
Abstract
Individuals with autism spectrum disorder (ASD) have deficits in social and communication skills that can cause problems such as difficulty interacting with others and challenging behaviors. Research has demonstrated the effectiveness of parents as intervention implementers to improve children’s communication skills. We evaluated the effects of a telepractice parent coaching communication intervention on communication skills of children with ASD utilizing a multiple probe design across participants. Parents applied strategies learned with their child, targeting communication skills, such as asking opinion-oriented questions or using augmentative and alternative communication to request items. Results indicated improvement in children’s communicative behaviors and a significant correlation between parent implementation of intervention elements and children behaviors. Effect size results for the participants indicated strong effects consistent with visually inspected data.
Keywords
Individuals with autism spectrum disorder (ASD) experience difficulty with social and communication skills (American Psychiatric Association, 2013). Early intervention can help promote the use of social skills for individuals with ASD (Landa, 2018). However, barriers to intervention, such as lack of functional communication, challenging behavior, and cost, can lead to high levels of stress for some parents (Krakovich et al., 2016). Behavioral interventions can be costly, about US$40,000–60,000 per child per year (Centers for Disease Control and Prevention, 2015). Intervention can also be time-consuming, with some programs requiring up to 40 hr per week for an average of 3 years for a child with ASD (Chasson et al., 2007; Payakachat et al., 2018). Further, many rural areas do not offer treatment, causing parents to have to drive long hours to get their children the services they need. Additionally, parents, who know their child best and spend the most time with them, are not likely to receive coaching from practitioners on how to work on their child’s skills at home (Baharav & Reiser, 2010). Limited resources within the family’s community result in a lack of social and long-term improvement for individuals with ASD (Chasson et al., 2007; Jones et al., 2017). Finally, the increase in children diagnosed with ASD constrains the availability of practitioners trained to provide intervention services (National Institute of Neurological Disorders and Stroke, 2009). Thus, practitioners should consider the use of nontraditional methods to deliver services to parents of children with ASD, such as online applications.
Telepractice may help ameliorate some of the barriers experienced by parents and practitioners by helping reduce time and effort while reaching areas that would not otherwise have services offered (Heitzman-Powell et al., 2014; Ingersoll et al., 2017). Telepractice is a method that uses technology to provide interventions via distance (Baggett et al., 2010). Telepractice can include live webinars, live meetings, or prerecorded videos to teach a skill. This method of coaching has been shown to be successful with parents of children with ASD and indicates promising results with high fidelity (Webb et al., 2010). That is, direct instruction of parents in the use of interventions via telepractice for their children with ASD results in success of parents implementing these interventions as intended. It can help improve unresolved issues of traditional, in-person, methods of instruction, such as shortage of professionals, lack of funds, transportation, lack of time, long waitlists, childcare, and location of homes in rural areas (Wainer & Ingersoll, 2015).
A number of studies have found the use of in-home parent instruction via telepractice useful with children diagnosed with ASD (Baharav & Reiser, 2010; Bearss et al., 2018; Ingersoll et al., 2017; Vismara et al., 2012). Findings suggest that high-quality services can still be maintained in an untraditional manner via distance programming (Baharav & Reiser, 2010). Teaching parents of children with ASD has also been found to improve the quality of life for parents who do not have the resources to provide intensive therapy for their children (Keen et al., 2010). Parents of children with ASD will likely continue to use the skills learned even after the program via telepractice has ended, which can bring long-term effects of therapy for families (Boisvert & Hall, 2014; Vismara et al., 2012). Other potential benefits include having flexibility in time and location for both the coach and parents (Boisvert & Hall, 2014). Benefits are also seen in increased family leisure, generalization, and maintenance of child outcomes extending past the time of training (Wainer & Ingersoll, 2013). Results should report on both the parent and child outcomes to determine effectiveness and maintenance of the use of skills; however, many studies only report on parent outcomes (Ingersoll & Berger, 2015; Ingersoll et al., 2017; Lindgren et al., 2016; Vismara et al., 2018). Our study presents data for both parents and children with follow-up data to evaluate maintenance use of skills learned.
The purpose of the current study was to investigate the relationship between parent use of multimodal communication intervention skills and communication skills of their children with ASD. The current study, evaluating the use of parent instruction via telepractice, reduced issues found in traditional methods of instruction while focusing on ways to implement new skills in different home environments for children with ASD. The research questions were (a) what was the multiple probe design magnitude of effects of parent implementation of intervention components on child communication behaviors? (b) was there a correlation between the parent implementation of intervention components (i.e., incentivizing communication, modeling, prompting, prompt fading, and expanding) and the use of communication skills of children with ASD.
Method
Experimental Design
We used a multiple probe design (Ledford & Gast, 2018) across three parent–child dyads and one triad to prevent long data probes when collecting baseline data. Implementation for participants was selected in order of their consent to participate. The data were collected on the effectiveness of telepractice parent coaching in a multimodal communication intervention in improving communication behaviors in children with ASD. The study included three main condition changes including baseline, intervention, and maintenance conditions. All three conditions in each level included generalization condition. Each participant began the intervention condition when they demonstrated a stable baseline, and the preceding participant showed an increase in the target behavior (during the intervention of the previous level). The methods for this study were developed drawing from contemporary quality standards for single-case experimental design, including What Works Clearinghouse (WWC) standards (Council for Exceptional Children, 2014; Ganz & Ayres, 2018; Horner et al., 2005; Kratochwill et al, 2013; Reichow et al., 2008; U.S. Department of Education, Institute of Education Sciences WWC, 2019). Although this project was a single-case experimental design, the proximal outcome measured for the parent coaching intervention was parent implementation, which is reported in the companion paper. Thus, we are unable to make a determination regarding the presence of a functional relation between parent implementation and child outcomes.
