
Abstract
The chronic care model (CCM) concerns both the medical and the cultural and linguistic needs of patients through the inclusion of cultural competence in the delivery system design. This literature review attempted to@@ identify the domains of the CCM culturally competent (CC) interventions that the adults from ethnic minorities suffering from type 2 diabetes mellitus report. We identified the CCM and the CC components in the relevant studies published between 2005 and 2014. Thirty-two studies were included. Thirty-one articles focused on self-management and 20 on community resources. Twenty-three interventions integrated cultural norms from the patients’ backgrounds. CC interventions reported the CCM at the individual level but need to address the organizational level more effectively. The scope of CC interventions should be expanded to transform health care organizations and systems.
Keywords
Introduction
The type 2 diabetes mellitus (type 2 DM) epidemic affects millions of people around the world and is predicted to continue to do so (Brinks, Tamayo, Kowall, & Rathmann, 2012; Chen, Magliano, & Zimmet, 2012; Holman, Forouhi, Goyder, & Wild, 2011). A higher prevalence of type 2 DM is observed among ethnic minority groups when compared to majority population groups, that is, African Americans compared to White Americans, South Asians compared to White British, and Turks and Moroccans compared to Belgians (Abouzeid, Philpot, Janus, Coates, & Dunbar, 2013; Garduño-Diaz & Khokhar, 2012; Gholap, Davies, Patel, Sattar, & Khunti, 2011; Gujral, Echouffo-Tcheugui, & Narayan, 2011; Khunti et al., 2013; Kountz, 2012; Vandenheede & Deboosere, 2009). These ethnic minority groups have a greater risk of retinopathies, renal disorders, neuropathies, amputations, and premature deaths due to type 2 DM (Bellary et al., 2010; Campbell, Walker, Smalls, & Egede, 2012; Kanaya et al., 2011; Y. Long, Gracely, Newschaffer, & Liu, 2012). Moreover, they usually have poorer glycemic control and lower adherence to treatments (Bellary et al., 2010; James et al., 2012; Parker et al., 2012) and are more frequently hospitalized for severe glycemic troubles (Kim, Ford, Chiriboga, & Sorkin, 2012). Several factors prevent migrants from accessing the appropriate health care. These include living and socioeconomic conditions (Abouzeid et al., 2013; Sims et al., 2011; Zheng et al., 2012) as well as linguistic and cultural barriers (Bell, 2011; Wilson et al., 2012). Moreover, discrimination and institutional or individual racism increase the challenges for ethnic minorities, leading to poorer health outcomes (Gonzales, Harding, Lambert, Fu, & Henderson, 2013; Pieterse, Todd, Neville, & Carter, 2012).
As a consequence, there is increasing pressure on health professionals and health services to become culturally competent (CC). CC interventions have been recommended in order to reduce inequality between the ethnic minorities and the general population and to improve the quality of care delivered (Brach & Fraserirector, 2000; Kirmayer, 2012). According to the holistic definition proposed by Betancourt, Green, Carrillo, and Ananeh-Firempong II (2003, p. 294), “a ‘culturally competent’ health care system has been defined as one that acknowledges and incorporates—at all levels—the importance of culture, assessment of cross-cultural relations, vigilance toward the dynamics that result from cultural differences, expansion of cultural knowledge, and adaptation of services to meet culturally unique needs. A culturally competent system is also built on an awareness of the integration and interaction of health beliefs and behaviors, disease prevalence and incidence, and treatment outcomes for different patient populations.” The development of CC interventions requires multilevel health care strategies including patients, health professionals as well as health services, and the health system itself (Betancourt, Green, Carrillo, & Ananeh-Firempong II, 2003; Kirmayer, 2012). This involves a wide range of interventions such as the development of diversity-oriented health policies, the deployment of interpreters and intercultural mediators in various health care facilities, the support of culturally specific health services or ethnically sensitive health promotion campaigns (Anderson, Scrimshaw, Fullilove, Fielding, & Normand, 2003; Betancourt et al., 2003; Fisher, Burnet, Huang, Chin, & Cagney, 2007). Moreover, previous studies have shown that CC programs may perform better for ethnic minorities than the non-CC programs (Henderson, Kendall, & See, 2011; Renzaho, Romios, Crock, & Sonderlund, 2013).
