
Abstract
Young adults with intellectual and developmental disabilities (IDDs) are at an increased risk of developing mental health disorders. Mindfulness may be one strategy that can help support the mental health needs of this particular population; however, those with (IDDs) may need additional support in cultivating the practice. The purpose of this study was to investigate the use of a wearable device designed to provide neurofeedback to help promote state mindfulness in young adults with (IDDs). Additionally, attention and affect mechanisms were examined, as well as the social validity of using the wearable device. Using an A-B-A-B single-subject study design, five (age range = 18–25) students completed 20 sessions that consisted of listening and not listening to neurofeedback. Results provide some support for the positive effect of neurofeedback on state mindfulness, paying attention to the breath, and positive affect. All five students reported acceptability of using the device.
The prevalence of individuals with intellectual and developmental disabilities (IDDs) varies between 1% and 3% globally, with a reported incidence of 9 and 13 per 1,000 in the world’s population (Harris, 2006; Katusic et al., 1996). Diagnostic criteria for an IDD include deficits in mental abilities and limitations in adaptive behavior that are observed before the age of 18 (American Psychiatric Association [APA], 2013). Individuals with IDD are at an increased risk of developing mental health disorders (APA, 2013; Dekker & Koot, 2003; Simonoff et al., 2008). One population-based study revealed a prevalence of 40.9% of those with IDD having a mental health disorder (Cooper et al., 2007), and a community-based study showed that 60.4% of individuals with IDD experienced at least one disorder (Deb et al., 2001). These mental health disorders can include behavioral, cognitive, and emotional disorders. Several of these disorders originate in early adulthood, which is why it is essential to support the mental health of young adults with IDD.
Mindfulness
One strategy that can be used to support mental health in young adults with IDD is the promotion of mindfulness in educational settings. Mindfulness is the ability to pay attention on purpose, in the present moment, and nonjudgmentally (Kabat-Zinn & Hanh, 2013), and state mindfulness refers to the quality of mindfulness at a particular point in time (Brown et al., 2015). Self-regulation theory is one framework that describes the processes by which mindfulness may support mental health outcomes. Baumeister et al. (1994) describe self-regulation as a multifaceted system of conscious personal control involving the ability to manage emotions and thoughts to achieve goals. The ability to be mindful at a particular moment in time can enhance self-regulation (Brown et al., 2015; Kabat-Zinn, 1994, 2003), which is a critical factor in supporting positive mental health (Baumeister & Vohs, 2003; Kabat-Zinn, 2003; Masicampo & Baumeister, 2007). Two ways that mindfulness may support self-regulation is by increasing attention (Holzel et al., 2007) and positive affect (Remmers et al., 2016). At its core, practicing mindfulness involves bringing awareness to current experiences and/or situations by way of regulating the focus of attention (Bishop et al., 2004). In addition, mindfulness is strongly linked with positive affect or pleasurable feelings, which also plays a key role in self-regulation (Tice et al., 2007). Thus, mindfulness may enhance self-regulation through a greater capacity for attentional focus and more positive affect.
Mindfulness-Based Interventions (MBIs)
MBIs have increasingly been used in samples of young adults with and without IDD. For example, a meta-analysis by Chiesa and Serretti (2009) identified 10 studies investigating mindfulness and mental health in young adults and found that the participants experienced significantly greater improvement in mental health outcomes (e.g., stress), compared to those who did not practice mindfulness. MBIs encompass self-regulatory strategies, such as focusing attention to the present moment, which can help promote positive mental health outcomes (Kabat-Zinn, 2003). Although studies often report lower levels of self-regulatory strategies in people with IDD (Nader-Grosbois, 2014), studies also discuss how self-regulation can be taught and how it can improve as the developmental age of the individual increases (Vieillevoye & Nader-Grosbois, 2008; Wehmeyer et al., 2003). As a result, young adulthood may be an ideal developmental period to implement self-regulation interventions, such as MBIs, for those with IDD.
Soles of the Feet is a common MBI designed specifically for those with IDD and has shown to be successful for this population by using simple self-regulatory strategies (Singh et al., 2003). Over the course of five 45-min sessions, individuals are taught to become aware of emotional precursors that can lead to aggressive or anxious behavior through mindful breathing and body awareness and learn to divert attention from the emotionally arousing thought or event to a neutral stimulus (i.e., soles of the feet; Felver et al., 2013; Singh et al., 2003). These self-regulation approaches can help the individual focus on sensations in the body and experience feelings of calmness (Felver et al., 2013; Singh et al., 2003). Studies that applied soles of the feet have shown improvements in mental health indicators such as aggressive behavioral disorders in young adults with IDD (Adkins et al., 2010; Singh et al., 2003; Singh, Lancioni, Winton, Adkins, Singh, & Singh, 2007; Singh, Lancioni, Winton, Adkins, Wahler, Sabaawi, & Singh, 2007; Singh et al., 2008). These studies highlight how an MBI that uses self-regulatory strategies can be used and be effective for those with IDD.
Other MBIs that use elements such as focusing on the breath and body scans, of mindfulness-based stress reduction (Kabat-Zinn, 2003) and mindfulness-based cognitive therapy (Segal et al., 2002) illustrate how valuable these interventions can be for those with IDD. Both types of mindfulness practice have shown promising results in improving mental health disorders in young adults with IDD (Harper et al., 2013; Idushohan-Moizer et al., 2015). In addition to the effectiveness of these MBIs, young adults with IDD report that they value mindfulness techniques that enable them to self-regulate their behaviors and emotions rather than having to be directed or managed by others (Chapman et al., 2013; Currie et al., 2019). Thus, there is evidence that a variety of mindfulness-based strategies can support the mental health needs of young adults with IDD.
With promising mental health benefits to be gained from the practice, more research is needed to effectively promote mindfulness in young adults with IDD. One reason for this is young adults with IDD are generally not mindful, due to lack of knowledge or awareness of the practice (Chapman & Mitchell, 2013). Another challenge that young adults with IDD may face when first learning about mindfulness is needing additional support to promote their practice (Chapman et al., 2013; Chapman & Mitchell, 2013; Hwang & Kearney, 2013). MBIs need to use innovative methods that are encouraging and motivating that can assist young adults with IDD to be mindful and cultivate the practice, thus integrating mindfulness within their lives (Chapman et al., 2013). Testing new methods for promoting mindfulness in young adults with IDD could help build upon existing strategies and perhaps increase their effectiveness.
