
Abstract
A self-report instrument assessing work-related factors among people with psychiatric disabilities would be useful when trying to match possible employment or prevocational opportunities with people’s desires and capacities. The aim of this study was to explore the factor structure, internal consistency, and construct and criterion validity of the Worker Role Self-Assessment (WRS) in this group as well as possible floor and ceiling effects. The participants were 283 clients from day centers for people with psychiatric disabilities and from outpatient units for people with psychosis. They completed the WRS and instruments selected to assess construct validity in terms of convergent (motivation for work and current activity level as reference variables) and discriminant validity (quality of life and self-rated health as reference variables). Two factors were identified, one tapping beliefs in a future worker role and one reflecting current capacities and routines. The internal consistency for the scale as a whole was good at 0.84. The factor reflecting a future worker role correlated as expected with the reference variables used to assess convergent and discriminant validity, whereas current capacities and routines showed a moderate association with quality of life and self-rated health, assumed to indicate discriminant validity. Criterion validity was shown in that those who had recent work experiences scored higher than the others on WRS. No floor or ceiling effects were identified. The findings indicate acceptable psychometric properties of the WRS. Further development is still warranted, however; the factor solution needs to be replicated and the construct validity should be further established.
Introduction
Work is an essential part of adult life, and a disability may severely hamper a person’s potential for gaining paid employment. Of all the disabled groups in Sweden, those with psychiatric disabilities are least likely to have a paid job and most likely to live under poor economic conditions (Swedish Board of Health and Welfare, 2010). Besides the importance of supporting oneself and one’s family, paid employment is essential for people with psychiatric disabilities for several other reasons, such as gaining social status, belonging in a social context, and shaping one’s identity (Gewurtz & Kirsh, 2007; Leufstadius, Eklund, & Erlandsson, 2009). It is thus imperative to find ways for supporting this group in finding their way to the employment market (Kirsh, Krupa, Cockburn, & Gewurtz, 2010). For that aim, assessments of work-related factors may be useful tools to judge a person’s capacities and find a match with possible employment or prevocational opportunities (Ilmarinen, 2009; Sandqvist & Henriksson, 2004).
Instruments of relevance for assessing work-related factors are often linked with a model for how to view work capacity. One example is the work ability index (Ilmarinen, 2001), which is related to the multidimensional work ability model (Ilmarinen & Tuomi, 2004). The latter evaluates not only the individual’s capacities but also his or her family, close social environment, workplace, work tasks, and societal context. Instruments that assess work ability should thus address not only work in a narrower meaning but also general personal capacities and access to environmental support. Sharing this view, a model that has stimulated the development of several instruments addressing work factors is the Model of Human Occupation (Kielhofner, 2008). This is another multidimensional model that includes the person’s volitional system, habits and roles, and performance capacity. The model sets these personal factors in relation to the physical and psychosocial environment and to political, economic, and cultural factors at the societal level. In comparison with the International Classification of Functioning, Disability and Health (ICF) (WHO, 2001), the Model of Human Occupation addresses the activity and participation components as well as personal and environmental factors. The outcome of the interplay between the individual and these contextual factors is reflected as participation in various arenas of human occupation, for example, engagement in paid employment. Among the work-oriented instruments based on this model are A dialogue about ability related to work (Linddahl, Norrby, & Bellner, 2003; Norrby & Linddahl, 2006), Assessment of Work Capacity (Sandqvist, Tornquist, & Henriksson, 2006), the Work Environment Impact Scale (Kielhofner et al., 1999), and the Worker Role Interview (WRI; Forsyth et al., 2006). All of these are based on interviews and/or observation and include an assessment made by the interviewer. The latter two have also been developed into self-report instruments, namely, the Work Environment Impact Scale–Self Rating and Worker Role Self-Assessment (WRS; Wastberg, Haglund, & Eklund, 2009), both of which were found reliable and valid when used in primary health care and work rehabilitation clinics, among other settings.
Self-reports are often convenient and time saving; and if the WRS is found to have acceptable psychometric properties also when used with people with psychiatric disabilities, it might be a valuable tool in endeavors to support that target group in developing a worker role. A role, in the context of the Model of Human Occupation (Kielhofner, 2008), is defined as a set of internalized attitudes and behaviors linked with a socially and/or personally defined position in a certain physical, social, and temporal habitat. The worker role is one of several internalized life roles that correspond to this definition. Examples of other internalized roles are being a friend, a parent, a student, a hobbyist, and so on (Kielhofner, 2008).
