
Abstract
Individuals with intellectual and developmental disabilities (IDD) are at greater risk of health-related issues due to obesity and lack of physical activity. This study examined using virtual reality (VR) exergaming to increase the physical activity of high school students with IDD. Four students participated in this multiple probe across participants design. Data were collected on each student’s total amount of time engaged in exercise and heart rate. Results indicate that all students increased the duration and intensity of their physical activity when using the VR exercise gaming (exergaming) intervention. The VR exergaming intervention increased the duration and intensity of the students’ exercise sessions. Results are discussed in terms of applying VR and other emerging technologies to support the exercise health needs of the individual in the study.
The prevalence of individuals with intellectual and developmental disabilities (IDD) among the general population is approximately 6.5 million people in the United States and 1–3% globally according to the American Association of IDD (Schalock et al., 2010). Severity levels (i.e., mild, moderate, severe, and profound) are based on the intelligence quotient score criteria and impairments seen before the age of 18 (American Psychiatric Association [APA], 2013). People with IDD include those with impairments of general mental abilities that impact adaptive functioning in three domains: conceptual, social, and practical (APA, 2013). Conceptual skills involve language and literacy, social skills involve interpersonal and social responsibility, and practical skills involve activities of daily living and personal care (APA, 2013).
In addition to the cognitive and perceptive limitations that can be experienced by individuals with IDD, their disability can put them at an increased risk for several health complications. Jansen, Krol, Groothoff, and Post (2004) conducted a review of studies comparing health issues between those with IDD and the general population and found that individuals with IDD are more likely to have diagnosed health problems, compared to the general population. These health problems can potentially have serious consequences on the lives of people with IDD. One particular health problem often reported in individuals with IDD is obesity, a health condition that is linked to an increased risk of coronary heart disease and other secondary health concerns for example high cholesterol (Eckel & Krauss, 1998). The Centers for Disease Control and Prevention (2014) report 19.8% of youth with an intellectual disability and 31.8% of youth with autism are obese, compared to 13.1% of youth without IDD. These findings are similar to other studies investigating the prevalence of obesity in youth with IDD. Lloyd, Temple, and Foley (2012) reported an overweight range from 4.1% to 26.3% and an obesity range from 4.6% to 32.6% in youth with IDD (N = 9,678). These results are comparable to other studies (Maiano, 2010; Rimmer, Yamaki, Lowry, Wang, & Vogel, 2010) that found a high prevalence of obesity in youth with IDD and concluded that obesity is a serious health concern for this particular population.
Leading a sedentary lifestyle is likely to be a major contributor to becoming obese and other health concerns. Most youth with IDD are not exercising on a regular basis, whether individually or recreationally (Rimmer et al., 2010). Rimmer, Rowland, and Yamaki (2007) suggest that a lack of access to a physically active lifestyle is one reason why youth with IDD are generally inactive. This includes inappropriate sports and fitness equipment, inaccessible fitness facilities and recreation areas (e.g., playground), and inexperienced staff lacking the knowledge to adapt fitness programs to meet the needs of youth with IDD (Rimmer, Rowland, & Yamaki, 2007). Another issue is the lack of knowledge or awareness of how to adopt a healthy lifestyle among youth with IDD (Rimmer et al., 2007). Clearly, physical activity–related interventions are needed that address these barriers to help lower obesity and improve the overall health in youth with IDD.
Numerous studies have shown that physical activity is a key factor in preventing health problems that result from leading a sedentary lifestyle and can positively impact the health, fitness, and behavior of adults and youth with IDD (Messent, Carlton, & Long, 1998; Rimmer, 1999). These studies have included various types of exercise such as aerobic physical activity (e.g., brisk walking) to resistance training programs (e.g., weight training; Khalili & Elkin, 2009; Shields & Taylor, 2010). For example, one study implemented a walking intervention on a treadmill for youth with IDD (N = 15) for 2 months, and results demonstrate a significant improvement in physical fitness (Lotan, Isakov, Kessel, & Merrick, 2004). While other studies show similar results concerning physical activity–related interventions (Carter et al., 2004; Stanish, Temple, & Frey, 2006), more research is needed that promotes youth with IDD to be active and address barriers associated with inactivity.
