
Abstract
Employment is fundamental to mental health recovery. The aim of this study is to construct a parsimonious profile indicating employment potential of people with major depressive disorder (MDD) to facilitate clinical assessment on employment participation. Data were drawn from Waves 1 (2001–2002) and 2 (2004–2005) of the National Epidemiologic Survey on Alcohol and Related Conditions. We included participants who had MDD at Wave 1 and were interviewed in both waves (N = 2,864). We conducted Classification and Regression Tree (CART) analysis to identify key characterizing factors of Wave 2 employment among 32 Wave 1 risk and protective factors. The results show that 82.1% of those employed at Wave 1 were likely to be employed at Wave 2. Among those unemployed at Wave 1, 51% of those motivated to work, measured by work-seeking behavior in the prior year, were likely to be employed at Wave 2. Among those unemployed and motivated to work, better functional mental health was associated with employment (>25.3 vs. ≤25.3). Results highlight the importance of motivation to work, shown in active work seeking, in facilitating employment despite clinical conditions.
Employment is fundamental to mental health recovery (Barber, 2012; Davidson & Roe, 2007; Jacobson & Greenley, 2001). Russinova, Wewiorski, Lyass, Rogers, and Massaro (2002) introduced the term “vocational recovery” to specifically address how persons with severe mental illness may have the capacity to achieve stable and meaningful participation in the competitive workforce. More specifically, studies of supported employment programs have found that employment is associated with improved psychiatric symptoms (Bond et al., 2001) as well as increases in psychosocial functioning (Eklund, Hansson, & Ahlqvist, 2004). Other studies have found that employment contributes to self-reported increased recovery, empowerment, self-esteem, personal growth, and a sense of purpose or usefulness (Auerbach & Richardson, 2005; Fossey & Harvey, 2010; Provencher, Gregg, Mead, & Mueser, 2002; Repper & Carter, 2011; Salzer & Shear, 2002; van Dongen, 1996).
Research has identified risk and facilitating factors that may influence the likelihood for persons with mental illness to obtain and retain employment. Studies suggest that clinical factors, such as psychiatric diagnosis, self-reported psychosocial functioning, and co-occurring medical conditions or disabilities, are negatively associated with obtaining competitive employment (Elinson, Houck, Marcus, & Pincus, 2004; Razzano et al., 2005), while recent work history, educational level, and younger age have significant positive association with obtaining competitive employment (Cook et al., 2008). Macias, DeCarlo, Wang, Frey, and Barreira (2001) found that both self-reported interest in work and receipt of vocational services significantly predicted obtaining competitive employment and the length of time needed to obtain employment.
In addition, research indicates that self-confidence and motivation to work, applicable work skills, person-job fit, and social and vocational support contribute to the likelihood of obtaining and retaining employment (Dunn, Wewiorski, & Rogers, 2008; Fossey & Harvey, 2010). Specific to depressive disorders, a recent review identified disorder-related indicators (severity and length), personal factors (age and previous history of breaks from employment), and types of work to be associated with work participation and work functioning in workers with depression (Lagerveld et al., 2010).
Despite research attesting to the impact vocational training and support programs have on work outcomes (Cook et al., 2008; Fossey & Harvey, 2010; Macias, DeCarlo, Wang, Frey, & Barreira, 2001), clinical judgment and mental health consumers’ self-assessment regarding the need for employment services do not always match (Casper & Carloni, 2006; Cook, 2006; Crane-Ross, Roth, & Lauber, 2000). Studies show that most consumers express the desire to work but receive less employment guidance from providers compared to guidance in other life domains (McQuilken et al., 2003). Clinical decisions on referrals to supported employment programs also tend to be influenced by consumers’ co-occurring substance abuse (Biegel, Beimers, Stevenson, Ronis, & Boyle, 2009; Frounfelker, Wilkniss, Bond, Devitt, & Drake, 2011), despite the explicit eligibility criteria set forth by Substance Abuse and Mental Health Services Administration for supported employment programs which include substance abusers (Substance Abuse and Mental Health Services Administration, 2009). However, the relationship between substance abuse and employment of persons with mental illness is inconclusive. While some studies suggest that substance abuse has a negative impact on employment outcomes (Lehman et al., 2002; Meisler, Blankertz, Santos, & McKay, 1997; Pickett-Schenk, Cook, Jonikas, & Banghart, 2004; Razzano et al., 2005), others have found limited contribution of substance abuse to functional impairment beyond impairments due to severe mental illness (Drebing et al., 2002) nor direct association between lifetime or current substance use and work participation (Bell, Greig, Gill, Whelanhan, & Bryson, 2002; Macias et al., 2001).
