
Abstract
This study investigated the perceptions of short-term assignments of medical services among participating health care professionals dispatched from Taiwan to underdeveloped areas. Structured questionnaires were mailed to four groups of professionals (physicians, pharmacists, nurses, and public health personnel) who had participated in any of 88 medical missions dispatched to 24 allied nations. A total of 278 returns were valid for analysis. Among them, 222 respondents reported that they had participated in just one overseas medical mission (79.9%). The majority of physicians, pharmacists, and nurses listed humanitarianism as their foremost incentive for participation. In contrast, public health personnel most frequently reported that they had been assigned to the mission abroad. Pharmacists, nurses, and public health personnel most commonly stated that their top goal was health care; but physicians said that aiding Taiwan’s diplomatic relations was their main motive. While all groups generally recognized language proficiency and cultural awareness as important for conducting successful short-term medical aid missions (STMMs), many members of groups did not rate their own capabilities in those area as sufficient, especially pharmacists (p < .001). Orientation for participants and training for local health workers were seen as relatively insufficient. In conclusion, there are considerable differences in the thoughts about STMMs across four key groups of heath personnel. The findings can help inform efforts to integrate evidence into the deployment of STMMs.
Introduction
Increasing numbers of professionals are participating in global health activities, such as humanitarian medical aid missions (Bajkiewicz, 2009; Mulvaney & McBeth, 2009; Nelson, Lee, Newby, Chamberlin, & Huang, 2008; Panosian & Coates, 2006; Snyder, Dharamsi, & Crooks, 2011). Medical aid missions involve dispatching a group of experienced health care providers into resource-poor areas for volunteer services (Johnson, Stieglitz, & Schroeder, 2009; Khan, Pietroni, & Cravioto, 2010; Walsh, 2004). Such endeavors improve health for people worldwide and reduce the health disparity among populations. Moreover, they can provide significant benefits—to the health care workers themselves as well as to the patients (Dupuis, 2006; Johnson et al., 2009). The success of these efforts has the additional benefit of helping improve the willingness of health professionals to volunteer to serve in underdeveloped locations (Thompson, Huntington, Hunt, Pinsky, & Brodie, 2003).
Medical aid missions are categorized into short- and long-term operations. Over the years, as many long-term outreach medical services have been replaced by sector-wide approaches (Hill, 2002; Sundewall, Forsberg, & Tomson, 2006), there has been a shift in focus from long-term overseas assignments to short-term medical missions (STMMs). There are three main categories for STMMs: emergency-response, surgical, and mobile services (Bajkiewicz, 2009). Emergency-response services provide postdisaster medical relief anywhere in the world. Surgical services provide dental and surgical aid in regions where such services are generally unavailable. And mobile services provide clinics in outlying villages where medical care is either lacking or inadequate.
Despite the benefits of STMMs, concerns have been raised regarding their long-term impact on recipient communities (Green, Green, Scandlyn, & Kestler, 2009; Jesus, 2010). Constraints against such missions exist, such as a lack of follow-up care, short duration, too many patients, language and cultural barriers, limited medications and supplies, and a lack of support services from local authorities. How to reduce the risks to aid workers and the potential harm to recipients have been the challenges (Bishop, & Litch, 2000; Jesus, 2010; Solheim, 2010).
Although for decades, a variety of health care professionals have engaged in providing humanitarian aid through STMMs, few studies have examined their perceptions (Bjerneld, Lindmark, Diskett, & Garrett, 2004; Green et al., 2009; Hunt, 2009; Jesus, 2010). Most investigations of previous studies lack profiles of large sample size. To be able to potentially improve the provision of STMMs, quantitative studies aiming to the perceptions and attitudes of the humanitarian aid workers could help understand and monitor the possible strategies that can be put in place to improve the efficiency of implementing such missions.
The composition of STMMs varies according to the specific type of care provided. Health care teams may consist of physicians, nurses, pharmacists, and public health personnel, with physicians and nurses acting as the principal health professionals, and pharmacists and public health personnel also playing important roles (Mitka, 2005; Murray, 1999; Pezzella, 2006; Wolfberg, 2006). When implementing health care programs to supplement local health systems, it is essential to understand the differences between these health providers’ points of view.
