
Abstract
Increasingly, health care is being delivered in large, complex organizations, and physicians must learn to function effectively in them. As a result, several medical and business schools have developed joint programs to train physician leaders who receive both medical degree (MD) and master of business administration (MBA) degrees. We examined several themes in relation to these programs, revolving around concerns about who is attracted to them and whether exposure to the differing cultures of medicine and business have an impact on the professional identities of their graduates as manifested in their motivations, aspirations, and careers. We addressed these issues by studying students in the joint MD/MBA program at Harvard Medical School (HMS) and Harvard Business School (HBS). Our data came from several internal sources and a survey of all students enrolled in the joint program in spring 2013. We found relatively few differences between joint program students and equivalent cohorts of HMS students in terms of personal characteristics, preadmission performance, and performance at HMS and HBS. Contrary to the concerns that such programs may draw students away from medicine, the vast majority embraced careers involving extensive postgraduate medical training, with long-term plans that leveraged their new perspectives and skills to improve health care delivery.
As the delivery of health care becomes increasingly complex, organizations and systems that provide care have come to recognize the need for leaders with perspectives that go well beyond the field of medicine itself (Ackerly et al., 2011; Gunderman & Kanter, 2009). One response to this trend, more common in North America than other parts of the world, has been the development of programs in which medical students receive their medical degree (MD) as well as a master of business administration (MBA) referred to as MD/MBA programs (Lazarus, 2010; Sherrill, 2000). The number of MD/MBA programs in the United States rose from 6 in 1993 to 33 in 2001; and by 2010, programs of this sort existed in more than 40% of the U.S. medical schools (Butcher, 2011; Goyal et al., 2015; Larson, Chandler, & Foreman, 2003).
Rather than simply receiving medical and business training in parallel pathways, many of these are “joint programs” in which a coordinated curriculum is designed by the faculty in a university’s medical and business schools. The most common model is for dual degree students first to spend a block of dedicated time pursuing the regular MD curriculum during which time their curriculum is focused on the acquisition of basic science information, then to follow with a comparable block of MBA classes, such as those on finance, marketing, and strategy. Thereafter, the remainder of the time is spent integrating requirements for the two degrees.
Although some variability exists across the goals and objectives of such programs, a core aspect of their mission, as stated by one such program, is “to develop outstanding physician leaders, skilled in both medicine and management, to take positions of influence in which they will contribute substantially to the health and well-being of individuals and society” (Harvard Business School [HBS], 2015). By complementing students’ medical knowledge and skills with management perspectives and organizational leadership competencies, graduates of such joint programs satisfy the requirements for graduation with both degrees and have the potential to be employed in a wide range of capacities.
Like any area of rapid growth, questions have arisen about MD/MBA programs that coalesce around three conceptual themes. The first theme is defined by matters of potentially conflicting orientations and values in the educational philosophies espoused, explicitly and implicitly, in business and medicine. Although contemporary expectations in health care are evolving from individual to team accountability, medical education has focused traditionally on encouraging self-reliance and self-determination; physicians must make rapid decisions on their own and stand individually accountable for their consequences. Although accountability is important in business education as well, the management and leadership styles that permeate business education focus on team building, collaboration, and consensual decision making. The question is whether individuals who thrive in one atmosphere can also thrive in the other?
A second theme addresses the question of the differing interpersonal orientations and motivations at the heart of medical and business training and the extent to which the professional identities of MD/MBA graduates are affected by one or the other. In medicine, altruism and empathy are centrally defining values; physicians are taught that all of their activities must center on the key consideration of the good of the patient. In contrast, in the culture of business, considerations such as profit and competitive advantage are emphasized. Traditionally, these have been unwelcome in medicine and are seen as inconsistent with the core mission of the physician. Considering the impact of business training on the professional identities of MD/MBA students, medical educators have raised the issue of the “traitor complex,” a concern that students who graduate from such programs may become bureaucrats rather than healers, business people who are interested in protecting the organizational bottom line rather than the best interests of patients (Chen, 2006; Kuo, 1997; Sherrill, 2005).
