
Abstract
Growing Up in New Zealand, a longitudinal study following nearly 7,000 children, has faced some unique challenges in identifying, enrolling, and retaining a large and diverse antenatal cohort. Identification of a study region with population demographics that enabled enrollment of an appropriately diverse sample was required as was intensive community and participant engagement in order to promote the study. Complementary methods used included direct engagement with prospective participants and the community and indirect engagement via media. Thus far, retention rates above 95% have been achieved by maintaining a multimethod approach that includes valuing participants and building trusting relationships, strong brand recognition, community engagement, maintenance of participant contact and location records, ensuring high-quality interactions between the participants and the study, pretesting measures and methods prior to the main cohort, and using participant feedback to inform the measures and methods used in future waves of data collection.
Growing Up in New Zealand is a longitudinal study of nearly 7,000 children and their families that began antenatally by enrolling pregnant women and their partners. This study will follow the cohort children, born in 2009 and 2010, in the context of their families and wider environments as they grow to adulthood in the 21st-century New Zealand (Morton et al., 2012). The overall objective of this new longitudinal study is to provide a robust, relevant evidence base to inform policy related to children and their families (Morton et al., 2012).Growing Up in New Zealand was designed to meet this objective and thereby create a valuable resource for the benefit of all New Zealanders, in particular (i) for researchers to gain a better understanding of the causal pathways that lead to particular developmental outcomes, (ii) for policy makers to inform strategies to optimize child health and development, and (iii) for the children and families who take part in this study as well as for all future generations of New Zealanders. In this article, we describe the strategies and processes that were developed to enable recruitment and retention of this cohort.
Study Design and Setting
The aim of Growing Up in New Zealand was to recruit a sample that was broadly generalizable to the current New Zealand births within a contiguous geographical region without resorting to a complex sampling design involving stratification, clustering, or disproportionate selection. Sampling within a discrete region is more time and cost efficient than sampling across multiple study regions (Poulton et al., 2006). It also maximizes the potential for local publicity and allows the development of a strong geographical identity. The first task, then, was to identify a region with the appropriate population diversity to allow the enrollment of a diverse sample.
The Growing Up in New Zealand study region is defined by the geographic boundaries of the areas governed by three adjacent district health boards (DHBs), the bodies that are responsible for health service provision at an area level (Auckland, Counties—Manukau and Waikato). Over 33% of all live births in New Zealand occur within the region defined by these three DHBs (Ministry of Health, 2010).
The demographics of this region provided the opportunity to enroll a diverse cohort without having to use stratification and disproportionate sampling by ethnicity. This is important in the New Zealand context, where one in every four children born in 2009 had more than one ethnicity (Statistics New Zealand, 2011).
The target size of the main cohort was determined by the explicit requirement that the sample had adequate statistical explanatory power for Māori (Morton & Morton Consortium, 2006), the indigenous people of New Zealand and that this explanatory power would remain adequate, given the expected rates of attrition (Morton et al., 2012). Māori experience poorer health, socioeconomic, and educational outcomes in comparison to the overall New Zealand population (Crengle, 2009; Robson, Cormack, & Cram, 2007). Māori are also more likely to experience discrimination (Robson et al., 2007) and are more likely to have a shorter life expectancy (Crengle, 2009). Explanatory power for Māori is thus a key objective for Growing Up in New Zealand in order to meet Treaty of Waitangi responsibilities (the treaty signed in 1840 by representatives of the British Crown and by Māori chiefs) to ensure the study can inform on Māori health and developmental goals and provide evidence to improve equity.
The study region chosen provides socioeconomic diversity that reflects the reality of New Zealand families with young children. In New Zealand, socioeconomic deprivation has been defined for small geographic areas (meshblocks, defined by Statistics New Zealand) using data collected at each national census on variables such as household income, ownership, and amenities, household member employment and education, and household crowding. The New Zealand Socioeconomic Deprivation Index (NZDep2006) provides a deprivation score using a decile index (Salmond, Crampton, & Atkinson, 2007; White, Gunston, Salmond, Atkinson, & Crampton, 2008). The areas comprising the most deprived 10% of households are given a deprivation index of 10, and the areas comprising the least deprived 10% of households are given a deprivation index of 1 (White et al., 2008). The distribution of socioeconomic deprivation in the Growing Up in New Zealand study region reflects the national distribution of household deprivation for all families having children in New Zealand currently (Morton et al., 2012).
Promoting Awareness by Consultation
As part of the study design, and prior to recruitment, Growing Up in New Zealand engaged with members of the DHBs (and the primary health organizations [PHOs] and individual primary care practices administered by each DHB), health professionals, and Māori, community, and cultural stakeholders within the study region. Within New Zealand, individual primary health care practices are part of a PHO. Each DHB in New Zealand administers the funding of their local PHOs. PHOs are responsible for the health care services delivered by the member practices to the population enrolled at each practice (Ministry of Health, 2002). The groups with whom Growing Up in New Zealand consulted, and the consultation methods and objectives are outlined in Table 1.
Summary of Consultations Completed, Consultation Strategies Used, and the Consultation Objectives.
