
Abstract
This article presents a practitioner-based approach to identify key combinations of contextual factors (C) and mechanisms (M) that trigger outcomes (O) in Dutch community-based health-enhancing physical activity (CBHEPA) programs targeting socially vulnerable groups. Data were collected in six programs using semi-structured interviews and focus groups using a timeline technique. Sessions were recorded, anonymized, and transcribed. A realist synthesis protocol was used for data-driven and thematic analysis of CMO configurations. CMO configurations related to community outreach, program sustainability, intersectoral collaboration, and enhancing participants’ active lifestyles. We have refined the CBHEPA program theory by showing that actors’ passion for, and past experiences with, physical activity programs trigger outcomes, alongside their commitment to socially vulnerable target groups. Project discontinuity, limited access to resources, and a trainer’s stand-alone position were negative configurations. The authors conclude that local governance structures appear often to lack adaptive capacity to accommodate multilevel processes to sustain programs.
Keywords
Health disorders associated with inactivity, including impaired health-related quality of life as well as direct and indirect economic costs, exert a substantial burden on societies and health systems (Craig et al., 2012). In the Netherlands, socially vulnerable groups, for example, those with low socioeconomic status (SES) or of non-Dutch origin, are generally less healthy than higher SES groups (Kunst et al., 2005) and are less engaged in sport and physical activity (PA) (Hildebrandt, Bernaards, & Stubbe, 2013; Wendel-Vos et al., 2009). In response to the observed inequities, it has been Dutch policy to promote community-based health-enhancing PA (CBHEPA) programs in order to improve the health and well-being of socially vulnerable groups (Ministry of Health Welfare and Sports, 2006, 2012; Storm, Aarts, Harting, & Schuit, 2011). The rationale for the Dutch government subsidizing recreational sport and physical activities schemes such as CBHEPA programs is based on the notion that participation in these programs supports the development of social capital and quality of life in a community by contributing to community bonding (Kawachi & Berkman, 2000; Lindström, Hanson, & Östergren, 2001; Putnam, 2000; Skinner, Zakus, & Cowell, 2008). Additionally, it may improve the health and well-being of participants (Hawe & Shiell, 2000; Kahn et al., 2002).
CBHEPA programs targeting socially vulnerable groups are usually so-called natural experiments by design, embedded in ongoing field practice rather than in an experimental setup. Consequently, they have an important contribution to make to the health inequities agenda, as they can play a role in investigating the determinants of health inequities and in identifying effective interventions (Petticrew et al., 2005). This, however, requires evaluation approaches that are sensitive to the operational conditions of CBHEPA programs as part of larger complex systems (Judge & Bauld, 2001). This study aims to identify key combinations of contextual factors and mechanisms that trigger outcomes of interest in Dutch CBHEPA programs from a practitioner perspective.
Evaluation in the Context of an Ecological Perspective on Human Health
Theories to develop and implement CBHEPA programs are based on an ecological perspective on human health, emphasizing the interaction between actors and factors within and across the different levels (Green & Kreuter, 2005; Herens, Wagemakers, Vaandrager, Van Ophem, & Koelen, 2013; Rimer & Glanz, 2005; Sallis et al., 2006). CBHEPA program theory is based on individual (Chatzisarantis & Hagger, 2009; Schwarzer, 2008; Sniehotta, Schwarzer, Scholz, & Schüz, 2005; Van Stralen, De Vries, Mudde, Bolman, & Lechner, 2009) and group-related behavioral theories (Burke, Carron, Eys, Ntoumanis, & Estabrooks, 2006; Estabrooks, Harden, & Burke, 2012; Harden, Burke, Haile, & Estabrooks, 2013; Spink, Wilson, & Priebe, 2010), and they build on concepts such as social cohesion, supportive environments, and community participation (Hawe & Shiell, 2000; Herens, Wagemakers, den Besten, & Bernaards, 2015; Kawachi & Berkman, 2000; Sallis et al., 2006; Toropainen & Rinne, 1998; Wagemakers, Vaandrager, Koelen, Saan, & Leeuwis, 2010). Furthermore, CBHEPA programs are underpinned by theories on intersectoral collaboration and coordinated action, addressing stakeholder involvement and community ownership (Best et al., 2003; Koelen, Vaandrager, & Wagemakers, 2012; Kothari & Armstrong, 2011; Sallis et al., 2006; Wagemakers et al., 2010).