Mindfulness Supported With Technology
A novel approach that can help address certain challenges in promoting mindfulness in young adults with IDD are MBIs supported with technology. Technology can include mobile and wearable devices and has been shown to support young adults with IDD in areas ranging from education (Blishchak & Schlosser, 2003) to employment (Wehmeyer et al., 2006), and more recently mental health (Luxton et al., 2011). Additionally, MBIs supported with technology are increasingly used to promote the practice of mindfulness. In a recent review of the literature, Plaza et al. (2013) discuss how mobile and wearable devices can support mindfulness daily practice and adherence due to the usability and ubiquity of these devices. Innovative methods of promoting mindfulness in young adults with IDD are needed, and MBIs supported with technology can address this need by furthering our understanding of how mindfulness can support this underserved population.
Research Questions
In this study, we addressed two main research questions: (1) Is state mindfulness present in students with IDD with the support of a wearable device that provides neurofeedback to help an individual be more mindful? and (2) Is there evidence that attention and affect may serve as mechanisms by which mindfulness facilitates self-regulation? We hypothesized that state mindfulness scores would be higher when receiving neurofeedback on the state of their mindfulness from a wearable device compared to not receiving feedback. We also hypothesized that students would pay more attention to their breath with the help of the neurofeedback compared to not receiving the feedback. Finally, we hypothesized that students’ affect would be more positive following the use of the neurofeedback compared to not receiving the feedback. Specifically, we expected their affect to be higher (i.e., more positive) after practicing mindfulness with neurofeedback than without. We also expected improvements in affect from before to after their mindfulness practice to be greater and in a positive direction when using neurofeedback compared to not using it. Through the use of interviews, we explored if an MBI supported with technology is socially valid for students with IDD.
Method
Participants
Following institutional review board approval, five students with IDD were recruited from a high school and a program at a postsecondary education institution for students with IDD in the United States. Inclusion criteria for the participants consisted of a diagnosis of a mild or moderate IDD and no comorbid mental health disorders. Prerequisite skills needed to participate in the study included being able to sit and complete the mindfulness session for 5 min and answer questions regarding the session as well. Individuals with a severe or profound severity level were not included in the study due to limited conceptual and communication skills (APA, 2013). Information regarding the IDD diagnoses was obtained from the special education teachers. The primary researcher asked the special education teachers to provide the severity levels, which came from the students’ school records. The following section includes a brief description of each student.
All five students were able to verbally communicate their responses to study questions and were able to independently ask questions before, during, and after the study. For example, saying “yes” or shaking their head and using direct eye contact when asked if they understood a question. The special education teachers reviewed the procedures and materials that the students would complete throughout the study. This was done to ensure that the students would be able to comprehend the procedures and materials and that it would be within their skill set to complete them. Any changes and suggestions from the special education teachers were incorporated into the procedures and materials. All five students were Caucasian. Two of the study participants, Luke and Hans, were both 18-year-old male students diagnosed with Down syndrome and autism spectrum disorder (ASD), respectively. Both participants were finishing their last year of high school. Another participant, Anakin was a 21-year-old male student diagnosed with Down syndrome and was finishing his first semester of a 2-year postsecondary education program for students with IDD. Leia and Kylo, two other participants were 22 and 25 years old. They were both diagnosed with ASD and were finishing their first semester in the postsecondary program.
Dependent Variables
State mindfulness
State mindfulness was assessed by the MUSE. The MUSE is a wearable electroencephalography (EEG) device that measures brain wave activity and provides continuous neurofeedback, which is displayed in a smartphone or tablet using Bluetooth connectivity (Krigolson et al., 2017). The MUSE detects individual brain waves to determine state mindfulness (Krigolson et al., 2017), which refers to the quality of mindfulness at a particular time (Brown et al., 2015). The MUSE provides calm, neutral, and active feedback regarding the mindfulness session. Calm feedback refers to the time spent being mindful (i.e., state mindfulness), and attention was focused on the breath. Neutral feedback refers to a person’s natural resting state. Active feedback refers to time spent not being mindful and not focused on the breath during the session. All three are reported in minutes and seconds per session, and the calm feedback represented the state mindfulness scores. Although the MUSE has not been tested on young adults with IDD, it has been tested against industry standard EEG systems including the Brain Vision actiCHamp system and the g.Tecg.USBamp system and has produced valid and reliable scores for detecting individual brain waves to determine state mindfulness (Hashemi et al., 2016; Kovacevic et al., 2015; Marcengo et al., 2017).
Attention
To assess attention, an adapted version of Tammen’s (1996) Attentional Focus Scale was administered. The original scale is a single-item bipolar scale with internal focus (e.g., breathing) and external focus (e.g., daydreaming) at either end of a 10-cm line. For this study, the anchors were modified to “paying attention to the breath” and “not paying attention to the breath.” The scale was administered immediately after each session by asking the students to mark an “X” or line to show, “how much you were paying attention or not paying attention to your breath during the MUSE session.” Attentional focus was scored by measuring the distance in centimeters and millimeters from the paying attention to the breath anchor on the left-hand side to the mark the student made and multiplying by 10 to obtain a score out of 100. Scores under 50 indicate a predominately focused attention to the breath, whereas scores over 50 indicate a predominantly unfocused attention to the breath. Previous research has provided evidence of score validity using this scale (Baden et al., 2005).
Affect
To assess the dependent variable affect, the Children’s Feeling Scale (CFS; Hulley et al., 2008) was administered. The CFS measures how one currently feels on an 11-point scale ranging from −5 (very bad) to +5 (very good), with smiley faces to help the individual understand the scale (Hulley et al., 2008). Students were asked before and immediately after the mindfulness session, “How do you feel right now? Circle a number.” Research has produced evidence of valid and reliable CFS scores for assessing current affect in children and adolescents (Hulley et al., 2008).
Social validity
Social validity of the MUSE was assessed by interviewing the students in a quiet meeting room at the school and were audio recorded using the Voice Memos application on an iPad. A total of five open-ended interview questions regarding the acceptability of and satisfaction with the MUSE intervention were asked at the end of the study by the primary researcher. These questions were developed in collaboration with the special education teachers to ensure that participants would be able to understand and respond to the questions. The five questions asked were (1) Do you think the feedback provided by the MUSE helped you pay attention to your breathing? (2) What did you like most about using the MUSE? (3) What did you not like about using the MUSE? (4) Is there anything that you would change about the MUSE that would make it better or easier for you to use? and (5) Would you recommend other students use the MUSE? The interviews included probing follow-up questions (e.g., Why do you think the feedback provided by the MUSE helped you pay attention to your breathing) to gather more specific data and field notes were taken. The interview questions were based on previous research assessing social validity in intervention studies (Wolf, 1978).