One method that is increasingly being utilized by researchers and practitioners to promote physical activity among youth with IDD is exercise technology interventions. These exercise technology interventions can include the use of virtual reality (VR) mobile or wearable devices, which can provide an immersive environment to engage users in a variety of games and 360° video experiences (Burdea Grigore & Coiffet, 1994). VR is a type of immersive technology that displays a fully artificial environment generally through the use of a dedicated set of goggles (Migram & Kishino, 1994). VR is separate but related technology to the immersive technology of augmented reality (AR) in which digital information is overlaid on a view of the real world.
The use of VR has previously been shown to benefit cognitive performance and social skills for youth with IDD, likely due to providing an inclusive environment and the ability to manipulate virtual worlds to resemble real-world settings (Standen & Brown, 2005). As a result, VR is now being investigated and implemented as a means to promote physical activity for those with IDD. For example, Lotan, Yalon-Chamovitz, and Weiss (2009) explored a 5- to 6-week VR exercise intervention aimed at improving the physical fitness for adults with IDD. Pre- and posttests of physical fitness indicators, such as energy expended and heart rate, showed significant improvement in the research group, compared to the control group (Lotan, Yalon-Chamovitz, & Weiss, 2009). These results are similar to a follow-up study that demonstrated significant improvement in pre- and postphysical activity measures in adults with IDD, compared to the control group following the completion of an 8-week VR physical activity–related intervention (Lotan, Yalon-Chamovitz, & Weiss, 2010).
Furthermore, Yalon-Chamovitz and Weiss (2008) report that VR physical activity–related games are perceived as enjoyable and successful by adults with IDD. The authors also reported that the participants enjoyed how there were different VR game options and how they could be adapted and modified to meet their individual needs (Yalon-Chamovitz & Weiss, 2008). VR games investigated in the study included “car racing” where the participant is the driver of the car and has to pedal in order for the car to go (Yalon-Chamovitz & Weiss, 2008). It appears that VR is a feasible method that can provide a safe environment that encourages adults with IDD to participate in levels of physical activity that are often not seen in this population (Lotan et al., 2010; Yalon-Chamovitz & Weiss, 2008). Additionally, McMahon and McMahon (2016) conducted a systematic review of the research literature of exercise technology interventions for individuals with IDD. The review identified only nine articles where the technology interventions were used to increase exercise and only four of those fit the definition of exergaming activities to promote physical activity (e.g., Weiss, Bialik, & Kizony, 2003). Overall, the review found that these studies reported increased motivation and improved physical activity indicators (McMahon & McMahon, 2016). However, many of the articles were pilot studies and involved adults with IDD. None of the studies included interventions using immersive wearable VR headsets to support exergaming for students with IDD.
The rationale for this study was to investigate the use of an immersive VR exergaming as a means to increase the duration and intensity of exercise sessions for youth with IDD. Research on new technology platforms is essential in order to establish an evidence base for their use with any population. This study addresses the need for additional exergaming research for individuals with IDD by examining a new platform of VR exergaming to support youth with IDD to be more physically active. As mentioned previously, the majority of the literature regarding exergaming and individuals with IDD has predominantly focused on adults with IDD. This research study examined how VR exergaming can help youth with IDD to exercise and contribute to the small, yet growing, body of literature. Addressing this particular gap in the literature can help further our understanding of how technology interventions can help youth with IDD be more physically active. VR exergaming is a new tool that can provide adaptable, inclusive, and modifiable physical activities, which could address certain barriers this population can experience, such as inaccessible exercise equipment, transportation, and motivation. It is also important to note the importance of implementing physical activity behaviors in early adolescence, rather than adulthood, among youth with IDD. Rimmer et al. (2007) describes adolescence as a “window of opportunity” for youth with IDD to adopt healthy, physical activity behaviors that can be carried into adulthood. VR exergaming could be one innovative method of instilling these physical activity behaviors in youth with IDD. While there is ample evidence that supports traditional exercise (e.g., walking; Johnson, 2009) as one way to increase physical activity among youth with IDD, VR exergaming is a new platform for physical activity that could prove to be an effective tool to increase physical activity. To determine whether VR exergaming can influence the physical activity levels in youth with IDD, this study examined the following research questions. Can a VR exercise game designed to promote physical activity as measured by an increase in the duration of an exercise session and calories burned for students with IDD? Additionally, does the VR exergaming have social validity for the students and their teachers who participated in the study?