As with other chronic illnesses, patients with type 2 DM require disease management to ensure high-quality care (Weingarten et al., 2002). Wagner’s chronic care model (CCM) has been proven to be a useful guide to improving care quality for chronic conditions (Coleman, Austin, Brach, & Wagner, 2009). In the 2003 update, paying attention to the cultural background of the patient was acknowledged as a component of the CCM (The MacColl Center, 2013). The CCM framework recommends the delivery of health care adapted to the cultural background of the patient. To achieve this objective, the CCM framework integrates cultural competence components in the design of the delivery system. The recommendation is to “give care that patients understand and that fits with their cultural background.” This apparently limited focus contrasts with the basic principles of models of cultural competence, which emphasize that attention should be given to cultural and linguistic traits within all aspects of health care, if a holistic perspective is to be applied (Campinha-Bacote, 2002). Beyond culture, holistic models of cultural competence include attention to health beliefs, socioeconomic factors, familial context, and racism or discrimination (Betancourt et al., 2003; Kirmayer, 2012; Saha, Beach, & Cooper, 2008). Moreover, according to previous studies, cultural competence should be deployed at patient level, health professional level, institutional level, and political levels (Anderson et al., 2003; Brach & Fraserirector, 2000). So far, as domains of health care interact, we may question whether cultural competence is present in other aspects of diabetes management. For example, patient education may require cultural competence in order for it to be effective for ethnic minority groups, and this should be reflected in the “self-management support” category of the CCM. We attempted to identify the domains of the CCM CC interventions that the adults from ethnic minorities suffering from type 2 DMs include. In other words, our research question was “in which aspects of type 2 diabetes management, is cultural competence included?” We have attempted to answer this question with a review of the international literature published between 2005 and 2014.
Method
Search Strategy and Data Extraction
We conducted a literature review to identify CC interventions in adults from ethnic minorities suffering from type 2 DM. The initial search strategy was developed for MEDLINE, based on the Patient Intervention Comparison Outcome (a process for building a search strategy in electronic databases) method. The main Medical Subject Heading terms were “cultural competence” AND “type 2 DMs” AND “ethnic minorities.” This strategy served as the basis for searching the other electronic databases and was adapted to the characteristics of the other databases to maximize sensitivity. We used truncated search terms to increase the sensitivity of our results. The inclusion criteria for the study design were not limited to randomized controlled trials but also included qualitative studies, cohort studies, and other designs. No restrictions were made on the length of the follow-up in the studies. The time span for the review was from 2005 to 2011. Between November 2011 and December 2011, we searched (1) MEDLINE, (2) IsiWeb of Science, (3) Database of Abstracts of Reviews of Effects (DARE), (4) the Cochrane Database, and (5) Dopher. We also identified three journals, namely, (1) The Diabetes Educator, (2) Ethnicity and Health, and (3) Ethnicity and Disease, in which we conducted additional queries. We updated our search in August 2014 and searched for additional articles published between January 2012 and July 2014. We also scanned the references of some key review articles that we had previously identified in our electronic searching. We only selected published material.
The data extraction procedure was based on the criteria developed by the Center for Reviews and Dissemination. Citations and abstracts were stored in the RefMan© program. Standardized review forms were developed in an Excel database in order to (1) identify the CC components of the interventions, (2) identify the CCM components within the interventions, and (3) identify the study characteristics and outcomes. The forms were based on the literature on cultural competence and on CCM (Betancourt et al., 2003; Bischoff, 2003; Bodenheimer, Wagner, & Grumbach, 2002a, 2002b; Brach & Fraserirector, 2000; Coleman et al., 2009; Griner & Smith, 2006; Pearson et al., 2005).
Study Selection
The review process of the articles was carried out by three reviewers (M.D., W.D., & V.L.). Each reviewer first individually checked the abstract on the basis of inclusion and exclusion criteria. Inclusion criteria were interventions with a clear focus on type 2 DM, presence of at least one group of patients identified as a member of an ethnic minority (in relation to the national context of ethnicity), and interventions in inpatient or outpatient settings. Three categories of exclusion criteria for the abstracts are article-, patient-, and intervention-related exclusion criteria (see Figure 1 for details of exclusion criteria). At the end of the review process, each abstract received a code, namely, A (accepted), C (further reading before final decision), or R (rejected). Divergent coding was discussed and the final decision for acceptance was made following the discussion. We then reviewed the full articles of those with abstracts in Categories A and C. A common measure of outcomes was then chosen to ensure better comparability between the studies. Glycated hemoglobin (HbA1c) was identified because it is a widely recommended clinical indicator of the follow-up and quality of diabetes care (American Diabetes Association, 2012) that may also reflect psychobehavioral changes such as better adherence to self-management activities. Articles without a measure of HbA1c were excluded.