Study Design
An A-B-A-B design was used to examine the relationship between the use of the MUSE and dependent variables (Ledford & Gast, 2018). There were a total of four phases (i.e., A-B-A-B) with five data points per phase, and the independent variable (i.e., the MUSE neurofeedback) was systematically manipulated. Both of these standards meet the What Works Clearinghouse (WWC, 2017) single-case design standard without reservations. However, interobserver agreement was not collected and does not meet the WWC (2017) single-case standards and is a limitation of this study.
Procedures
Each mindfulness session was 5 min for students during baseline (A) and intervention (B) phases. Prior to each session, the primary researcher read a brief script to the students explaining what mindfulness is and how to be mindful. Please refer to Table 1 for the script used for the intervention phase. The script also contains details about the operationalized definitions of students demonstrating “understanding” and “paying attention.” The script used for baseline is the exact same script without the information regarding how to listen to the MUSE. A total of 20, five-min sessions (i.e., 10 baseline and 10 intervention) were conducted over the course of 6 weeks for each student. All sessions were conducted individually in a quiet meeting room in their respective schools with only the participant and primary researcher in the room. The lights were on during each session.
A Sample of the Procedures Followed for Intervention Phase (B).
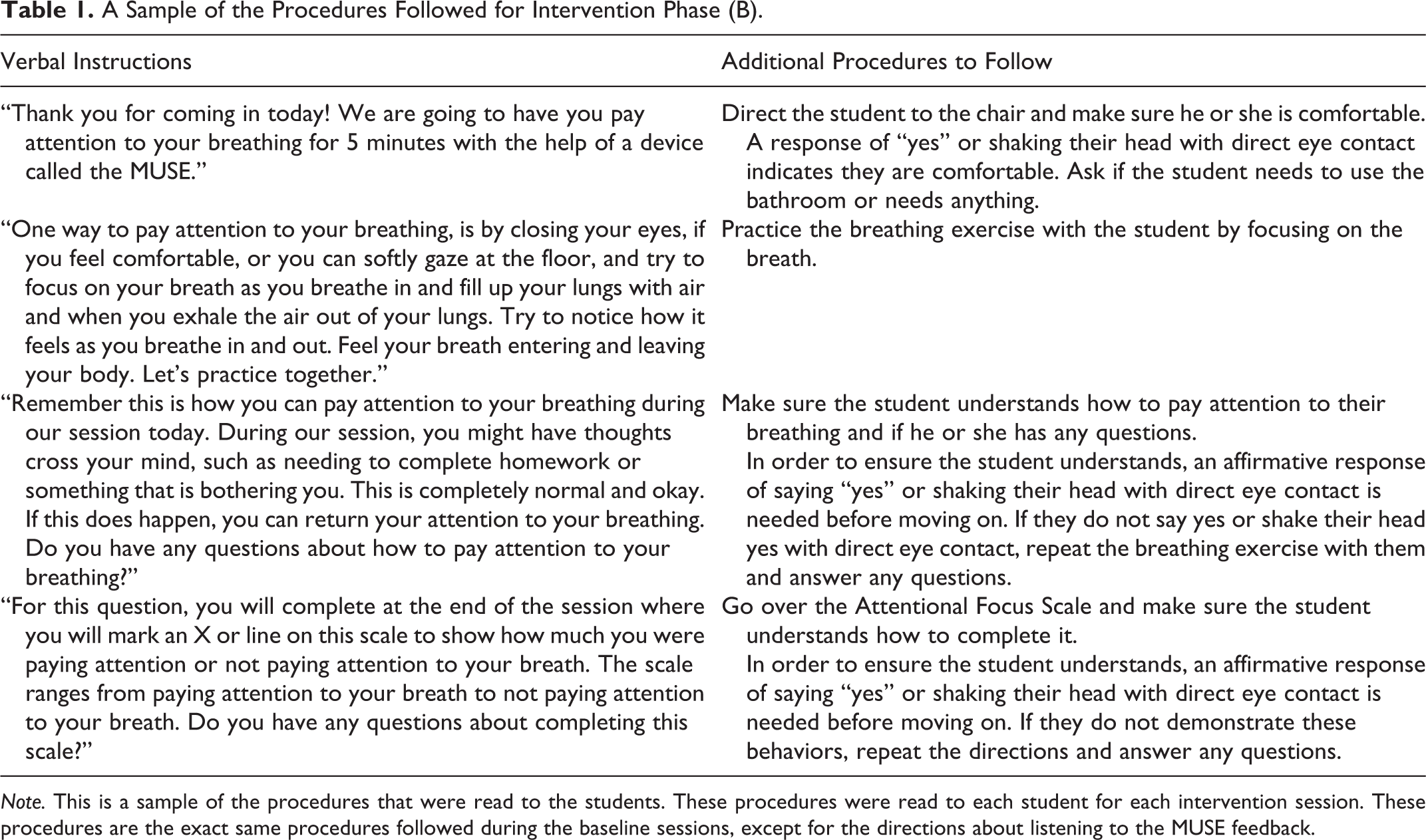
Note. This is a sample of the procedures that were read to the students. These procedures were read to each student for each intervention session. These procedures are the exact same procedures followed during the baseline sessions, except for the directions about listening to the MUSE feedback.
Baseline (A)
After students were given the general instructions, the MUSE headset was fitted for the student to wear while in a comfortable, seated position. Next, the MUSE was connected to the application on a smart phone or tablet via Bluetooth. During each baseline phase, students wore the MUSE for 5 min but with the neurofeedback cues on the device muted. Thus, the only direction students received about how to be mindful were the initial instructions to pay attention to their breath. This allowed us to obtain state mindfulness scores without providing feedback to the students.
Intervention (B)
In addition to the procedures used for the baseline phases, the students were able to hear the neurofeedback cues provided by the MUSE in the two intervention phases. All students listened to the “ocean” neurofeedback cues. During the mindfulness session, the MUSE translated brain signals into the sounds of wind, such as the ocean soundscape, and was heard from the smartphone or tablet. When the individual was focused on their breath, the wind sounds were calm and settled. If the individual’s mind began to wander and was not focused on the breath, the winds picked up and blew. Thus, the participants were cued to refocus on the breath and bring themselves back to the present moment.
Data Analysis
Means were calculated for study variables in each A and B phase using SPSS Version 25 for analyzing levels of the data. Additionally, a visual analysis procedure that is typically used in single-subject research (Ledford & Gast, 2018) was used to evaluate the state mindfulness and attention-dependent variables. To assess changes between baseline and intervention phases, two indicators were examined: trend and variability (Ledford & Gast, 2018). One way to determine the trend is the Nugent (2009) approach, where the researcher draws a straight line connecting the first and last data points in the baseline and intervention phases. A visual inspection of the data was conducted to determine whether the data were stable or varied in a particular phase.