Method
This study utilized a multiple probe across participants design for four students with IDD to determine whether a VR exercise game intervention can promote them to be more physically active during an exercise session. Physical activity indicators collected included the duration of the exercise, heart rate, and calories burned during the exercise session. Interobserver agreement (IOA) and procedural reliability were calculated as well and discussed in subsequent sections.
Participants
Emma was a 14-year-old female student diagnosed with fetal alcohol syndrome. She was interested and excited about technology but did not enjoy exercising. Emma was a new student at Sunnyside High School this year, and she was beginning to get acclimated to the high school experience. Emma was a young woman whose height was 5′5″ and she weighed 166 pounds at the time of the study.
Charlie was a 17-year-old male student diagnosed with autism spectrum disorder. His level of functioning was moderate but struggles with communication, social skills, and some repetitive behaviors (i.e., words). Charlie was interested in technology and exercising. He was part of the swim team at the time of the research and enjoyed videos on the computer. At the time of the study, his height was 5′8″ and he weighed 140 pounds.
Andrew was a 16-year-old male diagnosed with Down syndrome. He was enthusiastic about sports but did not enjoy riding the stationary bike when the study began. Andrew had been an active member of the wrestling team and was the manager of the football team. At the time of the study, Andrew’s height was 5′5″ and he weighed 183 pounds.
Henry was a 21-year-old male student diagnosed with intellectual disability and other health impairments (i.e., breathing, feeding). Due to his health issues, Henry’s exercise regimen was limited to walking for a short period of time or riding a stationary bike during his physical therapy once in a while for no more than 10 min. He was not very interested in technology at the start of the study. Henry’s height was 4′11″, and he weighed 100.6 pounds at the time of the study.
Setting
The setting for this study was a high school in the Pacific Northwest. Students were all in a transition special education classroom where students have classes in this self-contained classroom, but they go on outings in the community. Some of these outings include exercising, employment in the community, and shopping. During the data collection by the researchers, students in this study were taken to a quiet meeting room at the school for the baseline and intervention sessions. Testing the students in a quiet area helped to prevent peer positive or negative reinforcement from influencing the study. The stationary bike seat was adjusted to the preferred height of the users before each session.
Materials
The VR exercise gaming platform used was the Virzoom exercise bike and the HTC VIVE VR googles (Vive.com, US$499). The Virzoom (Virzoom.com, US$399) platform allows people to use a specially made stationary bike as a controller for a variety of VR games. For example, the faster the individual pedals on the stationary bike, the faster the vehicles in the game (race car, horse, helicopter, bike, Kayak) will go. As the user pedals the bike, they can look around themselves using the VR headset to see a 360° view of the interactive game world around them. The Virzoom bike has variable levels of resistance on a scale of 1–10. Because of the low initial levels of exercise reported by the students and their educators in discussions with the researchers before the start of the study, it was decided by the researchers that an appropriate low moderate resistance level of three would be a suitable level. The bike and headset were adjustable to fit the users’ individual sizes. The Apple Smartwatch, Version 2, was used to measure the heart rate of the student participants and to measure the duration of the exercise session.
Variables and Data Collection
Time
For all sessions, the amount of time engaged in the physical activity of using the exercise bike was measured. The maximum allowable time per session was set at 30 min for both baseline and intervention. This was selected because it is minimum amount of moderate physical activity recommended by the 2008 Physical Activity Guidelines for Americans (Physical Activity Guidelines Advisory Committee, 2008). Time was kept on the smartwatches worn by the students while they participated in the activity. Students were told to they were participating in an exercise session that could last as up to 30 min. They were told to say “I’m done” when they wanted to stop.
Heart rate
The participants’ average heart rate during the sessions was measured by the smartwatches worn during the sessions. The smartwatches used in the study were Apple Watches. While many wearable devices have limitations on their ability to accurately measure energy expenditure (EE; calories burned) including the Apple Watch, they have a high degree of accuracy for measuring heart rate (Wallen, Gomersall, Keating, Wisløff, & Coombes, 2016). El-Amrawy and Nounou (2015) compared several popular fitness trackers and found for heart rate the Apple Watch was one of the most accurate tested. The average heart rate was recorded at the end of the session.