Participants
Four children who were diagnosed with ASD and at least one parent or caregiver per child participated in the study. Inclusion criteria to participate in the study included the following: (a) individuals who were ages 3–15 years, (b) confirmation of the presence of ASD characteristics as indicated on ASD screening tools (described below), (c) co-occurring communication delay, expressive language impairment, receptive language impairment, or pragmatic language impairment, as indicated by the child’s parent, (d) no co-occurring diagnoses that precluded age-appropriate motor skills, (e) high-speed internet available in the families’ homes or work throughout the sessions of the study, and (f) one or both parents or caregivers available throughout the duration of the study. All participants from Coach-to-Communicate (C2C), a state-sponsored parent treatment service project providing coaching in communication skills for parents and caregivers of children with ASD, were potential recruits. All participants lived remotely from the coach; see approximate distance in each participant section. A total of 8,157 driving miles were saved across all families, defraying the potential travel expenses associated with service in rural areas (Heitzman-Powell et al., 2014).
All children who participated in C2C were reported by their parents to have been diagnosed with ASD. C2C required parents to complete the screening assessments which were used to confirm the presence of ASD characteristics. The ages of parent participants ranged from 36 to 57 years old. Their educational backgrounds ranged from bachelor to doctorate degree. Three dyads and one triad met criteria for participation in this research study. See Table 1 for parent demographics and Table 2 for a summary of formal assessment results for participants. Prior to intervention, parents completed the Autism Spectrum Rating Scale (ASRS; Goldstein & Naglieri, 2009) and the Social Communication Questionnaire (SCQ; Rutter et al., 2003) to determine the level and severity of ASD symptoms and eligibility into the study. Assessments were administered online and collected by an assessor who is a doctoral student in school psychology. Scores of 60 or above on the ASRS and/or 15 or above on the SCQ established eligibility into the study (results in Table 2).
Participant Demographics.
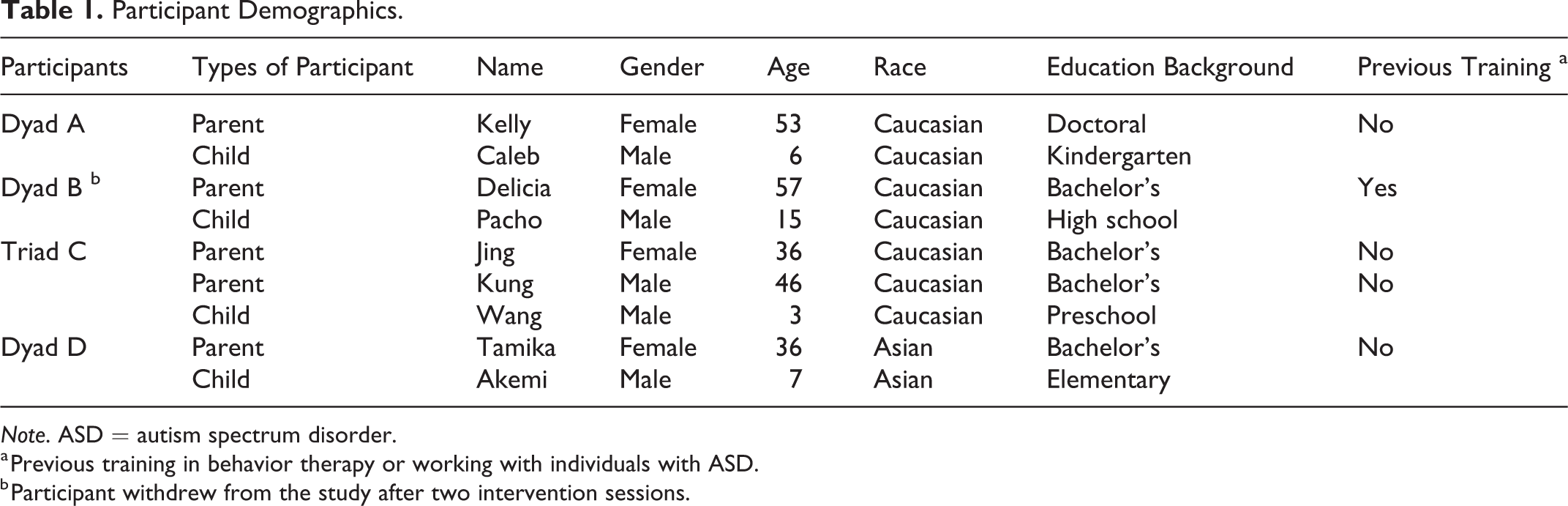
Note. ASD = autism spectrum disorder.
a Previous training in behavior therapy or working with individuals with ASD.
b Participant withdrew from the study after two intervention sessions.
Summary of Formal Assessment Results for Child Symptoms.

a ASRS = Autism Spectrum Rating Scale (Goldstein & Naglieri, 2009). b Social Communication Scale of the ASRS. c SCQ = Social Communication Questionnaire (Rutter et al., 2003).
Dyad A: Caleb and Kelly
Caleb was a 6-year-old boy who was diagnosed with ASD. According to his mother’s interview, he spoke fluently with age-appropriate vocabulary and grammar. However, he had little social interaction at school, lacked two-way communication skills, and rarely communicated with people other than family members. He only used natural eye contact with his mother and family members but did not use eye contact with others. Responses on the formal assessments indicated that Caleb showed characteristics of ASD. Caleb displayed age-appropriate self-regulation skills and was able to communicate well with adults by using phrased speech (e.g., “I will use the money for expenses of nerf guns,” “I broke the stick by the shovel. I used the shovel as an axe. The shovel is strong, strong like an axe.”). Areas for Caleb to improve included interacting with others and demonstrating social–emotional reciprocity. Thus, the target behavior goal for Caleb was to increase his initiating skills and maintaining conversations by asking opinion questions to others. His preferred items and activities (i.e., playing with puppet, feeding his hamster) provided the topics of conversation. The approximate distance of the coach to this family is 114.3 miles (2-hr drive) round trip. The total of travel miles that parents saved by participating in the telepractice coaching was 1,257 miles in the total of 11 sessions.