Additionally, the immediacy of effect was evaluated, which refers to immediate changes from the introduction or withdrawal of the intervention (Ledford & Gast, 2018). Finally, the percent nonoverlapping data (PND) were assessed, which refers to the extent of the overlap between the baseline and intervention conditions (Ledford et al., 2018). The mean, trend, variability, immediacy of effect, and PND were the five analysis tools used to determine whether there was a functional relation between the neurofeedback cues provided by the MUSE and the state mindfulness and attention-dependent variables. The mean for postsession affect and the affect change scores from pre to post were used to determine any changes and/or differences in affect.
A content analysis was conducted on the student responses to assess the social validity of using the MUSE. The primary researcher followed the recommendations of Erlingsson and Brysiewicz (2017) to complete a content analysis. Steps included dividing up the interview texts into smaller parts, referred to as condensed meaning units, and labeling these units by formulating codes and grouping them into categories and themes (Erlingsson & Brysiewicz, 2017).
Results
State Mindfulness
Means for state mindfulness and attention during baseline (A1 and A2) and intervention (B1 and B2) phases for the students are displayed in Table 2. Overall, the state mindfulness mean scores for the B1 phase were higher, compared to the A1 phase for most of the students. Luke was the only student to have a higher state mindfulness mean score during the A1 phase, compared to the B1 phase (M = 2:27 vs. M = 2:04). Four of the students had higher state mindfulness mean scores for the B2 phase, when compared to the A2 phase. Hans was the only student who demonstrated a higher state mindfulness mean score (M = 2:27) in the A2 phase, when compared to his mean score (M = 2:21) in B2 phase. For consistency of effect (i.e., similar data paths for the phases), Anakin’s and Leia’s B1 and B2 conditions were similar. Variability of the data was evident for all four students, except for Anakin’s B1 and B2 phase. However, there was an immediacy of effect apparent across the phases for all the students, excluding the A2 and B2 phase for Hans. Figure 1 displays the visual results of the dependent variable state mindfulness, and Table 3 shows a summary of the criteria used to demonstrate a functional relation between state mindfulness and the neurofeedback.
Means for State Mindfulness and Attention.
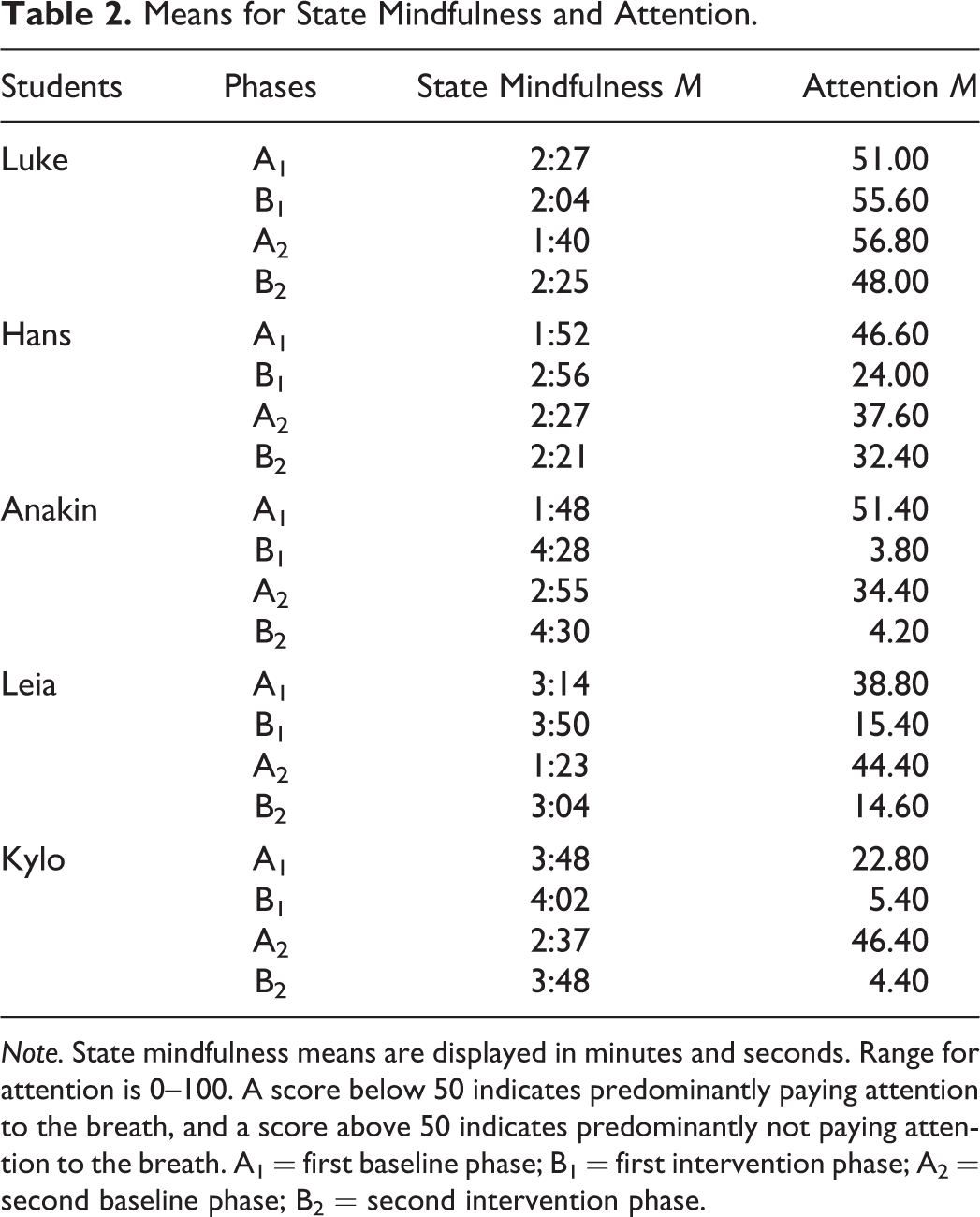
Note. State mindfulness means are displayed in minutes and seconds. Range for attention is 0–100. A score below 50 indicates predominantly paying attention to the breath, and a score above 50 indicates predominantly not paying attention to the breath. A1 = first baseline phase; B1 = first intervention phase; A2 = second baseline phase; B2 = second intervention phase.