The current study addresses psychometric properties of the Swedish WRS. The WRI (Forsyth et al., 2006), on which the WRS is built, includes items that address (i) motivation and interests, (ii) roles and habits, and (iii) environmental factors. The reason why the items cover a broader perspective than the specific worker role is that a person’s array of roles is shaped by factors such as interests, motivation, and psychosocial and physical factors in the environment. It is also assumed that a person’s different roles may influence each other, so that one role may promote or hinder the execution of the other. Both the WRI and the WRS were developed to assist clinical decisions about needs for vocational support but were also to be used as outcome measures in the context of work rehabilitation. The fact that these instruments address the worker role in a wider meaning, also including items that assess everyday routines in general and environmental support, ensures that factors that significantly influence people’s work capacity are included. It has been hypothesized that the WRI reflects the potential to return to work (Bejerholm & Areberg, 2014), which is also possible for the WRS.
The WRS includes 14 items thought to be relevant regardless of the respondent’s employment status. This differs from the WRI, which was developed for temporarily unemployed people who have a specific job to return to. Each of the 17 WRI items were considered for inclusion in the WRS, and those alluding to a specific work context were excluded or rephrased to also suit those who were not employed. This meant, for example, that a question regarding the physical environment was excluded, and 3 WRI items that concern the psychosocial environment were reformulated from addressing the workplace to targeting the larger context of family and support systems. This is described in more detail by Wastberg and colleagues (2009). The WRS was found to have acceptable content and construct validity, utility, internal consistency, and test–retest reliability among people with a variety of musculoskeletal or stress-related problems in ongoing work rehabilitation. The overall WRS Scale was not predictive of return to work, but an item targeting belief in having a work in the future showed predictive validity of return to work following completion of work rehabilitation (Wastberg et al., 2009).
The factor structure of WRS has not been investigated, however, nor has its psychometric properties in people with psychiatric disabilities. The current study was aimed at exploring factor structure, internal consistency, construct and criterion validity, and the presence of floor and ceiling effects of the WRS in persons with a psychiatric disorder.
Method
Baseline data from two projects were included in this study. Project 1 compared two groups of people with psychiatric disabilities, one attending day centers and the other attending an outpatient unit for people with psychosis, on subjective perceptions of everyday activities (Argentzell, Leufstadius, & Eklund, 2012). The project included seven day centers and three outpatient units. Project 2 investigated outcomes of an intervention implemented in day centers aimed at creating more meaningful activities for the attendees (Eklund, Gunnarsson, Sandlund, & Leufstadius, 2014). It included eight centers. Since the present study solely used the baseline data, the participants from the two projects were treated as one sample. All study participants fulfilled the criteria for having a psychiatric disability, which is the requirement for access to day center facilities in Sweden and is assessed by a social worker. A psychiatric disability is defined as having difficulty managing everyday life, in terms of self-care and taking care of one’s home, for 2 years or more due to mental illness (Swedish Government Official Reports, 2006). Ethical approval was obtained from the regional ethical review board at Lund University, reg. nos. 303/2006 and 274/2008, and the Declaration of Helsinki was followed. All study participants were guaranteed confidential treatment of data and gave their written consent.
Participants
Information meetings describing the respective projects were held by the research team at all centers. Written information was also handed out during the meetings. Day center attendees who were interested in participating gave their written informed consent either immediately after the meeting or via the staff during a period of 2 weeks after the information meeting. The exclusion criteria were dementia or a history of developmental disorder, primary substance use disorder, unable to understand Swedish, and currently being too confused to participate. Attending staff identified potentially eligible study participants who were invited to be in the study. The participation rate was about 50% in both samples based on those participants who were assessed by staff to be potentially eligible. This is equivalent to similar studies where the data collection is not embedded in the usual services (Bengtsson-Tops, 2004; Eklund, Hansson, & Ahlqvist, 2004). Characteristics of the participants, 175 of which were from Project 1 and 108 from Project 2, are presented in Table 1. The gender distribution was equal and the mean age was 46 years. A majority had a high school education and some kind of psychosis was the most commonly reported diagnosis.
Characteristics of the Participants.
Note. N = 283.
