
Abstract
The study aimed to assess the attitudes of laypeople toward clinical placebo use. One of three imaginary stories was presented randomly in a popular news portal and participants (6,404 individuals) were asked to rate nine statements about it. In the stories, placebo therapy was used in a deceptive way. Following the success of the treatment, the patient was informed that the remedy contained no active substances. Along with self-report of attitudes, questionnaires measuring dispositional optimism, somatosensory amplification and beliefs about the scientific validity of complementary and alternative medicine and holistic health were also completed. According to participants' ratings, helping patients is more important than avoiding deception. They did not think that they would have felt deceived in the described situation or that treatment would have been successful in a fully informed case. Patients' attitude toward deceptive placebo use appears to be more pragmatic than has been previously supposed.
Introduction
An extensive body of literature exists on various ethical aspects of clinical placebo use. There are both positive and negative arguments referring to effectiveness (Hróbjartsson & Gøtzsche, 2010; Rief et al., 2009), safety, and necessity (Foddy, 2009, 2011; Powell & Bailey, 2009). Furthermore, the doctor–patient relationship might also be affected: Is a positive placebo reaction the sign of a good therapeutic relationship (Brody, 2009), or rather does placebo use stand for missed opportunities for communication (Schenker, Fernandez, & Lo, 2009)? Is it paternalistic (Berger, 2009) by threatening patients' autonomy (Hester & Talisse, 2009), or can neither paternalism (Loewy, 2005) nor infringing on autonomy (Kolber, 2009) be the primal argument against placebos? Might it breach trust in the short term, or could it have even several long-term consequences (Cabot, 1909; Duffy, 2009; Golomb, 2009; Kanaan, 2009)? Summarizing the widespread arguments, the most significant underlying question appears to be that of whether patients are deceived or not. Under what conditions, and in the case of which expectations and consequences can one speak of “real” deception (Brody, 1982; Foddy, 2009)?
There are some forms of placebo use that can hardly be considered as nondeceptive. Such forms are for example to claim explicitly that an inert pill contains active substances or to prescribe placebos (treated as interventions) without any known therapeutic effect. Prescribing placebos without any further comment is also a subtle form of deception as patients implicitly expect active and effective medication (Cabot, 1909; Colloca & Miller, 2011). However, in the last decade scientific evidence about the effectiveness of placebo therapy in the treatment of various diseases and complaints has accumulated (Miller & Colloca, 2009; Pollo, Carlino, & Benedetti, 2011). It is also worth mentioning that deceptive administration of placebos (i.e., when patients are convinced that they received a potent pharmacological treatment) seems to be more effective than double-blind or conditional administration (i.e., patients are told that they receive drug-based or placebo-based treatment; Kirsch & Rosadino, 1993; Kirsch & Weixel, 1988; Pollo et al., 2001). These findings make the judgment about the ethical acceptability of placebo therapy more problematic (Foddy, 2011). What if a physician prescribes a placebo for a problem which is known to be placebo responsive after profound diagnostic processes do not discover any organic background to the complaint? Based on their own previous experiences and on available scientific evidence in similar cases, the doctor can claim that the patient has received an effective therapy. Following placebo administration, the patient's complaints end. As the treatment was successful, the physician admits that the given remedy contained no active substances. In this case, how would we define deception? Another question is what the patient's reaction would be. The arguments on these subjects are mere hypotheses without any empirical background. It is surprising, therefore, that one thing has almost completely been forgotten during the lengthy debate about and the quest for the patient's best interests—asking for the patient's opinion (Fassler, Meissner, Schneider, & Linde, 2010).