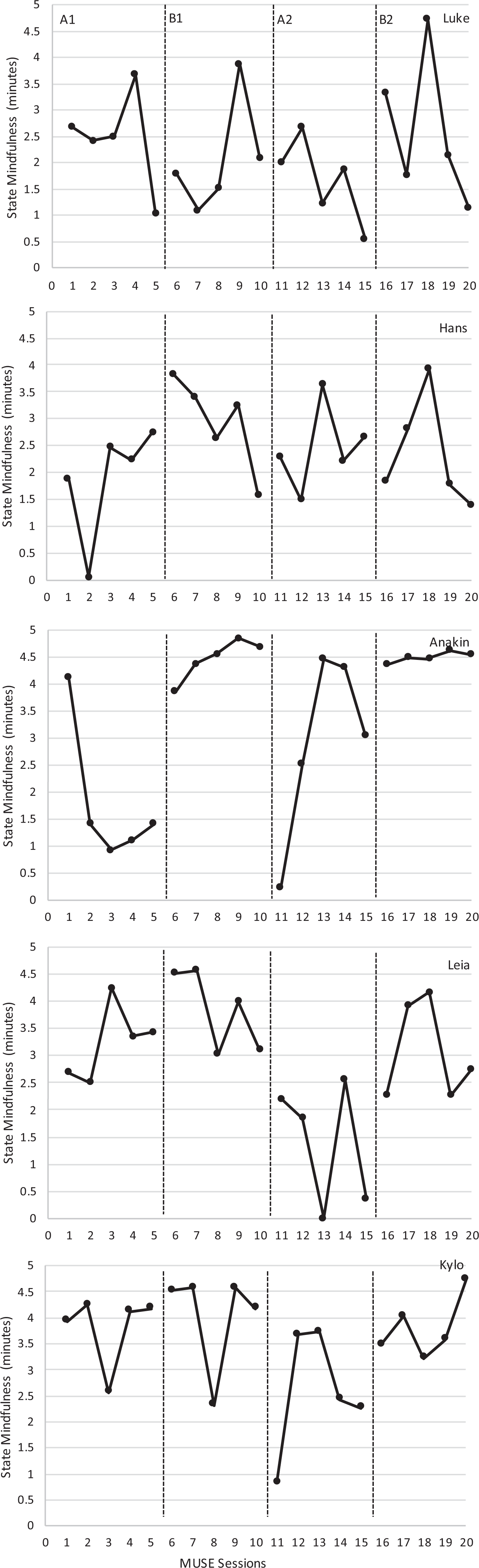
State mindfulness scores as time being mindful for each MUSE session.
Summary of Criteria Used to Determine Functional Relation State Mindfulness.
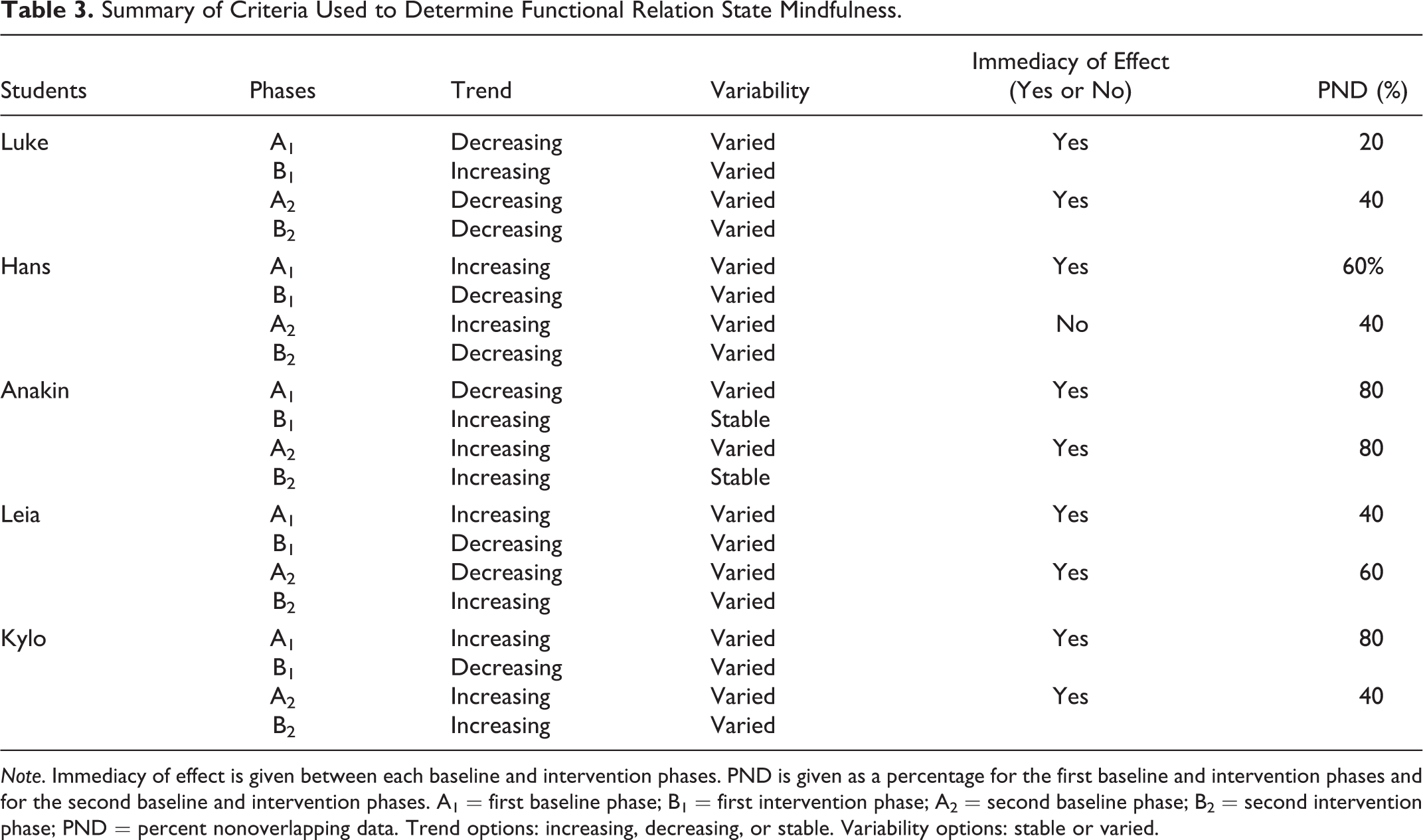
Note. Immediacy of effect is given between each baseline and intervention phases. PND is given as a percentage for the first baseline and intervention phases and for the second baseline and intervention phases. A1 = first baseline phase; B1 = first intervention phase; A2 = second baseline phase; B2 = second intervention phase; PND = percent nonoverlapping data. Trend options: increasing, decreasing, or stable. Variability options: stable or varied.