Many Taiwanese health professionals have been called upon to provide short-term medical care to patients in underdeveloped countries. These efforts involve groups of health care personnel traveling to medically underserved areas, usually extremely far from Taiwan. In this article, we report the results of a questionnaire survey designed to explore the perceptions of Taiwanese health care providers toward short-term assignments of volunteer medical services in underdeveloped areas. We examined how STMMs are perceived in relation to experiences among physicians, nurses, pharmacists, and public health personnel. This study allows us to compare and contrast various levels of perceptions toward STMMs among four key groups of health professionals. Our data provide further impetus for integrating evidence into the deployment of STMMs.
Method
Study Population
We surveyed health professionals dispatched by the Taiwan International Cooperation and Development Fund (TaiwanICDF) to allied countries for medical aid missions between 2005 and 2010. Since 2005, the TaiwanICDF has coordinated with 37 hospitals to dispatch health professionals, in the form of STMMs, to Taiwan’s partner countries. These hospitals may assign their employees to participate in the missions.
One to two weeks before each mission was dispatched, the TaiwanICDF arranged a 2-hr standardized orientation for all participants. This included an introduction to the host nation and its medical problems, a mission schedule, and discussion of the duties of participating members. Each participant received a booklet about their mission and its location. The orientations were similar in quality. In addition, the TaiwanICDF sponsored all costs associated with the medical missions, including transportation and travel, daily expenses, logistical support, medication and supplies, laboratory work, and accommodation. Each medical aid mission lasted 1–2 weeks.
Questionnaire Development
The development of an instrument to assess STMMs was based on a comprehensive literature review of publications of existing questionnaires. The review led us to base our questionnaire on that of Maki, Qualls, White, Kleefield, and Crone (2008). That questionnaire survey was designed to evaluate the quality of care for STMMs. The current survey, which is available upon request, was adapted to Taiwan’s situation and was complemented with questions deemed important for our research targets.
The questionnaire was examined by five experts to establish content validity. Their expertise included global health, humanitarian aid (medical missions), survey methodology (statistics), international relations (diplomacy), and tropical medicine. Each of the experts has more than 20 years of work experience in their fields and fully understood the functions of the medical mission. After adjustments based on the experts’ advice, the questionnaire was piloted in a group of nine health professionals participating in STMMs to estimate internal consistency using Cronbach’s coefficient α. The final questionnaire was modified based on the feedback we received from this pilot. In this survey, the Content Validity Index of .94 and Cronbach’s coefficient α of .73 indicate sufficient validity and reliability of parameters in the questionnaire. The questionnaire was accompanied by an introductory letter that stated the purpose of this study and assured confidentiality.
The questionnaire consisted of items to measure motivation, expectations, beliefs, daily workload, and the efficiency of short-term medical services. Questions regarding efficiency covered orientation efforts, intrateam communication, utilization of time, training of local health workers, personnel, and interpreter services (Maki, Qualls, White, Kleefield, & Crone, 2008). Questions regarding belief and efficiency were rated by Likert’s 5-point scale (completely agree, agree, neutral, disagree, and completely disagree). The daily workload was estimated by number of hours.
Study Administration
The study was conducted by postal questionnaire and distributed to health professionals in a 4-month period from January through April 2011. The survey was anonymous. A return envelope with postage prepaid was attached to the questionnaire. The study protocol was approved by the Research Ethics Committee of the National Health Research Institutes, Taiwan.
Data Analyses
Likert’s 5-point scale was dichotomized for further analyses. A self-rating report of either agree or completely agree was regarded as a favorable answer. Statistical analyses were conducted using a commercially available program (SPSS 12.0 for Windows, SPSS, IL). Significance was defined as p < .05.
Results
Data Collection
Questionnaires were distributed to 425 health professionals; 278 returns with complete answers were valid for analyses (response rate: 65.4%). There was no significant difference in professional specialties between respondents and nonrespondents. The respondents included 143 physicians, 23 pharmacists, 86 nurses, and 26 public health professionals. Enrolled physicians included 34 internists, 17 surgeons, 19 pediatricians, 11 obstetrician–gynecologists, and 62 specialists.