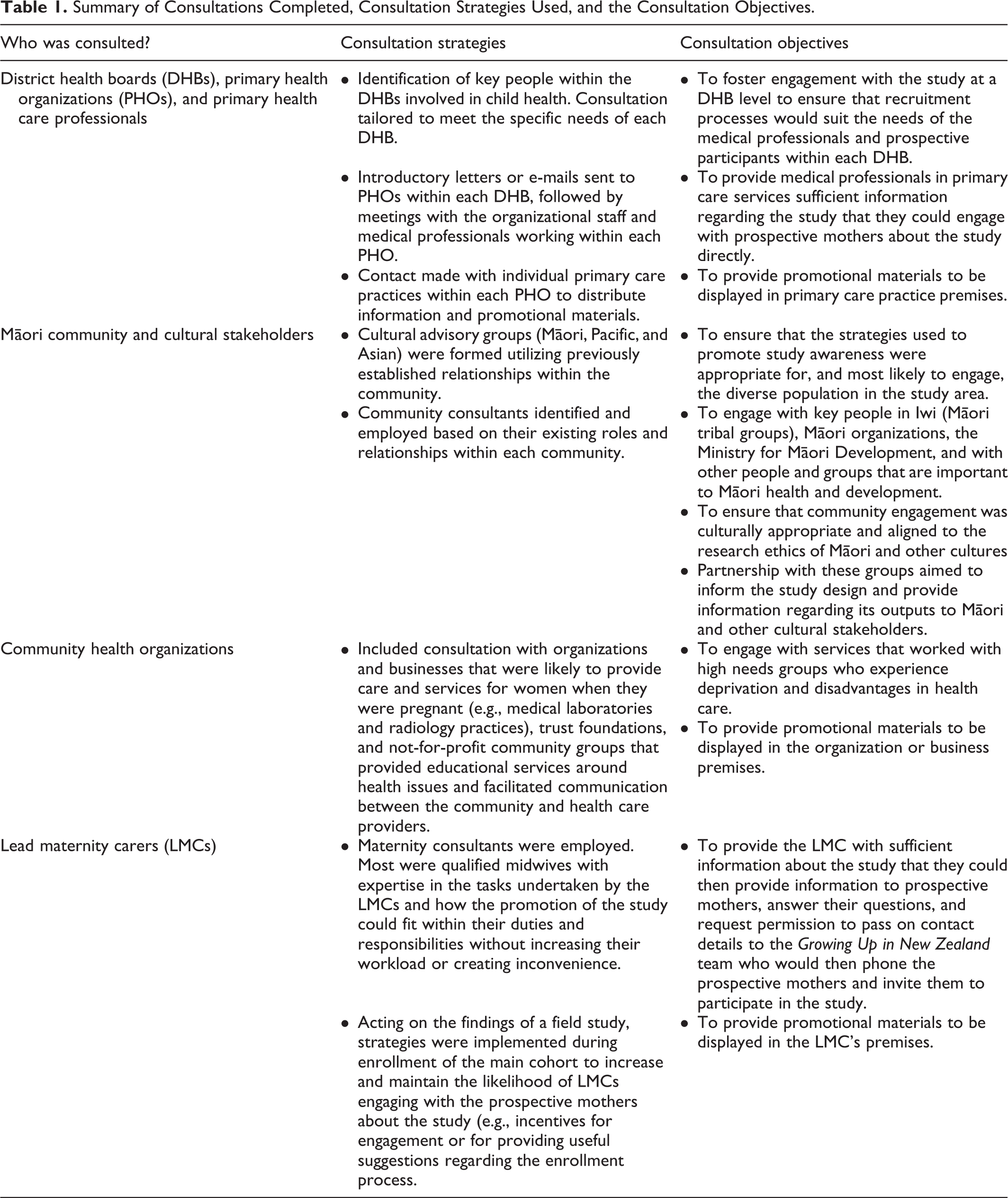
This consultation sought to ensure that the objectives of the study were relevant and the methods used for promoting awareness of the study were appropriate for the areas and the diverse population that would be involved. Consultation began at a national level and, working down through the organizational hierarchies, helped to ensure broad coverage and dissemination of information about the purpose and value of the study to the general population, and to groups within the population for whom the study has the greatest potential benefit. Consultation was tailored to the needs of each group. It generally involved presentations, discussions, and small-group meetings regarding how Growing Up in New Zealand and the stakeholders could work together.
An important part of the consultation process was to establish foundations for long-term relationships with stakeholders. This included making sure that the stakeholder expectations were within what Growing Up in New Zealand was able to provide. Being a longitudinal study, Growing Up in New Zealand required continued support from all of these key stakeholders in order to assist with endorsement and with the retention of participants, to ensure study relevance for stakeholder policy and programs, and for ongoing sustainability. Methods for maintaining these relationships were tailored to the needs of each stakeholder.
Consultation was followed by the implementation of a range of strategies to engage community members and to promote awareness of the study, involving both direct and indirect contact with prospective mothers.
Contacting a Diverse Population to Enable Antenatal Enrollment
The only eligibility criteria for participation in Growing Up in New Zealand was that the mother lived in the study region and had an estimated birth date for the child that fell between April 25, 2009 and March 25, 2010. Most longitudinal birth cohort studies enroll their participants at birth or soon after (e.g., Fergusson, 1998; McLanahan, et al., 2003; Yach et al., 1991). As all births in New Zealand are registered, enrollment at birth reduces difficulties with contacting prospective participants. There is, however, no register of pregnant women in New Zealand, and so an important challenge for Growing Up in New Zealand was how best to promote awareness about the study to a diverse population, so that all eligible pregnant women in the study region had the opportunity to participate.