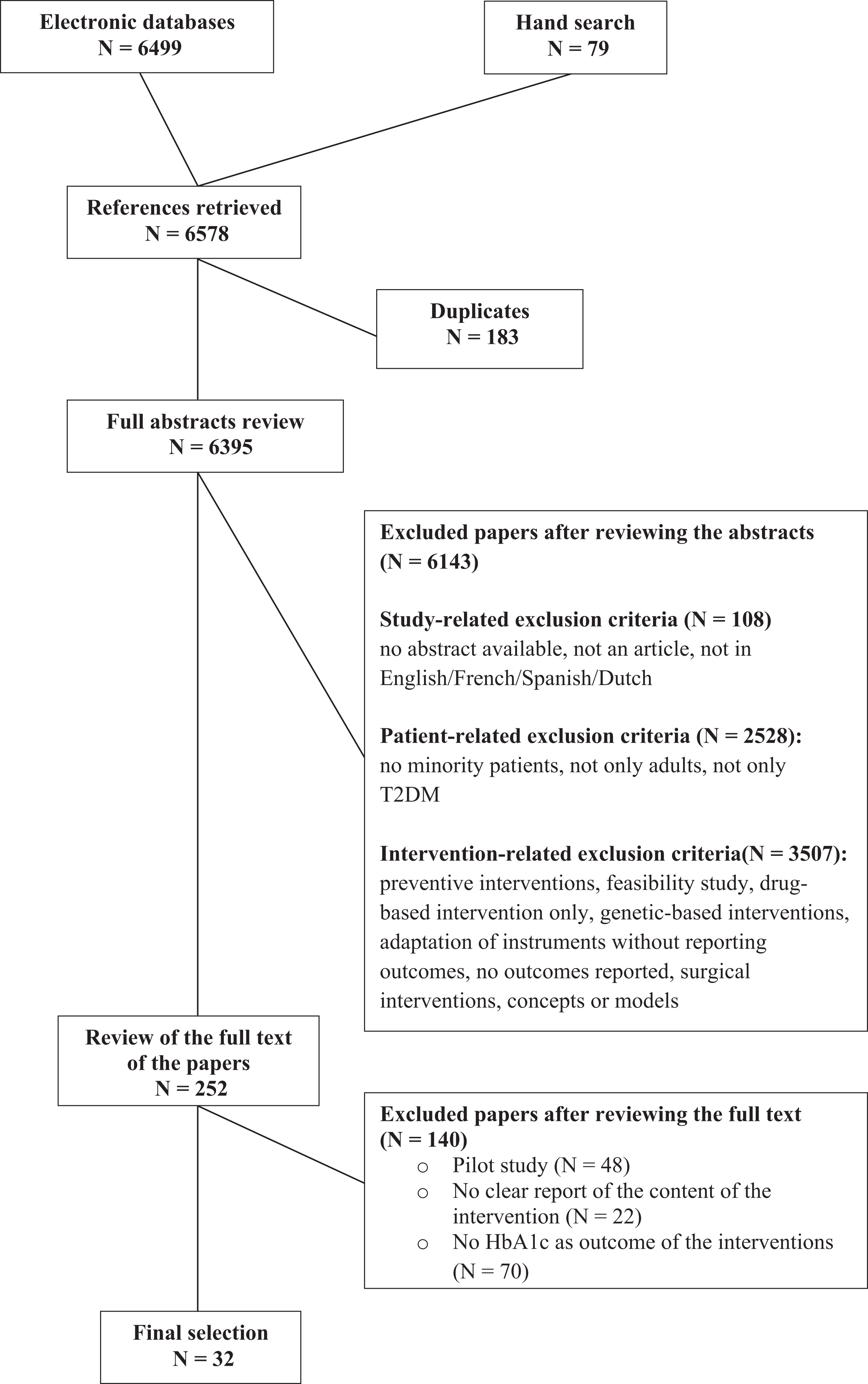
Review process of the literature search on culturally competent interventions in type 2 diabetes mellitus published between 2005 and 2014.
Classification of the Interventions
Two independent reviewers (M.D. and Marie France Libion) classified the interventions according to their CC components and CCM elements. Divergent coding was discussed and the final decision on the classification of the interventions was made by consensus. The definition and operationalization of the dimensions of the CCM were modeled on the classification used by Pearson and colleagues (2005). The CCM comprises six principal domains of actions, namely, (1) self-management support, (2) community resources and policies, (3) delivery system design, (4) clinical information systems, (5) decision support, and (6) health care organization (Bodenheimer et al., 2002a). Self-management support directly concerns the patient and includes components such as patient education and psychosocial support as well as self-management activities such as foot care or self-monitoring for glycemia. Delivery system design consists of changes in patient flows and clinical personnel through the introduction of care management roles, planned follow-ups, or synchronized visits. Decision support directly concerns health professionals. Decision support is aimed at improving their knowledge and skills through education and introducing guidelines, health protocols, or consulting external experts. Clinical information system concerns both health professionals and institutions. It may consist of reminder systems or performance feedback (Bodenheimer et al., 2002a, 2002b; Pearson et al., 2005; Tsai, Morton, Mangione, & Keeler, 2005). At the macro level, community resources and policies target patients and communities and involve, for example, partnership programs with local associations, collaboration with peers to deliver the intervention as well as policies aimed at improving the overall health of the patient.
