
Abstract
Studies that have examined gender differences in smoking cessation have produced mixed results. The purpose of the study was to examine whether there are gender differences in long-term smoking abstinence rates in smokers treated with nicotine patches at a smoking cessation clinic in Taiwan, where 39% of men and 5% of women smoke. This study included 1,065 smokers, comprising of 940 men and 125 women. Smokers were invited to attend the clinic every 1–2 weeks for a maximum of eight visits over 90 days, where they received prescriptions for nicotine patches, counseling, and educational materials. Participants were contacted by telephone at 1 and 3 years after the first visit and were asked whether they had smoked at all over the past 7 days. The results showed that women were significantly less likely than men to be abstinent at 1 year (adjusted odds ratio [aOR] = 0.64; 95% CI [confidence interval] = [0.41, 0.99]; p = .044) and 3 years (aOR = 0.44; 95% CI = [0.27, 0.74]; p = .02). More effective ways are needed to help female smokers quit in societies where smoking in women is rare and may be associated with social stigma.
Introduction
Gender differences in smoking cessation remain unclear. Several studies and one meta-analysis of clinical trials of nicotine replacement treatment reported lower quit rates in women (Bjornson et al., 1995; Ghani et al., 2012; Perkins & Scott, 2008), while more recent analyses of large population data sets from United States, Canada, and United Kingdom suggested lower quit rates in men (Fidler, Ferguson, Brown, Stapleton, & West, 2013; Jarvis, Cohen, Delnevo, & Giovino, 2013). A study conducted in a clinic setting in Taiwan found quit rates to be significantly lower among women (Hsueh et al., 2013). The current study examined gender differences in a large cohort of smokers who were followed for 3 years.
Method
Setting
The study was conducted at the Smoking Cessation Clinic at the Department of Family Medicine, Kaohsiung Veteran General Hospital, Taiwan. This clinic is run by the physicians who provide up to eight counseling sessions and nicotine patches over a 90-day period. The treatment is subsidized by the National Health Insurance.
Participants
Participants were smokers who wanted help in quitting and attended the clinic between September 2002 and July 2007. To qualify for treatment, participants had to be aged 18 years or older, have national health insurance, and smoking ≥10 cigarettes per day (CPD) or having a Fagerstrom Tolerance Questionnaire (FTQ) score ≥5 or a Fagerstrom Test for Nicotine Dependence (FTND) score ≥4. Smokers were excluded from the study if they were pregnant or with an acute unstable medical condition. These criteria are set by the Bureau of Health Promotion in Taiwan. Of the 1,096 participants who started treatment during this period, 31 died prior to the 3-year follow-up and were excluded from the analysis, resulting in the final sample of 1,065.
Intervention
At the first visit, participants received 15–20 min of counseling, educational materials, and a prescription for nicotine patches. Those smoking 20 or more CPD received Nicotinell TTS30® (delivering 21 mg/24 hr) for 4 weeks, followed by Nicotinell TTS20 (delivering 14 mg/24 hr) for 2 weeks and Nicotinell TTS10 (delivering 7 mg/24 hr) for 2 weeks; clients smoking fewer than 20 CPD were prescribed TTS20 for 6 weeks and TTS10 for 2 weeks. Following the first session, clients are encouraged, but not required, to attend every 1–2 weeks for a maximum of eight visits over 90 days. Participants receive nicotine patch prescriptions (a 1–2 week supply) only when attending the clinic. Support visits focus on managing withdrawal symptoms, coping with perceived barriers, and general motivational support.
Measures
At the first visit, clients provided demographic information, smoking history, and FTQ or FTND. Participants were asked to report the occurrence of tobacco withdrawal symptoms or side effects (yes or no) at each clinic visit. Clinic attendance, smoking status, and provision of nicotine patches were recorded at every contact.
Participants were contacted by telephone at 1 and 3 years after the first visit and three call attempts were made at the two time points. They were asked whether they had smoked at all over the past 7 days. Those who reported no smoking were classified as abstainers. Participants who reported being abstinent at both 1- and 3-year follow-up points were considered as achieving prolonged abstinence. Self-reports were not biochemically verified. Clients who did not provide follow-up data or were lost to follow-up were included as nonabstainers.