Contemporary longitudinal studies that have enrolled prospective mothers during the antenatal period have used different sampling strategies, including random sampling via door-to-door contact in neighborhood clusters that match the ethnic and socioeconomic distribution of the population (Sampson, Morenoff, Earls, 1999); consultations with health professionals who then spoke about the study with potential participants (Golding, Pembrey, Jones, & The ALSPAC Study Team, 2001; Jaddoe et al., 2006); approaching women in clinics (Richter, Norris, Pettifor, Yach, & Cameron, 2007) and maternity hospitals (Golding, et al., 2001); and various advertising strategies involving television, radio, newspapers, posters, and other media (Golding, et al., 2001).
Nearly every pregnant woman in New Zealand is eligible for publicly funded primary maternity care from a lead maternity carer (LMC 1 ; Ministry of Health, 2011), and these services are accessed by over 99% of all pregnant women in New Zealand (Health Funding Authority, 2000). Therefore, as outlined in Table 1, consultation with LMCs aimed to utilize their engagement with the prospective mothers as the primary awareness strategy for the study. A field study to test the effectiveness of LMCs as the primary method by which to inform pregnant women of the study showed that although this was a valuable method of raising study awareness, it would not result in the size or diversity of the sample required if it were the sole recruitment strategy (Morton Consortium, 2007). Therefore, while LMCs formed a key component of recruitment, this approach was supplemented with a range of additional strategies. These are outlined in the following section.
Promoting Awareness Through Indirect and Direct Contact With Prospective Participants and the Community
In order to promote awareness of the Growing Up in New Zealand study to the diverse population who live within the study region, indirect promotional methods were employed across a range of advertising media and locations, and presented in the languages most frequently spoken in the study region. The aim of these strategies was to increase awareness of the study with prospective mothers who may have been interested in participating and to increase awareness about the study more broadly. Promoting the study to the general New Zealand public aimed to both increase recognition of the study across the wider community and to help facilitate “word-of-mouth” advertising by promoting the study to other members of the community who may know of prospective mothers potentially interested in enrolling. Growing Up in New Zealand developed a retail team who were present in shopping malls, at community events, and busy locations across the study region. All of the indirect methods involved providing contact details (website address, a free phone number, and a text messaging service) that could be used to access further information or enroll in the study. A description of each of the indirect methods of promotion used is provided in Table 2.
Indirect Methods of Promoting Awareness of the Growing Up in New Zealand Study.
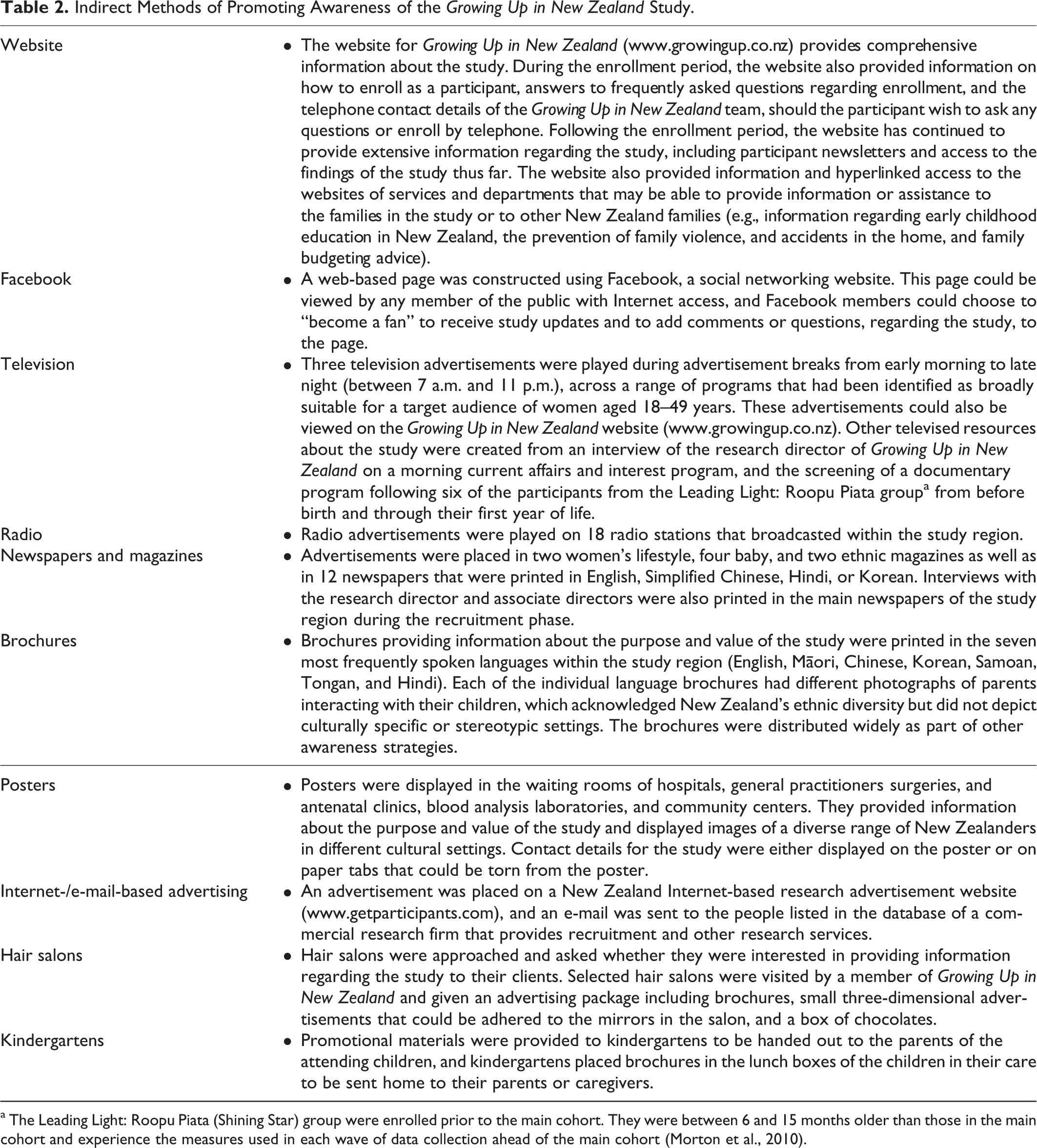
a The Leading Light: Roopu Piata (Shining Star) group were enrolled prior to the main cohort. They were between 6 and 15 months older than those in the main cohort and experience the measures used in each wave of data collection ahead of the main cohort (Morton et al., 2010).