Classification criteria for CC interventions were defined according to previous studies (Betancourt et al., 2003; Bischoff, 2003; Brach & Fraserirector, 2000; Griner & Smith, 2006; Kirmayer, 2012). We arrived at the following five categories: (1) cultural tailoring of interventions to meet the cultural needs of patients (responsiveness) in such a way that the content, the process, or the method used is adapted to the cultural background of the patient, for example, delivering the intervention in a church, including religious beliefs in the intervention, or adapting an existing educational intervention by adding specific cultural references; (2) interventions focusing on communication factors (including language concordance and interpreters); (3) interventions using peers or community members; (4) interventions targeting the patient-health professional ethnic concordance or ethnic matching (where the professional and the patient belong to the same ethnic group); and (5) training of health professionals to improve their cultural competence.
Results
Characteristics of the Included Studies
After reviewing 5,284 references and checking 102 abstracts, we found 25 studies that met our inclusion criteria (Figure 1). After the August 2014 update, seven additional studies were included. Table 1 shows the characteristics of the 32 studies, including the CCM components and the CC components. Ten articles had been published in diabetes-related journals, 10 articles had been published in health education–related journals, and the remaining articles had been published in nursing journals, public health journals, or community health journals. Most of the studies were conducted in the United Sates (n = 28). The duration of the studies varied from 3 to 24 months. In 10 studies, the outcomes were collected at least twice postintervention. Eight studies used a before/after design, while other studies were comparative studies comprising a control group. The control groups usually received standard care. In some studies, the participants in the control groups received the intervention after the follow-up period. Twenty-six interventions concerned patients belonging to a sole ethnic group, for example, a homogeneous group of Latinos. In four studies, participants belonged to various ethnic groups, including a nonminority group such as White patients compared with Black patients. In the two remaining studies, the participants were from various ethnic groups but without a majority group, for example, African Americans and Hispanics.
Characteristic of Selected Studies.
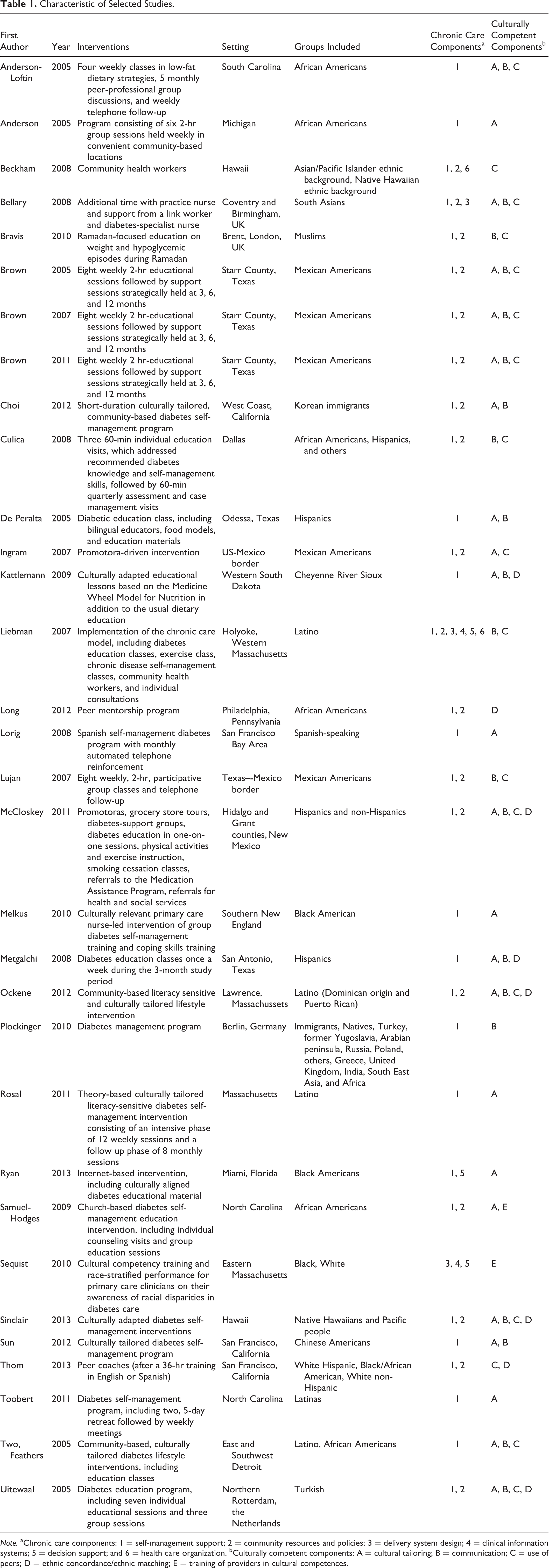
Note. aChronic care components: 1 = self-management support; 2 = community resources and policies; 3 = delivery system design; 4 = clinical information systems; 5 = decision support; and 6 = health care organization. bCulturally competent components: A = cultural tailoring; B = communication; C = use of peers; D = ethnic concordance/ethnic matching; E = training of providers in cultural competences.
