
Abstract
The aim of this study was to translate and validate the Alzheimer’s Disease Knowledge scale (ADKS) in a population of Greek general practitioners (GPs). The international standards for the forward and back translation approach were followed. For the validation step, 112 GPs, treating dementia in their daily practices, were enrolled from Crete. The questionnaire was assessed for the following psychometric properties: intraclass reliability, test–retest reliability, and construct and face validity. Internal consistency of the Greek ADKS was satisfactory (α = .65). A high repeatability of the instrument was found during the retest with 27 GPs (intraclass correlation coefficient = 1.0). Factor analysis showed that all the items from the original instrument can be used in the Greek version. The inter-item correlation revealed a high cross-correlation between the items of the questionnaire (α > .6). The data confirmed the validity of the Greek version of the ADKS for measuring GPs’ knowledge on the diagnosis and management of dementia.
Introduction
Dementia has become a major public health care problem with an impact on millions of patients and their families. As the prevalence of dementia is increasing dramatically due to the growth of the aging population (Ferri, Sousa, Albanese, Ribeiro, & Honyashiki, 2009) and as the scientific knowledge of Alzheimer’s disease (AD) grows rapidly, general practitioners (GPs) are required to keep their knowledge up-to-date to respond effectively to the problem. This is especially important for the GPs who serve as the first line of health care professionals to whom patients and their families present to for help. GPs should be thus adequately trained in the recognition and management of dementia to provide the best quality of care to their patients (Downs & Bowers, 2008; Dungen et al., 2012; Tsolaki et al., 2010; Tsolaki, Paraskevi, Degleris, & Karamavrou, 2009).
Several tools have been developed for assessing GPs’ knowledge of AD, but only three of them were found in the literature to be validated: the Alzheimer’s Disease Knowledge test (Dieckmann, Zarit, Zarit, & Gatz, 1988), the University of Alabama at Birmingham AD Knowledge test (Barrett, Haley, Harrell, & Powers, 1997), and the Alzheimer’s Disease Knowledge scale (ADKS; Carpenter, Balsis, Otilingam, Hanson, & Gatz, 2009). Among these tools, the ADKS is the most comprehensive; it captures more content areas and takes less than 10 min to complete. A further advantage of the ADKS is that it is the most recent tool and thus better reflects the current understanding of AD (Carpenter et al., 2009).
The aim of this study was to deliver a validated translation of the ADKS in the Greek language to serve the evaluation process of an educational intervention planned to be carried out within the Greek primary health care setting for Greek GPs.
Method
Study Sample
In April and May 2010, the questionnaire was delivered to 112 randomly selected GPs practicing on the island of Crete in both the private and the public sector. The sample is considered highly representative, since it includes two thirds (74.6%) of the number of GPs listed in the Prefecture of Crete. The criteria for the participants’ selection were (a) to be GPs, (b) to treat patients with dementia in everyday clinical practice, and (c) to speak Greek fluently or have Greek as their primary language. All participants provided written consent.
Questionnaire
The study participants were invited to complete the ADKS and a supplement on demographics, self-perceived knowledge about AD, and information on ease of completion. The ADKS questionnaire contains 30 true/false items that cover risk factors, course and epidemiology, assessment and diagnosis, symptoms, life impact, caregiving, treatment and management. In the development study, the ADKS was determined to have good psychometric properties (Carpenter et al., 2009). The questionnaire was self-administered and completed by the participants during face-to-face contacts at their practice. The time of the questionnaire’s completion was approximately 8–10 min.
Translation
The translation procedure was based on minimal criteria developed by the Scientific Advisory Committee of the Medical Outcomes Trust (Medical Outcomes Trust, 1997). A forward and back translation approach was followed, where two independent bilingual health care professionals translated the ADKS items into Greek. The reconciled Greek version was then back-translated by a native English speaker, not familiar with the original questionnaire. This back translation was sent to the developer of the original questionnaire for comments and suggestions, which were incorporated, to produce the revised Greek version of the ADKS.
A cognitive debriefing process was also followed for the cultural adaptation of the questionnaire. The reconciled Greek version was administered to eight GPs serving primary health care centers of Crete.
Reliability
Internal consistency was determined using Cronbach’s α (De Vellis, 1991; Nunnally,1978).Test–retest reliability (reproducibility) was assessed within a 4- to 6-week interval (Deyo, Diehr, & Patrick, 1991). A total of 27 GPs were randomly selected to complete the ADKS for a second time. For the second completion, the questions were presented in a different order to avoid any influence from participants memorizing the order of the answers (Deyo et al., 1991). Intraclass correlation coefficient (ICC) was used to calculate the test–retest reliability.