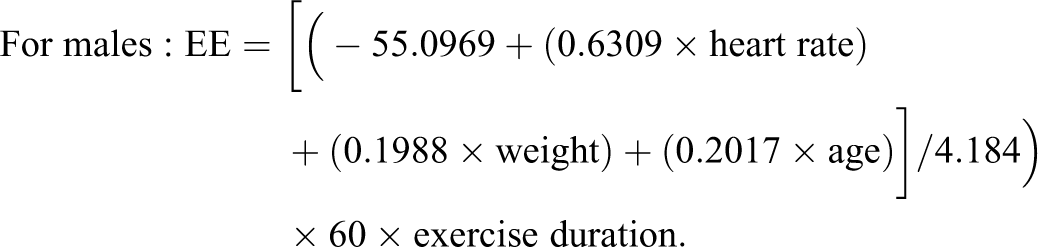
Calories total
Total calories burned for each participant session were calculated by estimating physical activity EE from heart rate, after adjusting for age, gender, and body mass (Keytel et al., 2005). The EE prediction equation can also account for when the individual’s measure of fitness is unknown and yields predictions that correlate significantly with testing samples and independent validation samples (r = .857). Using the heart rate data from the smartwatches and the age and weight data for the participants, the total calories burned were calculated for each participant in the EE prediction equation. Heart rate is in beats per minute (BPM), weight in kilograms, age in years, and exercise duration in hours.
Procedures
Baseline
During baseline, each participant completed a minimum of three exercise sessions on the stationary bike. Students were asked if they wanted to ride the bike, and if they said yes, they were told they could ride for as long or as little as they wanted up to a maximum of 30 min. Students were instructed to say “I’m done” when they wanted to stop. No additional feedback or prompts were provided.
This process occurred for a minimum of three sessions until the data were considered stable. Stability was determined using the “80%–20%” criteria of the stability envelope (Gast, 2010). If 80% of the data points fell on or within 20% of the mean of baseline, the data were considered stable. During baseline, participants wore a smartwatch that was used to measure the duration of their exercise and their heart rate.
Intervention
After the participants’ baseline sessions, the intervention was started with the first participant. During the intervention phase, the students used the VR exercise game Virzoom for as long or as little as they wanted up to a maximum session length of 30 min. Just as in the baseline phase, students were instructed to say “I’m done” when they wanted to stop. The first game for each session was a race car game called Go Fast Car, where individuals pedal the Virzoom Stationary bike to make the car accelerate around the track. In the game, individuals can look around from the point of view of a race car driver as they compete against the computer. If students chose to complete the race car game by finishing five laps around a track, the students were allowed to play a different virtual game called Kayak. In the Kayak game, users explore a pond and find ducks. Once they collected 20 ducks, they could choose to move on to a bike race game. Each one of these games if played to completion lasted between 8 and 10 min. Students were able to navigate the menus easily and quickly less than 20 s between games. The principle investigator and a member of the research team were beside the participants and able to view the students in game experience on the computer screen. An example of this is shown in Figure 1.

Virtual reality (VR) exergaming setup including bike, VR headset, computer, and display for the research member to monitor.
Research Design
A multiple probe across participants design (Gast & Ledford, 2010) was used to examine the relation between the VR exercise intervention and each participant’s performance. The VR intervention was introduced systematically across the participants. After the first participant reached criteria of at least three consecutive data points of improved performance from baseline, the second participant began the intervention phase. This continued until all four participants completed the intervention. The study was concluded when experimental control could be assessed across the different participants (Horner et al., 2005, p. 168).
IOA and procedural reliability
The researchers simultaneously collected IOA and procedural reliability data. IOA data were collected during a minimum of 50% of baseline condition and treatment condition for each participant. Observers simultaneously recorded the data including time and heart rate from the smartwatch. IOA was calculated by dividing the number of agreements of the participant responses by the number of agreements plus disagreements and multiplying by 100. IOA was 100% for each participant across all phases.