Demographic Characteristics
Thirty-one respondents reported that their last mission had been in 2006 (11.2%), with 40 reporting the same for 2007 (14.4%), 47 for 2008 (16.9%), 84 for 2009 (30.2%), and 76 for 2010 (27.3%). A total of 222 respondents stated that they had participated in only one medical aid mission to date (79.9%). There were discrepancies among the four groups in the following characteristics: number of missions participated in, gender, age, marital status, and academic degree. Most physicians (81.1%), pharmacists (78.3%), and nurses (84.9%) reported that their current assignment was the first time they had participated in an overseas mission. In contrast, 42.3% of public health personnel had participated more than once in STMMs. The average age was 43.4 years for physicians, 39.3 years for pharmacists, 37.3 years for nurses, and 41.7 years for public health personnel. The work experience was 10–15 years for all four groups. Males were predominant among physicians (80.4%). In contrast, females were predominant among nurses (96.5%). In addition, marriage was most common among physicians (65.0%) and least common among nurses (29.1%). Furthermore, 9.6% and 26.6% of participants had an additional PhD or master’s degree, respectively. The academic degrees of pharmacists and nurses were lower than those of physicians and public health personnel (p < .001).
Location of Overseas Missions
During the 6-year study period, the TaiwanICDF organized 88 missions to 24 nations on 4 continents, including 11 nations in Latin America and the Caribbean (Guatemala, Honduras, Haiti, Saint Lucia, Nicaragua, Panama, El Salvador, Belize, Dominican Republic, Paraguay, and Saint Kitts and Nevis), 8 nations in the South Pacific (Kiribati, Papua New Guinea, Tuvalu, Palau, the Solomon Islands, the Marshall Islands, Fiji, and Nauru), 2 nations in Africa (Swaziland and Gambia), and 3 nations in Asia (India, Thailand, and Indonesia). Of the four overall areas, the South Pacific received the most participants (55.0%), followed by Latin America (36.0%), Asia (7.9%), and Africa (1.1%). A majority of participants (82.7%) were dispatched to Taiwan’s diplomatic allies, including six of the visited countries in the South Pacific and all of the visited countries in Latin America and Africa.
Workload of Participants