There has been little research on patients' opinion regarding clinical placebo use recently (Berthelot, Maugars, Abgrall, & Prost, 2001; Chen & Johnson, 2009; Lynöe, Mattsson, & Sandlund, 1993). A questionnaire study completed by 300 rheumatology inpatients and 100 nurses working in the same French teaching hospital focused on the beliefs about placebo effects in the context of double-blind placebo-controlled trials on the treatment of pain (Berthelot et al., 2001). Ethical aspects were considered only in the minority of the questions. According to the results, 45% of the patients would encourage their physicians to use placebos, if needed, to improve quality of care. Moreover, 27% believed that physicians should tell their patients the truth. Most of the patients (64%) thought that it would be wrong to sell placebos in pharmacies or in outlets other than pharmacies (83%). Also, 15% of the patients believed they had received placebos in the past, while 28% said they would agree to take them. In New Zealand, 211 general practice patients of two primary care clinics participated in a questionnaire study investigating (1) how amenable patients are to the use of placebos in clinical practice, (2) their willingness to participate in a placebo-controlled clinical trial, and (3) their beliefs about the placebo effect (Chen & Johnson, 2009). Items of the questionnaire (Attitudes to Placebo Treatments scale) were short stories about a medical situation where participants were asked to express what they believed to be the right action for a doctor to take. According to the results, placebo use was considered more appropriate when it was used for the benefit of the patient, was at the patient’s request, or when there seemed to be no other available treatment. In contrast, placebo use was considered inappropriate when it was used for the benefit/benefits of the physician or in situations where it seemed use would be dangerous and without possible benefits to the patient. Interestingly, a significant difference between the answers of males and females was found, suggesting that male patients are more likely to view placebo use as more appropriate. Regarding patients' beliefs, the authors concluded that most patients are not well informed and have misconceptions about the placebo effect. A study conducted in Sweden investigated the opinion of 83 patients and 94 physicians focusing on the presence of paternalism in medical practice by the help of three case histories, one of which dealt with clinical use of placebo treatment and two with the use of not indicated drugs, for example impure placebos (Lynöe et al., 1993). As the use of impure placebos was demanded by the patients themselves, only one of the stories dealt with the aspects of the placebo problem that are discussed here. Judging by this case, namely giving placebo to a terminally ill patient, the majority of patients believed they could accept this treatment if there were only a minimal risk of the patient discovering what was going on. In summary, patients accepted placebo use in certain situations, and male patients usually seemed to be more likely to do so.
Our goal was to investigate patients' standpoint on clinical placebo use. We focused on the issue of deception by asking laypeople (i.e., actual and possible patients) to judge a medical situation in which all the conditions were ethical except for the lack of an explicit description of the remedy as pharmacologically inert, that is, as a placebo before administration. We also attempted to investigate the possible determinants of patients' ethical standpoint by asking them to complete several attitude and personality scales. We assumed that people with a holistic view of health and illness or with positive attitude toward complementary and alternative medicine (CAM) would be less strict in ethical judgment. Moreover, as more optimistic individuals seem to react better to placebo treatment (Geers, Helfer, Kosbab, Weiland, & Landry, 2005), a further assumption was that more optimistic patients would be more permissive in the question of placebo use. Finally, our fourth hypothesis was that people who are more sensitive to possibly pathological body processes (e.g., to pain) might be more pragmatic in this question. In other words, they would prefer relief of suffering over avoiding deception.
Methods
Participants
A questionnaire had been presented on a widely used Hungarian Internet news portal for a period of 5 days as a study investigating issues on illness and treatment. A total of 7,521 individuals completed the questionnaire. After excluding participants with missing data on age, gender, educational qualification, patient status (see later), or on any of the ethics-oriented questions, and participants under 18 years of age, 6,404 completed questionnaires (85.1%) remained. Of the included participants, 60.7% were males, mean age was 36.0 years (18-90; SD = 12.21) and 38.4% received some kind of medical treatment in the last 3 years. As for participants' educational attainment, 1.4% had completed only their primary education, 29.4% secondary education, and 69.2% had an academic degree (bachelor or above). Several weeks later, the issue concerning ethical and practical aspects of clinical placebo use was summarized in an article in the science section of the portal. The study has been approved by the Ethical Review Board of Faculty of Education and Psychology, Eötvös Loránd University, Hungary.