Characteristics of the Selected Interventions
Table 2 shows the characteristics of the selected interventions according to their design, the domains of the CCM, and the CC components in the 32 studies. Seventeen interventions included a collective and an individual component such as individual telephone follow-ups and educational group sessions. Nine interventions were delivered to a group of patients while the remaining six interventions were delivered via one-on-one interaction. When delivered to a group of patients, interventions consisted of educational group sessions. These group sessions focused on self-management skills, exercise and physical activity, or lifestyle. Some sessions also included sharing experiences with peers or health professionals. When delivered in one-on-one interactions, interventions consisted of individual education sessions, often combined with telephone follow-ups. Diabetes educators delivered interventions in 10 studies, while nurses were involved in 10 studies. Interventions were also delivered by dieticians (n = 6) and physicians (n = 5).
Characteristics of the Selected Interventions.

Domains of the CCM
On average, each intervention addressed two domains of the CCM. The most frequent domains of the CCM were self-management support (n = 31) and community resources and policies (n = 20). Among the interventions including community resources, we found interventions hiring link workers (i.e., promotoras) or developing partnerships with local associations such as churches. Six interventions modified the design of the delivery system by, for example, introducing a nurse case manager, synchronizing provider visits, or using open-access scheduling. In four studies, interventions consisted of the development of clinician information systems, mostly performance feedback. Four interventions aimed to support the decision-making process of the health professionals by, for example, introducing clinical guidelines. Two interventions modified the organization of health care by introducing interdisciplinary health care teams within the health care setting.
CC Components in the Interventions
On average, each intervention included two CC components. The most frequent CC components were cultural tailoring (n = 23) and communication (n = 19). In the cultural tailoring category, the 23 interventions adapted an existing intervention to the specific needs of the patients. In these cases, previously culturally blind interventions were adapted by including references to specific cultural norms of the patients’ cultural background. Nineteen interventions involved specific attention to communication factors, while seven interventions targeted ethnic matching (also reported as ethnic concordance) between the provider of the intervention and the patients. Communication factors and ethnic matching were mainly used with Hispanic/Latino and South Asian patients. In seven studies, ethnic matching occurred at the individual level. In one study, matching occurred between the patients and their health educators (Uitewaal et al., 2005) and in one other study, between the patients and the dieticians (Metghalchi et al., 2008). In five studies, matching occurred between the patients and the peers used to deliver the interventions (Kattelmann, Conti, & Ren, 2009; J. A. Long, Jahnle, Richardson, Loewenstein, & Volpp, 2012; McCloskey, Tollestrup, & Sanders, 2011; Sinclair et al., 2013; Thom et al., 2013). Twelve interventions relied on patients’ peers as CC participants in the intervention. In nine studies, peers received specific training to deliver the intervention to their counterparts. In 11 studies, peers were used as bridges between the health professionals and the patients to implement the interventions. More specifically, in two studies, peers were used to recruit participants. Eight interventions used culturally adapted educational material and only two interventions involved a professional interpreter. Health professionals received cultural competence training in only one intervention, and other training programs identified in the interventions were based on clinical issues.
Domains of the CCM identified in CC Interventions
Main findings
Table 3 reports the domains of the CCM that were addressed or incorporated by CC interventions. Individual articles may be represented multiple times in the table because what it compiles are individual CC strategies and the CCM components that they addressed. For example, if an article reported use of peers as a CC strategy and the use of peers addressed both self-management and community resources as the CCM components, that single intervention use of peers would be entered twice in the table, that is, once for the use of peers/self-management support and another for the use of peers/community resources and policies. Table 3 illustrates where the developers of the CC interventions focused their attention. Broadly speaking, the most common CC components addressed were cultural tailoring, communication factors, and use of peers. We noted that those articles that reported the commonly addressed components of CC interventions also reported the commonly addressed domains of CCM, that is, self-management support and community resources and policies.