Statistical Analysis
Baseline characteristics of men and women were compared using independent t-tests for continuous variables and χ2 or Fisher’s exact test for categorical variables. Seven-day point prevalence abstinence rates at 1 and 3 years and prolonged abstinence rate were compared between genders using the χ2 test. We also perform univariate analyses for baseline variables to select variables that predicted abstinence at 1 year, 3 years, and both 1 and 3 years. All variables in which there were baseline differences between men and women, plus variables that predicted abstinence at 1 and 3 years in univariate analyses, were entered into a forward logistic regression analysis. Statistical analyses were performed using SPSS, Version 17.0.
Results
The sample comprised 940 men and 125 women. Table 1 shows their baseline characteristics. Female smokers were younger than males, smoked fewer CPD, and had lower educational status and better health status.
Sample Characteristics.
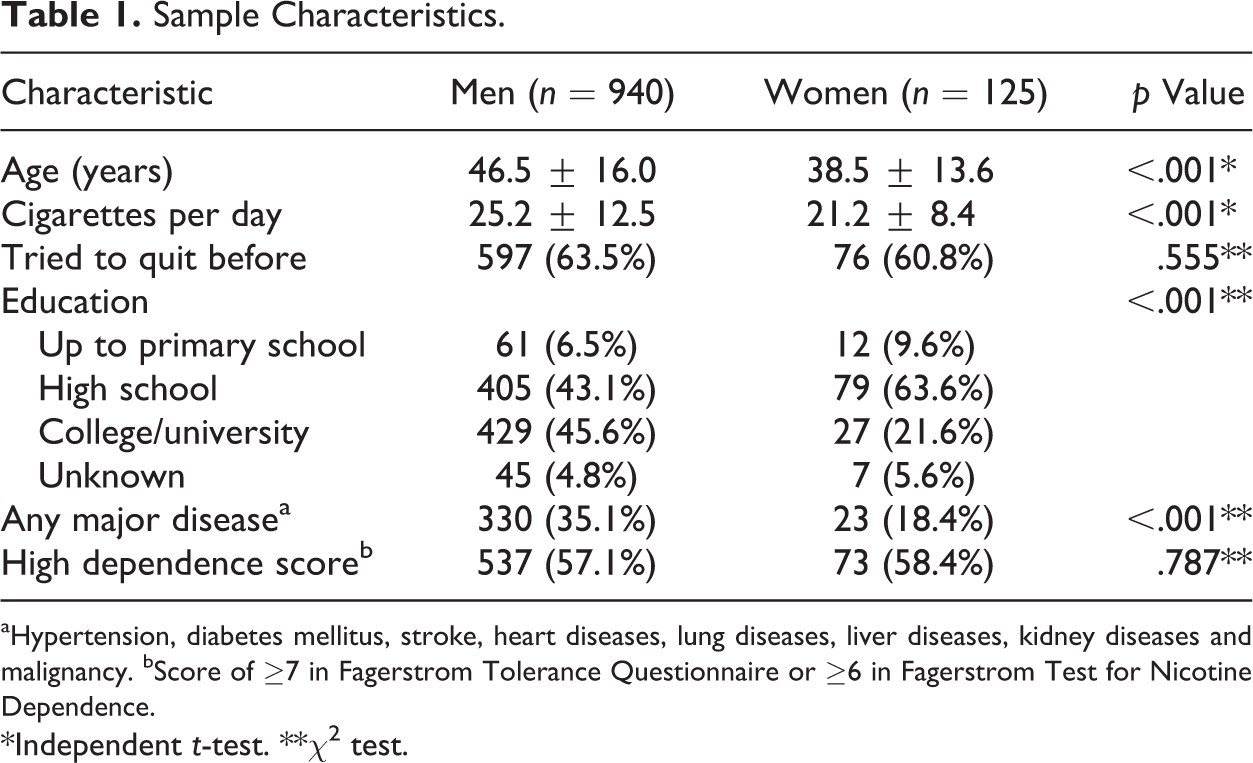
aHypertension, diabetes mellitus, stroke, heart diseases, lung diseases, liver diseases, kidney diseases and malignancy. bScore of ≥7 in Fagerstrom Tolerance Questionnaire or ≥6 in Fagerstrom Test for Nicotine Dependence.
*Independent t-test. **χ2 test.