Procedural reliability data also were collected during a minimum of 25% of all sessions for baseline and intervention for each participant. The procedural agreement level was calculated by dividing the number of observed researcher’s behaviors by the number of planned investigator’s behaviors and multiplying by 100. The procedural reliability was 100% for all students across all conditions.
Data Analysis
Visual analysis procedures were used to evaluate the results of the VR exercise intervention. To assess intervention effects, six indicators were used to examine within-phase and between-phase data patterns: (a) level, (b) trend, (c) variability, (d) immediacy of the effect, (e) overlap, and (f) consistency of data patterns across similar phases. Also, within-phase comparisons were evaluated to assess predictable patterns of data, data from adjacent phases were used to assess whether manipulation of the independent variable was associated with change in the dependent variable, and data across all phases were used to document a functional relation (Gast, 2010). Horner et al. (2005) recommended that a functional relationship or causal relationship is demonstrated after at least three occurrences of an effect at a minimum of three different points in time are observed. For each participant, the percentage of nonoverlapping data (PND) was calculated between the baseline and intervention phases (Scruggs, Mastropieri, & Casto, 1987). Scruggs and Mastropieri (2001) suggested interpretational guidelines of PND were used to evaluate the effectiveness of the intervention. Based on their guidelines, this study evaluated PND greater than 90% as a highly effective intervention, PND greater than 70% and less than 90% as an effective intervention, PND greater than 50% and less than 70% as questionable effective, and PND less than 50% was considered unreliable effectiveness for interventions.
Social Validity
The social validity of an intervention for the students is an important factor to measure for new interventions (Wolf, 1978). The purpose of this study is to give students access to an alternative mode of exercise and physical activity that would hopefully lead to socially meaningful outcomes. Since VR and exergaming are emerging technologies, understanding the social validity and user experience can inform this exploratory research. At the conclusion of the study, students were asked about their experience of using the VR exergame. Educators who worked with the students were also asked about the experience to provide additional points of view about the intervention.
Results