Dyad B: Pacho and Delicia
Pacho was a 15-year-old boy who was diagnosed with ASD. According to his mother’s interview, he used fluent speech and communicated with age-appropriate vocabulary and grammar. He also had age-appropriate attention and self-regulation; however, he lacked appropriate manner responding to others, asking for help in doing homework or household chores, and asking questions using two-way communication skills. He played games and did his preferred activities by himself, rarely communicating and joining activities with family members, except his brother. Thus, the target behavior goal for Pacho was to increase his initiating skills by asking questions to others. His preferred activity was watching cartoon movies. Unfortunately, Dyad B withdrew from the study after the second intervention session due to the child refusing to make a video recording and not wanting to continue the conversation with his mother. The approximate distance of the coach to this family is 121.4 miles (2-hs drive) round trip. The total of travel miles that parents saved by participating in the telepractice coaching was 364.2 miles in the total of three sessions.
Triad C: Jing, Kung, and Wang
Wang was a 3-year-old boy who was diagnosed with ASD. According to his parents’ interview, he had age-appropriate attention and self-regulation skills; however, he was nonverbal and frequently communicated by grabbing his parents’ hands and leading them to the item he wanted. He never used verbal cues to get attention. His parents tried to prompt him to use pictures to communicate at home. He also experienced difficulty with social communication. Thus, the target behavior goal for Wang was to increase his communication skills by using the communication pictures and communication application on a tablet to request items. His preferred items were his trampoline, pacifier, and blanket. He enjoyed physical play such as tickling but had no preference for particular toys. The approximate distance of the coach to this family was 478 miles (7-hr drive) round trip. The total travel miles that parents saved by participating in the telepractice coaching was 5,258 miles over 11 sessions.
Dyad D: Tamika and Akemi
Akemi was a 7-year-old girl who was diagnosed with ASD. According to her mother’s interview, she used phrased speech to communicate her needs and answer questions (e.g., “I would like to go to the library,” “We went to taekwondo for exercise”) but had limited communication with others, including difficulty responding to and initiating conversation. She also had difficulty adjusting in her routines and had a hard time maintaining attention and regulating her conversation and behavior, which may have further prevented her efforts to interact with others. Thus, the target behavior goal for Akemi was to increase her initiating and maintaining conversations by asking questions to others. Her preferred activities were watching cartoon movies, playing LEGO®, and participating in outside activities (e.g., zoo, mall, library). The approximate distance of the coach to this family is 116.2 miles (2-hr drive) round trip. The total travel miles the parents saved by participating in the telepractice coaching was 1,278.2 miles over 11 sessions.
Coach
The first author, a parent coach, provided all the parent coaching in this study. She had a master’s degree in special education and was a second-year doctoral student in a special education program at the time of the study. She received training in implementing applied behavior analysis strategies. The second author (a board-certified behavior analyst—doctoral designation) was her supervisor during the time of coaching sessions. Neither the coach nor the supervisor had a prior relationship with the participants.
Settings and Materials
Telepractice coaching condition consisted of 11 synchronous individualized coaching sessions (one session per week). The coach developed the treatment plan and set communication goals for each child after the initial interview session with the parent(s). All settings to provide the practice skills of each family were based on the child’s preferred activities and settings inside and/or outside the house. Operational behavioral definitions of children and setting are presented in Table 3.
The parent participants accessed the individual coaching sessions through their computers and internet connections. Parents provided communication strategies to their child and recorded and uploaded a 3-min video through a cloud drive, using Google drive shared folder, before the individual coaching session each week via a videoconference program. All parents used the child’s preferred toys and activities to practice the skills. Only Triad C provided the communication pictures and communication application on a tablet to the child. Details of each child’s materials are presented in Table 3.
Operational Behavioral Definitions of Children.
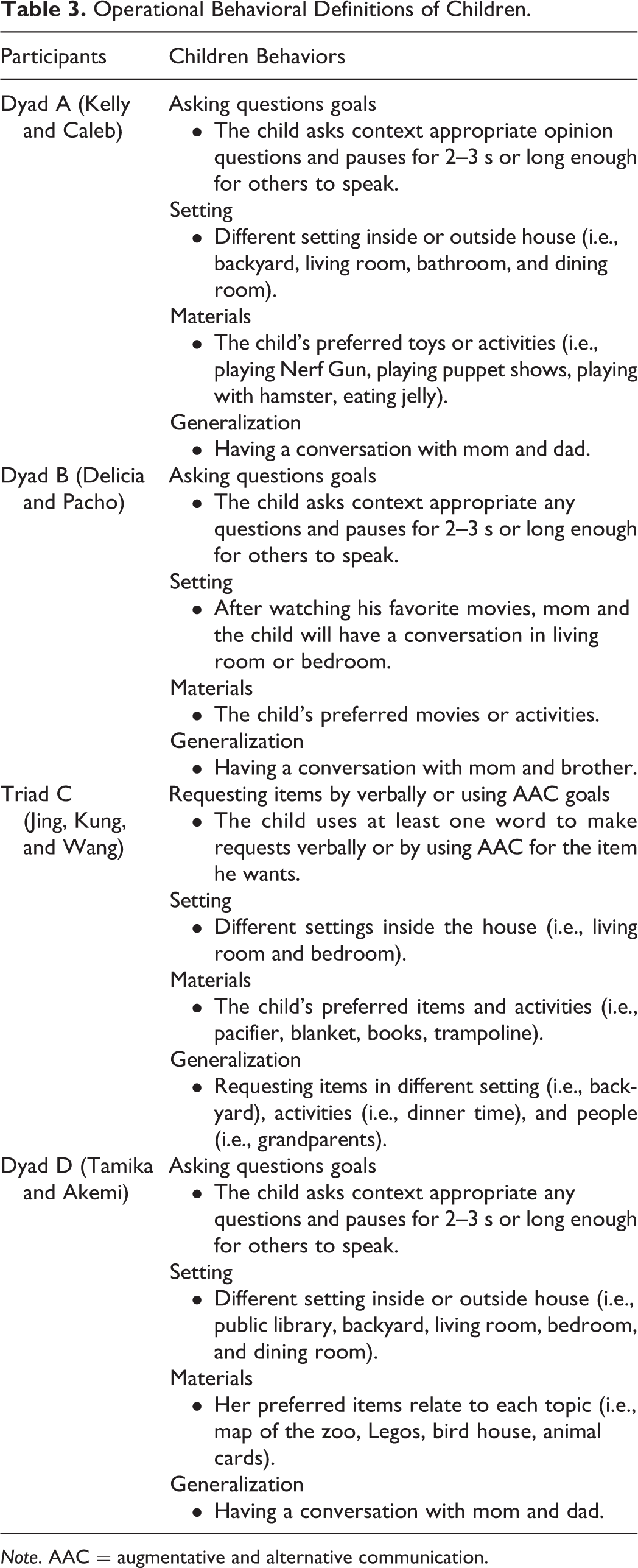
Note. AAC = augmentative and alternative communication.