Survey Instrument
First, participants were asked to answer questions concerning age, gender, educational attainment, and patient status (“Have you received any medical treatment in the last three years?”). Next, personality and attitude tests were completed (Holistic Complementary and Alternative Medicine Questionnaire [HCAMQ], Life Orientation Test–Revisited [LOT-R], and Somatosensory Amplification scale [SSAS], see below). Finally, participants were asked to read a short, imaginary story (it was chosen randomly from three similar stories, see below) and to answer questions about it. At the end of the questionnaire participants received a contact e-mail address for personal remarks and questions.
Personality Questionnaires
LOT-R (Scheier, Carver, & Bridges, 1994) is a 6-item scale that measures dispositional optimism as a generalized tendency of expecting positive outcomes. The Hungarian version of LOT-R proved valid and internally consistent (Cronbach’s α = .77-.81) in previous studies (Bérdi & Köteles, 2010). Its internal consistency was 0.83 in the present study.
SSAS (Barsky, Wyshak, & Klerman, 1990) refers to the tendency to experience a somatic sensation as intense, noxious, and disturbing. The 10-item questionnaire assesses sensitivity to mild bodily sensations that are uncomfortable and unpleasant but not necessarily pathological. The Hungarian version proved to be valid and psychometrically sound in previous studies (Köteles et al., 2009). Its Cronbach's α coefficient was .65 in the present study.
HCAMQ (Hyland, Lewith, & Westoby, 2003) consists of two correlating subscales: six items relate to beliefs about the scientific validity of complementary and alternative medicine (CAM) subscale and five to beliefs about holistic health (HH subscale). Cronbach's α coefficients for the two subscales of the Hungarian version were .81 and .68, respectively.
Stories
To avoid bias due to stereotypes connected to one particular illness, three different stories about different medical conditions were used in the research. The fictive stories were similar to each other in the following aspects: (1) there is a patient with a problem which is known to be responsive to placebo treatment; (2) appropriate medical diagnostic processes show no organic background; (3) the patient receives a medication from the doctor and the complaints end; (4) following the treatment, the physician admits that the medication contained no active substance, but (5) he has often achieved good results with it previously in similar cases; furthermore (6) he always informs his patients about the true nature of the treatment, even if it is not successful in the particular case. The word placebo was not used in any of the stories or in the questionnaire in order to avoid negative connotations.
Story A (insomnia)
There is a patient who has great difficulty falling asleep at night and wakes up tired in the morning. Extensive diagnostic procedures show no organic problems. The physician orders a pill which eliminates the complaints completely. The physician tells the patient later that the pills contained no effective substance, but it proved to be useful in similar cases, therefore he holds it effective and he orders it if necessary. Moreover, he always informs his patients about this treatment regardless of its effectiveness in the particular case.
Story B (irritable bowel syndrome [IBS])
There is a patient with meteorism, painful abdominal spasms, and sometimes loose stools. [From here, it is the same as Story A]
Story C (lower back pain)
There is a patient with lower back pain that has persisted for months. [From here, it is the same as Story A]
Questions and Statements About the Stories
All questions and statements were to be answered on a 5-point Likert-type scale (1 = strongly disagree/not at all; 2 = disagree/not really; 3 = can't decide/don't know; 4 = agree/to some extent; 5 = strongly agree/fully).
If it had happened to you, would you have felt deceived?
To what extent could you trust your doctor in the future?
Would your own complaints be alleviated or cured in a similar case?
The most important goal of a physician is to improve the condition of the patient, therefore the use of a medication containing no effective substance is acceptable in this case, even in the absence of previously informing of the patient.
Deception of the patient is to be avoided at any cost, therefore the use of a medication that contains no effective substance cannot be accepted without previously informing the patient.
No real deception happened in this case.
Informing the patient in advance would have been better.
The treatment would have been successful even if the patient had known that the medication contained no effective substance.
I find this research interesting.
