
Abstract
The purpose of this study was to determine the measurement properties of the Low Back Activity Confidence Scale (LoBACS) in individuals with post-acute low back pain (LBP) receiving nonsurgical intervention, including construct validity, factorial validity, and internal consistency reliability. Data were analyzed from an existing randomized clinical trial involving 112 patients with LBP. Evidence for convergent validity was observed through significant correlations between LoBACS subscale scores and other function, pain, and psychobehavioral measures. LoBACS subscales accounted for 36% of the unique variance in dependent variable measurements, suggesting a satisfactory level of statistical divergence between the LoBACS and other psychobehavioral measurements in this study. Cronbach’s α ranged from .88 to .92 for LoBACS subscales, and item-total correlations exceeded .6, indicating high internal consistency reliability. Principal axis factoring confirmed the hypothesized three-subscale structure by correctly classifying 14 of the 15 items. These findings indicate the LoBACS is valid and internally consistent to measure domain-specific self-efficacy beliefs.
Introduction
Low back pain (LBP) is among the most common and costly forms of disablement to society by way of substantial economic loss (Frymoyer & Cats-Baril, 1991), psychological and interpersonal disruption (Fritz, George, & Delitto, 2001), and emotional distress (Brox, Storheim, Holm, Friis, & Reikeras, 2005; Grotle et al., 2005). These deleterious effects of LBP on the individual suggest that an important relationship between psychobehavioral responses and disability may exist in individuals with LBP. In their systematic review, Chou and Shekelle (2010) identified the presence of maladaptive pain coping behaviors as an important predictor of worse outcomes at 1 year following onset of LBP (Rundell & Davenport, 2010). More specifically, researchers have applied Bandura’s self-efficacy (SE) construct (Bandura, 1989; Bandura, Adams, & Beyer, 1977) to explore the relationship between psychobehavioral responses to symptoms and clinical outcomes in individuals with LBP. Bandura (1977) broadly describes efficacy expectations as an individual’s task- and situation-specific estimate of personal mastery. SE beliefs can determine the presence (Bandura, 1977, 1989, 1997) or absence (Bandura, 1989) of behaviors, such as the ability to cope with LBP (Costa Lda et al, 2011; Denison, Asenlof, & Lindberg, 2004; Iles, Davidson, & Taylor, 2008; Jensen, Turner, & Romano, 1991; Lackner & Carosella, 1999; Lackner et al, 1996; Turner, Ersek, & Kemp, 2005; Turner, Holtzman, & Mancl, 2007). These observations have led some authors to suggest an intermediate role for SE in the relationship between fear and disability (Denison et al., 2004; Woby, Urmston, & Watson, 2007). This raises the importance of clinical measurements for SE in people with LBP, in order to predict those who may be at risk for prolonged disablement and associated costs.
Recently, the Low Back Activity Confidence Scale (LoBACS) was constructed to assess SE for behaviors that are commonly expected to affect function and optimal rehabilitation from LBP. The chief purpose of the LoBACS is to evaluate the magnitude of condition-specific SE beliefs in individuals with LBP (Yamada, Lewthwaite, Popovich, Beneck, & Kulig, 2011). A validation study that was conducted in a cohort of individuals with LBP receiving rehabilitation following single-level microdiscectomy indicated acceptable to excellent test–retest reliability and internal consistency of the LoBACS total and subscale scores (Yamada et al., 2011). LoBACS subscales also demonstrated concurrent validity with respect to measures of physical performance, physical activity, pain, fear beliefs, disability, and quality of life (Yamada et al., 2011). Findings from this study suggest the LoBACS demonstrates adequate measurement properties for an evaluative function in this population. However, the sample consisted mainly of individuals with long-standing LBP and whose clinical picture was severe enough to necessitate surgical intervention. This sample did not include individuals seeking nonsurgical treatment for LBP. Indeed, the validity and internal consistency reliability of LoBACS subscale scores remains unclear for individuals with post-acute LBP who receive nonsurgical intervention. The purpose of this study was to determine the convergent, divergent, and factorial validity of LoBACS subscale scores in individuals receiving solely physical therapy to address a post-acute bout of LBP.
Method
This study involved a secondary analysis of data from an existing randomized clinical trial that was designed to determine the effectiveness of three manual physical therapy procedures in individuals who met criteria for a clinical prediction rule. This method is described in detail elsewhere (Cleland, Fritz, Childs, & Kulig, 2006; Cleland et al., 2009) and the study was registered with ClinicalTrials.gov (NCT00257998). These LoBACS data were not included published reports of the parent study (Cleland et al., 2006, 2009).