Dependent Variables
The dependent variables were child behaviors. Any targeted communication behaviors of the child and independent target communication behaviors were displayed and measured by using 10-s partial interval procedures from the 3-min video recordings. We used the Poisson correction method to analyze the estimated count of dependent variables (Yoder et al., 2018). This calculation method is appropriate and more accurate when partial interval recording was used. Parents were required to record and upload 3- to 4-min videos to the shared Google drive folder to demonstrate their implementation of taught skills. Video length was specified to limit file size and ease uploading feasibility (upload speeds slow in some cases of bigger size videos). The targeted communication behaviors of the children were asking opinion-oriented questions (Caleb), asking any questions (Pacho and Amika), and using augmentative and alternative communication (AAC) intervention for requesting items (Wang). Parent implementation of intervention components was also measured and is reported in the companion paper (Wattanawongwan et al., 2020); the components were incentivizing communication, modeling, prompting, time delay, and expanding. Parents used those components to improve targeted communication behaviors of their child.
Study Procedures
Researchers contacted the parents to invite them to participate in this study and explained the consent form, following institutional review board protocol after participants applied to the C2C project. Parents started the baseline condition at the same time. The intervention condition started for each participant based on the data of previous participants, that is, once the prior parent participant began to improve and multiple data points indicated a trend, intervention began with the next dyad. The maintenance condition started 3 weeks after the last coaching session for two data collection probes. Each participant used preference items or activities to practice the strategies with their child.
Baseline condition
The coach conducted baseline via video recordings (3.5- to 4-min long) submitted into Google drive by each parent demonstrating the way they usually communicate with their child. The coach told the parent to use their smartphones to record the videos. In two families (Dyads A and D), either the parent who is the communication partner or the other parent captured the videos by holding the smartphone, and the other family (Triad C) used a tripod with the smartphone to capture the videos. During the baseline condition, the coach provided no communication strategies or feedback to parents. During videos, parents and their children communicate with each other using the activities previously agreed upon, and parents were allowed to provide communication devices to the child.
Telepractice coaching intervention condition
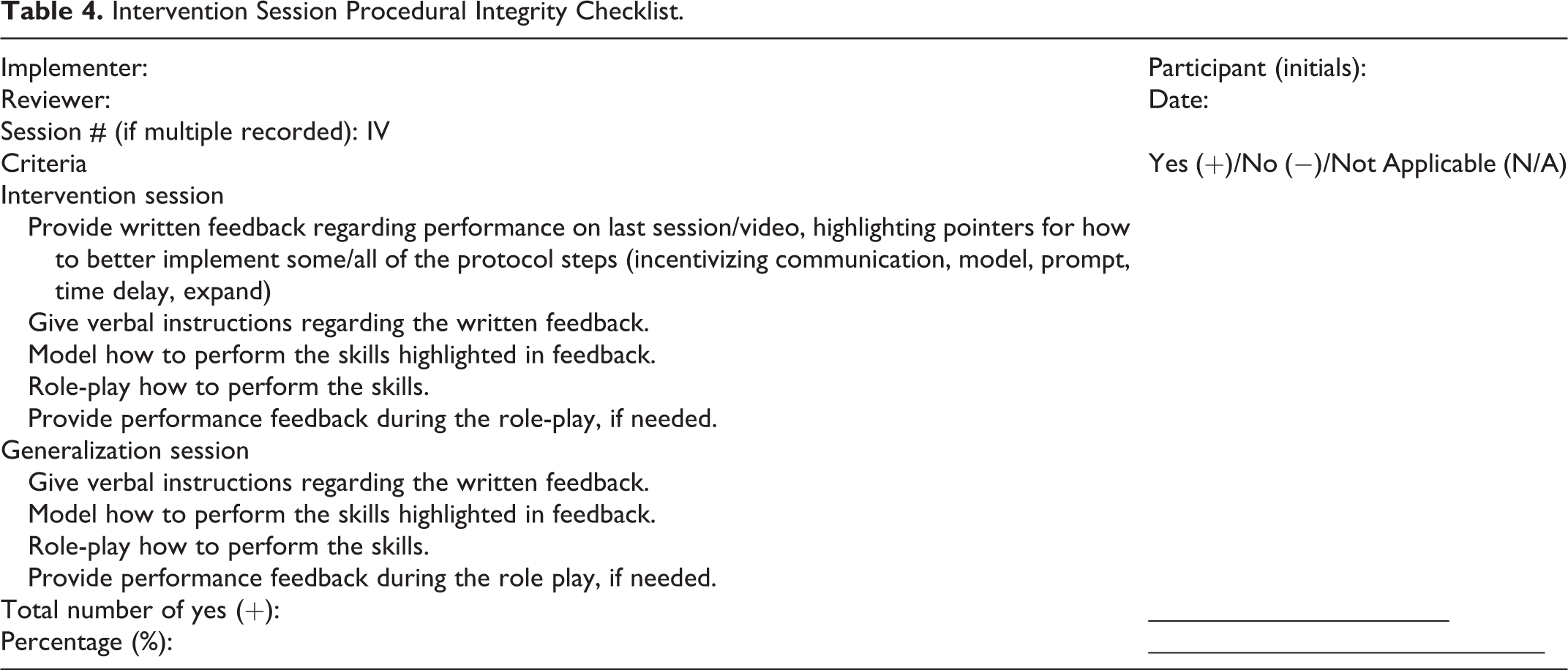
Parents received verbal and written weekly feedback and communication strategies by the coach via videoconference based on the video recording that each parent uploaded. Through the videoconference procedure, the coach instructed parents on specific ways to improve their communication with their child and clarify how to implement intervention strategies via interaction and role-play. The coach pointed out specific instances of communication strategies to parents while watching the recorded videos with the parents. Feedback began with what