Domains of the Chronic Care Model Identified in the Domains of the Culturally Competent Interventions.a
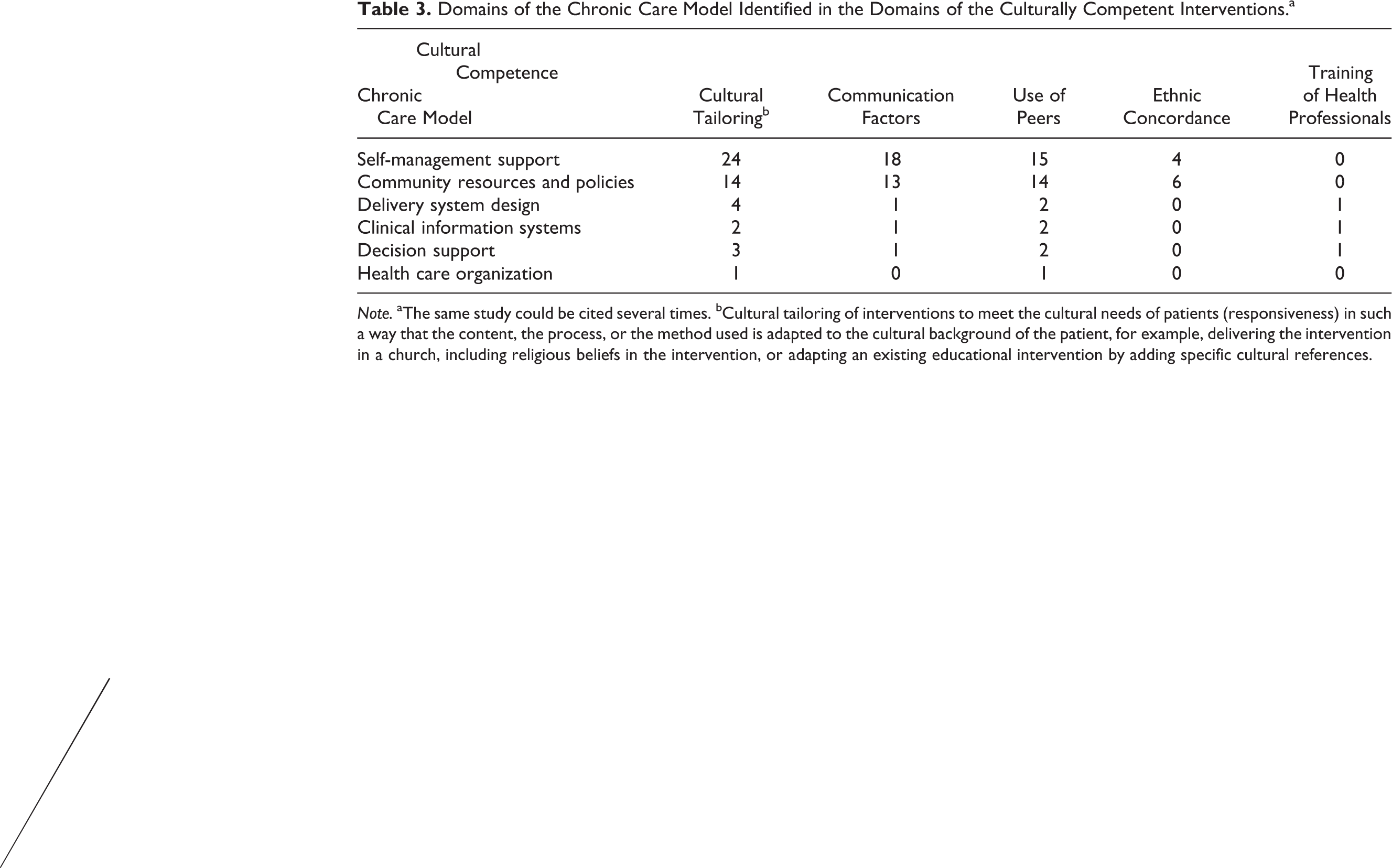
Note. aThe same study could be cited several times. bCultural tailoring of interventions to meet the cultural needs of patients (responsiveness) in such a way that the content, the process, or the method used is adapted to the cultural background of the patient, for example, delivering the intervention in a church, including religious beliefs in the intervention, or adapting an existing educational intervention by adding specific cultural references.
Self-Management Support and Cultural Tailoring
We observed that the self-management support was mostly reported in the category cultural tailoring (n = 24). In that case, interventions were adapted to the cultural background of the patients. For example, Kattelmann and colleagues (2009) integrated the concept of the Medicine Wheel Nutrition intervention in their intervention with the Cheyenne Sioux River. In other interventions matching self-management support and cultural tailoring, patients received dietary advice integrating traditional recipes and culturally appropriate substitutes, such as in the intervention of Beckham and colleagues with Hawaiian and Samoan patients (Beckham, Bradley, Washburn, & Taumua, 2008). When interventions were aimed at improving the level of physical activity, they relied on forms of exercise that were more likely to be accepted by the ethnic minority patients, such as dance for African American women.