Attention
Attention mean scores were higher in A1 phases than B1 phases, suggesting that the students were paying attention to their breath more when listening to the neurofeedback cues in the intervention phase than the baseline phase (Table 2). Luke was the only student who had a lower attention mean score in the A1 phase (M = 51.00) than B1 phase (M = 55.60). This finding indicates that he was paying attention to his breath more during that particular baseline phase. This is consistent with his state mindfulness mean score where he was more mindful during the A1 phase than the following B1 phase. Consistency of effect was evident in Anakin’s, Leia’s, and Kylo’s A and B phases. This included higher scores (i.e., not paying attention to the breath) in A1 and A2 and lower scores (i.e., paying attention to the breath) in B1 and B2 phases. An immediacy of effect was seen between the A and B phases for Anakin, Leia, and Kylo, but not for Hans and only between A2 and B2 for Luke. The data were stable for the B phases for Anakin, Leia, and Kylo, but not for Luke and Hans. Figure 2 contains the visual results of the dependent variable attention, and Table 4 displays a summary of the criteria used to determine a functional relation between attention and the neurofeedback.
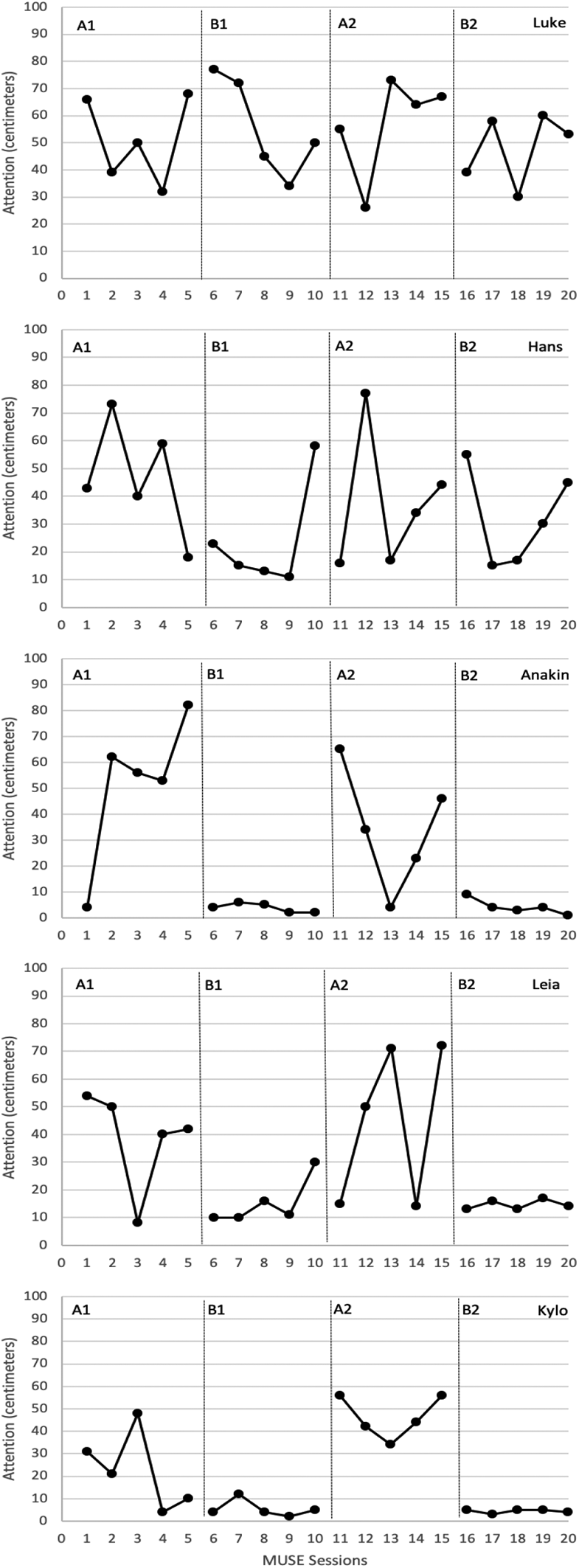
Attention scores for each MUSE session.
Summary of Criteria used to Determine a Functional Relation for Attention.
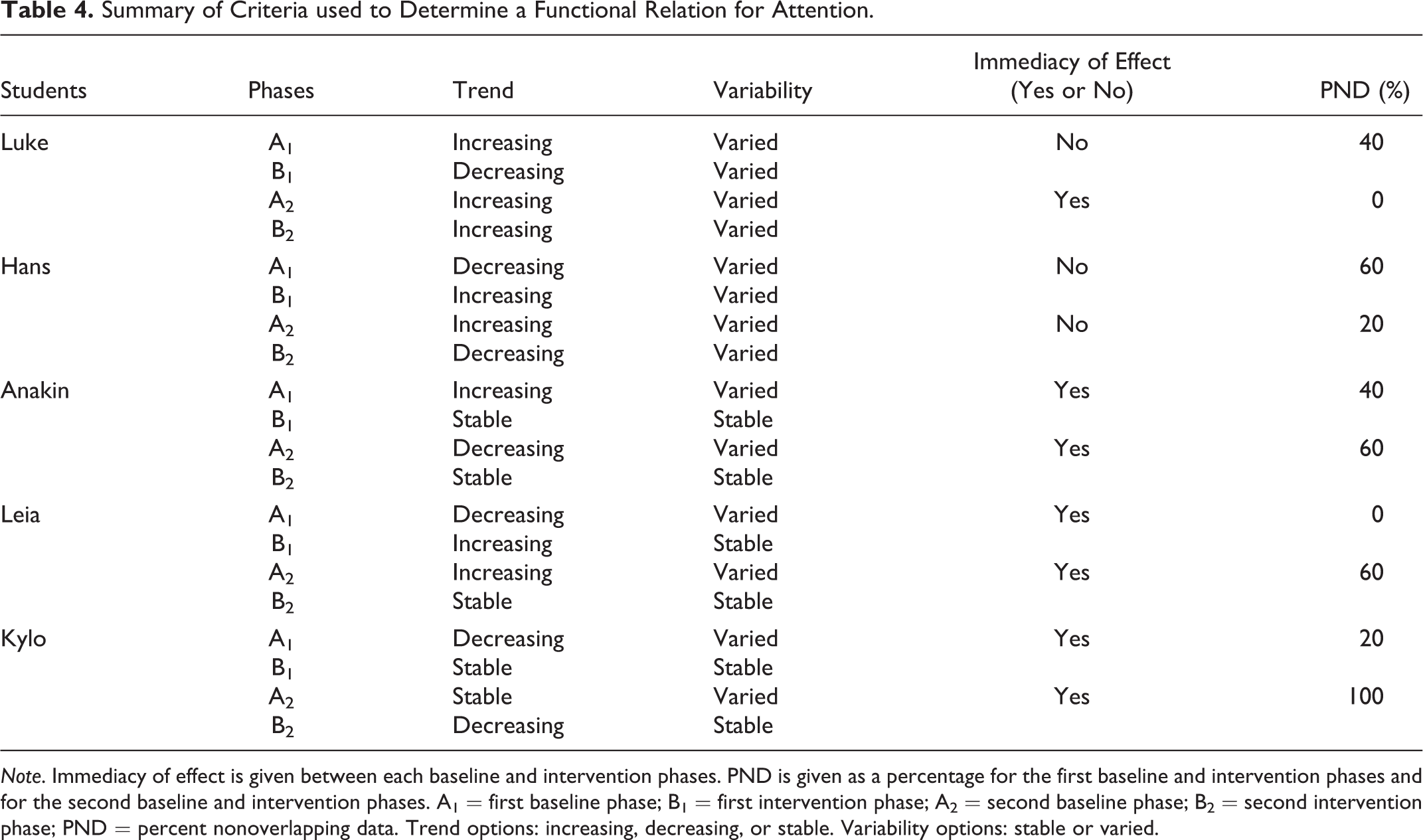
Note. Immediacy of effect is given between each baseline and intervention phases. PND is given as a percentage for the first baseline and intervention phases and for the second baseline and intervention phases. A1 = first baseline phase; B1 = first intervention phase; A2 = second baseline phase; B2 = second intervention phase; PND = percent nonoverlapping data. Trend options: increasing, decreasing, or stable. Variability options: stable or varied.