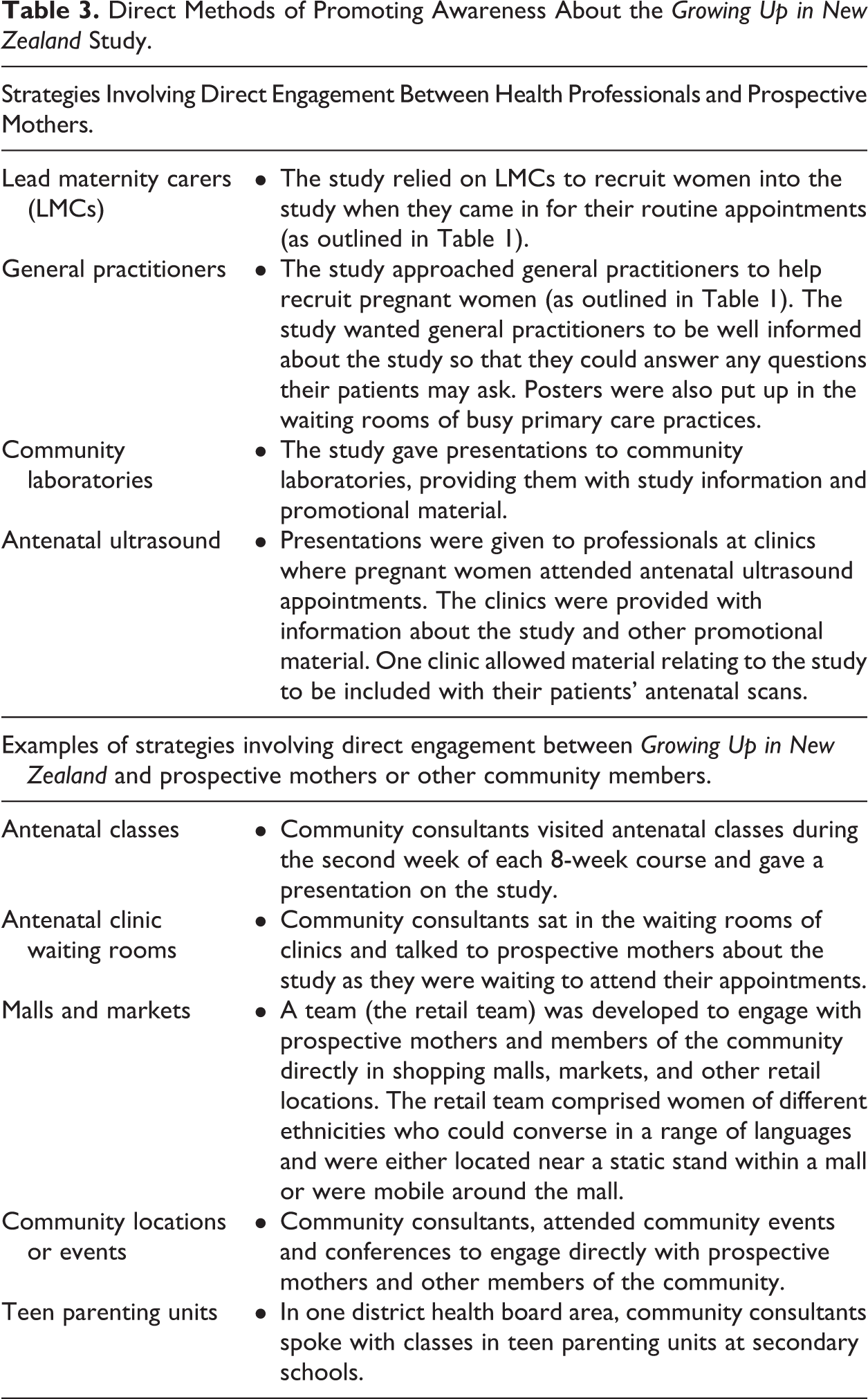
Strategies were also developed to allow the Growing Up in New Zealand team to engage with prospective mothers, and other members of the community more directly than could be achieved by the methods outlined in Table 2. Two main approaches were developed: direct engagement by a member of the Growing Up in New Zealand team with prospective mothers and other members of the community in community locations and health settings; and direct engagement by a member of the Growing Up in New Zealand team with health professionals who were in direct contact with prospective mothers. These health professionals then provided information about the study to their clients and were able to answer any questions they may have. An important component of this strategy was that the person who engaged directly with a prospective mother asked for permission to forward their contact details to Growing Up in New Zealand. This was followed by a phone call to the prospective mother from the study team within a few days to provide answers to any questions that the prospective mother may have or to enroll the prospective mother in the study. A description of some of the key methods of direct engagement is provided in Table 3. The telephone recruitment team included people who were multilingual.