Baseline data for the students indicated that the students had very low initial time of exercise and total calories burned on the stationary bike. The VR exercise bike intervention was implemented with each participant in succession, as they demonstrated the criteria of three consecutive sessions of improved performance. Figure 2 provides a graphic representation of the results of the single-subject research study for all four students (i.e., Emma, Charlie, Andrew, and Henry). Visual analysis of the baseline and intervention levels for the students shows the invention increased the time of exercise and the related variable of total calories burned. The trend for all four students shows an overall upward trend of increased time and calories burned once the intervention began. The variability was limited as shown by stable baseline data and the intervention data being closely aligned along the increasing trend line. All four students’ data demonstrate a strong immediacy of the effect, limited to zero overlap, and a high degree of consistency of data patterns across similar phases. Individual student results are presented below.
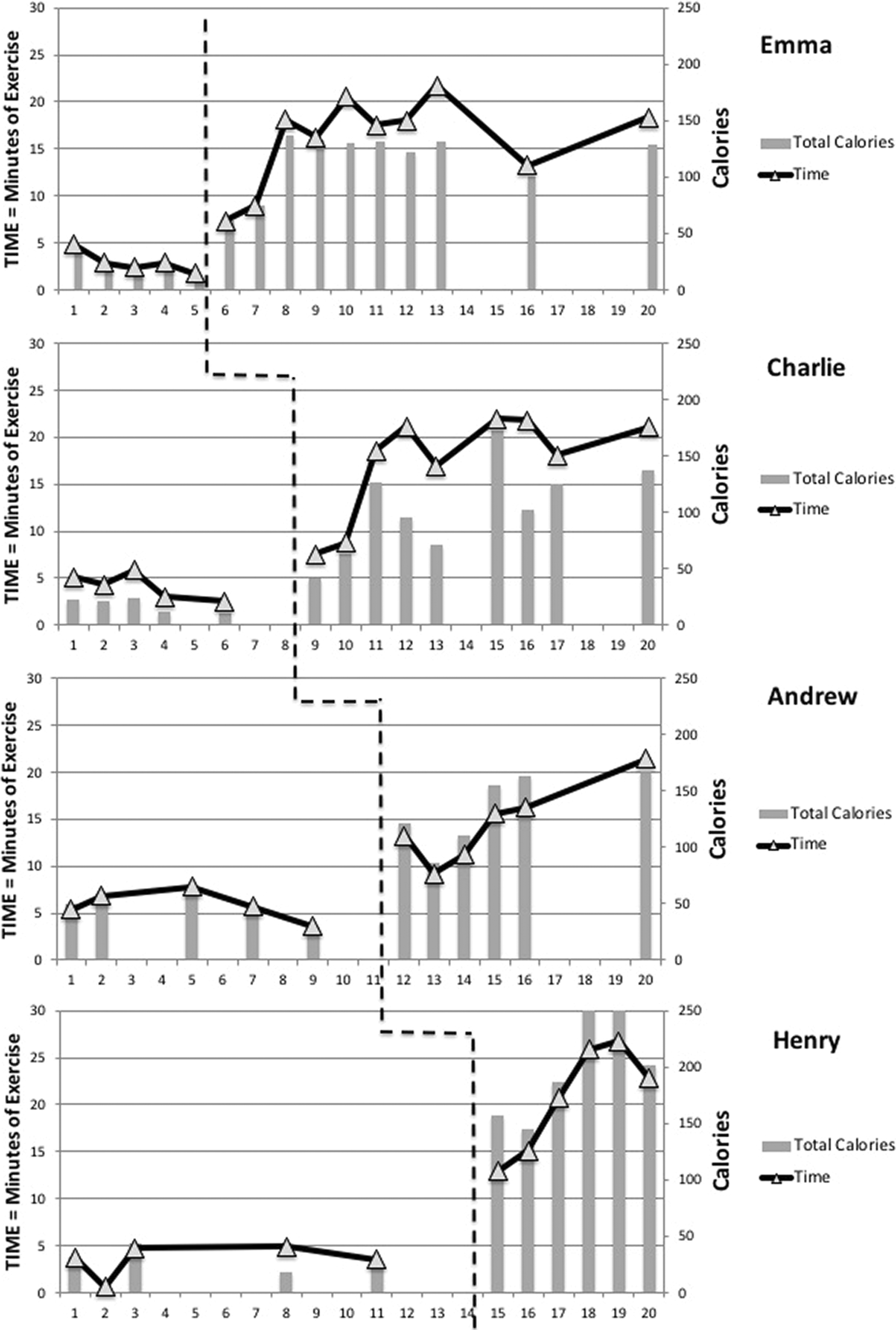
Results for the virtual reality (VR) exercise gaming multiple probe across four participants. Data show that VR exercise gaming was effective for increasing exercise duration and total calories burned.
Emma
During baseline, Emma had an average of 2 min 57 s of exercise on the stationary bike. Her average total calories burned per baseline session was 27.8, and her heart rate average was 128.4 BPM. During the VR exercise intervention, her total time of exercise on the stationary bike increased to an average of 16 min 01 s. Her total calories burned per session increased to 182.83, and her average heart rate was 133.5 BPM. Her PND for the total time engaged in exercise was 100%, and her PND for the total calories was also 100%.
Charlie
Charlie’s baseline exercise on the stationary bike had an average of 4 min 09 s with an average of total calories burned of 29.4 and a heart rate average of 91.2 BMP. During the intervention using the VR and stationary bike, his average was 16 min 51 s with 135 total average calories burned and 101.5 BPM as average heart rate. Charlie’s PND for the total time engaged in exercise on the stationary bike was at 100% and his total calories burned.
Andrew
A total average of 5 min 49 s was Andrew’s baseline for his exercise on the stationary bike. He had a baseline of 48 total calories burned and a heart rate average of 113.6 BPM. His average exercise minutes during the VR stationary bike increased to 17 min 22 s. In addition, his total average calories burned increased to 136.6, and his heart rate average was now 118.17. Similar to all other students, his PND was 100% for both his average exercise time and his average for total calories burned.
Henry
Finally, Henry’s total average exercise on the stationary bike was 3 min 30 s for the baseline. His total average calories burned were 29.25, and his heart rate average was 113.8 BPM during baseline data collection. During the VR intervention, Henry increased his total average exercise minutes to 20 min 41 s, his total average calories burned to 181.8, and his heart rate to 131.33 BMP. His PND was 100% for his average exercise minutes on the stationary bike as well as his total calories burned.