Collecting practice-based evidence on CBHEPA programs should, therefore, build on the knowledge of different stakeholders. In the course of program delivery, practitioners generate knowledge and create hypotheses about what works for whom in what circumstances (Judge & Bauld, 2001; Pawson & Tilley, 1997). Dealing with such real-life complexity issues requires efforts to understand better contextual and historical influences, mechanisms, and the impact of unexpected events or factors in relation to (intended) outcomes (Barnes, Matka, & Sullivan, 2003; Blamey & Mackenzie, 2007; Byng, Norman, & Redfern, 2005; Jolley, 2014; Judge & Bauld, 2001; Marchal, van Belle, van Olmen, Hoerée, & Kegels, 2012; Pawson, 2002; Pawson, Greenhalgh, Harvey, & Walshe, 2005; Rifkin, 2014).
Using a Realist Perspective
To identify key combinations of contextual factors and mechanisms that trigger outcomes of interest in Dutch CBHEPA programs, our study builds on a realist evaluation perspective. Pawson and Tilley (1997) developed realist evaluation, arguing that, in order to be useful for decision makers, evaluations need to indicate what works, how, in which conditions, and for whom rather than to answer the question, does it work? (Pawson, 2003). Realist evaluations start with an account of the processes that explain how an intervention leads to a particular outcome, initially formulated as a middle range or program theory based on existing theories, past experience, and previous evaluations or research studies. The final research product from realist evaluation is not a statement of effect size, as the same program will have different effects in different contexts, but a refinement of the program theory (Pawson, 2002; Pawson & Tilley, 1997).
Realist evaluation is presented by Pawson as an additional model in systematic research on evidence-based policy and practice, alongside meta-analysis and narrative reviews, by comparing program mechanisms. According to this perspective, it is not programs that work but rather the underlying reasons or resources that they offer actors to generate change. Whether the choices or capacities available in an initiative are acted upon depends on the nature of the actors and the circumstances of the initiative (Pawson, 2002). It is for this reason that realist evaluation seems promising for evaluating multilevel CBHEPA programs (Marchal et al., 2012).
Method
The study followed a multiple case study design (Yin, 2003). To identify mechanisms relating to outcomes of CBHEPA programs and contextual influences, we examined six ongoing Dutch CBHEPA programs between 2012 and 2014, summarized under the denominator: Communities on the Move (CoM). CoM was developed and disseminated in line with national policy objectives by the Netherlands Institute for Sports and Physical Activity (2003–2012), targeting inactive, socially vulnerable groups. Its overall aim was to enhance PA levels in socially vulnerable groups in order to improve participants’ quality of life and societal participation. Since 2012, CoM has been subject to a comprehensive evaluation study (Herens et al., 2013).
A longitudinal action research approach was adopted. At the start of each collaboration with a CBHEPA program, an exploratory interview was conducted, followed after 12–18 months by a focus group using a narrative timeline technique (Wielinga & Vrolijk, 2009). The timeline technique was chosen, as it is designed to respect contextual and historical influences, generating data based on stakeholders’ individual and collective perceptions, thus reflecting CBHEPA program dynamics over time (Wielinga & Herens, 2013). In addition, the timeline technique visualizes actor perceptions of what matters most, offering both the researcher and participating practitioners a way to gather data on program progress (Hughes, 2008; Koelen & van den Ban, 2004). Realist synthesis was used in the data analysis, facilitating the identification of the contextual factors and program mechanisms determining outcomes in each of the CBHEPA programs (Pawson, 2002).