Rather than focusing on the impact of MD/MBA training, a third theme has been raised about the attributes of those who are oriented toward obtaining the joint degrees. Could students who are attracted to such programs be atypical of their peers, whether in their values and motivations or their academic capabilities (Sherrill, 2000, 2001). As an example, some question whether students who enroll in MD/MBA programs might be the most academically talented in their respective classes, implying that these programs are skimming the “best and brightest” students and turning their heads from medicine to business. Conversely, others have speculated that such programs may serve as a safety net for less academically accomplished students, raising the concern that the very people who may be determining the administrative policies and practices of modern medicine are those with lower levels of academic prowess or performance
While substantial speculation exists on these matters, the “data” supporting these various positions have been more at the level of opinion and anecdote, with just a few notable, although small-scale, exceptions. For instance, in a recent paper, Patel et al. (2014) described the career paths and perspectives of 30 years of graduates from the Wharton Health Care Management Program, the oldest program in the United States offering joint MD and MBA training. They found that many of their graduates were not involved in clinical practice careers. In contrast, data presented by Goyal et al. (2015) and Goldman and Wallace (2010) indicate that the great preponderance of students who graduate with both MD and MBA degrees remain in some form of medically related practice.
In the light of these themes and the paucity of solid evidence to address them, we sought to provide answers to several questions: Do any demographic or prior performance differences exist between students in the joint program and the rest of their medical school classmates? Do the two groups demonstrate similar or different levels of academic performance in their medical school and business school curricula? What is the nature of the self-descriptions (i.e., professional identities) of students in the joint program? What career paths do students in the joint program aspire to and pursue?
Our data derive from several different sources associated with the joint MD/MBA program established in 2005 at Harvard Medical School (HMS) HBS. Interested medical students apply for entry into this joint degree program during their second year of medical school. After completing their third year at HMS, during which time accepted students take additional management-related requirements, students spend their fourth year entirely at HBS. During their fifth year, students complete remaining requirements for both degrees, dividing their time between the two schools. Joint program students graduate 5 years after their matriculation at HMS, with the MD degree from HMS and the MBA degree from HBS. If the two degrees were to be pursued independently, students would spend 6 years to complete them, 4 years at HMS and 2 years at HBS. Between 10 and 14 students are admitted annually, and as of June 2014, a total of 67 students had completed the joint degree program.
Method
The data for this paper come from several different sources: (1) the HMS Student Assessment Database, (2) the HMS Financial Aid Office, (3) the HMS Office of Student Affairs, (4) the HBS Registrar’s Office, and (5) an anonymous survey of all students enrolled in the joint MD/MBA program during the academic year 2012–2013. The HMS Student Assessment Database contains relevant records from the Office of Admissions and the Registrar’s Office, including demographic information, Medical College Admission Test (MCAT) scores, undergraduate college and major, college grade point average (GPA), U.S. Medical Licensing Examination (USMLE) Step I and Step II Clinical Knowledge (CK) scores. Selectivity of college was coded according to the classification system used by the Princeton Review (2012). This database also contains measures of academic performance such as clinical clerkship grades and number of times students have scored in the bottom quartile on major first-year course examinations (which has been found internally to be predictive of performance during the HMS core clinical year).
Data from the Financial Aid Office include comparisons of the financial aid status of all HMS students versus students in the joint program. For the joint program students, data from the HBS Registrar’s Office included all MBA program grades, reflecting performance in both the required and the elective curricula of HBS (calculated based on credit hour, not per course). Because the data came from so many different sources at two different Harvard schools, the graduating classes for whom data were available varied, and therefore the numbers upon which various comparisons were made differ; the cohorts considered are noted in each analysis. Most important, however, all comparisons of MD/MBA students to non-MD/MBA students were made between students in the same cohorts, thereby avoiding any confounding effects of comparing a given set of MD/MBA cohorts to noncomparable cohorts of HMS-only students.