All groups of health personnel worked about 12 hr each day. Physicians, pharmacists, nurses, and public health personnel spent 7.4, 7.4, 7.8, and 5.6 hr on patient care, respectively. Health workers spent 1.3 hr daily on daily meetings and the same amount of time on helping educate local health workers.
Motivations for Participation
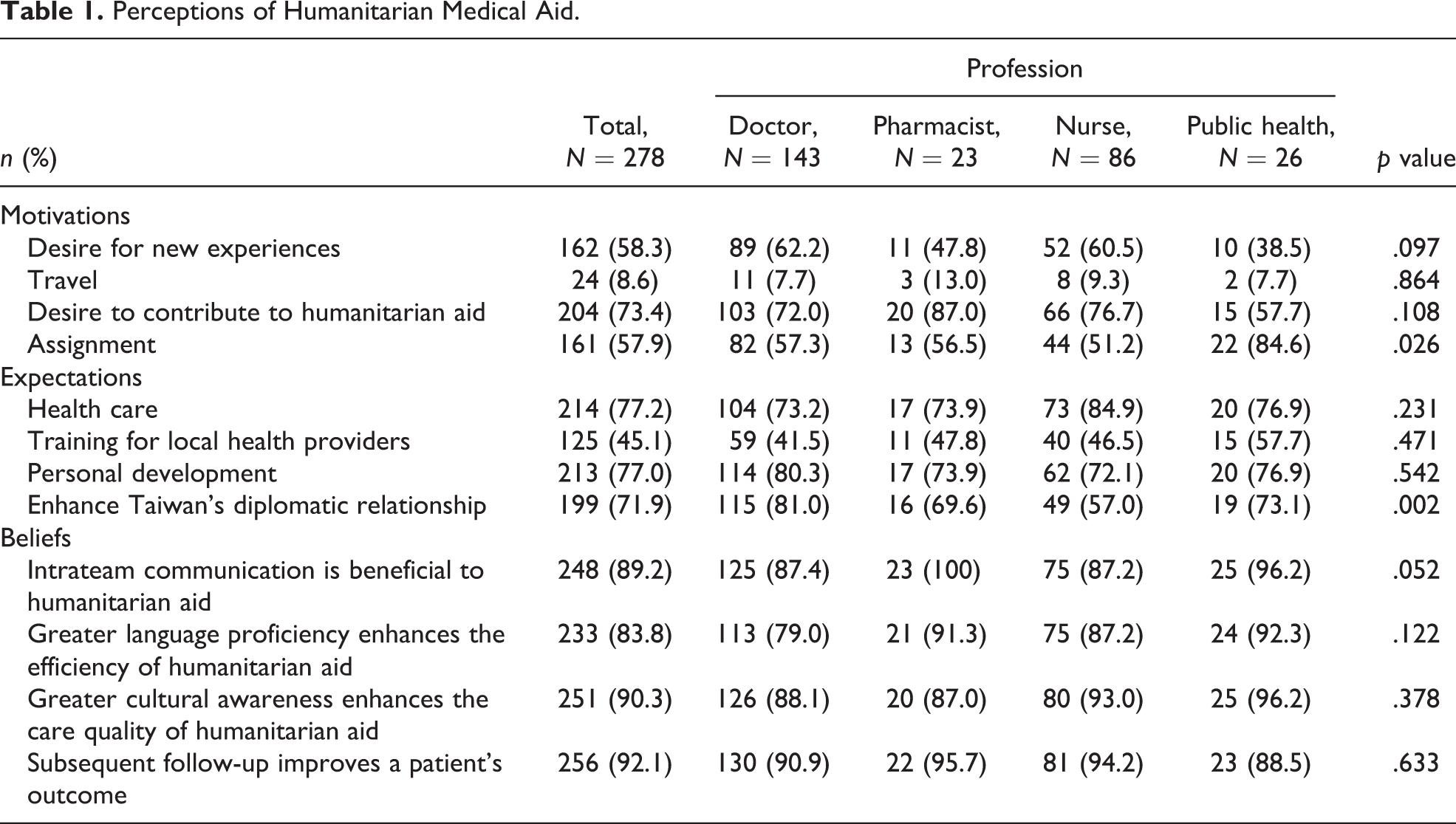
Overall, 68.0% of the health professionals expressed two or more motives for their participation in STMMs (Table 1). The most common motivation was the desire to contribute to humanitarian aid (73.4%), followed by the desire for new experiences (58.3%), assignment (57.9%), and travel (8.6%). There was a significant difference in the “assignment” category among the four groups, with it being much more common for public health personnel.
Perceptions of Humanitarian Medical Aid.
Expectations of Participation
The most commonly perceived goal to accomplish was health care (77.2%; Table 1). In addition, 77.0% believed that providing humanitarian aid would help their personal development. Furthermore, 71.9% perceived the STMMs as a means to enhance Taiwan’s diplomatic relationships. However, only 45.1% of participants perceived training for local health workers as an important goal. There was a significant difference among the four groups in the view of the importance of international diplomatic relations. Helping diplomatic relations as a goal of STMMs was more common among physicians than among the other professionals.
Facilitators of Efficiency
Overall, 89.2% of health professionals reported that they believed good intrateam communication is beneficial to the efficiency of STMMs (Table 1). Furthermore, 83.8% of health professionals believed that greater language proficiency enhances the efficiency of STMMs; and 90.3% believed that greater cultural awareness enhances the care quality of STMMs. In addition, 92.1% of health professionals believed subsequent follow-up can improve patient outcomes. There were no significant differences in these beliefs among the four groups.
Familiarization With Native Language and Local Culture
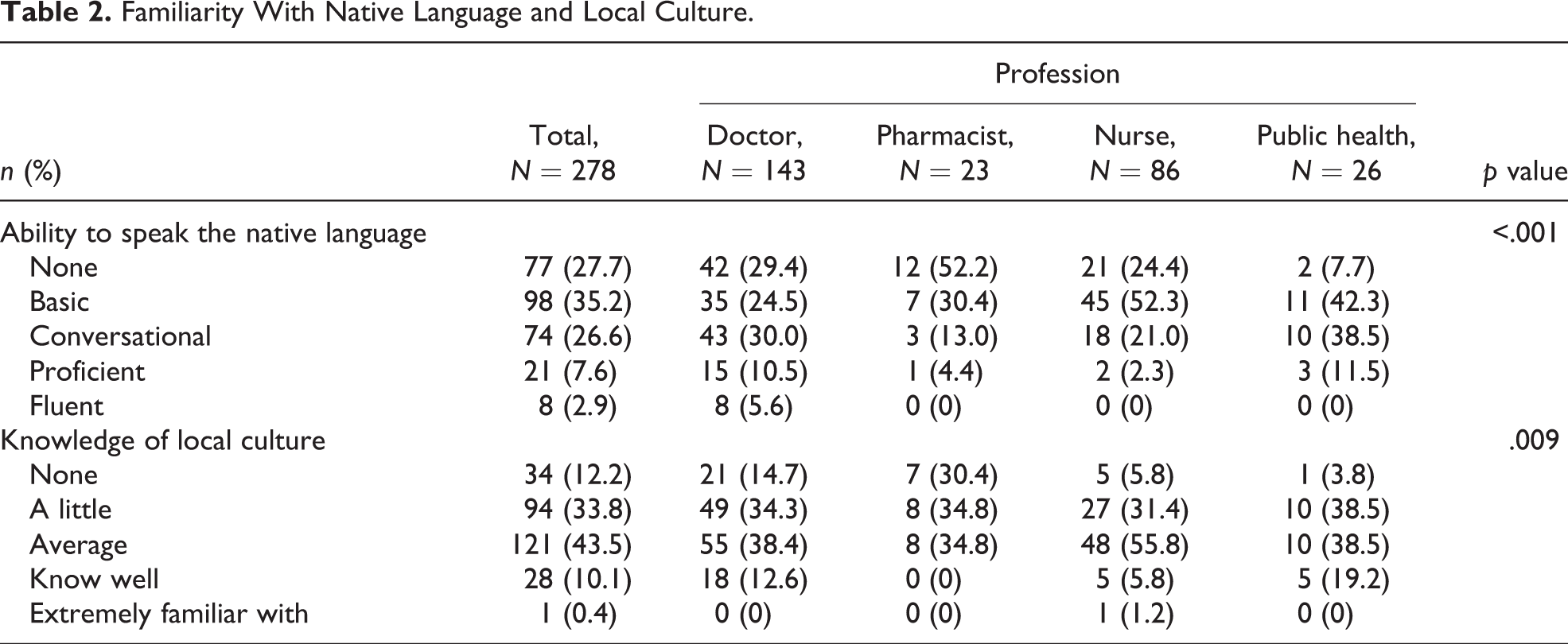