Communication and Use of Peers
Self-management support was reported in the categories communication (n = 18) and use of peers (n = 15). In interventions reporting both self-management support and communication, leaflets and other education material were provided in the preferred language of the patients. Interventions reporting self-management support and use of peers included the involvement of peers as participants or leaders in the activities, with or without the support of health professionals.
Community Resources and Policies and Use of Peers
We also observed that community resources and policies were approached through the use of peers (n = 14), cultural tailoring (n = 14), and communication (n = 13). Some interventions relied on resources provided by religious communities to enroll patients in the interventions. Other interventions were held in community-relevant locations for the patients, such as churches for African Americans or community centers (Samuel-Hodges et al., 2006). There was only one intervention that aimed to train health professionals in cultural competence. This intervention was combined with the introduction of patient subgroup-stratified performance reports and recommendations to support the clinical decisions (Sequist et al., 2010). Contrary to the CCM framework, only a few interventions integrated cultural competence components into the domain delivery system design. The same was observed for the domains clinical information systems, “health care organization,” and decision support. Finally, only one intervention reported all six domains of the CCM. This intervention aimed at implementing the CCM for Latinos with type 2 DM.
Results from the Sensitivity Tests
We initially tried to meta-analyze the results but the sensitivity tests were inconclusive because of the heterogeneity of the patients enrolled in the studies, the follow-up duration, and other design issues. The χ2 test for the heterogeneity was highly significant (coefficient value: 300.84, p < .0001), supporting the hypothesis that our data are too heterogeneous to be used in a meta-analysis. The I 2 statistic had a value of 98.7%, indicating that 98.7% of the variance is attributable to the heterogeneity of the studies.
Discussion
This literature review addressed the following research question, “which are the domains of the CCM framework CC interventions that adults from ethnic minorities suffering from type 2 DMs tend to report?” We identified 32 articles that met our inclusion criteria. Our findings show that cultural competence is being pursued with a limited number of strategies that, in turn, are addressing limited dimensions of the CCM. Articles reporting interventions addressing cultural competence also tended to address the self-management support and community resources and policies domains of the CCM but pay less attention to other domains of the CCM such as delivery system design or health care organization.
Although the developers of the CCM recommend cultural competence as a dimension of the delivery system design, we observed the presence of cultural competence in the development of self-management aspects of the intervention. These interventions did not imply modification of the delivery system design, that is, they focused on patients, with minimal emphasis on health services or on health professionals. These findings are supported by the review of Peek, Cargill, and Huang (2007).
The interventions we identified targeted mainly patients and their families but paid less attention to health professionals or health services. Why is this so? First, modifying health services and/or the health care setting requires the serious involvement of managers as well as funding to adapt health services to the specific situation of ethnic minority patients with type 2 DM (Brach & Fraserirector, 2000; Kirmayer, 2012). Integrating a chronic care perspective into health services requires a similar commitment to organizational change and to improving practice by integrating CC components. As well as the willingness of health professionals to become more competent in intercultural and chronic care, the commitment of informal and formal leaders is also essential at the service, managerial, and political levels in order to develop and sustain projects. Developing chronic care or CC care may result from demands of the patients but may also be influenced by political priorities (Nolte & McKee, 2008) or international recommendations such as the Memorandum of the Council of Europe on Health Care in a Multicultural Society (Council of Europe, 2006). The funding of health programs and health initiatives is part of the political process and needs a window of opportunity to receive the attention of policy makers (Shiffman & Smith, 2007).
Second, if they are to persist, organizational changes must be accepted and sustained by both health professionals and local communities (Grol & Wensing, 2004). Few interventions brought health professionals and local communities together with a view to establishing a strong partnership. Collaborative approaches between communities and health services may help to clarify the values and expectations of health professionals and patients (Wallerstein & Duran, 2006) and consequently lead to better adherence by patients. To support the development of organizational changes, interventions should involve more participatory-based approaches in which both the community and the health professionals work together to develop the health program. This approach has already been used in health promotion projects (Wallerstein & Duran, 2006) and has shown promising results (Pazoki, Nabipour, Seyednezami, & Imami, 2007).
Third, health professionals may not be aware of the CC approach or of chronic care management. Working within CC and chronic care perspectives implies working within a patient-centered perspective (Bodenheimer et al., 2002a; Saha et al., 2008). Training of health professionals or at least improving their awareness about these issues is an essential step in the development of a health system providing CC chronic care (Kirmayer, 2012).