Direct Methods of Promoting Awareness About the Growing Up in New Zealand Study.
The Success of These Methods in Contacting a Diverse Population
In total, Growing Up in New Zealand received 10,324 referrals 2 (information regarding the source of the referral was missing for two referrals). Direct engagement with an LMC resulted in the greatest number of referrals (4,273 [41%]), and subsequent enrollments (2,645 [39%]) of any method of direct or indirect engagement. Of the remaining strategies, direct engagement with prospective participants in shopping malls, at community events, and in other community locations resulted in the second largest number of referrals (4,010 [39%]) and subsequent enrollments (2,361 [35%]). For both the LMC and direct engagement methods, a “consent to call” strategy was used. Many prospective participants found it more convenient to provide their contact details to consultants and be contacted by the Growing Up in New Zealand team rather than contact Growing Up in New Zealand directly. The retail team and community consultants worked together when promoting the study at community events. This combined the regional expertise of the community consultant with the promotional expertise of the retail team.
All remaining referrals were received via the free phone number, the web-based referral form, or by short message service (SMS). These referrals were deemed self-referrals as the prospective participants contacted Growing Up in New Zealand following exposure to information about the study from another source. Self-referrals also included those that were the result of direct engagement with a Growing Up in New Zealand team member, health professional, community consultant, or member of the retail team but where the consent to call strategy was not used or given (e.g., antenatal classes and clinics and community laboratories). A small percentage of self-referrals (10%) involved a person contacting Growing Up in New Zealand by web, phone, or SMS on behalf of someone else.
Referrals received via the web, phone, or SMS methods accounted for 2,039 (20%) of total referrals and 1,815 (27%) of subsequent enrollments. Of these, the web-based approach resulted in the most referrals, with 1,299 (64%) of 2,039 referrals (resulting in 1,202 [66%] of 1,815 subsequent enrollments). In comparison, the free phone number received 479 (23%) referrals (resulting in 427 [24%] subsequent enrollments), and the SMS number received 261 (13%) referrals (186 [10%] subsequent enrollments).
When contacting Growing Up in New Zealand, prospective participants were asked to provide information about where they had heard about the study. This information was only available for the 2,039 (20%) prospective participants who self-referred directly to Growing Up in New Zealand. Posters and other media placed in specific locations included codes that could be quoted by prospective participants when they contacted Growing Up in New Zealand. When the participants quoted these codes, the specific location and medium of the referral source could be recorded.
The sources reported by each of the people who contacted Growing Up in New Zealand via the web, free phone, or SMS and other opportunities are shown in Figure 1. Television was the most commonly cited information source followed closely by LMCs and information provided at maternity clinics where the consent to call strategy was not used. Friends and family provided the third greatest source of web, free phone, and SMS referrals (and subsequent enrollments), demonstrating the success of promoting awareness to the wider community, followed closely by other health clinics which included diagnostic laboratories and radiology clinics. Smaller numbers of referrals (and subsequent enrollments) were achieved through other sites and forms of promotion. It should be noted that a small number of referrals also reported engagement with the retail team (in shopping malls or other community locations).
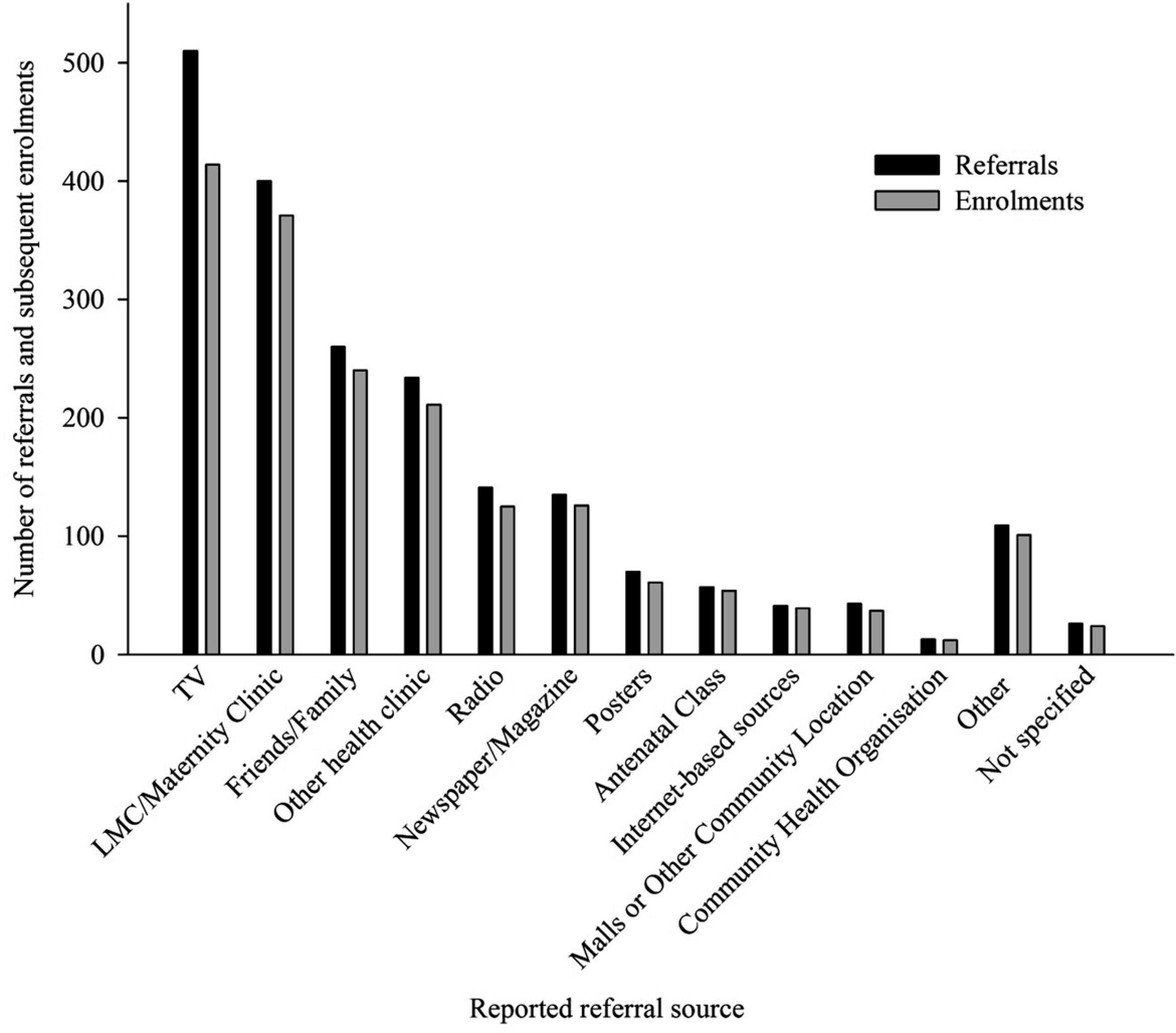