The student survey, which was conducted in the spring of 2013, was sent electronically via SurveyMonkey to all 34 students enrolled in the joint program at that time. Designed in consultation with the leadership of the joint program, the survey included questions that were written specifically to address students’ professional identities as well as their career intentions and aspirations. These included open-ended questions about students’ reasons for entering the joint program, their future professional plans at three points in time (upon graduation, 5 years of postgraduation, and 10 years of postgraduation), and their ultimate career position/title. In addition, students were asked to describe themselves as a future professional by selecting one of four choices beginning with the stem “I see myself as ….” The alternatives were: “a physician with invaluable training that gives me skills and insights into management perspectives and practices,” “a professional manager of a health care organization with a background and training as a physician,” “a member or leader in the health care arm of a consulting firm,” and “an entrepreneur in the arena of health care or health care management.”
A fifth option was also available: “None of the above; a better description of myself in the future would be …” with an option to provide a free-text answer. The survey was reviewed by the HMS institutional review board and determined to be exempt.
The open-ended data were coded independently by two of the authors (E.K. and S.N.F.). Using the conventional approach guidelines proposed by Hsieh and Shannon (2005), we allowed themes to emerge upon the reading of the open-ended responses rather than beginning with preconceived categories into which the definitions should be placed. In a first round of coding, we reconciled any differences in categories to be used; and upon reaching consensus, the coders continued independently. The vast majority of codes assigned to the responses were identical, and, in the few instances of disagreement, agreement was reached after brief discussion. For the quantitative data, we compared joint program students to students in the same medical school cohorts who were not in the joint program by applying independent t-tests, chi-square, and Mann–Whitney U tests, as appropriate.
Results
Characteristics of the Students
Table 1 compares students in the joint program and students in the equivalent years at HMS not in the joint program on seven unique characteristics. Data on gender and minority status were available for six consecutive cohorts of students (graduating classes of 2008–2013), whereas, for the other variables in the table, comparative data were available only for the classes of 2008–2011. We found no strong or consistent patterns of difference between joint program students