Data Analysis
Data were analyzed using SPSS version 17 software. In order to assess participants' ethical standpoints more reliably and to avoid multiple statistical comparisons, the ethics-oriented questions (Questions 1, 2, 4, 5, 6, 7) were subjected to a dimension reduction method. The remaining three questions were excluded from this analysis because they refer to other aspects of the story (Questions 3 and 8: expected effectiveness of placebo-therapy; Question 9: personal interest). As data proved to be appropriate for a multivariate analysis (Kaiser-Meyer-Olkin (KMO) index = 0.893; significance of Bartlett's test <0.001), exploratory factor analysis was applied using maximum likelihood method for extraction. Only the first factor's eigenvalue (4.074, explaining 67.9% of total variance) was above 0, therefore a one-factor solution was used. This factor, called ethical standpoint, was used for further analysis. Means of the ethical standpoint variable across the three stories were compared by one-way analysis of variance and by a post hoc analysis using Bonferroni corrections. As the ethical standpoint variable was not normally distributed, nonparametric methods were used for further analysis. Differences in ethical standpoint scores related to participants' gender and patient status were investigated using Mann-Whitney tests, effect sizes were calculated using the formula r = Z/√N. Correlations between participants' ethical standpoint score and other assessed variables were estimated by Kendall's tau b coefficients.
Results
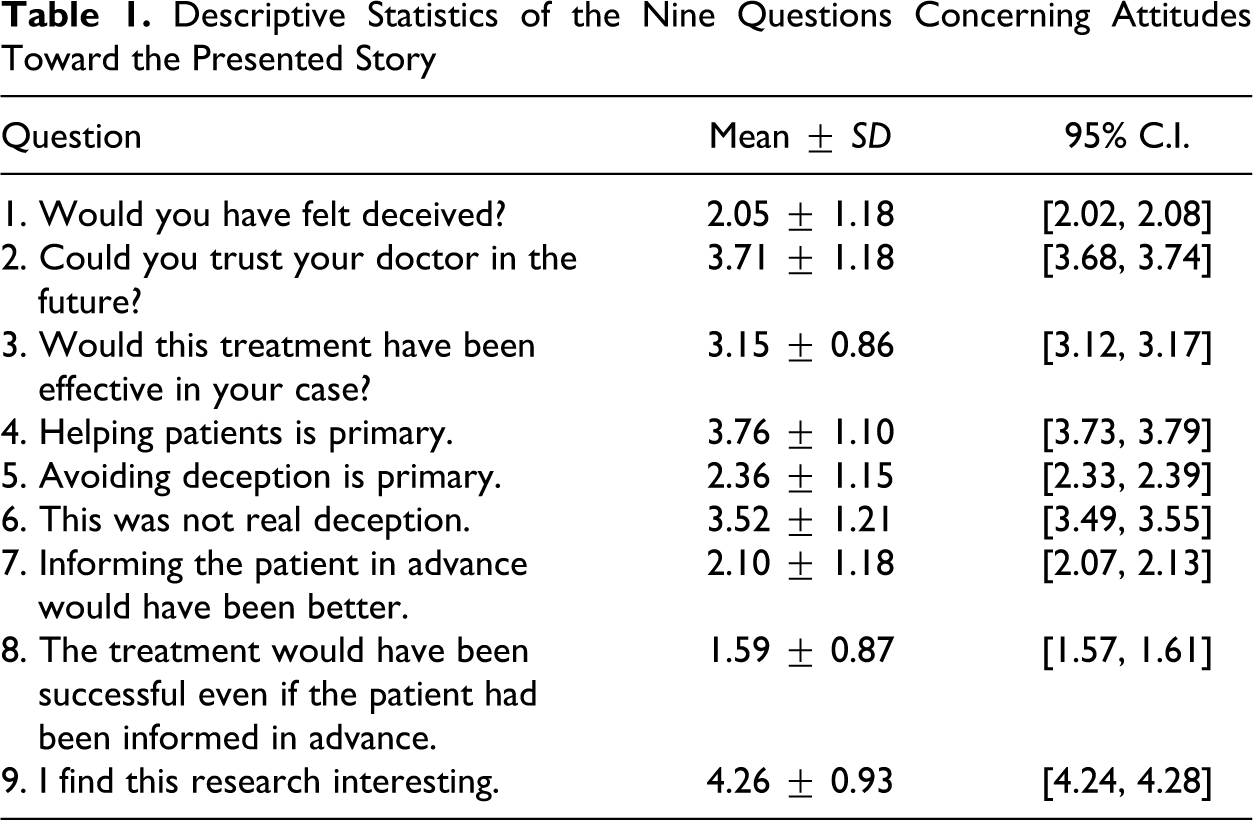
Descriptive statistics of the nine questions concerning the story and the problem are presented in Table 1.