Validity
Construct validity was evaluated by comparing ADKS scores across respondents’ characteristics, such as age, clinical experience, participation in support groups, attendance of educational programs on AD, and sources of information about AD. Exploratory factor analysis was conducted to extract potential underlying dimensions of the ADKS (Bowling, 2002). The Kaiser–Meyer–Olkin (KMO) test was used to determine the appropriateness of the data set for factor analysis (χ2 = 659.9, df = 435, p < .001; Kline, 1996; Malhotra, 1996). Principal component analysis with Varimax rotation method was used. A factor was considered important if its eigenvalues exceeded 1.0.
Results
Translation
The developer of the ADKS (Brian Carpenter) made only structural comments on six back-translated questions after reviewing the report on the forward and back translation. These comments were taken into account in the final Greek version of the ADKS. The pretest of the questionnaire with the eight GPs serving the Greek public health care system did not render any changes to the study questionnaire. All GPs had a good understanding of the questionnaire and had no suggestions for improvements. Two of the eight GPs that participated in the face validity process reported problems with the comprehension of the instrument. These problems were mostly associated with terms used with different meaning in the Greek context. Their comments were incorporated into the final Greek ADKS instrument.
Participants’ Characteristics
Detailed information on the participants’ sociodemographic characteristics is presented in Table 1. Most of the GPs were men; one fifth of them had a family member with AD, but very few of them were acting as caregivers for an AD patient. The mean age of the GPs was 42.56 (standard deviation [SD] 6.2) and the mean clinical experience was 12.21 (2–30) years.
Participants’ Characteristics (N = 112).
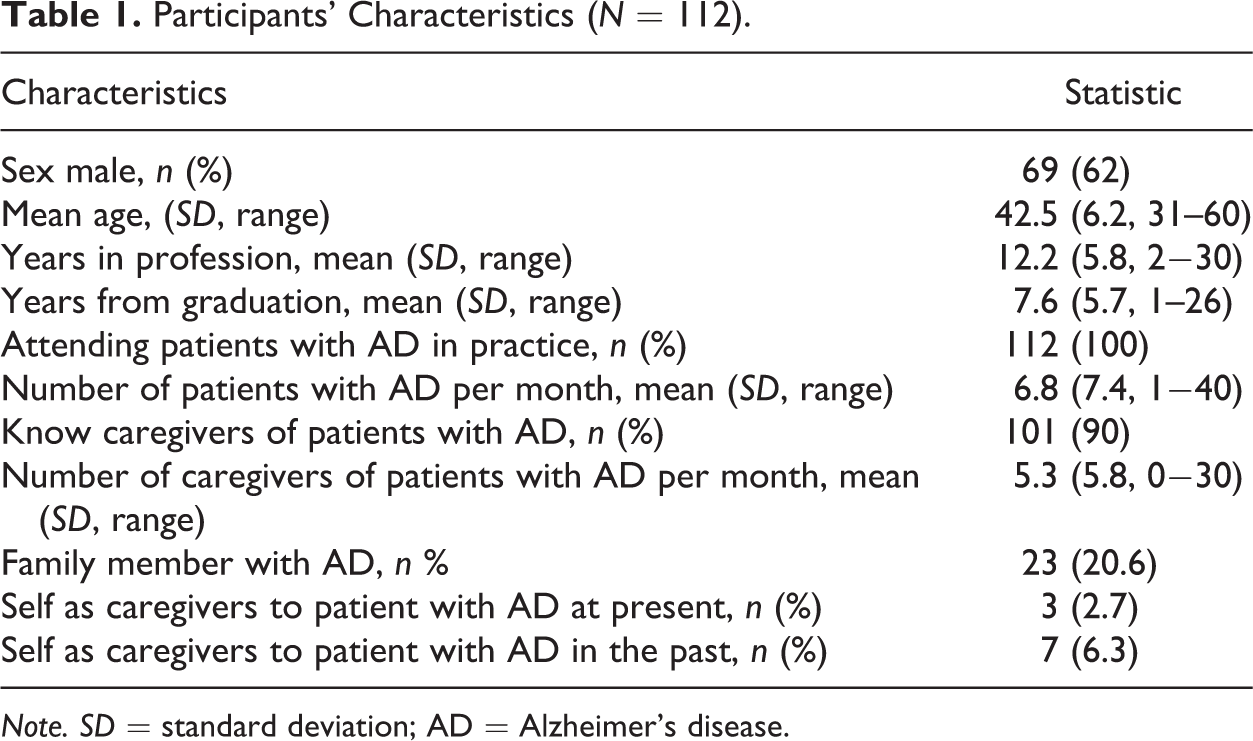
Note. SD = standard deviation; AD = Alzheimer’s disease.
Reliability
The Cronbach’s α for internal consistency was .65. The ICC for the test–retest was 1.0. The mean ADKS score was 22.3 (SD 2.45) for both applications.