and the larger medical school cohorts from which they came. The two groups were not significantly different in ethnicity (based on Underrepresented in Medicine status) or major (comparing those in science, technology, engineering, and math fields vs. those in the humanities and social sciences). Data from the Financial Aid office indicate that of all the active MD/MBA students in the years 2008–2013, 62% (18 of 29) were on scholarship, which is comparable to the 59% (378 of 641) of MD students on scholarship who were not members of the joint program. Joint program students were more likely to be male (p < .001), and a higher percentage (94% vs. 73%) came from the most selective undergraduate colleges and universities (p = .01). Concerning premedical performance, total MCAT scores were not different between groups; however, the mean undergraduate GPA of the joint program students was slightly but significantly lower (3.78 vs. 3.85, respectively, p < .01).
Comparison of Characteristics of All Students Enrolled in the HMS New Pathway and All Students Enrolled in the Joint MD/MBA Program in the Same Years.
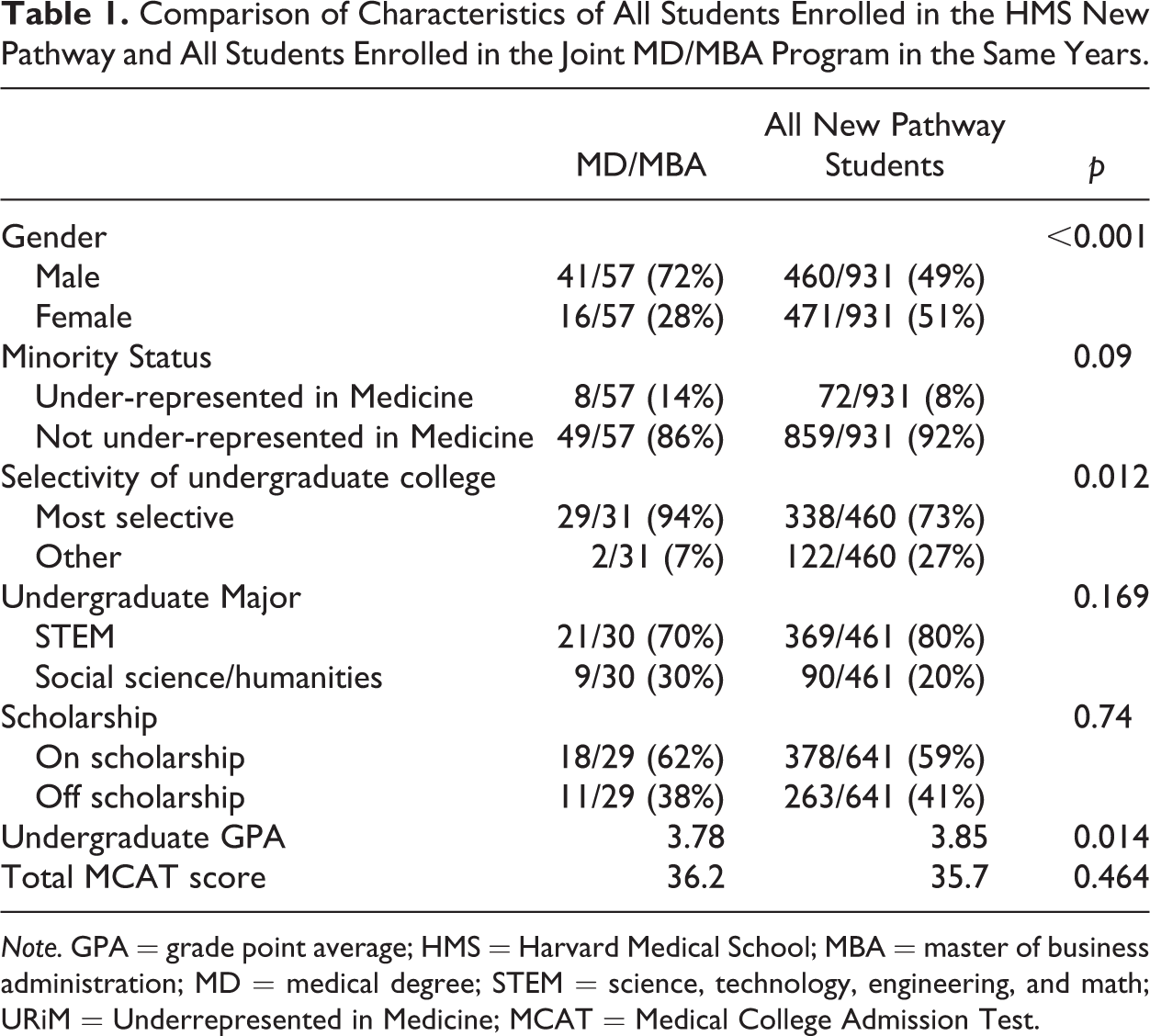
Note. GPA = grade point average; HMS = Harvard Medical School; MBA = master of business administration; MD = medical degree; STEM = science, technology, engineering, and math; URiM = Underrepresented in Medicine; MCAT = Medical College Admission Test.
Academic Performance in Medical and Business School
Performance on national and local exams was comparable between joint program students and their nonjoint program peers. For the graduating classes of 2008–2013, mean scores on USMLE Step I were not significantly different (237.14 vs. 234.30, respectively) nor were Step II CK scores (238.27 vs. 241.77, respectively). At HMS, data on students falling into the bottom quartile on three or more first-year major exams were available for three cohorts, 2008–2011; 24% (7 of 29) of those in the joint program met this bottom-quartile criterion compared to 19% (61 of 315) of those in the larger cohort, a difference that was not significantly different.
The clinical performance of the two groups of students was also similar, based on data from the graduating classes of 2008–2012. Converting the four levels of HMS core–clinical–clerkship grades to numerical equivalents (4 for the highest; 1 for the lowest, as is done in calculating a Grade Point Average (GPA)), we found that mean clinical grades across the seven core clerkships for joint program and for HMS-only students (3.56 vs. 3.44, respectively) were not different. On the HMS Comprehensive Exam (a nine-station objective structured clinical examination taken at the end of Year 3 after completion of all core clinical clerkships), total scores were also statistically equivalent (66.90 vs. 64.51, respectively).