The LoBACS is a 15-item questionnaire that was used to measure SE beliefs related to the individual’s performance of back-relevant functional activities such as standing, carrying, and pushing (Functional SE [LoBACS-FN]; 7 items); SE for self-regulation of back health (Self-regulation SE [LoBACS-SELFREG]; 3 items); and SE for exercising regularly (Exercise SE [LoBACS-EX]; 5 items; (Bandura & Cervone, 1986; Lackner & Carosella, 1999; Nicholas, 2007; Williams & Myers, 1998). Each LoBACS item is structured as a statement to which the respondent rates his or her level of agreement on an 11-point scale anchored at 0% and 100%, with higher numbers indicating higher levels of SE. The LoBACS subscale and total score demonstrates satisfactory test–retest reliability, internal consistency, and preliminary estimates of validity in individuals with LBP following single-level microdiscectomy (Yamada et al., 2011). Disability, pain, and fear-avoidance beliefs are related constructs to SE. Well-validated questionnaires to measure each constructs were selected for analysis of LoBACS convergent and divergent validity. The Oswestry Disability Questionnaire (ODQ) was used to measure self-reported disability related to LBP (Fairbank, 2000; Fairbank, Couper, Davies, & O'Brien, 1980; Fairbank & Pynsent, 2000). The average of best, worst, and current pain on an 11-point numeric pain rating scale (NPRS) was used to represent the subject’s level of pain over the previous 24 hr (Childs, Piva, & Fritz, 2005; Jensen, Turner, & Romano, 1994). The Fear Avoidance Beliefs Questionnaire (FABQ) was used to assess the level of symptom-related activity-avoidance beliefs in the cohort, consisting of a Physical Activity subscale (FABQ-PA) and Work subscale (FABQ-W; Crombez, Vlaeyen, Heuts, & Lysens, 1999; Jacob, Baras, Zeev, & Epstein, 2001; Waddell, Newton, Henderson, Somerville, & Main, 1993; Waddell et al., 1993).
Descriptive statistics were calculated for demographic data and outcome measurements. Scoring for the LoBACS included scores for each LoBACS subscale, representing the mean of responses for component items. Convergent construct validity with regard to disability (ODQ), fear-avoidance beliefs (FABQ), and pain (NPRS) was established using Pearson correlations. Principal axis factoring (PAF) was used to determine discriminant construct validity, which is to say, whether the LoBACS is statistically coherent from NPRS, FABQ-PA, FABQ, and ODQ measurements (Cleland et al., 2006, 2009). Internal consistency reliability for LoBACS subscales was tested using Cronbach’s α and item to subscale total correlations. PAF was also used to assess the hypothesized three-subscale structure of the LoBACS. Statistical significance was considered α ≤ .05 for all analyses. PASW Statistics 18.0 for Mac (IBM, Quarry Bay, Hong Kong) was used for all statistical analyses.
Results
One hundred and twelve subjects were enrolled into the parent study. Mean age was 40.4 ± 11.5 years (standard deviation), 52% were female, and the mean body mass index was 19.6 ± 4.5. The mean duration of symptoms was 50.0 ± 34.9 days. Symptoms were most commonly localized to the low back and buttock (n = 111; 99%) and distal to the buttock (n = 78; 70%). Symptoms distal to the knee were reported in only six subjects (5%). Prior to the current injury episode, 95 subjects (85%) had worked regular duty. Sixty-one subjects (50%) reported missing work related to their current bout of symptoms, and 18 subjects (16%) were unable to work full duty within the 6 weeks prior to enrollment at the time of the study. Two subjects (2%) reported receiving an attorney’s advice regarding their symptoms and no subjects reported engagement in litigation at the time of the study. Fifty-two subjects (46%) also reported at least one prior episode of pain. Among prior episodes, primary localization to the lumbar spine was most frequent (n = 47; 90%).