Study Setting and Population
Six CBHEPA programs were selected (purposive sampling). The objective of using multiple cases was to achieve conceptual power rather than population representativeness. For each case, relevant stakeholders for interviews and timeline sessions were recruited by local project coordinators in collaboration with the researcher (first author). The study population consisted of local stakeholders, primarily representatives of implementing organizations (project coordinator, exercise trainer), municipal or welfare organizations’ community workers, and other actors from local networks (Table 1).
CBHEPA Program Characteristics.
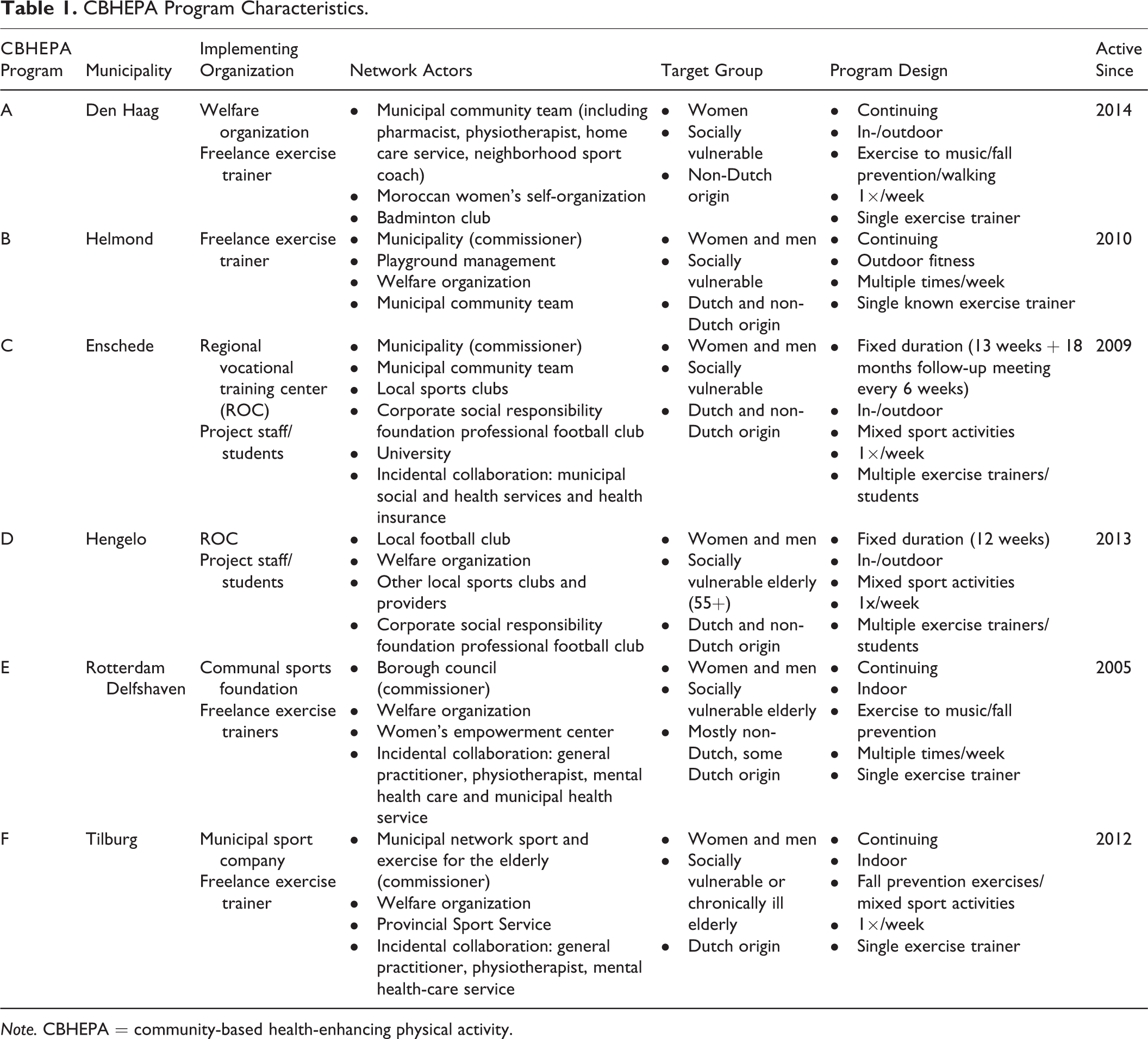
Note. CBHEPA = community-based health-enhancing physical activity.