Instruments
The WRS
The WRS (Wastberg et al., 2009) is a self-report questionnaire based on the items in the WRI (Ekbladh, Thorell, & Haglund, 2010; Forsyth et al., 2006). The version used in the present study has 14 items tapping different aspects of the worker role, as shown in Table 2 which also shows the domains to which the items pertain. The respondent rates the extent to which the statement is applicable to him or her on a 4-point Likert-type scale ranging from 4 = fully agree to 1 = fully disagree.
Items Included in the Worker Role Self-Assessment Instrument.

Note. V = the volitional domain; RH = the roles and habits domain; E = the environmental domain.
Instruments for assessing construct validity of the WRS
Construct validity is often assessed in terms of relationships with other instruments, and a variety of terms are used depending on (1) whether a valid standard measure of the construct at target exists already and (2) the closeness between the target construct and the selected reference construct from a theoretical point of view (Streiner & Norman, 2008). Since no established self-report measure addressing the worker role exists and since it would be important to assess relationships with similar as well as dissimilar constructs to obtain an appropriate assessment of construct validity, we sought to evaluate the convergent validity and discriminant validity of the WRS Scale. Convergent validity is the agreement between constructs that are assumed to be more highly linked with each other according to theory, while discriminant validity addresses level of agreement between constructs that according to theory should be dissimilar or less highly associated. A third way of evaluating construct validity is to test the instrument’s ability to discriminate between known groups, often termed criterion validity (Streiner & Norman, 2008).
As already mentioned, the original WRI (Forsyth et al., 2006) aimed at evaluating aspects of motivation and interests, roles and habits, and performance capacity. Therefore, in order to assess convergent validity of the WRS, reference variables were identified that were thought to be theoretically similar to these concepts. The reference variable chosen to reflect motivation and interests comes from a set of 4 items addressing motivation for engaging in day center activities (Eklund & Tjornstrand, 2013). One of these is worded “I would prefer having a job to go to.” The response scale is a Visual Analogue Scale, where the respondent marks his or her rating on a 100 mm line. A panel of mental health care users and professionals estimated that the item had face and content validity (Eklund & Tjornstrand, 2013). The participation scale from the 9-item Satisfaction with Daily Occupations instrument (SDO; Eklund, 2004) was used as another reference variable, assumed to share features with roles, habits, and performing activities. The SDO is an interview-based questionnaire that addresses participation in, and satisfaction with, everyday activities within the areas of work, leisure, domestic tasks, and self-care. Each item has two parts, where the first asks whether the respondent presently participates in the activity (yes/no) and the second asks for the respondent’s satisfaction with engaging or not engaging in that activity. Satisfaction ratings were not used for assessing convergent validity, however, since satisfaction with everyday activities was regarded dissimilar to perceptions of one’s worker role. The SDO has shown good psychometric properties in terms of construct validity and test–retest reliability (Eklund & Gunnarsson, 2007), and the participation scale has shown convergent validity in terms of a strong correlation with occupational engagement (Bejerholm & Eklund, 2006). The WRI would have been a logical choice for reference instrument but was considered too time consuming to be used with the current target group.
It was reasoned that variables such as quality of life and health would be regarded as less similar to the worker role from a theoretical point of view. The quality of life instrument used was the Manchester Short Assessment of Quality of Life (MANSA; Priebe, Huxley, Knight, & Evans, 1999), which includes a general quality of life item and an additional 11 items addressing satisfaction with different life domains, such as economic situation, work, friends, family, housing conditions, physical and psychological health, security, and so on. The respondent rates his or her satisfaction with the targeted domain on a scale ranging from worst possible satisfaction (1) to best possible satisfaction (7). The Swedish version of MANSA was used, which was found to have good internal consistency (α = .81) and satisfactory construct validity (positive correlations with social network, empowerment and psychosocial functioning, and negative correlations with number of needs for care, perceived devaluation and discrimination, and rejection experiences; Bjorkman & Svensson, 2005). The health assessment used was a rating of self-rated health, namely, the first item from the Medical Outcome Scales (Short-Form Health Survey-36; Ware & Sherbourne, 1992). Use of this item, worded “In general, how would you say your health is?” has been proposed as sufficient, since it correlates highly with the scale as a whole and provides a reliable estimate (Bowling, 2005).