The degrees of familiarization with the native language and local culture are shown in Table 2. There was a significant difference in the language proficiency among the four groups (p < .001). Language proficiency was relatively deficient, especially among pharmacists. Approximately 50% of physicians and public health personnel claimed to have the ability to converse about health care in the local language. In addition, there was a significant difference in the knowledge of local culture among the four groups (p < .01). Pharmacists had less knowledge of local culture than the other personnel.
Familiarity With Native Language and Local Culture.
Efficiency in the Implementation of STMMs
Overall, satisfaction was greatest with interpretation services (95.3%), followed by efficient utilization of time (82.0%), intrateam communication (77.3%), sufficient personnel (76.7%), orientation conference (63.5%), and training of local health workers (48.2%). There were no significant differences in the above six areas among the four groups (data not shown).
Comparison of Perceptions of STMMs: Experienced Versus Nonexperienced Participants
To further understand whether experience is associated with STMMs, we compared the perceptions of first-timers and repeat participants. When compared with first-timers, respondents who had participated more than once in STMMs had more sufficient knowledge of local culture (p < .05). The other perceptions—including motivation, expectation, belief, efficiency, and ability of native language—carried no significant differences (data not shown).
Discussion
The current study is the first questionnaire analysis to explore the attitudes, beliefs, motives, and efficiency of health care professionals who venture to underdeveloped areas for short-term assignments of volunteer medical services. We developed a profile of STMMs and identified important characteristics worthy of further attention. In our study, all four groups of health professionals had positive beliefs about such missions. Most health providers on STMMs require interpreters to bridge the language gap. The ability to communicate is essential to international medical initiatives, so problems in this area represent a significant barrier (Hunt, 2011; Suchdev et al., 2007). In addition, most participants lack sufficient acquaintance with local culture, which can be a barrier to administering appropriate medical interventions (Hunt, 2011; Jesus, 2010).