At intake into the parent study, subjects reported decreased function, self-regulation, and exercise SE. The LoBACS-FN score was 45.3 ± 23.5 (range: 1–94), LoBACS-SELFREG score was 58.0 ± 22.5 (range: 17–100), and LoBACS-EX score was 62.3 ± 20.8 (range: 28–100). Subscale scores generally demonstrated low but significant correlations with measures that are related to the SE construct, including ODQ, NPRS, FABQ-PA, and FABQ-W. LoBACS-SELFREG showed nonsignificant correlations with both FABQ-PA and FABQ-W as well as low negative correlations with ODQ and NPRS. Cronbach’s α for LoBACS-FN was .90, LoBACS-SELFREG was .88, and LoBACS-EX was .93. All LoBACS subscale scores demonstrated moderate to strong positive correlations with LoBACS total score and all other subscale scores (p < .01). Corrected item to subscale total correlations generally exceeded .6, except for the correlation between LoBACS-FN subscale score and Item #7 (“Stand in a slow moving line for 3 hours”; Table 1). Hypothetical item classification aligned with PAF results for 14 of the 15 LoBACS items (Table 2). The only item for which PAF failed to confirm hypothetical item membership was Item #2 (“I believe that I can move a heavy phone book from an overhead cabinet to a low shelf”).
Item-Total Correlations and Cronbach’s α for Subscales of the Low Back Activity Confidence Scale.
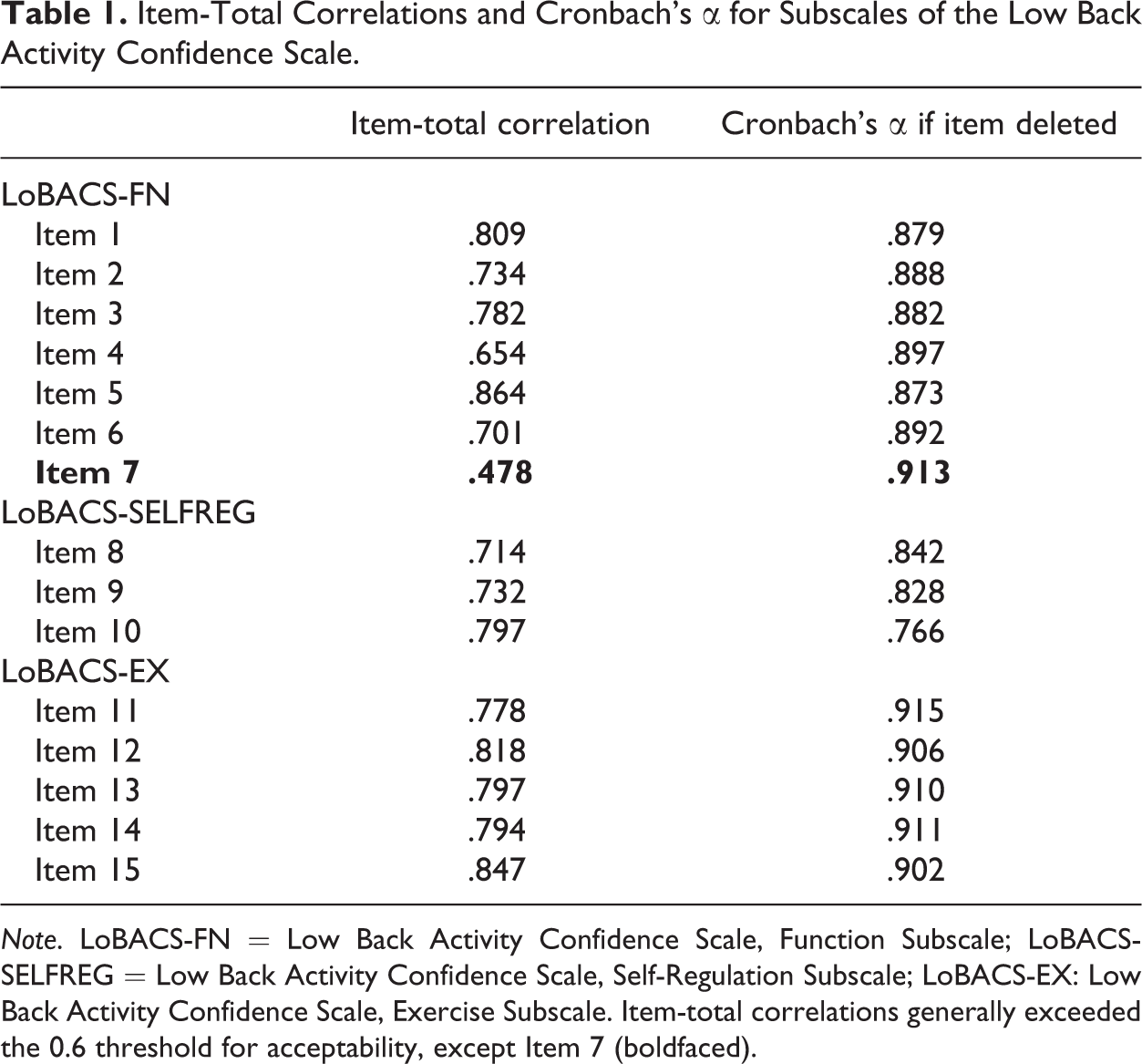
Note. LoBACS-FN = Low Back Activity Confidence Scale, Function Subscale; LoBACS-SELFREG = Low Back Activity Confidence Scale, Self-Regulation Subscale; LoBACS-EX: Low Back Activity Confidence Scale, Exercise Subscale. Item-total correlations generally exceeded the 0.6 threshold for acceptability, except Item 7 (boldfaced).