Participant reported referral source, received through the website, free phone, and SMS (N = 2,039). LMC = lead maternity carer; SMS = short message service.
It was not possible to track exposure to study information exactly to determine the single most effective form of promotion. The breadth of strategies used to promote awareness of the study meant that many prospective participants were exposed to information about the study from more than one source. This became apparent during direct engagement with prospective mothers as, in December 2009 toward the end of the recruitment phase, 84% of women who were eligible to enroll in the study and were engaged with directly by a Growing Up in New Zealand team member within a shopping mall or at another community location had heard of the study from another source. Also, the majority of women who were engaged with directly during the antenatal classes had enrolled in the study already.
Monitoring of feedback from the participants and the reported frequency that individual referral codes were cited allowed for flexibility and adaption of strategies to best meet the needs of the project and the diversity of the enrolled cohort. For example, the use of hair salons and kindergartens to help promote the study was quickly shown to be ineffective, with only two referrals citing the hairdressers and no referrals citing the kindergartens as where they had heard about Growing Up in New Zealand. The identification of these strategies as ineffective allowed time and resources to be concentrated on other, more successful, strategies.
Response Rates
Overall, 89% of referrals made by web, phone, or SMS resulted in a participant enrolling in the study. This was greater than the response rates (with total referrals as the denominator) achieved through the consent to contact strategy used by the LMCs (62%) or the community consultants and retail teams (59%). The greater response rate of the web, phone, and SMS methods is not surprising as the additional effort required to self-refer is likely to be an indicator of interest in subsequent enrollment. However, the absolute numbers of referrals and enrollments achieved through the web, phone, and SMS contacts are much lower than those resulting from the LMCs, community consultants, and retail teams. Therefore, while the web, phone, and SMS contacts were a valuable strategy for allowing prospective participants to contact the study, direct engagement was responsible for enrollment of most of the cohort.
The Growing Up in New Zealand Cohort
Antenatal interviews were completed by 6,822 women (66% of all referrals; Morton et al., 2012). This resulted in a cohort size, including multiple births, of 6,846 children (Morton et al., 2012). Consent to participate was also obtained from 4,401 of the mothers’ partners, with 99% describing themselves as the biological father of the child (Morton et al., 2010). Overall, the enrolled cohort is broadly generalizable to current births in New Zealand (Morton et al., 2010). The cohort includes sufficient numbers of each main ethnic group in New Zealand to ensure that findings can be used to inform practices and policies to optimize outcomes for all New Zealand children (Morton et al., 2012). A detailed profile of the main cohort for Growing Up in New Zealand cohort was published in 2012 (Morton et al., 2012).
In addition to the main cohort, a group of approximately 200 families were enrolled in the Leading Light: Roopu Piata (Shining Star) group (Morton et al., 2010). The children in these families are between 6 and 15 months older than those in the main cohort (Morton et al., 2010) and experience the measures used in each wave of data collection ahead of the main cohort (Morton et al., 2010). Their valuable feedback guides revisions or alterations to the measures or methods used in the study prior to its implementation with the main cohort. Some of these families also volunteered to be involved in media campaigns and formed the basis of a documentary about the study that was screened on New Zealand television.