Our study also represents the first survey to compare the views of four key groups of health professionals. While those in all four groups generally agreed upon the key elements for conducting successful STMMs, there were variations among the different specialties. First, physicians were more likely than the other groups to regard STMMs as a means to gain and maintain diplomatic friendships. Health aid to resource-limited countries has been proposed as a useful method to gain their friendship (Kickbusch, 2011). Taiwan has official diplomatic relations with only 23 nations, making this consideration perhaps different than it would be for people in many other countries. In an attempt to help both foster and cement diplomatic ties, the TaiwanICDF was established to represent Taiwan in overseas cooperation projects. Its funding comes from Taiwan’s Ministry of Foreign Affairs. In addition to providing humanitarian aid, the TaiwanICDF aims to promote international relations between Taiwan and its developing partner nations. Providing economic assistance and foreign aid (such as grants, loans, and technical support) to diplomatic allies is part of Taiwan’s foreign policy (Chan, 1997). On the other hand, the deployment of STMMs supported by the TaiwanICDF is based on Taiwan’s strategic interests and is designed to rally international support to break through diplomatic barriers (Tubilewicz & Guilloux, 2011). Therefore, Taiwan’s health aid is not only a humanitarian gesture but also a political consideration.
Second, our study found that assignment to a mission was more common among public health practitioners. This is because they were mostly assigned by the TaiwanICDF to take charge of essential logistic support.
Third, we noticed that pharmacists had relatively deficient language proficiency and cultural awareness. This is probably because pharmacists in Taiwan have fewer opportunities to learn foreign languages and about others culture than those in the other three groups. There has been a marked increase in the number of pharmacists involved in the provision of humanitarian health care services (Bussieres, St-Arnaud, Schunck, Lamarre, & Jouberton, 2000). Their important role in STMMs has been recognized (Johnson et al., 2009). They can provide valuable contributions to patient care because pharmacy services are scarce in underdeveloped nations. To our knowledge, this study is the first to investigate the thoughts of pharmacists toward STMMs.
Although all groups of our participants generally recognized language proficiency and cultural awareness as important for conducting successful STMMs, many members of groups did not rate their own capabilities as sufficient. Development of a language class focusing on medical terminology and local culture might be valuable to the participants (Mulvaney & McBeth, 2009; Suchdev et al., 2007). However, finding qualified teachers and teaching material, especially for the languages of remote tribes, is sometimes impossible outside the local setting. In addition, there is the question of how much language proficiency could practically be obtained in advance, especially for missions that may last only 1 or 2 weeks. Given the high level of satisfaction with the interpreters that were assigned to such missions, language did not appear to pose a substantial obstacle to STMMs that had translators available. Nonetheless, in cases where medical aid workers can speak additional languages, it would be beneficial to match, if possible, their service to destinations where such languages are spoken.
In our study, the desire to contribute to humanitarian aid and the search for new experiences were common motives for volunteers. These findings are in accordance with the results of a previous study (Bjerneld, Lindmark, McSpadden, & Garrett, 2006). In our study, however, more than half of our respondents named “assignment” as a motivation for their participation. The likely cause is that most of our participants were employed by hospitals that collaborate with the TaiwanICDF, with hospital superintendents then assigning participation in STMMs. Nevertheless, we found that most who listed “assignment” as a reason for their participation reported additional motivation as well (data not shown).
There are limitations to this study. First, this is a self-rated survey, not an audit of actual practice. Inaccuracy may occur in a retrospective questionnaire survey due to time elapse. However, there was no other reliable method to collect such data. We think the majority of respondents recalled their missions accurately because such experiences are uncommon and memorable. Second, the response rate was 65.4%; we believe, nevertheless, that the respondents can represent all the participating members because their backgrounds were similar to those of the subjects who did not respond to our postal questionnaire (data not shown). Third, our study found that a small number of participants did not agree with the usefulness of language ability, teamwork, cultural awareness, or follow-up support. We do not know how they weighted these issues in relation to each other or other factors. Fourth, our questions focused mainly on the perceptions of participants in STMMs and did not investigate the outcome of patients. Further studies are needed to evaluate the impact of STMMs on the recipient nations.
In conclusion, we distinguish the thoughts of key health professionals on STMMs. There are considerable differences in perceptions across the four key groups of heath personnel. A majority of participants were motivated by the desire to help others and to become self-fulfilled. Although all the professional groups agreed that language capability and cultural awareness are both important for improving the efficiency of STMMs, the members of these groups, especially pharmacists, lacked sufficient skills in these areas. Our study sheds some light on the perceptions of participants in four professions. We hope this survey provides further impetus for integrating evidence into the deployment of STMMs.
Footnotes
Acknowledgments
The authors are grateful to the participants who gave their time in this study. The authors thank Yu-Chun Tseng and Jun-Han Lee for their assistance in the collection of questionnaires.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Health Research Institutes, Taiwan (grant number PH-100-SP-09).