The fact that joint program students took their required and elective HBS courses with the rest of the HBS students allowed us to compare the performance of joint program students with that of the other HBS students in their business-related courses. In both the first-year required curriculum and the second-year elective curriculum at HBS, grades for each course are distributed strictly according to a prescribed set of ranges. In the HBS required curriculum, the highest grade, designated as Category I, is given to 15–20% of all students enrolled in a given course. The lowest grades, Categories III and IV, are assigned to exactly the bottom 10% of all students in the course (with no faculty discretion as to percentage). All other students receive Category II.
Analysis of the data from the 67 joint program students who had completed required curriculum courses at HBS, from the program’s first class through 2014, indicated that 18% of the credit-hour grades (408 of 223) awarded to joint program students were Category I, directly in the middle of the prescribed (15–20%) range for all students in required courses, and 8.5% (189 of 223) were at Level III, just below the 10% prescribed range. In the elective curriculum, 15–25% of all students in a given course are awarded Category I grades, and 10% receive Level III grades. For the 57 joint program students who had taken elective curriculum courses through 2013, 26% (248 of 947) of all the credit-hour grades awarded were Category I, just slightly above the high end of the prescribed range, and 7.5% (71/947) were at Level III, slightly below the prescribed range.
Self as Professional
The professional identity data came from the student survey, for which the response rate was 83%. Although response rates differed slightly by students’ year in the program, the rate was acceptable for each of the 3 years: 82% (9 of 11) in the third year; 100% (13 of 13) in the fourth year; and 60% (6 of 10) in the fifth year.
When students were presented with the open-ended question about why they chose to enter the Joint MD/MBA Program, 26 students provided codable responses, and these were categorized as falling primarily into one of two main themes, split equally (13 each). The first was more self-focused and included mentions of a good fit with personal interests and goals (“interested in hospital management and enjoy managing and working with other people;” “felt it played to my skills and interests.”). The second theme focused on making an impact and contributing to the improvement in health care and the health care system. Doing so would be achieved in some cases by gaining new knowledge, skills, perspectives, and credentials while in other cases by bridging the perspectives of business and medicine: I hope to work on improving health care delivery throughout my career, and I feel that the MD/MBA will give the optimal toolkit for making an impact in this area. So that I could sit at the table when decisions about the way I would practice medicine and serve my patients … were being made and bring my experience, insights, and ingenuity to bear in the design of health systems.
Sixteen students provided answers to the open-ended question, “In what ways has your image of yourself as a professional changed?” Among the answers, three broad themes emerged. The most common, mentioned by eight students, was a reflection of professional growth, especially in terms of broader awareness of issues and perspectives, and heightened confidence in oneself: More confident in my views on business of healthcare. More driven to research and criticize current healthcare systems. More confident I can have an impact. Greater confidence in my ability to make and follow through on decisions, to devise solutions, to fail and learn from failing; a greater sense of ambition: If I don’t speak up, someone else will, and I’ll have no one to blame but myself if I don’t like the results …. Meeting students who were working hard to launch new companies and technologies made me realize that I should take more risks. Specifically, I should venture outside of a strictly academic career to accomplish my goals of trying to push technologies outside of the laboratory setting.
A third theme, one that was not anticipated, was mentioned by three students and referred to the reinforcement of their self-image as a physician: Being away from medicine and among former business professionals [i.e., other MBA students] taught me that I could never leave medicine. Going to business school solidified my image of myself as first and foremost a physician.
The students’ responses to the open-ended questions mentioned earlier were consistent with their selections when asked to choose which of four statements “best describes your image of yourself as a future professional.” The majority of students (15 of 28; 54%) chose the option “I see myself as a physician with invaluable training that gives me insights into management perspectives and practices”; 35% (10) chose “I see myself a professional manager of a health care organization with a background and training as a physician”; 12% (3) selected “I see myself as an entrepreneur in the arena of health care or health care management”; and no students chose “I see myself as a member or leader in the health care arm of a consulting firm” or “none of the above.”