Subscale Structure of the Low Back Activity Confidence Scale.
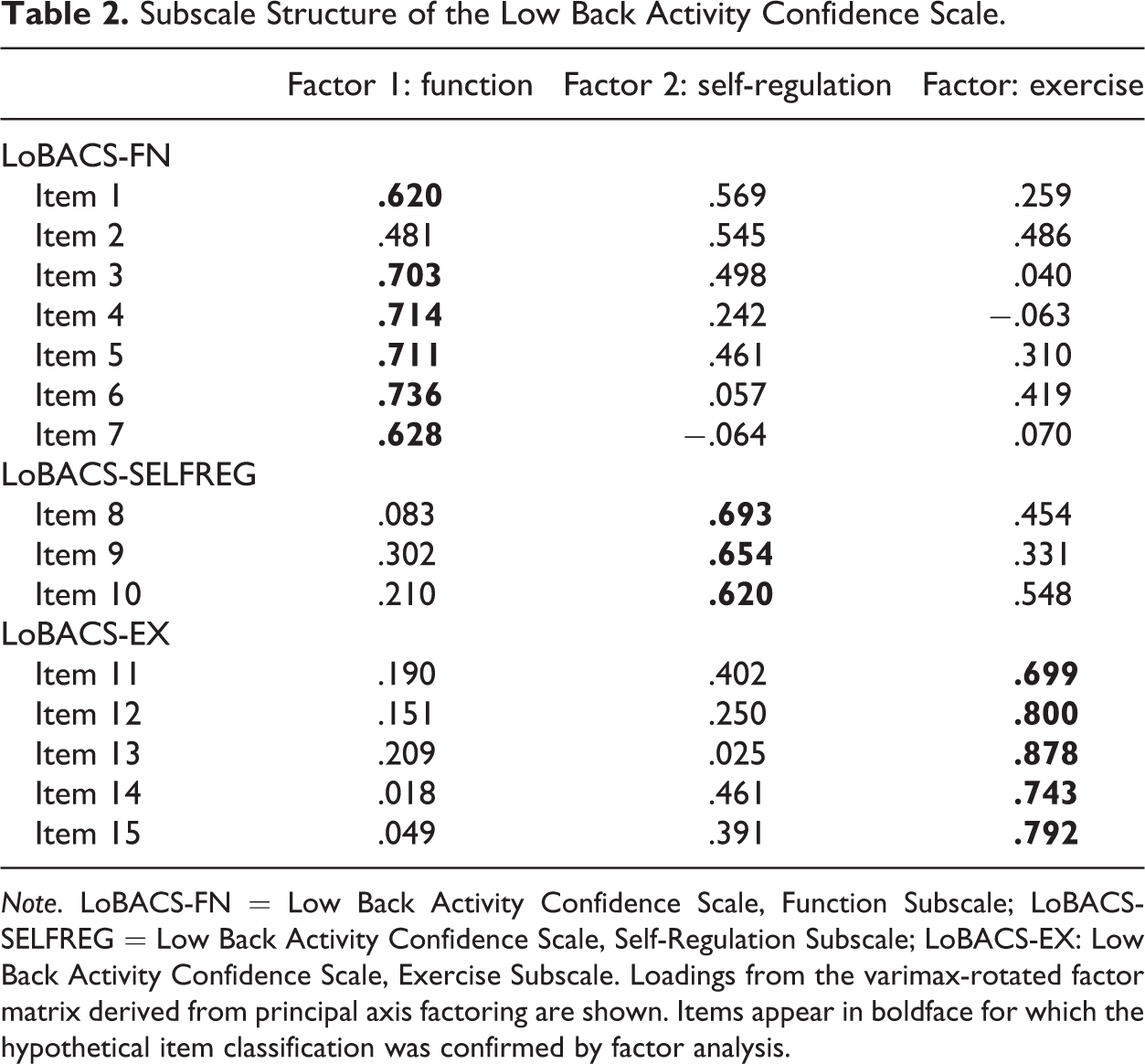
Note. LoBACS-FN = Low Back Activity Confidence Scale, Function Subscale; LoBACS-SELFREG = Low Back Activity Confidence Scale, Self-Regulation Subscale; LoBACS-EX: Low Back Activity Confidence Scale, Exercise Subscale. Loadings from the varimax-rotated factor matrix derived from principal axis factoring are shown. Items appear in boldface for which the hypothetical item classification was confirmed by factor analysis.