At the time of writing (June 2012), face-to-face interviews have been conducted with the mothers and partners during the antenatal period, and when the children were approximately 9 months old. Further face-to-face interviews with the main cohort when the children are 2 years old are nearing completion at the time of writing. Telephone-based interviews were conducted when the children were aged approximately 6 weeks, 35 weeks, 16 months, and 23 months; and phone-based interviews when the children were aged 31 months were in progress at the time of writing. A list of the study objectives, research questions, and constructs measured are provided in the cohort profile publication (Morton et al., 2012). Linkage has been completed with perinatal data and is in progress with other electronically stored data which describes health care utilization by the cohort during the first year of life (Morton et al., 2012).
Retention Rate and Strategies
Beyond enrollment, one of the greatest challenges of any longitudinal study is the retention of the cohort over time. Minimizing attrition, and the bias in it, is particularly important when the sample is diverse. Some participants are more likely to be lost from the study than others (Ribisl et al., 1996), resulting in a sample that becomes increasingly biased, thus compromising both the internal and external validity of the study (Ribisl et al., 1996). Therefore, strategies to optimize retention rates must be an essential feature of the study design (Given, Keilman, Collins, & Given, 1990) and implemented from the beginning of the study (Ribisl et al., 1996). Growing Up in New Zealand has implemented multiple strategies that aimed to maximize retention across the study. The retention rate of Growing Up in New Zealand at the 9-month interview was 95% (Morton et al., 2012). Those participants who skipped the 9-month interview have been given the option to reengage with the study at a later time (Morton et al., 2012).
Tracking
The greatest source of attrition is failure to locate participants at the next scheduled follow-up (Ribisl et al., 1996). Therefore, tracking the contact details of the participants in the study is important to minimize attrition that could be otherwise avoided. Growing Up in New Zealand maintains a database of the address and contact details of the participants at the time of each contact. Participants are also asked to provide the details of alternative contacts, usually of family and friends, which can be used to help locate the participant. If neither the participant’s contact details nor the alternative contacts result in connecting with the participant, a Growing Up in New Zealand team member may visit the participant’s house. Face-to-face contact such as this has been shown to be more effective in retaining participants than contact in writing or by phone (Sullivan, Rumptz, Campbell, Eby, & Davidson, 1996).
Interviews
The people with whom the participants are most frequently in contact are the study interviewers. As such, the conduct of the interviewers and the rapport that they build with the participants are the most important factors in ensuring the continued engagement of the participants with the study (Sullivan et al., 1996). This makes effective interviewer selection and training imperative (Ribisl et al., 1996). In addition to their interviewing skills and experience, Growing Up in New Zealand interviewers were selected based upon their potential ability to develop a rapport with the participants and to make their interviews enjoyable, professional, and nonjudgemental. The interviewers received comprehensive training, including how to conduct the interviews (both the in-person and telephone-based interviews are computer aided); familiarity with the content of the interview; briefing notes regarding the purpose of the items in the questionnaires; information regarding culturally appropriate behavior; and the overall importance of punctuality and professional conduct.
A choice was offered to match interviewers with participants based on ethnicity, language, and availability (preferred time and location). Most interviews were conducted in English, and interpreters, including those fluent in New Zealand Sign Language, were provided where they would best meet the needs of the participants. Where an interviewer was fluent in a language other than English, attempts were made to match them with participants who would have otherwise required an interpreter. Attention was also paid to the suitability of interviewers for the questions being asked. For instance, during antenatal interviews, only female interviewers were employed to interview the pregnant women (some of the male partners spoke with male interviewers).
Flexibility of scheduling, to minimize inconvenience to the participants, is also important (Marmor, et al., 1991). Growing Up in New Zealand attempts to schedule interviews for those times that best suit the participants, including the evenings and weekends. Further, all in-person interviews are conducted at the participant’s home or at a place of the participant’s choice. This reduces the likelihood of attrition due to difficulties that participants may have with travelling to an interview. Telephone-based interviews begin with an enquiry as to whether this is a suitable time. The interview is rescheduled if necessary.
Satisfaction With the Study and Continued Engagement
Attrition may also result from dissatisfaction with the study or its methods. Therefore, it is important to minimize the likelihood of this occurring by implementing strategies to ensure the participants’ continued satisfaction with their involvement in the study. Growing Up in New Zealand has implemented multiple strategies to ensure ongoing quality checks regarding the experience of participants in the study.
Data from the Growing Up in New Zealand leading light
Roopu Piata participants provide information about the questionnaires and methods prior to their implementation with the main cohort. The interviewers themselves are also key informants regarding the utility of the questionnaires.
When participants have queries or concerns about the measures being used, these are addressed in the first instance by the interviewers. If a participant requires further information beyond that which the interviewer can provide, their query is referred to a member of the research team. The participant is then contacted by a Growing Up in New Zealand team member and further information regarding their query is provided.
Auditing is essential
Growing Up in New Zealand has developed an auditing process for its in-person interviews. The antenatal interviews were managed by an external research company. This company conducted an audit of 40% of all interviews conducted. Feedback cards (postcards) were sent by mail to 30% of the participants interviewed by each interviewer, and an additional 10% of the audits were conducted via telephone.