The CBHEPA programs involved in our study did not start from scratch; rather, they were generally embedded in ongoing national and local (policy) developments and existing collaborative structures. They were initiated by different types of actors, namely, representatives of two welfare organizations, two local sports promotion organizations, and a regional education center (ROC) covering two municipalities. The initiative to start a CBHEPA program usually came from individuals, driven by an inner motivation to use PA as a means to improve the lives of socially vulnerable target groups.
The CBHEPA programs could be distinguished into two types. Two programs used a project-based intervention design, building on a predefined framework or format, usually organizing activities for a fixed period of time (12–13 weeks). In these programs, we could connect to start-ups of new PA groups. Four CBHEPA programs used a continuing, service-oriented design, driven by the aim to provide for sustained sport and PA schemes tailored to the needs of the target group. In these programs, we could connect to ongoing activities in existing groups (Table 1).
Data Collection
Data were collected between 2012 and 2014. In a semi-structured interview, data were collected for each CBHEPA program in relation to intended outcomes of interest, the mechanisms associated therewith and contextual factors (e.g., organizational issues, networks involved or funding). Five semi-structured interviews were conducted with program coordinators and exercise trainers (n = 9), covering six different CBHEPA programs (Table 2).
Data Collection Scheme CBHEPA Programs.

Note. CBHEPA = community-based health-enhancing physical activity.
aAt the time of the interview, one respondent was ill and therefore did not attend. bThe ROC had initiated two different CBHEPA programs in two municipalities, acting as overall implementing agency. The two initiatives were discussed in one interview.
After 12–18 months, for each CBHEPA program, a focus group using the narrative timeline technique was organized. Timeline participants were identified by local project coordinators and jointly invited by the local project coordinator and researcher (first author), thus reaching a total of 39 participants (Table 2).
Each timeline session was conducted on-site, following a stepwise procedure. Each session was facilitated by the researcher (first author). First, once the purpose and procedures of the timeline session were explained, a prepared timeline, drawn on flip charts and divided into three rows, was put up on the wall. The top row was intended to reflect on occasions of positive energy during the process, the middle on occasions that took energy away, and the bottom on breakthrough occasions (new insights, opportunities). Milestones in the process (e.g., critical incidents or meetings, months or years) were marked by the researcher, dividing the timeline with vertical lines. Second, individual perceptions were collected. All participants were asked to recall occasions that mattered most in the process, which then were marked by the facilitator on the prepared timeline. Then, the participants were asked to write down in brief statements how these occasions mattered to them individually. Each participant was provided with a marker and self-adhesive sheets (post-its) in three colors: green for energizing (☺) or inspiring events or occasions, red for energy draining events (☹), and yellow for occasions of insight or breakthrough (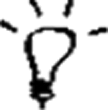 ). The statement, for example, “When we actually started the first group, it gave me a thrill,” would be written on a green sheet. Each participant placed his or her statements on the corresponding milestone on the timeline. Third, a plenary dialogue was facilitated, using the visualizations on the timeline. Clusters of colored post-its on the timeline usually indicated periods, in which significant changes had taken place. Then the group discussed what had been written in order to come to a mutual understanding of what had happened. Finally, conclusions and action points were noted. Each timeline session took around 1½ hr.