Although there are numerous benefits of work, the array of risk and facilitating factors related to employment and inconclusive findings on co-occurring substance abuse issues make it challenging for service providers to assess consumers’ potential for work and to facilitate employment participation. To inform clinical judgment on providing vocational intervention for persons with major depressive disorder (MDD), we purposefully take an exploratory approach and examine a variety of risk and facilitating factors associated with employment in a general population sample. In this study, we used the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), a nationally representative survey of all noninstitutionalized U.S. adult civilians (National Institute on Alcohol Abuse and Alcoholism [NIAAA], 2010). NESARC included a diagnostic interview that allowed for identification of MDD and co-occurring substance abuse issues as well as various factors associated with employment. We conducted Classification and Regression Tree (CART) analysis (Breiman, Friedman, Olshen, & Stone, 1984), a robust tree building statistical procedure that identifies key characterizing factors of a target outcome through data mining rather than testing predetermined hypotheses. CART has been applied to a range of health issues to aid clinical decision making, such as generating rules for nurse–patient assignments (Sundaramoorthi, Chen, Rosenberger, Kim, & Buckley-Behan, 2009), identifying characterizing factors of recurrent falling among community-dwelling seniors (Leclerc et al., 2009), and diagnosing chest pain (Cricheon, Hinde, & Marchini, 1997). With the application of CART, our study aims to identify the strongest baseline characterizing factors of the employment status 3 years later among persons with MDD.
Method
Sample
Data were drawn from Wave 1 (2001–2002) and Wave 2 (2004–2005) of NESARC. The NESARC overall response rate was 81%. Young adults aged 18–24 and Black and Hispanic individuals were oversampled. Data were weighted to reflect the demographic characteristics of the population based on the 2000 U.S. Census. The sample is comprised of NESARC participants who had MDD in the year prior to Wave 1 and who were interviewed 3 years later (N = 2,864). MDD was measured by using the NIAAA Alcohol Use Disorder and Associated Disabilities Interview Schedule–Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; AUDADIS-IV, Grant & Dawson, 2000). This study was exempted from human subjects review by a university’s Institutional Review Board.
Outcome Variable
The outcome measures were employed or unemployed at the time of Wave 2 surveys. Employment was defined as: (a) working full time or part time; (b) employed but not at work due to temporary illness, injury, or paid vacation; or (c) employed but absent from work without pay.
Risk and Protective Factors
Thirty-two factors of employment at Wave 1 were identified in the following domains. Demographic characteristics included sex, age (aggregated into four age-groups: 24 and younger, 25–44, 45–64, and 65 and older), and race/ethnicity (collapsed into White and non-White groups). Employment status at Wave 1 was measured in the same way as the outcome variable. Education was measured by the highest grade or year of school completed. Health insurance was a dichotomized measure of having none or any of the following types of insurance: Medicare, Medicaid, military healthcare, and private health insurance. Social support was measured by the number of related adults in the household. Marital status was collapsed into a dichotomized measure of married and living with someone as if married or not. Motivation to work was operationalized as work-seeking behavior currently and/or at any time in the prior year.
Past year medical and mental health conditions were measured by the following. Past year medical condition was a dichotomized measure of having none or any of the six types of diseases: arteriosclerosis, hypertension, liver diseases, heart diseases, gastrointestinal diseases, and arthritis. Past year substance abuse and dependence were measured with the AUDADIS-IV (Grant & Dawson, 2000). The AUDADIS-IV includes detailed assessment of DSM-IV abuse and dependence criteria for alcohol and 10 drug classes. Items were collapsed into alcohol, drug, and nicotine subcategories. Past year manic/hypomanic disorders and anxiety disorders were also measured by the AUDADIS-IV. The AUDADIS-IV includes four anxiety disorders: social phobia, specific phobia, generalized anxiety, and panic disorder, all of which were collapsed into a dichotomized measure of having none or any type of anxiety disorders. Psychosis was measured by a dichotomized response to whether there was schizophrenia or psychotic illness or episode in the past year. The number of major depression episodes and attempted suicide over life time was also identified.
Lifetime use of alcohol or drug intervention was a dichotomized measure of having none or any of 13 (for alcohol issues) or 14 (for drug issues) types of treatment and services, such as 12-step self-help, professional interventions, and employee assistance program. Similarly, lifetime use of treatment for MDD, manic/hypomanic disorders, and anxiety disorders were dichotomized measures of seeking none or any help from professionals, hospitals, emergency room, and prescribed medication for their disease. Finally, a dichotomized response to whether most recent episode of major depression was in remission in past year was also included in the analysis.