Descriptive Statistics of the Nine Questions Concerning Attitudes Toward the Presented Story
Absolute values of loadings of the six ethics-related questions on the ethical standpoint factor were about or above 0.7 which indicates a high level of conceptual consistency. The positive end of the ethical standpoint factor represents an overall preference of avoiding deception, while the negative end represents a more utilitarian approach (e.g., helping patients is preferred).
The three stories were rated differently by the participants (means and SDs of ethical standpoint scores): Story A (insomnia) was rated lower (−0.88 ± 0.91, N = 2,202) than Story B (IBS; 0.03 ± 0.97, N = 2,140) and Story C (lower back pain; 0.06 ± 0.98, N = 2,062). According to the results of the analysis of variance, differences among the ratings were significant, F(2) = 14.562, p < .001. Post hoc analysis showed no significant difference between Story B (IBS) and C (lower back pain), while both of them scored higher (p < .001) than Story A (insomnia).
Mann-Whitney tests revealed significant (p < .001) differences between genders and between patients and nonpatients (Z = −10.818 and −4.183, respectively): women had higher scores than men on the ethical standpoint variable (mean ranks were 3,001.36 for men and 3,512.92 for women) and individuals that had received some form of medical treatment in the last 3 years scored higher than people without any treatment (mean ranks were 3,278.86 and 3,080.24, respectively). Effect size calculations indicated a small effect for both cases (r = .13 and .05, respectively).
Table 2 summarizes the results of correlational analyses on the relationships between ethical standpoint and participants' educational qualification, age, and questionnaire scores. The ethical standpoint was practically not influenced by participants' educational qualification, age, and SSAS score (the latter two correlations were statistically significant but very weak). Dispositional optimism, holistic attitude toward health and illness, and positive attitude toward CAM methods showed weak negative correlations (between −0.15 and −0.11) with participants' ethical standpoint.
Correlations Between Participants' “Ethical Standpoint” Score and Other Assessed Variables
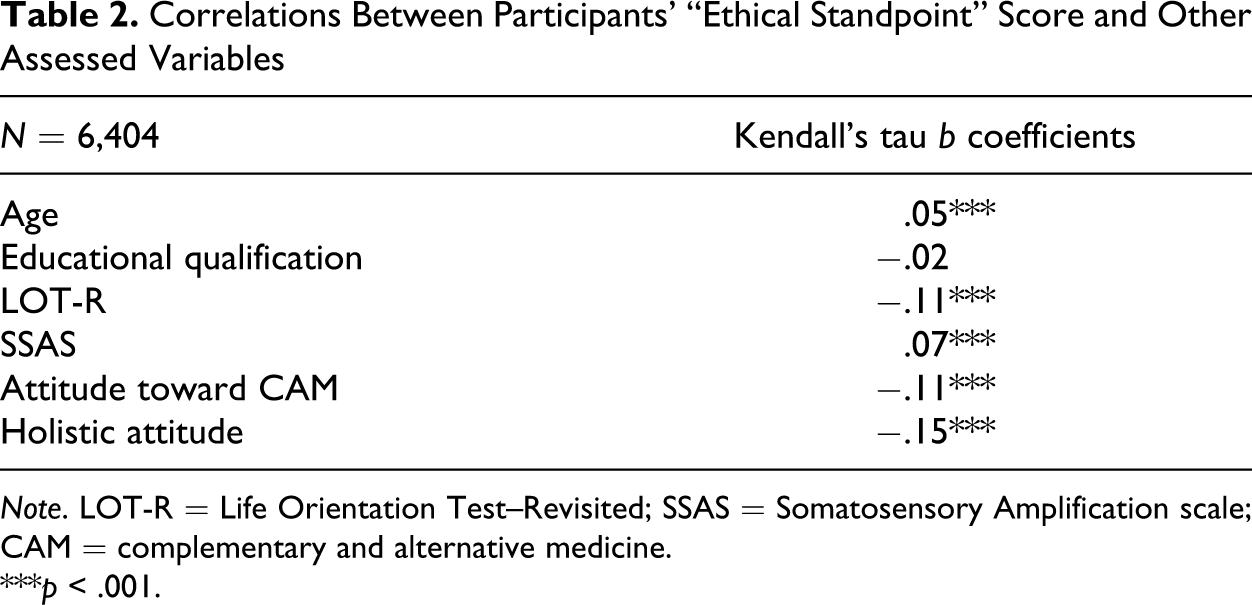
Note. LOT-R = Life Orientation Test–Revisited; SSAS = Somatosensory Amplification scale; CAM = complementary and alternative medicine.
***p < .001.
Discussion
According to the judgment of actual and possible patients: (1) effectiveness of a therapy is considered more important than the ethical issues surrounding deception (Questions 4 and 5). (2) Under the described conditions, placebo therapy is not considered genuinely deceptive (Questions 1 and 6). (3) The described form of deception is regarded as necessary for the therapeutic effect (Questions 7 and 8). (4) If the treatment proves to be effective, and patients receive information about it later, trust in physicians will not be damaged (Question 2). (5) Placebo treatment can be beneficial (Question 3).