Plans, Aspirations, and Career Directions
Finally, students were asked what their plans were immediately after graduation from medical school, then 5 and 10 years later as well as to list their ultimate career position or job title. The results for postgraduation plans were clear and simple. Without exception, all students indicated their intentions of beginning internship and residency. At 5 years, 54% (15 of 28 respondents) anticipated that they would still be in training, either completing residency or in a fellowship program. The other 46% (13) imagined themselves in clinical practice, some with additional administrative, quality improvement or entrepreneurial roles. At 10 years, 64% (18 of 28) of the students mentioned a combination of clinical practice and some additional administrative or leadership roles. Of these students, three imagined themselves having a leadership role in an academic department, four saw themselves as involved in special projects such as quality improvement in addition to their clinical roles, and another four expressed that in addition to their clinical roles they intended to be engaged in business, industry, or entrepreneurship. Concerning ultimate goals, the two most common designations were chief executive officer or chief medical officer (of a hospital or hospital network, provider organization, or a health care technology company), stated by 11 respondents, and chair or chief of a department at an academic medical center or hospital, by four. Two students listed Surgeon General as their ultimate position, and one indicated several options including Head of the World Health Organization or Minister of Health.
Data on postgraduation training were available from HMS records for all 67 joint program graduates, from the first in 2008 through the graduating class of 2014. Of the 67, 63 (94%) entered a residency program, 60 with their graduating class and 3 within an additional 1 to 2 years after graduation. Over the same period, 96% (1062 of 1104) of all HMS graduating students entered a residency with their graduating class.
Of the MD/MBA graduates who entered a residency, 34% (22 of 64) chose medicine and 34% (22) chose a surgical subspecialty. Nine percent (6) chose emergency medicine, 6% (4) chose dermatology, 8% (5) chose radiology, and 6% (one each) chose pediatrics, psychiatry, anesthesia, and radiation oncology. During the same time period, 26% (292 of 1108) of the entire graduating class entered a medical residency and 18% (194 of 1108) entered a surgical specialty residency.
Discussion
The merger of medical and business training is a relatively new phenomenon about which we are still learning. In this study, we explored data about the students who opted to pursue the HMS-HBS joint MD/MBA program to provide an evidence base to address several questions the answers to which, previously, had been heavy on speculation and conjecture but light on data. We sought to determine whether students who choose to pursue the joint MD/MBA degrees are different from other medical students in meaningful and measurable ways and to shed light on the extent to which exposure to a different educational environment has an impact on the professional identities, aspirations, and pursuits of those in this program.
With few exceptions, students in the joint program and their nonbusiness school peers were similar on most relevant demographic and prior performance characteristics. In contrast to the MD-only program, whose gender distribution is approximately half male and half female, joint program students were more likely to be male, 72%, than female, 28%. This enrollment pattern is a reflection of the gender distribution of HMS students applying to the joint MD–MBA program (over 6 years, a mean of 76% of the applicants were male and 24% were female, with a range of 70–88% male; 12–36% female) and is consistent with a general overrepresentation of males in MBA programs across the United States (Schulte, 2015). Concerning their level of achievement prior to entering medical school, a larger percentage of the joint program students came from the most highly selective colleges, and their college GPAs were slightly lower. These differences, while significant, were relatively small and reflect the fact that the vast majority of students in both groups came from the most selective schools and had extremely high GPAs.
Once in medical school, students in the two groups had comparable academic performance in their medical program, as measured by course and clerkship performance and USMLE scores. In HBS as well, their grades were generally comparable to those of their business school peers. In short, we found little evidence suggesting that medical students opting for training in business as well as medicine are measurably different in their characteristics or performance (neither better nor worse) compared to their medical school and business school peers.
An expressed concern about joint MD/MBA programs is that the process of obtaining the MBA degree may lead young physicians to become so engaged in management and business that they would forsake their identities as doctors. Although it is possible that our students’ intentions may not match their actual long-term career trajectories, all of the self-descriptive and aspirational data they have provided from the survey indicate that they see themselves primarily as physicians.