Functional health status was measured with the SF-12v2 health survey, which provides norm-based summary scores of physical health and mental health in the prior 4 weeks. There were 8 subscales, including physical functioning, bodily pain, general health perceptions, energy/vitality, social functioning, mental health, role functioning due to emotional problems, and role functioning due to physical problems (Ware, Kosinski, Turner-Bowker, & Gandek, 2002). In norm-based scoring, each scale had an average score of 50 and the standard deviation of 10. An individual respondent’s scale score below 45 indicated that his or her health status was below the average range ( User’s Manual, 2007).
Analysis
We used IBM® SPSS® Statistics 20 software for analysis. All estimates were weighted by the sampling weights to represent the U.S. population. Univariate analysis was conducted on the outcome variable and risk and protective factors. The 32 factors of employment were compared between Wave 2 employed and unemployed groups using chi-square tests or t-tests.
We then conducted CART analysis (Breiman et al., 1984) to identify key characterizing factors of employment. CART is a procedure to generate a binary tree-structured solution containing a subset of characterizing factors in accordance to their importance in indicating a given outcome. The procedure starts with the entire sample. All of the factors are investigated to identify a factor and its value that splits the sample into binary subgroups with best external heterogeneity and internal homogeneity. For each resulting subgroup, this procedure repeats until no further splitting is possible according to prespecified tree growing rules. We preset tree depth to 5 levels, subgroups to contain no fewer than 50 cases, and the Gini index to .0001 for determining factors’ importance in reducing impurity within subgroups. The tree was then pruned according to the risk <10 (standard error) to identify a simpler tree, balancing the additional tree accuracy and tree complexity that a split would generate.
Finally, we performed additional logistic regression models to verify a suppression effect that we identified in the results from the CART analysis. We conducted this analysis by following the procedures set forth by MacKinnon, Krull, and Lockwood (2000, p. 176).
Results
Table 1 shows the characteristics of the weighted sample. To highlight, at Wave 1, 59.9% were employed, and 19.6% were looking for work. The average scores of the functional health scales are between 41.2 and 48.1 with the average score of 42.5 (SD = 13.6) for role functioning due to emotional problems. At Wave 2, 59.6% were employed.
Sample Characteristics.

Note. Weighted sample N = 16,194.
Differences in the 32 factors between the employed and unemployed groups at Wave 2, using chi-square tests or t-tests, were all significant at p < .01 level (two sided/tailed), except the following: health insurance (p = .186), marital status (p = .442), work seeking (p = .170), past year drug abuse/dependence (p = .622), and past year manic/hypomanic disorders (p = .514).
The CART analysis showed that employment at Wave 1, work seeking as the measure of motivation to work, and the role emotional subscale of functional health status as measured by the SF-12v2, respectively, were the most important factors associated with future employment (Figure 1). A large majority of cases who were employed at Wave 1 (82.1%) were likely to be employed at Wave 2. Among those unemployed at Wave 1, more than half of those who were actively seeking work (51.1%) were likely to be employed at Wave 2. Among those who were unemployed and not seeking work at Wave 1, only 17.1% were likely to be employed at Wave 2. Among those who were unemployed and actively seeking work, better functional health status in the role–emotional subscale (i.e., disability in role functioning resulting from emotional problems such as depression or anxiety) was associated with employment (>25.3 vs. ≤ 25.3). These three characterizing factors accurately classified 80.4% of all cases according to their Wave 2 employment status, including 90.7% of those who were employed at Wave 2.