In order to characterize the sample, a background questionnaire requesting sociodemographic data was used. It also asked for self-reported diagnosis, which was subsequently coded according to the International Classification of Diseases (ICD-10) classification (WHO, 1993) by a psychiatrist. The validity of these self-reported diagnoses was supported by expected differences between diagnoses in psychopathology ratings based on the Brief Psychiatric Rating Scale (BPRS) (Crippa, Sanches, Hallak, Loureiro, & Zuardi, 2001; Kolakowska, 1976), such as higher levels of psychotic symptoms in participants with schizophrenia or schizoaffective disorder and higher levels of depression in those with mood disorders (Eklund & Sandlund, 2012).
Procedure
Project assistants, who were not involved in the participant’s treatment and who had prior experience from collecting data for research projects, performed the data collection. The project assistant met each participant in private, and the data collection took place in a secluded and quiet room at the day center.
Data Analyses
The dimensionality of the WRS Scale was analyzed with exploratory structural equation modeling (ESEM; Marsh et al., 2010), using MPlus 7.11 (Muthén & Muthén, 2012). We tested two models, one assuming that the scale consisted of one factor and the other that it had two factors. To guide further decisions regarding the models, we used the fit indices root mean square error of approximation (RMSEA) and confirmatory factor index (CFI). In addition, we consulted the modification indices to follow up on misfit in the models.
As a complementary analysis, we investigated Cronbach’s α and McDonald’s Ω (1999) to estimate the internal consistency of the scale. McDonald’s Ω has two variants, the hierarchical, which measures the reliability of the general factor of a scale, and total, which measures the total amount of systematic variance. To calculate the Ω hierarchical and total, we used the exploratory factor analytic approach suggested by Revelle and Zinbarg (2009) implemented in the psych package (Revelle, 2015) of R (R Core Team, 2013). We supplemented these measures with an Ω total based on a one-factor confirmatory factor analysis (CFA).
Further analyses were performed with the IBM SPSS Statistics 22.0. Pearson correlations were used to assess convergent and discriminant validity. The strength of relationships was estimated according to the limits proposed by Cohen (1992). He suggested correlations of .1–.3 to be weak, .3–.5 to be moderate, and .5 or more to be strong.
Frequency tables were used to explore possible floor and ceiling effects. A proportion of 20% or more of participants with a maximum score or a minimum score is considered to be sizable and indicates a ceiling and a floor effect, respectively, whereas a proportion of 5% or less of a sample with a maximum or minimum score reflects sound and effective measurement (Holmes & Shea, 1997; McHorney, Ware, Lu, & Sherbourne, 1994).