parents did well, then moved to what they could improve, and their goals for the next week. These were provided in written form and discussed verbally during the weekly meeting. The coach used the weekly feedback form, a detailed checklist of communication strategies (see Online Appendix 2). Parents then practiced the communication strategies (e.g., incentivizing communication, modeling, prompting, prompt fading, expanding) with their child as much as they could during the week. Only one to two videos per week were recorded and uploaded to Google drive for review and data collection by the coach. The coach encouraged parents to practice all taught strategies with their child. Prompting was faded after the children progressed enough in their communication skills to no longer be dependent on the prompt. The intervention condition was conducted in each family’s natural setting and used each child’s preferred items or activities. Further details, including fidelity of implementation for the parent-coaching procedures, are provided in the companion paper (Wattanawongwan et al., 2020). See Table 4 for intervention condition procedural integrity checklist.
Intervention Session Procedural Integrity Checklist.
Maintenance
Maintenance condition was conducted 3 and 6 weeks after the last intervention session. Parents provided the communication strategies to their child during the maintenance condition and uploaded one video to the cloud drive before the booster coaching session from the coach. No coaching sessions were provided to parents for 3 weeks prior to the probe data in the maintenance condition. The coach provided feedback about each weekly communication strategy to each parent during the booster session. The setting and activities used when working on communication skills with their child were the same as with the intervention condition.
Generalization
During generalization, parents provided communication strategies to their child using different settings, activities, and/or people based on each family’s preference. Generalization data were collected at least 1 and up to 4 times per condition across all conditions for each participant. Dyad A, Dyad B, and Dyad D chose providing strategies with different people for the generalization condition (e.g., dad for Dyads A and D, brother for Dyad B).
Triad C provided a generalization condition using different activities, people, and settings. The coach changed the generalization from activities (dinner time) to setting due to the child already making progress in requesting skills at dinner time. However, the parents tried to provide the generalization skills in a different setting (outside), saying this was not their normal routine activity. Then, they decided to do generalization with different people (grandparents).
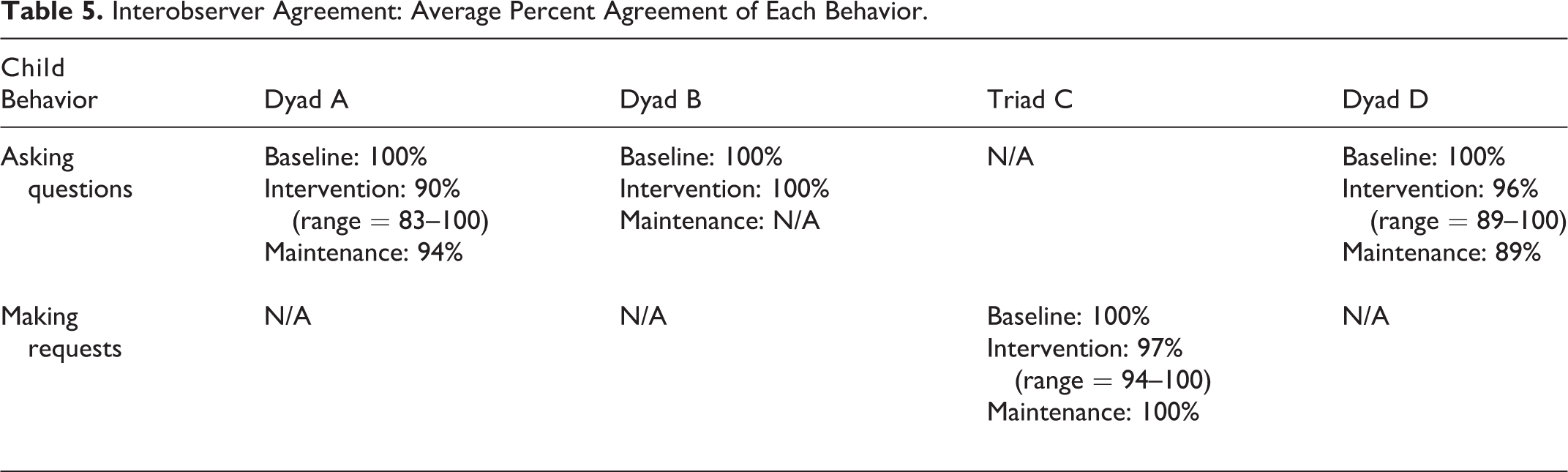
Interobserver agreement (IOA)
We calculated IOA via interval-by-interval agreement. IOA data were conducted for a 25%–50% of each condition (i.e., baseline, intervention, maintenance) for each participant. We calculated the IOA by dividing the total of agreement intervals by the total of agreement and disagreement intervals. Then, we multiplied that number by 100 to obtain the percentage number. The first author trained two doctoral students in collecting IOA and conducting procedural integrity. See Table 5 for average percentage of agreement of each behavior.
Interobserver Agreement: Average Percent Agreement of Each Behavior.