Historically, a very small percentage of the program’s graduates did not actually go into residency (by choice, not by failure to match). Moreover, the overall profile of residencies they intended to pursue was typical of that of their fellow students, except for an emerging trend towards surgical subspecialties, which typically require long and intensive advanced training, indicative of the students’ extended commitment to medicine.
As noted, this pattern of commitment to medicine is consistent with the data of Goldman and Wallace (2010) who reported on the postgraduation career directions of MD/MBA graduates. Our findings and Goldman and Wallace’s findings, however, are somewhat contradictory to the findings of Patel et al. (2014) who studied MD graduates of the University of Pennsylvania (UP) who also received degrees from the UP’s Wharton School of Business. Patel and colleagues noted that recent Wharton graduates were less likely to enter into residency programs than earlier graduates and that the greater the number of years since their MBA graduation, the more their former students were likely to have moved out of medicine as their primary work sector. The interpretation of their findings, however, is confounded by two characteristics of their sample. First, not all of the physicians they studied were enrolled in a simultaneous joint MD/MBA degree program. Second, the majority (51%) of the graduates they surveyed received their MBA degrees after completing their MD, suggesting the possibility that at least some of the MBA graduates they studied may have chosen to pursue an MBA based on a preexisting interest in making a career path change.
Our study has several limitations. First, the findings we report derive from a relatively small sample of students and graduates of a joint program from the medical and business schools of one university with a unique identity and reputation. Second, the aspirations of these students may be affected by a number of factors as they complete their medical training, many of which are difficult to anticipate or capture. Third, disentangling the impact of causative factors is not possible; therefore, we cannot identify with certainty the extent to which our findings reflect students’ preexisting interests, attitudes, and aspirations as opposed to the impact of their medical and business training.
While acknowledging that we cannot be certain that our findings would generalize to other schools and other programs, we believe that they might inform faculty (at any school or university) who would care to design a joint medical business curriculum that broadens their students’ skills, perspectives, and career options while maintaining their commitment to medicine and high-quality care.
In proposing the central law of improvement, Berwick (1996) has stated that “every system is perfectly designed to achieve the results it achieves” (p. 619). We suggest that as much as these findings may be the product of a specific institution, they are very much the product of intentional design, and therefore informative to other institutions with similar goals. In order to keep their medical students from forsaking their identities as physicians, programs offering medical students training in business and leadership might consider following several guidelines, enumerated below, that were built into the Harvard MD/MBA joint program.
First, the goals and objectives of the program need to be articulated clearly, and applicants should be screened carefully to ensure that those admitted hold values that are congruent with the program’s mission. Students with ambitions to pursue other kinds of careers outside clinical medicine should be discouraged from applying. Second, faculty leaders in both business and medicine need to reinforce the strong expectation that students would enter and complete clinical residency after graduation with the MD and MBA degrees. Third, restricting applications until after the first full year of the MD program may also contribute to capturing academically accomplished students whose expectations from the joint program align with the program mission. This policy ensures that potential applicants are well known to the faculty who can then counsel them on the advisability of pursuing the joint degree program. Finally, in terms of curriculum, instead of relying on two parallel but unconnected degree programs, designers of joint degree programs would be well advised to create an integrative experience, and opportunities for class work and project work should be taught and mentored jointly by medical school and business school faculty.
Conclusion
Graduates of schools of medicine can choose from an increasingly broad array of career settings and roles. In all of these potential careers, the future success of health care will depend in large part on whether physicians are able to function effectively as part of increasingly large and complex organizations. Possessing the competencies developed as part of an MBA are likely to expand the range of careers and positions for which physicians can qualify and enhance their performance in any of these roles.
We learned from this study that the attributes and performance levels of joint degree MD/MBA students were comparable to those of other medical students, ranging from prematriculation to the time of their graduation. In addition, joint degree students in our program continued to focus their professional trajectories within the realm of medicine while, at the same time, gaining unique perspectives and skills. Such training is likely to enable them to provide needed leadership to an evolving medical care system, thereby addressing a pressing societal need.
Footnotes
Authors’ Note
The survey was reviewed and determined to be exempt by the HMS institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.