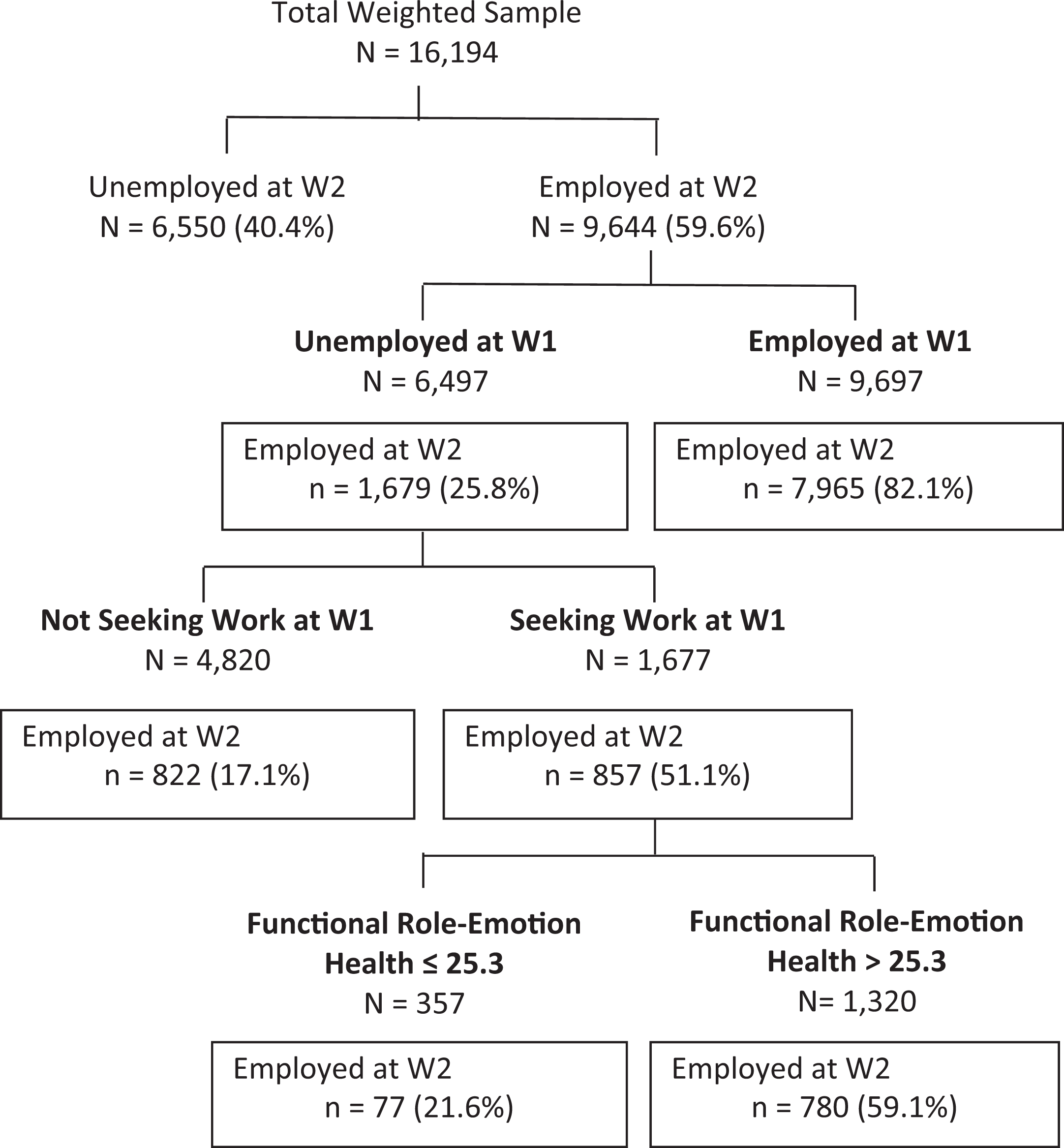
Classification and Regression Tree Model of Wave 2 employment in persons with major depressive disorder. Note. n (%) represents the weighted number of subjects employed at Wave 2 and its percentage in its respective category.
Although not a significantly associated factor in bivariate analysis, work seeking stood out as one of the strongest characterizing factors in CART analysis, known as the suppression effect (MacKinnon, Krull, & Lockwood, 2000). We examined the suppression effect by following the approaches proposed by MacKinnon and colleagues (2000, p. 176). As shown in Table 2, we found that in a simple logistic regression model where Wave 2 employment was regressed on Wave 1 work seeking, the coefficient of Wave 1 work seeking was −.055 (Model 1). In a multiple logistic regression model where Wave 2 employment was regressed on both Wave 1 work seeking and Wave 1 employment, the coefficient of Wave 1 work seeking became .467, while the coefficient of Wave 1 employment was 2.646 (Model 2). This result shows that after controlling for Wave 1 employment, Wave 1 work-seeking coefficient not only increased its magnitude in its absolute value but also showed its effect in the opposite direction (from negative to positive). That is, the effect of Wave 1 work seeking on Wave 2 employment was suppressed by Wave 1 employment.
Suppression of W1 Employment on the Effect of W1 Work Seeking on W2 Employment.