Data Analysis
Visual inspection
The child’s target communication behavior data were visually inspected to determine the promise of effect between the intervention communication strategies used by parents and the child’s behaviors. We compared data in level, trend, and variability within and across conditions for all participants (Byun et al., 2017; Gliner et al., 2000; Horner et al., 2005). The data also analyzed for immediacy, overlap, and consistency between conditions (Horner et al., 2005). Parent implementation of intervention components is graphed and analyzed in the companion paper (Wattanawongwan et al., 2020).
Effect size
Effect size scores of the child’s target communication behaviors were calculated via the Tau-U calculating program from the website for single-case research (Vannest et al., 2016). Tau-U scores indicated the effects degree between baseline and intervention conditions. Scores ranged between −1.0 and 1.0 for each child’s targeted behavior. A negative score indicates the decreasing of the child’s target behavior, and a positive score means the increasing of the target behavior (Parker et al., 2011). A recent review of research (Ganz et al., 2017) indicates that Tau-U values may be roughly interpreted as follows, for AAC interventions for individuals with ASD and intellectual or developmental disability: strong to very strong effects: 0.93–1.00, moderate effects: 0.80–0.92, low effects: 0.65–0.79, no to very low effects: ≤0.65.
Correlation
Pearson’s correlation coefficient (r) in STATA® (StataCorp, 2017) was used to determine the relationship between parent implementation of each intervention component and the child’s target communication behaviors. The data from the correlation determined the significant or insignificant correlations between variables of parent implementation of each intervention component and the child’s target communication behaviors.
Results
Data support a functional relation between parent implementation and children behaviors based on visual analysis. There was a significant positive correlation between all parent implementation of intervention components (incentivizing communication, modeling, prompting, and expanding) and children behaviors. A significant negative correlation was found between prompt fading and children behaviors, as expected.
A positive change in level and immediacy of effect was noted for the use of any intervention component as observed from baseline to intervention across all four participants. The magnitude of the effect of the dependent variable is larger for Triad C and Dyad B than Dyad A and Dyad B. Generalization data for any intervention component used are similar to baseline, intervention, and maintenance data for all three participants. The level and consistency of data for the independent use of the target skills for intervention and maintenance are similar across all three participants. In addition, there is little variability in intervention data for all participants. The level of child independent demonstration of the target skill in intervention showed almost no use of behavior components for Dyads A and B, whereas the data begin no use of behavior components and exhibit a positive trend for Triad C and Dyad D.
See Figure 1 for estimated count of engaged in any and independent target communication behaviors across all children. See the companion paper for an estimated count of engaged in behavior (Poisson correction) in any component behaviors across all parents (Wattanawongwan et al., 2020).

Estimated count of engaged in any and independent target communication behaviors across all children.
Participant A: Caleb
For Caleb, baseline data for asking any opinion question lie on or just above the x-axis (0%). A positive level change from baseline to intervention and a stable trend with little variability is characteristic of the intervention condition. Maintenance data are at the same level as intervention data. The level of the data from baseline to intervention increases and then stays the same from intervention to maintenance. Data for the generalization of any asking behaviors are similar to baseline, intervention, and maintenance data. Data points for independent communication in baseline are characterized by a stable trend and minimal variability.
Baseline data for independently asking opinion questions were 0%. A small-level change from baseline to intervention is noted. A stable trend with limited variability for independently asking questions is observed during the intervention condition. A decrease in level for independent behaviors from intervention to maintenance is mentioned. No distinct-level changes were noted for any of the conditions. Generalization data are similar to the baseline, intervention, and maintenance data for independent behaviors.
Participant C: Wang
For Wang, baseline data for any requesting behavior lie on the x-axis. A positive level change between baseline and intervention data was observed for any requesting behavior, with an increasing trend having little variability in intervention data. Maintenance data are observed to be at a level consistent with intervention data.
Baseline data for independently requesting lie on the x-axis. No level change from baseline to intervention was noted. There is an increasing trend with little variability in the intervention condition for independently requesting. Maintenance data for making independent requests are at a similar level to intervention data. No definite level changes were noted in between conditions for independent behaviors. Generalization data for independent requesting behaviors are similar to baseline and intervention data. Generalization for baseline data is at a higher level than data in the baseline condition.
Participant D: Akemi
Akemi’s baseline data for any asking question behavior lie on or just above the x-axis. A positive level change for any asking question data is observed between the baseline and intervention conditions. An increasing trend with moderate variability describes the intervention condition for Akemi. Data for maintenance are at a similar level to data in intervention for any asking question behavior. Generalization data for any asking question data are at the same level as data at the end of intervention. There is a change in level between the baseline and intervention conditions but no definite change in level between the intervention and maintenance. Generalization data for any asking question behavior are at a similar level to data in baseline, intervention, and maintenance conditions.
Data for independent asking question behavior are similar to any asking question behaviors with the exception of the level in intervention and maintenance. Any asking question behavior data are at a higher level than independent asking question behaviors in both the intervention and maintenance conditions.
Effect Sizes for Child Independent Target Behaviors
Researchers evaluated effect sizes to support visual inspection of the results of children’s behaviors across the three participants. Dyad B was excluded from the effect size calculation based on the short period of their coaching session. The children’s target behaviors were selected by each family based on their child’s current level of communication and their needs. Communication behaviors included requesting and asking questions. The overall omnibus effects demonstrated a strong effect size of 0.90. See Table 6 for effects of parent implementation intervention on independent target behavior in children.
Effects of Parent Implementation Intervention on Independent Target Behaviors in Children.