Overall, these findings indicate that laypeople's attitudes toward deceptive placebo use appear to be more pragmatic than was previously supposed by health care professionals. However, the focus of the previous studies differs slightly from our investigation. Their results are basically in line with the recent findings. In the study made in France (Berthelot et al., 2001), almost half of the patients said that physicians should use placebos to treat their patients if needed to improve quality of care, and 73% of the patients who gave this reply said the physician should not tell the patients that the treatment was a placebo. The results of Chen and Johnson (2009) show that many patients are amenable to the use of deliberate administration of placebo in some circumstances (see above), suggesting—as the authors say—that the major issues of placebo use (deception and lack of informed consent) are tolerated by the patients surveyed. In the study conducted in Sweden (Lynöe et al., 1993), the majority of patients could accept placebo treatment in a terminal medical condition if there was only a minimal risk of the patient discovering what was happening. None of these results show the obligate preference of informed consent. The results are also in accordance with the attitudes and practice of Hungarian general practitioners (GPs) who seem to prefer patients' well-being over full, informed consent (Ferentzi, Köteles, & Bárdos, 2010, 2011).
As it can be seen in a systematic review (Fassler et al., 2010), placebos are still used in medical practice, despite the controversial ethical status of its usage. Although normative ethical rules cannot be delivered from descriptive ethics, for example from the mere description of people's beliefs about morality, it is worth to consider why people seem to be more permissive than ethicists or than what is normally expected. Health holds great value and if in a given situation both physician and patient want to achieve the goal of good health, they do not mind lowering their ethical standards. This is especially true if they are not aware of other alternatives (see below) and regard deception as necessary for successful placebo treatment. It is worth mentioning that placebo therapy without deception (i.e., with informed consent) is considered legal and acceptable (American Medical Association Council on Ethical and Judicial Affairs, 2006). Surprisingly, we have some evidence (although not conclusive) suggesting that placebo therapy without deception can also be successful (Aulas & Rosner, 2003; Kaptchuk et al., 2010; Sandler & Bodfish, 2008). Another proposed alternative might be authorized deception, such as informing the patients about the possibility of deception (Miller, Wendler, & Swartzman, 2005). Participants of the current study may not have been aware of these possibilities. Nevertheless, our results are quite clear-cut: if people have to decide, they clearly prefer being both deceived and cured to being neither deceived nor cured (Questions 7 and 8).