Social Validity
The participants and their educators (teacher and paraprofessional) were asked about their experience during the intervention. All of the students indicated a strong preference for the VR exergaming session condition. Social validity was used to determine how the student felt about this novel immersive VR gaming experience. One of the potential concerns by the researchers was the possibility for the students to feel uncomfortable, disoriented, or scared by the VR session. The social validity results from the students were brief, despite efforts to get them to elaborate more. The comments from the teacher and students were positive in their view of the VR exergaming (see Table 1).
Social Validity Questions for Students and Teachers.

Note. VR = virtual reality.
In addition to the student and teacher comments, the teacher shared that All of my students loved wearing the VR gear and participating in the games that went along with it. Once the research was over, they were not very interested in only riding the stationary bicycle. They loved the VR part and only participated in the cycling part because it was required to make the game work. If the VR gaming system was more affordable and easier to use and set up, I think it would a valuable tool to use in the classroom as a behavior incentive and also for exercise.
Discussion
This study supports previous findings that exercise technology interventions can be used to increase the physical activity of individuals with IDD. This study extends the previous research by examining a new exergaming platform using the immersive technology of VR. The findings show that VR exergaming can be an additional tool to support increasing the physical activity of individuals with IDD. This study demonstrated a functional relation between the intervention of VR exercise games and increased duration of exercise for all four participants with IDD. The VR intervention at least tripled their total amount time engaged in physical activity per session compared to the baseline condition. The participants were in fact eager to use the exergaming system throughout the duration of the study.
Importance
Research demonstrates that individuals with IDD are more likely to have health-related challenges due to obesity, lifestyle factors, and genetics (Eckel & Krauss, 1998; Janicki et al., 2002; van Schrojenstein Lantman-de Valk, Metsemakers, Haveman, & Crebolder, 2000). Regular exercise is one way of addressing these challenges for individuals with IDD. However, for individuals with IDD, starting and staying active in regular exercise is an ongoing problem. The ability to go to the exercise facility or place of interest for participating in physical fitness is a limiting factor (Rimmer et al., 2007). Facilities are often not equipped to readily handle individuals with IDD and associated physical challenges. At the same time, easy transportation to “fitness centers” or gyms can be challenging. This is compounded with an overall lack of continued interest. Beginning, maintaining, and advancing through fitness regimens is difficult for most people. Activities that are considered boring, uneventful, and routine make ongoing motivation extremely difficult for individuals with or without IDD. It is not surprising, then, that Heller, Hsieh, and Rimmer (2004) found that after a 6-month follow-up, 87% of the participants with Down syndrome had stopped with the exercise regime.
Exercise technology interventions such as exergaming are one promising way to increase the amount and intensity of exercise for individuals with IDD. The use of VR in exercise acts to mitigate several potential barriers. The interactive game features provide engaging interactive activities, challenges, and encouragement that increased the physical activity of the participants.
With the incorporation of VR exergames, exercise becomes an interactive experience that can utilize various components of gaming to enhance the experience and encourage more long-term activity. Rewards, challenges, immersive experiences, and the ability to choose different environments and activities work to keep participants interested and engaged in exercise. For participants with IDD, this type of activity can act to bridge the various gaps that prevent them from continuing in directed or individual exercise programs.
This study provides important implications for practice when using VR exergaming to increase the duration and intensity of physical activity for students with IDD. This system was implemented as a portable system that had to be set up and broken down repeatedly because of the space limitations at this school. It would be much easier to install it as a permanent resource in a school or gym. The cost of the system (US$1,500–US$2,000) also probably makes it a better fit for a shared use at a facility rather than an individual’s home. A fixed installation of this system would eliminate the setup and calibration time and allow for greater independent use of the exergaming by the student with IDD. Just as many schools have designated spaces in a classroom to support calm down, sensory, or other needs, this system could facilitate an exercise outlet inside of the classroom. VR exergaming is another potential tool that educators could implement to support students with IDD. VR exergaming could provide an outlet for physical activity similar to taking a walk without having to leave the classroom. Taking a walk is a common behavior regulation strategy to help students who need an outlet for physical activity or to get break from a trigger in the classroom. For classrooms with a limited staff of teachers and paraprofessionals, taking a student for an exercise break out of the classroom often means one less adult in the classroom and lost instructional time. This system could provide that exercise outlet without requiring the student and a staff person to leave the classroom. The VR headset provides an immersive visual and auditory experience that can redirect them from other classroom distractions.