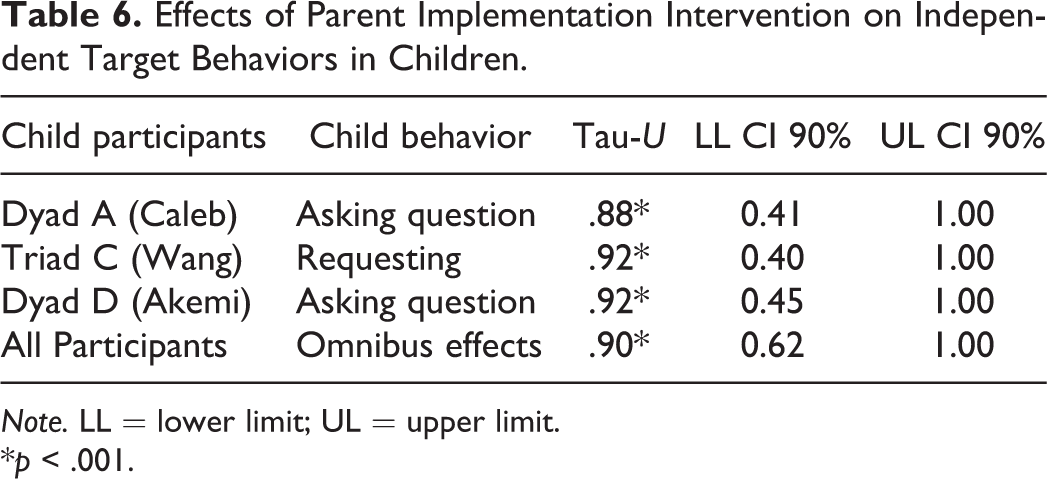
Note. LL = lower limit; UL = upper limit.
*p < .001.
For each target behavior, all participants demonstrated a moderate effect size. The effect size for Dyad A (Caleb) was 0.88 for asking questions. The effect size for Triad C (Wang) was 0.92 for requesting. The effect size for Dyad D (Akemi) was 0.92 for asking questions. There was a significant positive correlation between all parent implementation of intervention components (incentivizing communication, modeling, prompting, and expanding) and children behaviors. A significant negative correlation was found between prompt fading and children behaviors. The results of the correlational analysis are presented in Table 7.
Pearson’s Correlations Between Parent Implementation of Intervention Components and the Children’s Use of Target Behaviors.
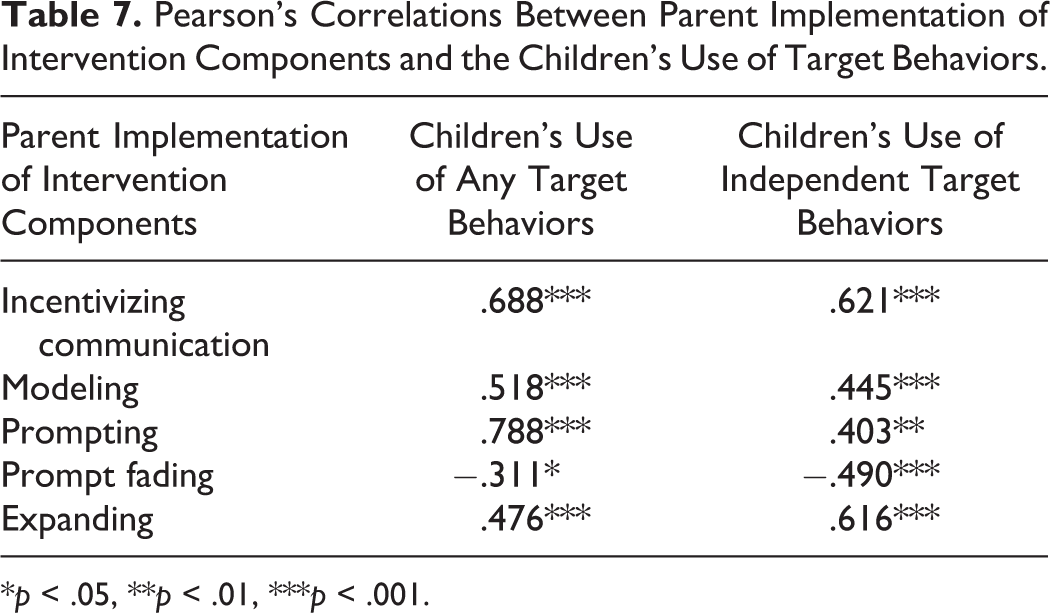
*p < .05, **p < .01, ***p < .001.
Correlations Between Parent Implementation and Child Communication
There was a significant strong positive correlation between children’s use of independent target behaviors with parent implementation of incentivizing communication (r = .621, p = .000) and expanding (r = .616, p = .000). Modeling (r = .445, p = .000) and prompting (r = .403, p = .00) were statistically significant with a moderate positive correlation.
All parents implemented prompting to their child until the child’s target behavior increased, then parents started prompt fading. Prompt fading contributed to the improvement in children’s independent target behavior. A significant moderate negative correlation was found between children’s use of independent target behavior and prompt fading (r = −.490, p = .000), as anticipated.
Discussion
Data from this study suggest that our telepractice parent coaching model had a positive impact on child outcomes. Visual inspection of the data indicates that the children made gains, both in all target communicative behaviors, which included prompted behaviors, and in independent use of target communicative behaviors. Furthermore, for each participant, there was a narrowing of the gap between the two, indicating that most of their communicative behaviors were independent by the end of intervention. Also of interest, maintenance data indicate that the children maintained these skills over a month past cessation of intervention and generalization data appear to follow the pattern of the target behaviors, which is promising. Effect size results for the participants indicate strong effects and gains indicated via visually inspecting the data. Finally, correlations between parent use of each of the components of the intervention and their children’s communication outcomes were positive for all components with the exception of prompt fading, which was negatively correlated, as expected. That is, prompt fading by the parents was associated with an increased use of independent child communication, which was expected and an indicator that parents, with telepractice coaches’ input, were able to gauge when it was appropriate to fade prompts rather than overusing them.