Affect
Means and standard deviations for presession affect, postsession affect, and affect change between baseline (A1 and A2) and intervention (B1 and B2) phases for the students are displayed in Table 5. Luke was the only student who reported a higher A1 postsession affect mean (M = 3.40). This affect score is consistent with his state mindfulness and attention scores, where he was more mindful and paying more attention to his breath in the A1 phase, compared to the B1 phase. All postsession affect scores were higher in the B2 phases than the A2 phases, except for Luke where he selected +5 for all of his presession affect and postsession affect. This means there was no change in his affect between these particular phases. In addition, Luke was the only one who had a higher affect change in the A1 phase than B1 phase (M = 3.40 vs. M = 2.60), which is consistent with his previous mean scores for the other variables.
Means and Standard Deviations for Affect.

Note. Range for affect is −5 to 5. A1 = first baseline phase; B1 = first intervention phase; A2 = second baseline phase; B2 = second intervention phase.
Social Validity
Three themes emerged from the analysis of the participants’ responses: (1) students liked how the sounds (i.e., neurofeedback) from the MUSE helped them pay attention to their breathing, (2) the MUSE was easy to use, and (3) they would recommend the MUSE to other students. A […] in the quotations signifies text that was removed to increase clarity. Support for liking the MUSE sounds and how it helped them pay attention to their breathing can be seen in Kylo’s response.
“Do you think the feedback provided by the MUSE helped you pay attention to your breathing?”
“Yes.”
“Yes? Why do you think that?”
“The calm ocean waves made it so my mind did not wander.”
The ease of using the MUSE was the second theme seen across the students’ responses and is evident in their comments. For example, both Luke and Hans said, respectively: “I used the […] MUSE and it’s easy” and “I-I like easy, and to me […] the MUSE is easy to use for me.” The third theme, focused on student recommendation of the MUSE, was evident in all comments, including Leia’s “cause it, it would help, help’em [student], you know, help’em relax and if they’re stressed and stuff like that.”
Summary
Based on the mean, trend, variability, immediacy of effect, and PND, there is evidence that there was a functional relation between listening to the neurofeedback cues and state mindfulness for Anakin, Leia, and Kylo. However, this was not true for Luke and Hans. A functional relation between listening to the neurofeedback cues and paying attention to the breath was observed for Anakin, Leia, and Kylo. These students were able to pay more attention to their breath when using the neurofeedback cues, compared to no neurofeedback cues. Yet this did not occur for Luke and Hans. Except for Luke, all postsession affect scores were more positive or remained the same after listening to the neurofeedback cues for Hans, Anakin, Leia, and Kylo. In terms of social validity, all five students reported the acceptability and supported the social validity of using the MUSE to promote mindfulness.
Discussion
Based on the growing evidence of how practicing mindfulness can support positive mental health outcomes in young adults with IDD (e.g., Adkins et al., 2010; Harper et al., 2013), the current study investigated the use of a wearable EEG device to promote mindfulness in students with IDD. Specifically, a primary aim of this study was to determine if the use of neurofeedback cues, provided by the wearable EEG device called MUSE, could result in higher state mindfulness, attention, and positive affect. Qualitative data were also collected to explore the social validity of using the MUSE for students with IDD.
Overall, the data suggested that some of the students experienced higher state mindfulness when using the MUSE than when not using the MUSE. A functional relation between the use of the neurofeedback and higher state mindfulness was demonstrated for Anakin, Leia, and Kylo. For Luke and Hans, the state mindfulness scores were more variable, and the data did not show a clear and sustained increase in state mindfulness as predicted. Thus, the data provide partial support for the hypothesized relation between the use of the neurofeedback from the MUSE and improving state mindfulness in these students. Variability in the effectiveness of the MUSE may be explained by students’ level of functioning. Luke and Han’s levels of disability were labeled as moderate, whereas the other three were identified as having mild disabilities. Research has shown that differences in level of functioning can greatly influence the adaptive functioning of young adults with IDD, which can impact how they learn and react to certain situations (De Bildt et al., 2005). As a result of the severity differences, these students may have responded differently to using the neurofeedback from the MUSE.
Another possible reason why the neurofeedback did not work for these two students may be due to their developmental age. These two students were the youngest (i.e., 18 years old) and still in high school, while the other three were between the ages of 21 and 25 and were in college. The older students may have more pronounced self-regulatory skills that can help them practice mindfulness due to their age (Vieillevoye & Nader-Grosbois, 2008), compared to the younger students. Moreover, the students in college were at different phases in their lives, such as living independently on their own, compared to the high school students. Greater independence may provide more opportunities to develop self-regulatory skills, which could explain higher responsiveness to the MUSE intervention. Additionally, extending the condition lengths to obtain more stability for these two students may have been needed to observe effects. Conducting more sessions at baseline before introducing the MUSE could have provided more stability and less variability in these particular students.