In addition to school or gym settings, VR exergaming could be implemented in the home for adults with IDD. Many adults with IDD have limited transportation options, which may become a barrier for exercise. An in-home VR exergaming system like the one in this study could therefore eliminate the transportation barrier. The cost of implementing this VR exergaming system at the beginning of the study (approximately US$2,000) has already decreased to approximately US$1,000. Because of the rapidly dropping price of this type of technology, it is now comparable to the price of other “at-home” exercise equipment. For individuals with IDD and their caregivers, it is readily available for home use. These changes help to address the challenges of cost and setup that were identified by the student’s teacher.
Limitations
Although this study indicated positive outcomes, results must be interpreted within the context of this study and several limitations need to be considered. For example, the intervention’s VR system (HTC Vive, VR capable computer, and Virzoom exercise bike) used in this study represent a fairly new and still financially expensive intervention. The Virzoom bike costs US$399, the HTC Vive costs US$799 at the time of the study but is now under US$500, and VR capable computer was over $1,000. This particular game system was very accessible to the users and included many examples of multiple means of representation that helped the users select their interactive workout programs (i.e., the race car game had icons for a race car in additional to words). The game’s menus were easy for the students to navigate and select. Accessibility could be a limitation in other platforms and will need to be assessed as a barrier in future interventions. The initial setup of the system (VR headset, computer, bike, and calibration) takes about 10 min. The participants in this study did not have to set up the system on their own and would not be able to complete this independently without significant practice.
The study did not include a maintenance phase, and future studies should include a maintenance phase to measure the longer term effects of the intervention. In addition, like similar to other single-subject design studies, only a small number of students participated. Future research could recommend larger number of participants in the study to enhance generalizable findings. This study did not compare this intervention against multiple types of traditional exercise. Future research could compare this intervention against two or more other forms of traditional exercise in an alternating treatment design. I would not put the characteristics of participants as a limitation either. In this study, the intervention continued on a set selection of games (race car, Kayak, and bike race), but a more open free play option could be more engaging and motivating for some individuals. Future research could also recommend replicating this study with other populations. The small size makes it difficult to generalize the results to a broader population of students with IDD. This study requires replication across a larger number of participants, ages, and types of disabilities.
Future Research
Future research is needed related to examining the potential of VR exergaming to support the needs of this population. This example of exergaming required the use of an exercise bike, but many other VR exergaming examples are available. Future studies could examine other exercise games such as rowing machine-based games or some of the many room scale VR games using handheld controllers in which users dodge, duck, and jump as they interact in the VR game. Future studies with a longer duration could examine the weight loss effects of the VR exergaming interventions. Also, it is worth noting that while the Apple Watch was only used as a data collection tool, the participants were very interested in checking their progress at the end of each session on the watch. Future research could explore the effects of using a smart watch to self-monitor physical activity for this population. This line of research could examine the effectiveness of using a wrist-worn activity measurement tool throughout the day for individuals with IDD and determine if there are implementation or accessibility barriers to be addressed. While this study was focused on exercise interventions, immersive VR experiences also have potential academic applications that need to be examined. VR exergaming is by its nature going to be in a fixed location because you cannot safely cross a street in a VR headset looking at virtual world, but this is not true of all immersive technologies. Future studies could compare VR exergaming options to other related but separate immersive technologies such as AR. AR exergames allow for additional opportunities in public spaces such as parks and other community spaces. Finally, future studies should compare the effects of VR exergaming to traditional exercise promotion interventions such as a group fitness class.
Conclusion
VR exergaming demonstrated a functional relation to improved exercise duration for the participants in this study. This is a promising tool to help students with IDD achieve the physical activity recommended guidelines (Physical Activity Guidelines Advisory Committee, 2008) of a minimum daily amount of 30 min of moderate physical activity. VR exergaming is an emerging technology that will continue to evolve as new exergames become available. Future research needs to explore how VR exergaming can support physical activity and exercise for people with IDD to help individuals with IDD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.