Results
The participants’ mean rating (SD) on the WRS was 41.7 (8.3) on a scale that can range between 14 and 56, thus indicating positive worker role perceptions.
Factor Structure of the WRS
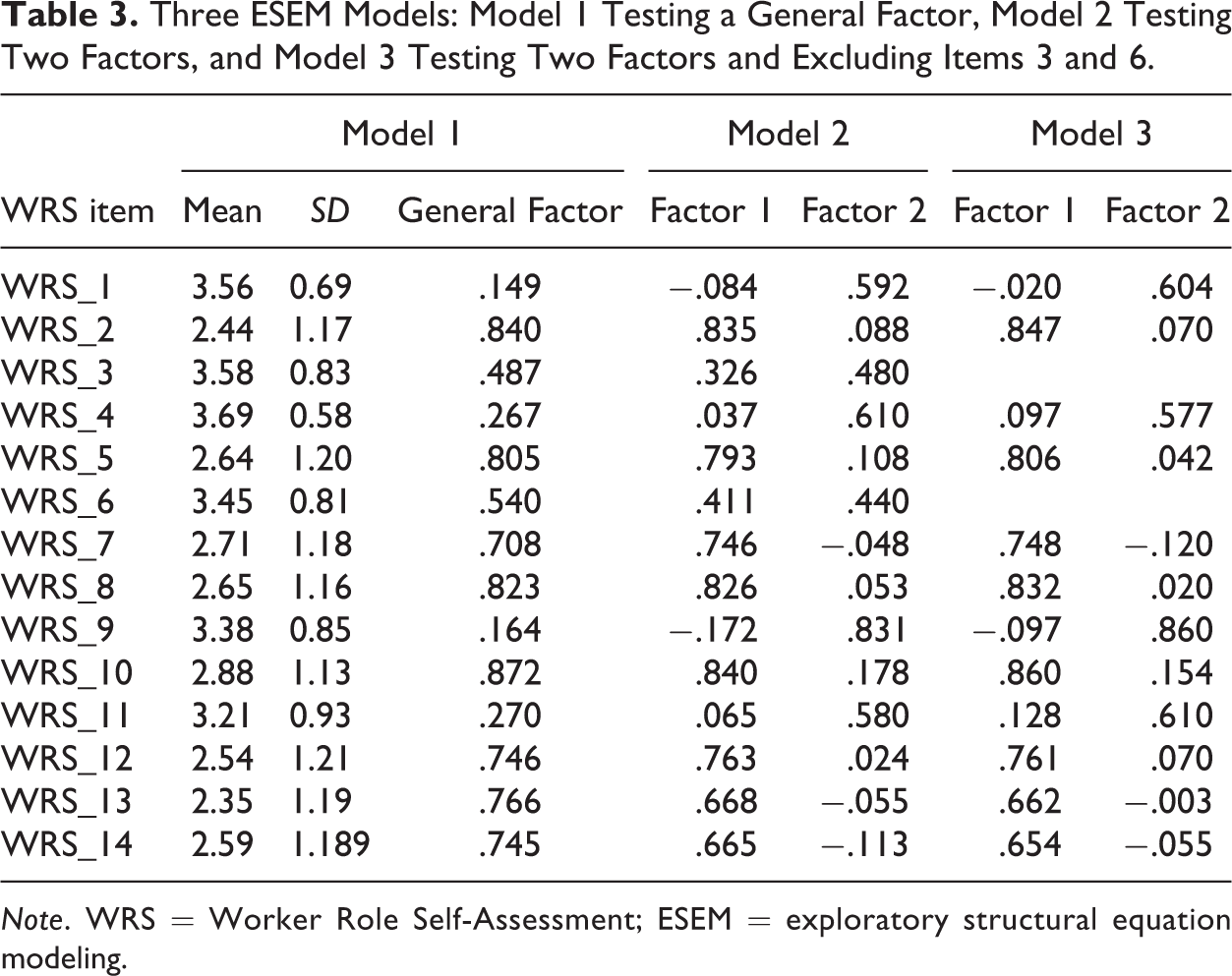
The variables were defined to be categorical and we therefore used (WSMLV) as our estimator when performing the ESEM. The first model tested only one factor (equivalent of a CFA with one factor) and did not reveal close fit to the data, χ2(77) = 717.9, RMSEA 0.171, CFI = 0.840 (see Model 1 in Table 3). This model was tested against an ESEM model with two factors, and the fit was much closer to the data, χ2(64) = 308.74, RMSEA = 0.116, CFI = 0.939. In this model, most of the items had loadings aligned with a two-factor structure (Model 2 in Table 3). The first factor concerned beliefs in a future worker role and the other reflected current capacities and routines in more general terms. The correlation between the factors was .175. After consulting the modification indices, we found that Items 13 and 14 had common variance beyond what was explained by the factors. We attributed this to the very similar phrasing of the 2 items and added an error correlation between Items 13 and 14. After this addition, the model fit was clearly better, χ2(63) = 227.1, RMSEA = 0.096, CFI = 0.959, and the factor correlation was .165. Two items were, however, still problematic; Items 3 and 6 had high secondary loadings in addition to a rather high error correlation. We tested two different strategies to address this problem; first, we added the error correlation between Items 3 and 6 to the model. This increased the fit even more, χ2(62) = 179.5, RMSEA = 0.082, CFI = 0.971, but the items still loaded on both factors. Second, we tested a model excluding Items 3 and 6 (Model 3 in Table 3). The new model showed a similar fit, χ2(42) = 137.8, RMSEA = 0.090, CFI = 0.974, to the model including the items. However, the models are not recursive and cannot be compared directly based on the fit indices.
Three ESEM Models: Model 1 Testing a General Factor, Model 2 Testing Two Factors, and Model 3 Testing Two Factors and Excluding Items 3 and 6.
Note. WRS = Worker Role Self-Assessment; ESEM = exploratory structural equation modeling.
Internal Consistency
The Ω hierarchical for all items was .73, α was .84, and Ω total was .88 (.86 based on a one-factor CFA). This indicates that the general factor was reliable. On the other hand, 4 items did not reveal high loadings on the general factor, namely, Items 1, 4, 9, and 11 (see Table 3). Deleting these 4 items resulted in an Ω hierarchical of .84, α was .87, and Ω total was .91 (.89 based on a one-factor CFA), suggesting that those items did not contribute to the reliability of the full scale and supporting the ESEM finding of a two-factor model.