Interestingly, all five students had surprisingly high state mindfulness scores in their first baseline (i.e., no neurofeedback) phase. In order to measure differences in state mindfulness between using the neurofeedback and not using the cues, the students were taught how to practice mindfulness before each session throughout the study. This may account for the higher than expected state mindfulness scores observed in baseline. Although the MUSE seemed to not be of added benefit for some of the students, introducing and explaining how to practice mindfulness helped the students be mindful even without the neurofeedback. This particular finding is consistent with empirical evidence from other MBIs that emphasize how individuals with IDD may not generally be mindful but can comprehend and learn the construct (Chapman & Mitchell, 2013). The high baseline state mindfulness scores support these previous findings, and the current study further highlights how students with IDD can learn how to practice mindfulness through support and guidance.
Similar to state mindfulness, attention scores were higher when using the neurofeedback compared to not using the cues for some of the students. These scores provide some validity evidence for using the MUSE to increase state mindfulness. A functional relation was shown between using the neurofeedback from the MUSE and higher attention scores for Anakin, Leia, and Kylo. However, again, this was not true for Luke and Hans. Their collected data did not display a continuous and well-defined pattern of paying attention to the breath as expected. Therefore, there is partial support for the hypothesized relationship between using the neurofeedback and paying more attention to the breath. Previous research shows how attention may be one mechanism that explains the relationship between mindfulness and heightened self-regulation (Holzel et al., 2011). However, the targeted samples in these studies have primarily been experienced meditators (Holzel et al., 2007), clinical (Kabat-Zinn et al., 1985), and general populations (Lutz et al., 2008). As for individuals with IDD, the majority of research is predominantly focused on examining outcomes and the effectiveness of MBIs and not investigating mechanisms (e.g., Hwang & Kearney, 2013). Those individuals with IDD are at an increased risk of developing mental health disorders (APA, 2013), and understanding the causal pathways that link mindfulness and enhanced self-regulation can provide insight into how to create the most effective MBIs for young adults with IDD.
In terms of affect, some of the students reported more positive postsession affect when using the neurofeedback to practice mindfulness. Postsession affect scores were more positive in the intervention phases for Hans, Anakin, Leia, and Kylo and provide partial support for the hypothesized relationship between using the neurofeedback cues from the MUSE and more positive affect for these students. Change in affect was either more positive or remained the same between the phases, which provides further support of the hypothesized relationship in these particular students. However, this was not true for Luke and the data does not support the predicted relationship of using the neurofeedback and positive affect for this student. It is important to note that none of his postsession affect scores were more negative than his presession affect scores for all of the phases. This is seen among the other students as well and suggests that practicing mindfulness can help improve affect in students with IDD, regardless of using neurofeedback or not. This finding is consistent with previous studies that show how MBIs can support positive affect and reduce negative affect in clinical populations (Tacón et al., 2003) and college students (Sears & Kraus, 2009). Similar to this study, even brief MBIs (e.g., 10-min or less of mindful practice) can support positive affect in general populations (Arch & Craske, 2006). The present study adds students with IDD as participants in a growing and promising list of how practicing mindfulness can cultivate positive affect.
The social validity interviews provide insight about how the students felt about using the MUSE to practice mindfulness and their responses support the social validity of using the device. Themes from the social validity interviews from the students reveal that the neurofeedback from the MUSE can help students with IDD practice mindfulness, the MUSE is easy to use, and all of the students would recommend the MUSE to other students. Traditionally, social validity is assessed via questionnaires (Carter, 2009); however, we wanted the opportunity to ask follow-up questions and obtain as much information as possible, especially since this is the first study evaluating the social validity of the MUSE for students with IDD. However, additional measures, such as the special education teachers completing a questionnaire to rate if the student was less anxious or more relaxed following a MUSE session, could provide further evidence of the effectiveness of using the MUSE. Although this intervention was not effective for all of the students, the students still expressed their satisfaction with the MUSE and how the device is a promising means of promoting mindfulness for students with IDD. These findings are consistent with other studies investigating the social validity of MBIs for individuals with IDD (Felver et al., 2017). The aforementioned studies together with the current study further highlight the acceptability of using a variety of mindfulness strategies with young adults with IDD.
Several studies highlight how individuals with IDD need continued support and innovative methods to help them cultivate the practice of mindfulness, especially when first being introduced to the practice (Chapman & Mitchell, 2013; Chapman et al., 2013; Hwang & Kearney, 2013). Although there is some evidence of promoting positive mental health outcomes using neurofeedback in youth with IDD (Kouijzer et al., 2009, 2010; Scolnick, 2005) and using neurofeedback to promote state mindfulness for general populations (Sas & Chopra, 2015), this was the first study to our knowledge to use a wearable EEG device to promote state mindfulness for students with IDD. Not only does this device help an individual to be mindful, it also provides an objective means of measuring mindfulness, which can provide more reliable and valid information than subjective measures, such as self-report (Greco et al., 2011). The results also have important implications for practitioners who work with individuals with IDD. The MUSE gives an objective measure of how mindful individuals are in real time, which can provide opportunities for practitioners and individuals to go over the results together. This may encourage and motivate individuals with IDD to practice more mindfulness, which may help them develop self-regulatory strategies that can promote positive mental health outcomes.
Limitations
There are several limitations of this study that need to be addressed in future research. Although the MUSE has shown to be valid and reliable in detecting state mindfulness in general populations, it has not been tested on young adults with IDD. Additionally, the reliability and validity of the Attentional Focus Scale and CFS have not been tested for young adults with IDD and is a further limitation. Participant information regarding intelligence and adaptive behavior measurements were not collected for this study, and the lack of these scores creates a serious limitation that future studies can consider. Another limitation is that all participants received the baseline and intervention in the same order. This makes the study vulnerable to the threat of sequence effects that could have influenced the students’ performance. Also, the absence of a maintenance phase does not provide information on lasting treatment effects. One last limitation is the lack of procedural fidelity or interobserver agreement that could help enhance the internal validity of this study.
Recommendations and Conclusion
Future recommendations include comparing the effects of using the MUSE in individuals with different IDD severity levels. This could enhance our understanding on how those with varying severity levels respond to using the MUSE. Additional future studies could investigate the effects of using different methods of guided mindfulness practice, such as a mindfulness app or another neurofeedback device, in young adults with IDD. This could provide insight into how young adults with IDD respond to various modes of the practice. One last recommendation is investigating how the use of the neurofeedback from the MUSE can promote positive mental health outcomes such as anxiety and depression. Young adults with IDD are at an increased risk of developing mental health disorders, and practicing mindfulness may be one approach that can address this issue. As a result, it is imperative to understand how the practice can benefit and be fostered among those with IDD. The findings from this study provide partial support for the use of a wearable EEG device designed to provide neurofeedback to help promote state mindfulness for students with IDD. The results of this study further suggest that students with IDD can learn and practice mindfulness, with or without the aid of neurofeedback. Thus, continuing to promote the practice of mindfulness for individuals with IDD is one way to support the unique needs of these individuals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.