Limitations of the Present Study
This literature review has some limitations. First, eligibility was limited to English-, Spanish-, Dutch-, or French-language publications and to published, indexed studies. It is likely that more interventions on type 2 DM exist that have not been published. However, some have suggested that these limitations do not substantially affect the results of reviews (Egger, Juni, Bartlett, Holenstein, & Sterne, 2003). We are aware that a publication bias could occur, as is the case with all literature reviews. A more extensive search might have identified more diverse literature than we have found, but our findings appeared to be representative of the field of type 2 DM interventions.
This literature review focused on a specific chronic condition. This may prevent the extrapolation of conclusions to situations involving other chronic diseases and comorbidities. type 2 DM is traditionally acknowledged as a condition affecting adults, although the mean age of newly diagnosed patients is decreasing (Fagot Campagna et al., 2000). Perspectives could be different for chronic conditions diagnosed in childhood, such as type 1 DM, or environment-based chronic diseases such as asthma (Bailey et al., 2009). Moreover, we excluded articles that did not report HbA1c, as our initial plans were to evaluate outcomes and that including these articles might extend or modify our findings.
The low number of interventions developed at the service level or institutional level could be a reporting bias. Authors may not have reported modifications at the service or institutional level. Organizational interventions are more difficult to define, assess, and report (Rychetnik, Frommer, Hawe, & Shiell, 2002; Ukoumunne, Gulliford, Chinn, Sterne, & Burney, 1999). Using a clinical outcome as the intervention outcome in our review may have prevented us from identifying studies with interventions at the service level. However, previous studies reported that interventions at the institutional/service level are still lacking for CC health care and chronic care (Stein, 2009).
The organization of the health system may also play a role in the development of interventions at service level. We did not take national health systems into account in our analysis. In some countries, the health care organization acknowledges chronic care as a basic component of its system while, in other countries, integration of chronic care in health services has just begun, as highlighted in two World Health Organization (WHO) reports (WHO, 2011, 2012). The same is observed for CC care, that is, some health systems are pioneers in the development of CC care, while other countries still need to integrate intercultural care into their health policies (Lorant & Bhopal, 2010). This last statement may also explain why we found studies mainly from the United States in our review. Local and national contexts must, therefore, be key elements of further studies aimed at assessing both chronic care and CC care. Although the majority of the studies identified have been conducted in the United States, we believe that our findings may also concerned European contexts, especially in continental Europe where the attention to diversity is not (yet) included in the delivery of health care (Ingleby, 2011; Lorant & Bhopal, 2010).
Our review aimed to assess whether or not CC interventions report the domains of CCM. It is true that our search strategy did not identify a sample of articles addressing the CCM and type 2 DM among which the existence of CC components might have been appraised. Our reasons were, first, that the basic principles of current models of cultural competence emphasize that attention should be given to cultural and linguistic traits within all dimensions of health care. Therefore, if models of cultural competence are coherent with the CCM, which they should be, they should report the different domains of the CCM. Second, CC interventions, worldwide, are generally focused on targeted groups, that is, it is unlikely that studies of the CCM in the general population would consider these groups. Indeed, the landmark studies of such models rarely refer to the ethnicity or race of the participants (Bodenheimer et al., 2002a, 2002b; Pearson et al., 2005; Tsai et al., 2005). Further research should focus on CCM interventions for type 2 DM and appraise the existence of CC within these interventions.
Recommendations
To our knowledge, this study is one of the first to use the CCM framework to shed light on the targets of CC interventions for ethnic minorities with type 2 DM. Further interventions need to be CC in a thorough way, not just adopting one or two “token” CC strategies (e.g., a pamphlet in Spanish, a poster with ethnically diverse models, and dietary recommendations reflecting cultural practices). Consequently, further interventions need a template not only of CC strategies but also of the key areas of interventions to provide criteria for assessing the extent of the implementation of cultural competence. The CCM provides a common and useful template in this regard. Our findings show that CC strategies are generally confined to the self-management and community supports components of CCM. It highlights a priority of research to identify how cultural competence may be extended to other components of the CCM and, more broadly, health care in general.
Footnotes
Authors’ Note
The technical appendix of the literature review is available on request to the corresponding author.
Acknowledgments
The authors would like to thank Marie France Libion (MFL) for her substantial contribution to the data analysis, Isabelle Aujoulat for reviewing the manuscript, and the four anonymous reviewers for their valuable comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through a research fellow grant from the Fond de la Recherche Scientifique de Belgique (F.R.S.-FNRS) awarded to Marie Dauvrin (grant number: FC84070 2009-2013). Marie Dauvrin is currently a postdoctoral researcher funded by the program Prospective Research for Brussels (INNOVIRIS) of the region of Brussels Capital, Belgium. The sponsors have had no involvement in the study design, data collection, data analysis, manuscript preparation, and/or publication decisions.