In addition, we tested a model without Items 3 and 6, which loaded on both factors resulting from the ESEM. The Ω hierarchical for the full scale decreased to .78, α to .89, and Ω total to .92 (.89 based on a one-factor CFA), suggesting that Items 3 and 6 contributed to the general factor’s reliability but made the scale multidimensional (indicated by the somewhat higher discrepancy between Ω hierarchical and total). Thus, both the ESEM analysis and the reliability analysis suggest that the scale is multidimensional and that it should be regarded as having two factors with a rather low intercorrelation. Taken together, the analyses indicated that all items could be kept as in Model 2.
Construct Validity
The associations between the factors from Model 2 and the selected reference variables are shown in Table 4, which also includes descriptive data. Factor 1, tapping beliefs in a future worker role, discriminated clearly between those who had been working during the past month and those who had not, thus indicating criterion validity. The other factor, reflecting current capacities and routines, did not separate the groups. Factor 1 also showed statistically significant associations with being highly motivated for work and with a high activity level, but also with better self-rated health. Factor 2, which concerns current capacities and routines, was associated with better quality of life and better health. The associations with Factor 1 mainly confirmed the hypothesized relationships, whereas those with Factor 2 did not.
Associations Between the Two WRS Factors Based on Model 2 and the Reference Variables.
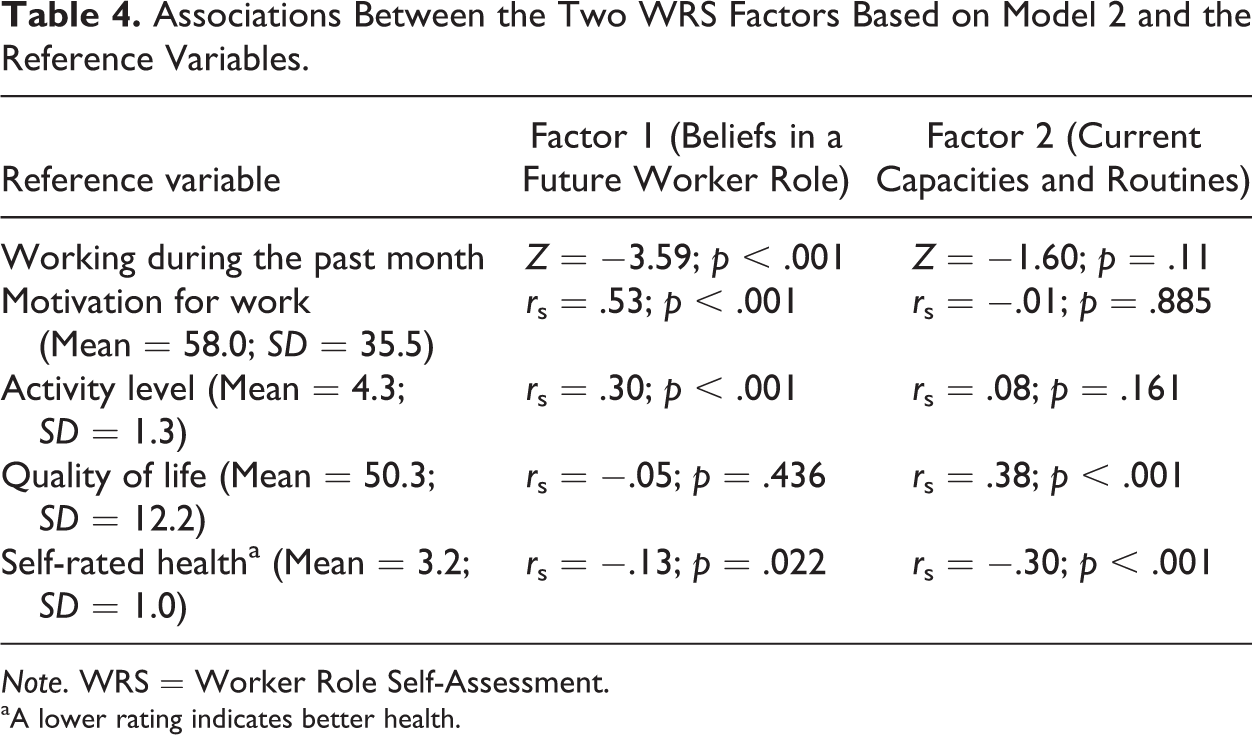
Note. WRS = Worker Role Self-Assessment.
aA lower rating indicates better health.