This result was verified by an alternative method also proposed by MacKinnon and colleagues (2000, p. 176). In a simple logistic regression model where Wave 1 employment was regressed on Wave 1 work seeking to identify the relation between the two, the coefficient of Wave 1 work seeking was −.649 (Model 3). The product of the coefficient of Wave 1 work seeking in Model 3 and the coefficient of Wave 1 employment in Model 2 (−1.717) has the opposite sign from the coefficient of Wave 1 work seeking in Model 2 (.467), showing the suppressor effect of Wave 1 employment. Additionally, the binary correlation between Wave 1 employment and Wave 1 work seeking was −.129 (p < .001), indicating a significant negative correlation.
Discussion
Wave 1 work history was found to be a significant characterizing factor of employment among persons with MDD. This finding is consistent with results of previous studies on employment among persons with a variety of mental health conditions (Anthony & Jansen, 1984; Burke-Miller et al., 2006; Campbell, Bond, Drake, McHugo, & Xie, 2010; Fossey & Harvey, 2010). Stability and duration of prior work are associated with future employment outcomes (Goldberg et al., 2001). In addition, Fossey and Harvey (2010) conclude from a review of qualitative studies that psychological effects of work history such as self-esteem and self-efficacy may influence future employment outcomes.
Another important finding is the association between work-seeking behavior and Wave 2 employment in persons with MDD. Our analysis on the suppression effect indicated that Wave 1 employment mediated/suppressed the effect of Wave 1 work seeking on Wave 2 employment in bivariate analysis, likely, because once people had work, they were not seeking work. This is supported by the binary correlation of –.129 (p < .001) between Wave 1 employment and Wave 1 work seeking. Because having work is most likely the result of seeking work, this finding shows that both seeking work and having work need to be considered to account for the potential of people who are motivated and in the process of seeking employment.
This finding has implications for future research on motivation to work. Prior research indicates that motivation to work is critical to obtaining and retaining employment (Auerbach & Richardson, 2005; Macias et al., 2001). Motivation to work might be expressed by desire to work and active work seeking. Both desire to work and active work seeking are consistent with a recovery-based approach to mental health services, as these factors underscore notions of consumer preference and empowerment, that is, gaining/regaining a sense of control and volition over life domains (Davidson & Roe, 2007; Jacobson & Greenly, 2001). However, emerging evidence suggests that active work seeking in persons with serious mental illness is associated with better employment outcomes, compared to a self-reported desire for employment (Alverson, Carpenter, & Drake, 2006). In their study, Alverson and colleagues found that all participants expressed a desire to find employment but only 15 of the 25 (60%) were “active work-seekers” (Alverson et al., 2006). They suggest that work-seeking behavior might be a better measure of motivation to work than expressed desire for work. Findings of a study by Macias and colleagues (2001) also suggest behavioral exposure to work, such as participation in supported employment services and work, is a stronger indicator than initial stated interest in work, in retaining employment. Our study adopted work seeking as behavioral manifestation of work motivation and again showed its significance in Wave 2 employment status.
The finding on the importance of functional role-emotion health status on employment outcomes echoes previous research. Perceived better health and functional (social, cognitive, and physical) characteristics are strongly associated with working status (Elinson et al., 2004). MDD is associated with pervasive and chronic psychosocial disability in day-to-day functioning. However, the severity of depressive symptoms varies over a long-term course, and when it decreases, psychosocial disability decreases as well (Judd et al., 2000). Our finding of the SF-12v2 role-emotion health associated with employment similarly suggests that functional mental health, rather than the clinical diagnosis of MDD, may more accurately reflect the potential of employment participation during the course of MDD, even when the score was much lower than the average of the scale (25.3 and 50, respectively).
The application of the CART procedure allows associated factors to emerge according to their relative importance to the target outcome (i.e., employment status). The top three factors—Wave 1 work history, work seeking, and functional role-emotion health—which emerged from the epidemiological data set are all strength-based factors. Clinical conditions, including substance use disorders, were also included in the analysis but none emerged as the most important factors in characterizing people with employment at Wave 2 in our analysis. This is consistent with an earlier review in which little or no correlation was found between symptomatology and functional skills (Anthony & Jansen, 1984) and with mental health consumers’ personal accounts of factors influencing their entry/reentry into the workforce (Dunn et al., 2008; Fossey & Harvey, 2010). Additionally, the supported employment literature provides little empirical support for excluding consumers from vocational services based on psychiatric history, diagnosis, or clinical work readiness (Bond, 2004). Our findings are consistent with research showing that substance abuse has limited (Drebing et al., 2002) to no direct impact on work outcomes among persons with mental health conditions (Bell et al., 2002; Macias et al., 2001).