). The statement, for example, “When we actually started the first group, it gave me a thrill,” would be written on a green sheet. Each participant placed his or her statements on the corresponding milestone on the timeline. Third, a plenary dialogue was facilitated, using the visualizations on the timeline. Clusters of colored post-its on the timeline usually indicated periods, in which significant changes had taken place. Then the group discussed what had been written in order to come to a mutual understanding of what had happened. Finally, conclusions and action points were noted. Each timeline session took around 1½ hr.
In between the two points of data collection, each field visit, telephone call, or e-mail contact were documented for all CBHEPA locations. These notes proved valuable data sources to track program progress and sudden incidents or changes; for example, changes in program fees, staff turnover, or even transfer of the program from one organization to another. The information was used in the preparation of the timeline sessions to identify milestones in retrospect for each CBHEPA program.
Data Analysis
Initial interviews and timeline sessions were all anonymized and transcribed ad verbatim. A longitudinal perspective was used, considering the initial interviews as the baseline data and the retrospective timelines as follow-up measurements. Our analysis was stepwise, data driven, and thematic (Braun & Clarke, 2006), using Atlas.ti (7.5.9). Coding was developed based on a realist synthesis protocol. In realist evaluation, the focus is on context–mechanism–outcome (CMO) configurations. Data extraction takes the form of an interrogation of the baseline inquiries for information on what works for whom in what circumstances. The analysis of qualitative data from interview transcripts is then based on coding in terms of outcomes as observed by respondents, context conditions, and description of underlying mechanisms in the actual intervention (Marchal et al., 2012).
Step 1: All transcripts were coded by the first author in discrete terms of contexts (C), mechanisms (M), and outcomes (O). Step 2: Quotes coded as “context” were further thematized into historical-, organizational-, programmatic-, and participant-related codes. Quotes coded as “mechanism” were also further thematized into organizational-, programmatic-, and participant-related codes as were quotes coded as “outcome” (Table 3).
Operationalization of Context–Mechanism–Outcomes Concepts in CBHEPA Programs.
Note. CBHEPA = community-based health-enhancing physical activity.
aBased on Byng et al. (2005); Jagosh et al. (2015); Pawson (2002); Pawson et al. (2005). bBased on Jackson and Kolla (2012). cBased on Fetterman and Wandersman (2005); Herens, Wagemakers, Vaandrager, Van Ophem, and Koelen (2013).
Each theme was further refined into subthemes, that is, organizational policy, program resources, or participant attitudes, and labeled as supportive (+) or restraining (−), thus addressing the aim of differentiating and accumulating evidence on positive and negative CMO configurations (Pawson, 2002).
All coding procedures were done independently by two researchers (first author and a junior researcher). We found that the same phenomenon could be coded as outcome or context, or as context or mechanism, as was also found by Byng, Norman, and Redfern (2005). This was mainly attributable to different underlying researchers’ perspectives. For example, the first author would label a subsidy scheme for PA promotion as a condition, enabling the implementing agency to initiate a CBHEPA program. Therefore, this was coded as a supportive contextual factor, whereas the second researcher would label this as a supportive financial mechanism. The final argument to label this example as context was that, although the subsidy scheme in itself is a governmental mechanism to enhance PA promotion, it is beyond the control of a CBHEPA program. This and other differences in coding were discussed until consensus was reached, thus making explicit that all coding was based on the perspective of the actual CBHEPA program implementation activities.
Step 3: Following procedures for data reduction as suggested by Byng et al. (2005) and Jackson and Kolla (2012), for each case, outcomes of interest in relation to contextual factors were identified based on the initial interviews, depicting the historical and organizational setup of each CBHEPA initiative.