The univariate analyses showed no gender difference in 7-day point prevalence abstinence rates at 1-year follow-up (men vs. women = 31.9% vs. 24.8%, p = .106), but women had significantly lower point prevalence (men vs. women = 29.8% vs.16.0%, p = .001) and prolonged abstinence rates (men vs. women = 20.1% vs. 11.2%, p = .017) at 3 years.
The following variables also predicted 7-day point prevalence abstinence at 1-year follow-up: lower cigarette consumption, making a previous quit attempt, and lower nicotine dependence (FTQ < 6 or FTND < 7). The predictors of 7-day point prevalence and prolonged abstinence at 3-year follow-up were gender, age, CPD, previous quit attempts, and nicotine dependence (Table 2).
Univariate Relationships Between Baseline Variables and Smoking Status at 1 and 3 Years.
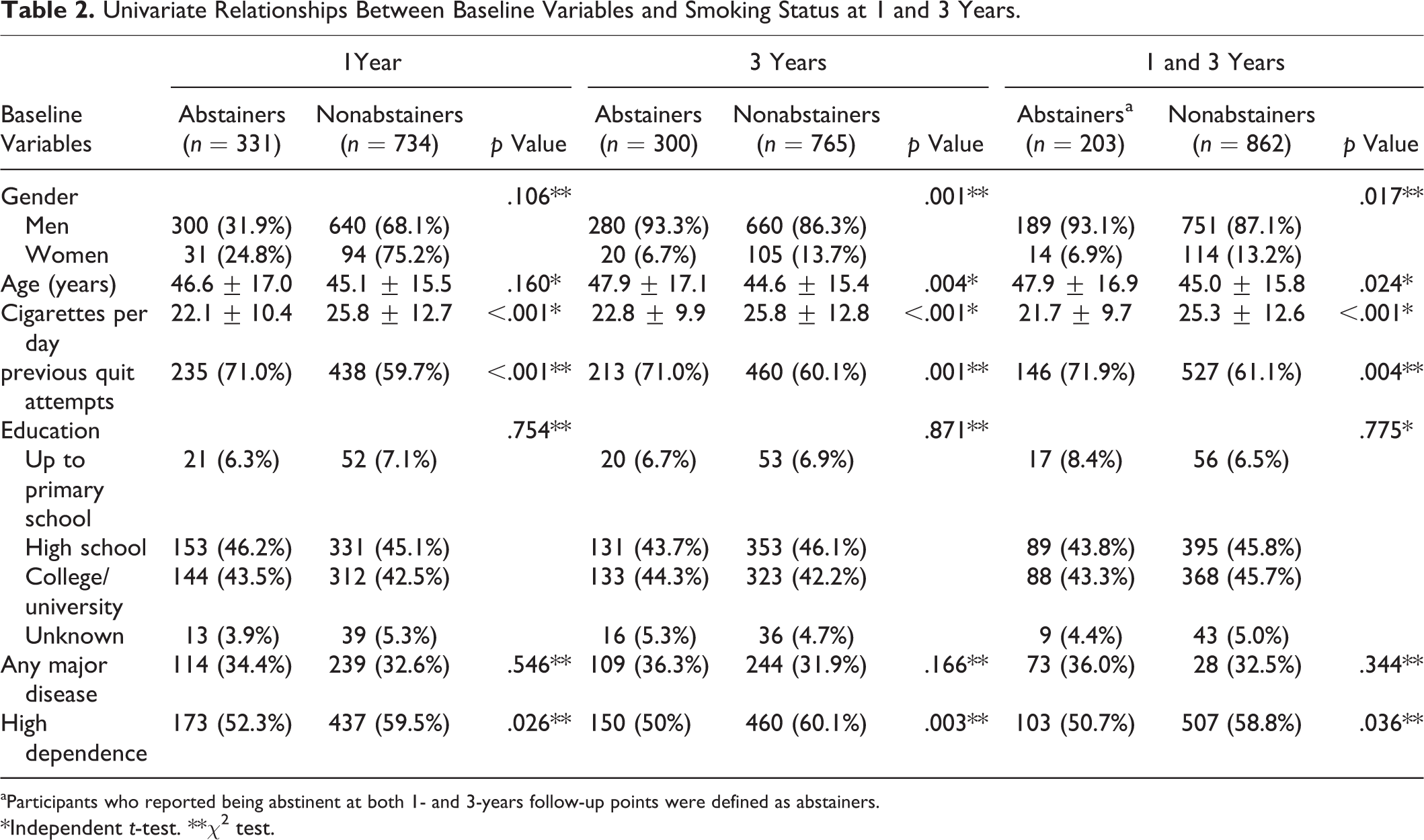
aParticipants who reported being abstinent at both 1- and 3-years follow-up points were defined as abstainers.