Validity
The results of the bivariate analysis revealed that GPs with less clinical experience (p = .038), less years since graduation (p = .015), and those with higher attendance at educational programs for AD (p = .044) tended to have higher ADKS scores. In addition, those who reported using web-based and academic sources of information about AD as well as those not using family as a source of information about AD had higher ADKS scores compared to those who did not use these sources of information (p = .026, p = .057, and p = .010, respectively).
Exploratory factor analysis revealed 12 factors with an eigenvalue > 1 and the model was rejected. More models with 5–9 factors were tested, but no adequate model was identified and item content suggested no meaningful factor interpretation. Cronbach’s α coefficient did not exceed the minimum acceptable limit of .6. Consequently, the ADKS was found to function better as a summed-items questionnaire of overall AD knowledge, and not as separately scored subscales, which is consistent with the developer’s guideline (Carpenter et al., 2009).
Performance on the ADKS
The percentage of participants’ correct answers on the ADKS revealed that 8/30 questions of the ADKS received correct answers by almost all the participants (>90%; Questions 5, 11, 14, 17, 20, 21, 29, 30). These questions measured the course of the disease (two questions), assessment and diagnosis (two questions), caregiving of AD patients (one question), life impact (one question), symptoms of the disease (one question), and treatment and management of the disease (one question). On the other hand, some items had very low number of correct answers (<30%; Questions 2, 6, 13, 16). These questions measured risk factors (two questions) and caregiving (two questions).
Discussion
Main Findings
The purpose of this study was to translate the ADKS in the Greek language and validate the tool in a sample of Greek GPs. The data confirm the reliability and validity of the Greek version of the ADKS for measuring GPs’ knowledge of the diagnosis and management of dementia. More precisely, internal consistency was adequate for a scale that is new in research (Nunnally, 1978). Test–retest reliability was high in both applications distributed 4–6 weeks apart, which is considered an adequate time period between applications, in addition to the change in the order of questions. Furthermore, the findings on the sources of information on AD seem to be in line with other studies (Carpenter, Zoller, Balsis, Otilingam, & Gatz, 2011; De Vellis, 1991). These studies have demonstrated that those who use scientific sources instead of popular media (TV, radio) have a better knowledge of AD, which partly reflects our findings showing higher ADKS scores for those receiving information from Internet sources and those participating in educational programs for AD and related disorders. Although our results showed a difference of marginal statistical significance between GPs who received information from academic sources and those who did not, this finding could guide future research with a larger sample and in different European settings.
Testing of construct validity showed good inter-item correlation. The subscales that were revealed through factor analysis did not result in a meaningful interpretation and implying that the ADKS should be used as a summed-item questionnaire that may reflect several dimensions, as in the original version.
Implications for Practice
The use of the translated ADKS is expected to contribute positively to the collection of necessary information to develop educational programs on AD in accordance with GPs’ needs and to assist in forwarding an integrated care system for patients in Crete and throughout Greece.
The current study provides direction about the design of future educational interventions based on individual characteristics and ADKS scores. In particular, the results revealed that GPs with more years of clinical experience tended to have more knowledge deficits and could benefit from educational programs.
The separate items of the scale pinpoint areas on GPs’ knowledge that need improvement and should be included in an educational curriculum, such as the knowledge about the genetics of AD as well as the nonpharmacologic treatment and the knowledge about prevention. The risk factors of AD and caregiving of AD patients are among the areas of knowledge that also need to be addressed through educational interventions based on our outcomes.
Limitations
First, the true/false design of the tool, contributing to a low variance between questions (Carpenter et al., 2009) may have limited the internal consistency of the Greek ADKS to a minimally acceptable level. Second, the population consisted of relatively young physicians, as general practice in Greece is a rather new specialty of medical practice. This may have impacted the results because younger GPs tend to perform better in terms of dementia diagnosis and disease management. Third, the sample was drawn from one region of Greece and this limits the generalizability of the study findings. Fourth, the ADKS is not an exhaustive assessment tool and therefore some areas of interest might not have been captured but it is adequate for capturing general knowledge about AD (Carpenter et al., 2009). Fifth, ceiling effects may have emerged in groups of physicians with more expertise in the disease, as in the original ADKS.
Conclusion
The data confirm the reliability and validity of the Greek version of the ADKS for measuring GPs’ knowledge on the diagnosis and management of dementia. Due to its short length and good psychometric properties, the ADKS may be a helpful needs assessment tool for those planning dementia education for health care providers in Greece.
Footnotes
Acknowledgments
The authors would like to thank the author of the original paper Dr. Carpenter for his contribution and his continuing interest in this study. The authors would like to express our appreciation to Dr. Paterakis Emmanouil for his contribution to the data collection and to all general practitioners who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.