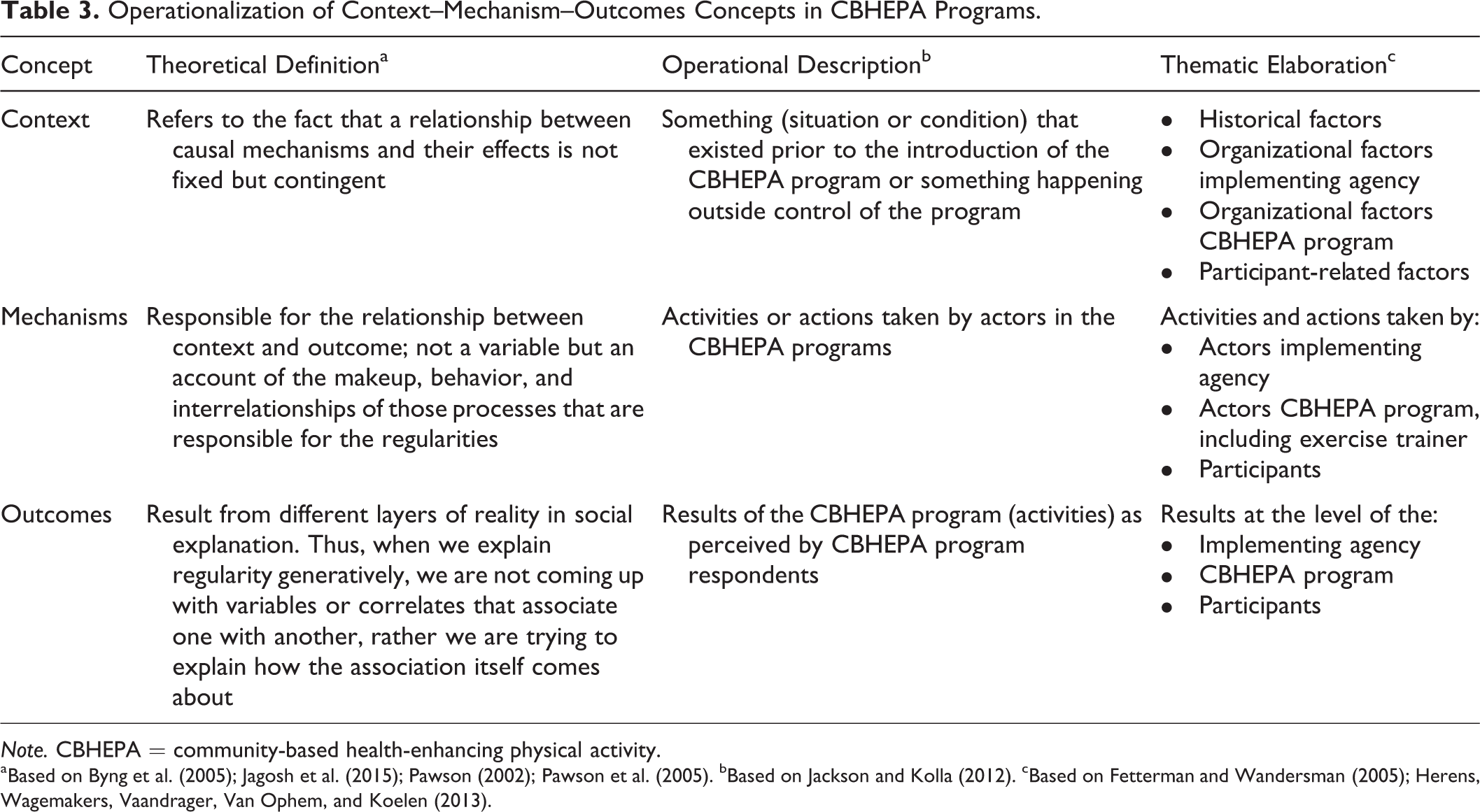
Step 4: Then the outcomes of interest were pooled from all cases. At the organization level, the main domain of outcomes of interest related to community reach; at program level to program sustainability and intersectoral collaboration; and at participant level to enhanced active lifestyles and societal participation (Table 4). On pragmatic grounds, we restricted our further in-depth analysis of CMO configurations relating to outcomes of interest identified in at least five programs.
