remain in the “official” market, as we have seen, such treatment can have the impact of further entrenching ideas that the industry is profit driven and rigid. This can pave the way for opportunists to enter the alternative healthcare market, capitalizing on a layperson’s understanding of health and the human experience.
These findings should be seen as a demonstration of the political nature of medicine. While it is well understood that medicine can be structurally political, we should begin recognizing the importance of our economic and political reality in forming our common sense (Foucault 1994; Gramsci 1992; Illich 2016; Zola 1972). Though muddled, a popular conception of the institutions, how to navigate within them, and their usefulness exists, informing the actions of a significant portion of the population. Understanding what medicine is (and is not) is essential in tracking changes within the medical system. Additional research expanding the underlying political and collective understandings of medicine will be helpful in combatting public health issues that have been hard to approach.
Limitations
Several factors limit this study. Firstly, the sample size of twelve episodes is relatively small. Goop and UnWell have a dearth of episodes compared to other wellness education programs. For example, the health and wellness talk show The Doctors has fourteen seasons, with seasons often exceeding one hundred episodes (IMDb Staff 2008). Further, most health and wellness programs are in a talk show format, covering topics with different guests and new information several times. Goop and UnWell are limited-series programs and are unable to revisit topics.
Additionally, Goop’s and UnWell’s biases are more overt than syndicated or other shows, as they do not have to worry about advertiser pressure compounding studio demands. These competing interests often force shows writ large to be less “polarized” towards one side or the other—one can see admissions by former showrunners that their studio forced them to suppress a gay relationship until the series finale as proof (Johnson 2020; Millman 2020). Netflix’s reliance on subscriptions rather than advertising dollars has led to a relatively pro-controversy censorship system at the company (Tassi 2022). The profit motive in the studied shows more overtly, especially Goop. While Goop does not market its products explicitly, the topics and treatments shown broadly promote its brand identity and legitimate the products offered and the “ lifestyle” that comes with them. Notably, “outside” commentaries did not portray negative experiences with the treatment. Likewise, UnWell allows the treatments and companies showcased to promote themselves with relatively little pushback. Both shows, thus, suffer from false balance. UnWell represents all treatments within the “marketplace of ideas,” where it will ultimately be up to the viewer to decide what is best for them, while Goop makes no such apologies.
While these limitations color what can be inferred from the shows, this does not inhibit our ability to elucidate the neoliberal ideology reproduced. Hegemonic ideology is reproduced in all but the most critical media. Therefore, it is crucial to explore how topics, products, and treatments are understood by people, even if the fulcrum is artificially placed. To overcome the limitations discussed, further research should be conducted to examine how neoliberalism is reproduced in syndicated shows compared to limited series like Goop.
Footnotes
Acknowledgements
I want to thank Dr. Naomi Rosenthal, Dr. Kristen Shorette, and Dr. Jamie Sommer for their insightful feedback during the creation of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.