The results of this study have multilevel implications. At the practice level, our findings suggest the absence of clinical conditions not be the sole determinant of consumers’ qualification for vocational services. Instead, service providers need to assess consumers’ strengths for vocational development (Anthony & Jansen, 1984). This aligns with defining rehabilitation readiness as one’s willingness to engage in the process of rehabilitation toward the accomplishment of a goal (Farkas, Sullivan Soydan, & Gagne, 2000). Service providers thus focus on assessing consumers’ perceived need for change; commitment to change; self-awareness of skills, interests, values, and preferences related to a desire role; awareness of options and demands; and willingness to establish therapeutic alliance for providing vocational services (Roberts & Pratt, 2007).
Moreover, for programming and service provision, we recommend vocational services made available to any consumer with a stated interest in employment or engagement in active job seeking, regardless of their type or severity of clinical condition. As previously discussed, work history has a significant influence on future employment. We thus argue for the importance of appropriate vocational services that provide exposure to work opportunities to consumers with limited work histories. Particularly, supportive, consumer-centered approaches can address issues that undermine both work motivation and actual work performance (Kirsh, Cockburn, & Gewurtz, 2005; Krupa, 2011). An example of such an approach is the standardized individual placement and support (IPS) model which considers consumers’ desire to work, includes rapid job placement, ongoing vocational assessment and supports, integrated vocational and mental health services, and targets competitive employment as the desired outcome (Becker & Drake, 1994; Bond, Drake, & Becker, 2008). The extensive evidence supporting IPS demonstrates that the holistic, consumer-centered programming leads to higher rates of competitive employment and longer job retention than other vocational rehabilitation models. These outcomes have been demonstrated across clinical diagnoses, including depressive disorders and schizophrenia (Bond et al., 2001, 2008).
On a policy level, our findings suggest that the scope of vocational services should be broadened to consumers who, based on their clinical conditions, may not have been previously assessed as strong candidates for vocational recovery. Many mental health consumers express interest in work, yet national surveys suggest only about one half of those with a serious mental illness (including MDD), are working at any given time (Elinson et al., 2004; Mechanic, Bilder, & McAlpine, 2002). Cook (2006) notes that the small scope of effort is a fundamental policy problem in vocational rehabilitation; mental health programming only involves limited vocational training and support. Models such as IPS could be integrated into mental health services, giving more consumers the option to work. Additionally, policy-based barriers to employment—such as stringent income eligibility requirements for Social Security Disability Insurance and Medicaid —should be overcome in both vocational rehabilitation and integrated models of care (O’Day & Killeen, 2002). Cook (2006) suggests that offering benefits planning and financial education to address consumers’ concerns about the effects of paid employment on cash and medical benefits does not affect their motivation to work.
For future studies, we support greater focus on the strengths-based research approach, which seeks to identify and enhance the inherent strengths of mental health consumers as well as to mobilize assets in their larger social environment (Maton et al., 2004). For persons with MDD, this involves extending the scope of investigations from a focus on pathology to a focus on personal and community characteristics that may foster greater vocational participation. Additionally, exploratory studies that allow understudied factors of vocational participation to emerge hold promise in expanding research, practices, and programming for improving vocational recovery of persons with MDD and other mental health conditions.
Our study has several limitations. First, employment in the NESARC was measured at only two time points. Future longitudinal studies that measure employment at multiple time points are needed to better capture employment trajectories of persons with MDD. Second, work-seeking behavior was measured by a single dichotomized item. Future research using more sophisticated measurement is needed to confirm our findings. Third, the timeframes for MDD and functional health status measurements did not overlap (past year and past month, respectively), thus their association was uncertain. Fourth, the survey relied on self-report. However, studies have shown good consistency between respondents’ and collateral reports of substance use (Connors & Maisto, 2003; Hjorthøj, Hjorthøj, & Nordendoft, 2012). Finally, unlike a conventional regression model, CART does not provide confidence intervals and thus precludes assessment of the reliability of an estimate.
Despite these limitations, the study has the strength of a prospective design and a large and nationally representative sample which supports the generalizability of the results. The use of CART analysis resulted in a parsimonious profile of factors indicating the employment potential of persons with MDD. The relative importance of the characterizing factors highlighted the significance of motivation to work manifested as active work-seeking behavior in facilitating employment. Remission of clinical conditions need not be a pre-condition to support vocational development of consumers with MDD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.