This study extends prior research on the use of telepractice to instruct parents of children with ASD. For example, prior studies primarily focused on parent implementation skills, with a few exceptions (e.g., Ingersoll et al., 2017; Vismara et al., 2018). The current study measures the distal child outcomes and evaluates the correlation between parent frequency of implementation and child frequency of use of new communication skills. This multilayer intervention (i.e., coaches instruct parents, parents instruct their children) design does not allow for establishment of a functional relation related to the child communication; however, the novel use of correlation analyses provides promising evidence for telepractice coaching of parents to use simple behavioral strategies. Furthermore, this study relies on direct observational data, unlike some of the prior research (e.g., Kuravackel et al., 2018), at the individual child level, over time. Further, prior literature on the use of telepractice to instruct parents of children with ASD primarily focused on addressing challenging behavior (e.g., Bearss et al., 2018; Simacek et al., 2017; Suess et al., 2014) or imitation (e.g., Wainer & Ingersoll, 2015). However, the current study expands prior work relating to child communicative behaviors. This study also affirms the importance of designing interventions for families that are both effective (Baharav & Reiser, 2010) and also acceptable to family members and feasible for them to implement (Boisvert & Hall, 2014; Wainer & Ingersoll, 2013). This is particularly critical during times of disaster; however, such considerations would be particularly beneficial for families that are normally unable to reach high-quality services due to time constraints, geography, or cost (Ingersoll et al., 2017).
Limitations
The work does have some limitations. For one, because the child behaviors reported here are collateral, or distal targets, we did not implement a design with the children that allows us to state that the children’s improvement was due to our parent coaching treatment. That said, the correlation results are fairly compelling. Two, the data are quite variable, which may make them more difficult to interpret, although we expected this to be the case, as the parents were instructed to implement as felt natural, rather than giving a particular target. Three, one dyad withdrew from the project, the only adolescent participant. While the parent provided an explanation, the child refused to make a video recording to be shared with the telepractice coach, it remains unclear whether or not this withdrawal could have been prevented had the approach been better adapted for this age-group or to accommodate the family’s schedule. Four, the videos were short and selected by the parents; thus, it is possible that the data may have demonstrated fewer gains had a more random selection of activities been recorded. Unfortunately, given that the families were located throughout a large state, it would not have been feasible for the researchers to collect weekly video clips themselves and short clips were chosen so as to be feasible to the parents and encourage continued participation. Five, we used the time sampling method, 10-s partial interval recording measurement, to measure the dependent variables for both parents’ behaviors and child’s communication behaviors. We should consider using Poisson correction to determine adjustments for computing accurate data (Yoder et al., 2018).
Future Research
This line of work suggests several paths for future research. Anecdotally, we noted, as we viewed videos of the families, that participant affect and quality of interactions between parents and children appeared to improve over the course of the study. Future research would be beneficial measuring outcomes such as parent report of their beliefs of the efficacy of this approach on their children’s outcomes and observational data on the affect and quality of interactions between parents and children over the course of the intervention. Our maintenance data were collected no more than 6 weeks following the final core coaching session; future research should measure longer term outcomes. Study of similar approaches involving instruction of peer and sibling and other natural communicative partners via telehealth is warranted. Finally, a cost analysis comparing implementation of telepractice coaching versus in-home coaching should be conducted to provide evidence that this practice is both efficacious and potentially less expensive for payers, such as insurance providers and local education agencies (Heitzman-Powell et al., 2014).
Implications for Practice and Research
This study has a number of implications for practitioners, particularly in light of the evidence in favor of efficient and potentially cost-saving approaches such as telepractice. The growth observed throughout the telepractice coaching intervention, however, is indicative that long distance, intensive, short-term, individualized coaching of authentic communicative partners can have positive outcomes that can be maintained following the cessation of treatment and that can generalize to untargeted child communication behaviors. Providing such instruction to parents, who are with their children the most and longest, is a critical approach to addressing communication deficits, particularly given that communication is ubiquitous across contexts. Furthermore, this article extends beyond current methodological standards in a number of ways and serves as a model for other single-case researchers (Ganz & Ayres, 2018). The use of correlations, as conducted in this study, is certainly beyond what is typically reported in single-case designs. Further, we paid particularly careful attention to currently suggested methodological standards for single-case design, including thorough descriptions of participants and implementers, collection of extended generalization and maintenance data, and implementation in natural contexts.
Conclusion
This carefully designed study provides evidence of correlation between parent implementation of multimodal communication intervention components and the children’s communicative behaviors within the context of a telepractice parent coaching approach. Further work is needed to expand this body of literature to include more study of parent-implemented multimodal communication intervention and the impact on their children’s communication outcomes. Despite some limitations, this is a promising evaluation of strategies to increase communication in children with ASD across natural contexts.
Supplemental Material
Supplemental Material, Appendix_1_companion_paper_(authors,_in_press) - Communication Intervention Implementation via Telepractice Parent Coaching: Child Outcomes and Correlations
Supplemental Material, Appendix_1_companion_paper_(authors,_in_press) for Communication Intervention Implementation via Telepractice Parent Coaching: Child Outcomes and Correlations by Sanikan Wattanawongwan, J. B. Ganz, Lauren M. Pierson, Valeria Yllades, Ching-Yi Liao and Sarah K. Ura in Journal of Special Education Technology
Supplemental Material
Supplemental Material, Appendix_2_Weekly_feedback_form_(1) - Communication Intervention Implementation via Telepractice Parent Coaching: Child Outcomes and Correlations
Supplemental Material, Appendix_2_Weekly_feedback_form_(1) for Communication Intervention Implementation via Telepractice Parent Coaching: Child Outcomes and Correlations by Sanikan Wattanawongwan, J. B. Ganz, Lauren M. Pierson, Valeria Yllades, Ching-Yi Liao and Sarah K. Ura in Journal of Special Education Technology
Footnotes
Authors’ Note
The opinions and conclusions expressed in this document are those of the authors and do not necessarily represent the opinions or policy of the THECB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in whole or part by grants from the Texas Higher Education Coordinating Board (THECB) Autism Grant Program and Coach to Communicate (C2C): Partnering to Improve Communication for Individuals with Autism (Awards No. 17108 and 20465).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.