*Independent t-test. **χ2 test.
When these univariate predictors were entered into a logistic regression model with the baseline variables that differed significantly between genders (with or without any major disease history and education levels), gender was a significant predictor of smoking cessation at all three time points (Table 3). The total of 613 men and 66 women attended the clinic more than once and were included in the analysis of withdrawal symptoms and adverse effects. There were no gender differences in reports of insomnia, headache or dizziness, anxiety, difficulty concentrating, skin rash, itchy skin, and nausea. More women than men reported increased appetite (4.5% vs. 0.7%, p = .023).
Predictors of Abstinence in Multivariate Analyses.

Note. aOR = adjusted odds ratio; CI = confidence interval.
Discussion
In this sample of Taiwanese smokers who were seeking treatment, long-term abstinence rates were lower in women than in men. These gender differences remained even when we controlled for a range of other variables that were associated with long-term cessation outcomes.
In many Western countries, the prevalence of smoking among men and women is roughly similar (Birmpili et al., 2012; Croghan et al., 2009). In Taiwan, men have a much higher prevalence of smoking (39.0%) as compared to women (5.1%; Chang, Sung, Zhu, & Chiou, 2014). This difference is common in many other Asian countries such as China, Japan, and Malaysia (Ghani et al., 2012; Wang, Cho, Xiao, Wajsbrot, & Park, 2013). As such, smoking among men is seen as “normal,” while smoking among women is associated with a degree of social stigma (Ghani et al., 2012).
In the light of these social norms, female smokers may differ from male smokers on a number of characteristics. For example, female smokers may be more likely to have characteristics linked to “social deviance.” Indeed, the gender groups differed in most baseline characteristics we collected. Although we were able to control for these differences in the statistical analysis, there are likely to be many other ways in which male and female smokers differ which we did not record.
Given the lack of gender differences in smoking cessation outcomes in countries where the prevalence of smoking in men and women is similar, it is likely that our findings reflect different profiles of male and female smokers in Taiwan rather than any intrinsic hormonal or psychological gender differences. It is possible, for example, that female smokers may have felt more embarrassed, due to social stigma, than men to access treatment services and more likely to dropout. In most Asian countries, smoking among men is common and seen as normal, while smoking among women is rare, and so this condition may be not limited in Taiwan. In these countries, it may therefore be important to offer cessation programs that maintain some anonymity for smokers. Digital strategies, such as web or app-based tools or SMS text messaging, that can be accessed from the privacy of one’s own home may provide some possible solutions. Such interventions should include a combination of behavioral support and pharmacotherapy.
Along with the strengths of this study, which include a large sample size and a “real-world” setting, there are some limitations that must be considered. We were only able to measure self-reported abstinence, as follow-up was undertaken by telephone. This, combined with our 7-day point prevalence abstinence measure, is likely to have resulted in slightly inflated rates. This however was unlikely to affect gender differences. The results concern a clinical sample of smokers seeking help and may not generalize to the majority of smokers who do not attend stop-smoking treatment, but the proportion of men and women in our sample reflected well the Taiwanese population where 39% of men and 5.1% of women smoke (Chang et al., 2014).
In summary, among smokers who attend for specialist smoking cessation treatment in Taiwan, women have lower long-term quit rates than men. This may, in part, be due to women not being able to utilize the full benefit of stop smoking services and effort may need to be invested in finding more appropriate ways to help women quit in societies, where smoking in women is associated with significant social stigma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hayden McRobbie and Peter Hajek have provided consultancy to, and received research funding from, manufacturers of smoking cessation medications.
Funding
The author(s) disclosed receipt for the following financial support for the research, authorship, and publication of this article: This work was supported by the Kaohsiung Veteran General Hospital. The authors appreciate the colleagues in the Kaohsiung Veterans General Hospital. Kaohsiung Veteran General Hospital (Grant number VGHKS98-CT3-07 and VGHKS99-CT3-02).