Examination of Floor and Ceiling Effects
Frequency distributions of item ratings showed that the lowest rating was used by between 1% (for Item 4—awareness of commitments and obligations) and 24% (for Item 13—support from different authorities) of the participants. The highest rating was used by between 25% (for Item 2—viewing work as part of future life) and 75% (for Item 4—awareness of commitments and obligations) of the participants. Regarding the scale as a whole, only 0.4% of the sample had the lowest score and 3.2% the highest score.
Discussion
The findings clearly indicated that the WRS is not unidimensional, and a two-factor solution was found. One factor concerned a narrower aspect of work and mainly included the items where work is specifically mentioned. The other reflected capacities and routines in more general terms. Model of Human Occupation (Kielhofner, 2008) defines a role as a set of internalized attitudes and behaviors linked with a defined position in a certain environment (thus work in this study), but it also emphasizes the importance of habits and routines as an overarching structure that encompasses roles (Kielhofner, 2008). The two-factor solution of the WRS appears consistent with this model, the first factor tapping the worked role per se and the second tapping habits and routines.
The WRS Scale as a whole showed satisfactory internal consistency. Items 1, 4, 9, and 11 showed low loadings on a common factor, but since a two-factor model fitted the data better and all of these had loadings of >0.40 to Factor 2, we suggest retaining these items in the WRS. Another reason for retaining them is that they capture essential aspects of the worker role according to the Model of Human Occupation (Kielhofner, 2008). Items 3 and 6 were somewhat problematic because they loaded on both factors, but they contributed to the internal consistency of the scale as a whole and address important aspects of the worker role. Our recommendation is therefore to retain these items and to use the full 14-item version of the WRS that we tested in this study.
Factor 1 (beliefs in a future worker role) discriminated clearly between those who recently had a job and those who had not, indicating criterion validity. This factor also showed expected associations with the reference variables. The association with the motivation for work item was strong according to the guidelines proposed by Cohen (1992), whereas the association with activity level was moderate. There was also a statistically significant relationship, but weak, with self-rated health. Factor 2 (current capacities and routines), on the other hand, did not discriminate between recent workers and nonworkers nor was it associated with motivation for work or activity level. Instead, it was moderately related to personal well-being in terms of quality of life and self-rated health. The results tend to converge into a scenario with Factor 1 that taps the essence of the worker role, particularly beliefs in having that role in the future, and Factor 2 that seems to capture capacities and routines that support the worker role but are more general in nature and may also support other life roles.
Examination of possible ceiling and floor effects indicated no such effects. A previous study on the WRS, where the target group was people with mixed problems who participated in vocational rehabilitation, suggested that the WRS could produce ceiling effects (Wastberg et al., 2009). This was, however, not the case in this study of people with psychiatric disabilities.
These psychometric properties of the WRS suggest that it reliably and validly assesses the worker role among people with psychiatric disabilities. Since two factors gave the best model fit, the authors suggest using these two factors rather than the scale as a whole. The fact that 2 items loaded on both factors should not constitute a major problem in this respect. The WRS provides the respondent’s view of his or her worker role and may contribute valuable information in initial assessment and at follow-ups in vocational training. It can also serve as a tool in research projects when an easily administered and brief assessment of self-reported work role is desired. The WRS is, however, less suited when in-depth and detailed information about an individual’s work situation is needed.
Methodological Considerations
It would have been interesting to compare the WRS with the WRI, but that was not feasible in the current study because it was considered too time consuming and tiring for the target group, in light of the other assessments of reference variables needed. WRI is the interviewer’s report on items that are equivalent to the WRS items and that difference in perspective could be important. Previous research comparing the perspective of “the other” (such as a staff member or a researcher) and the respondent has only found weak correlations concerning, for example, ratings of engagement in productive occupations (Tjörnstrand, Bejerholm, & Eklund, 2013) and the respondent’s quality of life (Eklund & Hansson, 1998). Whether similar diverging findings would be obtained when comparing WRS and WRI ratings is a topic for future studies.
Conclusion
The findings indicate acceptable psychometric properties of the WRS, as indicated by satisfactory internal consistency, a factor solution that yielded two interpretable and theoretically distinct factors, preliminary construct and criterion validity, and the absence of floor and ceiling effects. Further development is still warranted, however; the factor solution needs to be replicated and the construct validity should be further established.
Footnotes
Authors’ Note
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Primary data may be obtained on request from the author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.