Connections between the participants' ethical standpoints and four personality-related correlates (positive attitudes toward (1) holistic view of health and toward (2) CAM-methods, (3) dispositional optimism, and (4) somatosensory amplification tendency) were hypothesized in the study. In the cases of the first three hypotheses, weak negative correlations (from −0.15 to −0.11) were found. As the positive end of the ethical standpoint variable refers to a less permissive attitude, the direction of these correlations is in line with the hypotheses. The magnitude of these correlations, however, shows very weak (i.e., practically negligible) relationships. Therefore, holistic worldview, preference of CAM-methods, and optimism have not proven to be important determinants of the ethical standpoint regarding clinical placebo use. Connections with proneness to somatosensory amplification were even weaker and in a positive direction. Thus, the fourth hypothesis can also be rejected.
As for the three different medical conditions mentioned in the stories, participants were more permissive regarding deceptive placebo therapy in the case of insomnia than in cases of IBS and lower back pain. This is an important finding as it might indicate the relative nature of ethical judgments. In the eyes of laypeople, insomnia may seem easier to alleviate and/or more placebo-responsive than the other two conditions because it appears to be a more “psychic” or brain-related complaint. As such illness-specific details were not investigated in our study, these are mere speculations. The existence of these differences, however, sheds light on further possible factors influencing participants' ethical judgments. This is in accordance with previous findings. The study conducted by Berthelot et al. (2001) shows that according to patients' opinions, the placebo-effect depends on the nature of the symptom (78%) and on the personality of the patient (91%). Similarly, Chen and Johnson (2009) found that 65% of the participating patients either agreed completely or agreed for the most part that the effectiveness of a placebo was dependent on the personality of the patient. Considering the further influencing factors of the ethical judgments around the decision making of placebo usage in a particular medical situation, it is worth highlighting that the distinction between placebo responders and nonresponders is highly problematic (Kaptchuk et al., 2008).
Males proved to be more permissive toward deception in placebo treatment, which is in accordance with previous empirical results (Chen & Johnson, 2009; Lynöe et al., 1993). According to the results of effect size calculations, however, participants' gender did not have a considerable impact on their ethical standpoints. As for participants' patient status, a less permissive attitude was expected in the patient group, as these people were more involved in the problem and therefore were supposed to be more sensitive to deception. Unfortunately, the difference between patients and nonpatients was even smaller than between males and females. Thus, no major determinants of ethical attitude were found in the study.
The most important shortcoming of the study is its imaginary nature. Picturing a story is far from being in a similar situation. Thus, one has to be cautious regarding the conclusions drawn from the results. On the other hand, experimental investigations of this issue appear to be impossible in an ethically permissible way. Moreover, as ethicists' theories are also about imaginary stories, asking laypeople to picture the same scene does not lead to less valid results. Some of the statements investigating ethical standpoints were rather evocative which could have had an impact on participants' rating. A further issue is that the results cannot be generalized to the whole population of Hungary because of the nonrepresentative sample. Completing the survey form online has its own further well-known limitations. Most importantly, only those who are interested in the issue participated in the study, albeit this does not necessarily mean a positive bias toward placebo use. Moreover, participants could have access to information sources discussing the problem in detail while answering the questions. It would be worth conducting further studies concerning patients' ethical standpoint on representative samples in other regions, as cross-cultural differences may exist.
Footnotes
Acknowledgments
The authors wish to thank Csaba Magyarósi (www.index.hu) for assistance in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Hungarian National Scientific Research Fund (OTKA K 76880) and by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences (for F. Köteles).