Independently of the contracted research company, Growing Up in New Zealand conducted a telephone audit of 5% of the antenatal interviews. For the 9-month and 2-year interviews, all auditing, both by post (5% of all interviews) and via telephone (30% of all interviews), are conducted by Growing Up in New Zealand. All auditing methods have involved presenting the participants with a series of questions regarding their experience of the interview, both content and delivery. The participants are also provided with the opportunity to communicate any further feedback they wished to provide. Where this feedback involved a specific question, the participant was later contacted by a Growing Up in New Zealand team member who addressed their query. Feedback regarding the interview delivery was given to the interviewers, with any information that might identify the participant removed. Any concerns that were raised regarding the content or delivery of the interview were referred to, and addressed by, the research or interview teams. Overall, the feedback received about the interviews and the interviewers has been very positive.
Strategies to help the continued engagement of the participants have also been implemented. Regular contact with the participants is important (Sullivan et al., 1996). It has been suggested that participants should be contacted at least every 6–12 months to maintain accurate contact details (Hunt & White, 1998). By the time that the children in Growing Up in New Zealand are 2 years of age, their families will have been in contact with the study on seven occasions, three of which are face-to-face interviews at their home. The remainder of these contacts are telephone interviews that also schedule the in-person interviews and check contact details. In addition to this, participants are sent a newsletter every 3 months, which provides updates on the study, a message from the study director, and other items of interest including articles featuring some of the Leading Light: Roopu Piata families who have volunteered to take part in media activities. A section of the website dedicated to the participants has also been developed. This provides access to resources, including answers to frequently asked questions, an outline of the initial findings, information regarding privacy and confidentiality, and electronic copies of the participant newsletters.
Cost constraints and ethical considerations have prevented us from being able to reimburse participants directly for their time. In order to thank them and acknowledge their importance to the project, participants are given small gift bags at the end of each interview, containing goods which have been mostly provided through sponsorship by local companies (e.g., food samples, books, small toys, toiletries, and discount vouchers for New Zealand businesses).
Summary and Conclusion
Growing Up in New Zealand faced a number of challenges in recruiting a suitably diverse population in the antenatal period, with sufficient numbers to be able to provide adequate statistical explanatory power for Māori and other key subgroups within the sample. The aim then was to implement strategies to promote the study that would allow all eligible women the opportunity to enroll in the study, and hence the study to be broadly generalizable to the current population of births. This was achieved first by choice of geographical area and then by a comprehensive range of strategies that included early and continued engagement with health, community, Māori, and cultural organizations; direct engagement with prospective mothers and other members of the community through LMCs, and retail and community consultants in community locations; and indirect engagement with prospective mothers and the wider community through a variety of advertising media.
LMCs provided the greatest contact with prospective mothers. Direct engagement with community and retail teams in shopping malls, at community events, and in other community locations also proved to be a valuable strategy. The value of promoting the study to the wider community and the importance of using a broad range of indirect engagement methods were demonstrated by the large proportion of women who had heard of the study from another source when engaged with directly by the retail team or a community consultant, and the number of women who cited their referral source as “family and friends” when contacting the study through the web, free phone, or SMS services.
Growing Up in New Zealand now faces the challenge of retaining such a diverse sample over the longitudinal course of the study. The 9-month interview was completed by 95% of the cohort, with further families having the option to return to the study at a later date. With the next face-to-face interviews currently underway targeted methods have been developed to ensure that those who skipped the 9-month interview are encouraged to maintain engagement with the study. Retention thus far has been aided by the use of a number of strategies to ensure: the continued public recognition of Growing Up in New Zealand; accurate tracking of the location of the participants (including those who have moved within New Zealand or overseas); alignment of the study processes with Māori; and community needs and most importantly, the continued positive experience of the participant families who make up Growing Up in New Zealand. Valuable feedback provided by the Leading Light: Roopu Piata group helps to ensure that the measures and methods implemented with the main cohort are acceptable to the participants, scientifically robust, and allow the findings to inform future policy and improve outcomes for New Zealand children. Feedback from the main cohort has also been instrumental in refining the measures and methods used in the future collection of data. Finally, key to the continued positive experience of the participants is their interactions with the interviewers. Thus, identifying and employing interviewers for their abilities to engage with the participants, and comprehensive training to ensure accurate and efficient data collection, are imperative to the success of the study. Valuing participants and building relationships based upon trust will remain central to the continued success of Growing Up in New Zealand.
Footnotes
Acknowledgments
The authors would like to acknowledge the following people for their roles in the recruitment process for Growing Up in New Zealand: Adrienne Bell, Diana Benfell, Donna Bernasconi-White, Wayne Borell, Bob Bulpin, Lisa Corkill, Bernadette Corner, Monique Davies, Caroline Everard, Florence Falconer, Carol Hedgman, Kim Heathcote, Linda Hefford, Leone Inu, Raymond (Moko) Kumar, Jessica Lawton, Tania Milne, Sheralee Patea, Avril Robinson-Payne, Libby Rodrigues, Mele Siakumi Kautoke, Peter Tricker, Juliette Wotton, and the Mall Recruitment Team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The University of Auckland; the Ministry of Social Development; the Ministry of Health; the Ministry of Research, Science, and Technology; the Health Research Council of New Zealand; the Ministry of Justice; the Families Commission; the Children’s Commission; the Department of Labour; the Ministry of Education; Housing New Zealand; and Sport and Recreation New Zealand.