LoBACS subscale scores, NPRS, and FABQ subscale scores coalesced onto three factors that accounted for 74% of total variance in the data. Factor 1 included LoBACS-FN (factor loading [FL]: .66), LoBACS-SELFREG (FL: .93), and LoBACS-EX (FL: .78), so it was named the “Self-Efficacy” factor. The Self-Efficacy factor accounted for 36% of explained variance (EV) in the data. Factor 2 (EV: 20%) consisted of FABQ-W (FL: .85) and NPRS (FL: .34), so it was called the “avoidance and pain” factor. Factor 3 (EV: 18%) involved the ODQ (FL: .62) and FABQ-PA (FL: .61), so it was named the “avoidance and disability” factor. LoBACS-EX loaded weakly onto the avoidance and disability factor.
Discussion
This study reported on the clinimetric properties of the LoBACS to measure SE in patients with acute and post-acute LBP who met a manual therapy clinical prediction rule and received nonsurgical intervention. The LoBACS demonstrated evidence of construct validity with regard to measures of disability, pain, and fear-avoidance beliefs. Associations between LoBACS subscale scores and measures of disability, pain, and fear-avoidance beliefs were in the anticipated directions but yet small in magnitude, which suggests a substantial portion of variance was left unexplained by these univariate relationships. Internal consistency reliability was sufficient for LoBACS subscales without indication of item redundancy, and the hypothetical factor structure of the LoBACS also was confirmed. The findings of this study are clinically relevant, because the LoBACS improves on previous measurements of SE by way of its specificity to LBP-related behaviors. The self-regulatory and exercise SE subscales of the LoBACS may demonstrate greater value than general SE measurements to predict individuals at risk for nonadherence to an ongoing exercise regimen (Fontaine & Shaw, 1995; Jones, Harris, Waller, & Coggins, 2005; Robertson & Keller, 1992). This study also represents a meaningful extension of prior findings in individuals with LBP who sought surgical intervention (Yamada et al., 2011).
The findings of this study suggest that future research should involve the LoBACS to deal with additional questions this particular study was not designed to address. This study’s findings should not be expected to generalize to all individuals with LBP, so it should be repeated in other populations of special clinical interest such as individuals with LBP related to occupational injuries. Future randomized clinical studies and prospective cohort studies should utilize the LoBACS in combinations with other pain, activity-avoidance beliefs, and disability measurements. The LoBACS should be empirically compared to other questionnaires that have been designed to measure SE in health behaviors. This study was not designed to assess the specific causal relationships among SE, fear avoidance, pain, and disability, so ongoing research should use the LoBACS to further assess the hypothesis that SE mediates the relationship between fear avoidance, disability, and LBP (i.e., Denison et al., 2004). Future studies also should help establish the validity of the LoBACS to measure SE in individuals with LBP, which may lead to improved patient classification and the development of psychoeducational interventions that are matched to patient subgroups based on their SE beliefs (i.e., Denison, Asenlof, Sandborgh, & Lindberg, 2007). The LoBACS can contribute to these ongoing lines of research that will improve our collective understanding of the interplay between psychobehavioral factors and patient functioning, as well as the relevance of SE beliefs in clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the American Academy of Orthopaedic Manual Physical Therapists and Cardon Rehabilitation Products to J.A. Cleland.