Synthesis of Intended Outcomes of Interest of Six CBHEPA Programs.
Note. CBHEPA = community-based health-enhancing PA.
Step 5: For each case, timeline narratives were analyzed for CMO configurations. Through linked coding procedures, mechanisms–outcomes dyads were formed in relation to contextual factors, using the Atlas.ti (7.5.9) program to link codes and define relationships (Friese, 2012).
Step 6: In a second level analysis across cases, CMO configurations were further elaborated. To facilitate data interpretation, the coded data were reduced, via reference to the CMO configurations in the case studies, to a tabular form for each outcome of interest under consideration. This matrix allowed a visual overview of cases, mechanism, outcomes, and contexts. Symbols such as + and − were used to track supportive and restraining contextual factors and mechanisms. Contextual factors were labeled as generic if they related to all outcomes of interest covered by each outcome domain. They were labeled as specific when they related to a particular mechanisms–outcome dyad. In the findings presented below, the clearest quotations illustrating respondents’ views in relation to CMO configuration are included.
Ethical Considerations
The authors declare that the study was conducted in accordance with the general ethical guidelines for behavioral and social research in the Netherlands (Central Committee on Human Related Research, 2002). All respondents entered into the research with voluntary consent. They were provided with information about the purpose and contents of the study, and guarantees of confidentiality and anonymity were given prior to each interview and evaluation session. Moreover, participants were able to withdraw from the study at any time for any reason.
Results
Reasons for launching a CBHEPA initiative were mainly historically rooted: past (success) experiences at organizational level with PA projects and long-standing working relationships within the target communities (trust/enthusiasm). Furthermore, the presence of related health and welfare projects and established community networks were factors of importance.
CMO Configurations That Matter in Community Outreach
Community outreach, highlighting the outreach to vulnerable target groups and visibility as main outcomes, was identified as a main outcome domain for organizations involved in CBHEPA programs. Generic contextual factors supporting community outreach related to the personal passion for sport and PA of all actors involved, who identified a strong belief in the benefits of sport and PA for empowering vulnerable target groups as relevant. Furthermore, established, sometimes formalized, collaborative structures at municipality level reinforced by integral community-oriented policies were identified as supportive factors indicating long-standing trustful relationships among involved community-based actors. Generic contextual factors restraining community outreach related to organizational dynamics, for example, organizational restructuring, policy changes, such as national policies reshaping local social welfare policies, staff turnover resulting in loss of qualified personnel, or lack of continuity and involvement of network representatives. Another generic contextual restraining factor related to a lack of policy interest to reach out to socially vulnerable target groups (Figure 1).

Context–mechanism–outcome configurations on community outreach: Reach target groups (O1) and organizational visibility (O2).
Reach to community target groups (O1)
Respondents perceived CBHEPA programs as a good strategy to reach out and stay close to practice, for example, community stakeholders and target groups. Key supportive mechanisms at organizational level to reach the target population related to professional freedom of action for initiators or project coordinators. This involved collaboration with key actors in the community to bring together necessary resources and skills and a flexible application of project terms of reference such as expanding the recruitment area or diversification of groups. Supportive mechanisms at the exercise trainer level were securing the use of qualified trainers familiar with the target groups, the organization, and management of group-based PA activities so as to ensure social support, and the use of highly personalized approaches to reach out to individual participants and their social networks. Contextual factors in support of these mechanisms were past experiences and lessons learned from different projects over the years, suggesting the presence of a body of knowledge on how to act and highly committed professionals and actors eager to make a difference for the target population.
Restraining mechanisms were predominantly mentioned in relation to loss of the most vulnerable individuals and nonattendance; these were perceived as persistent and highly time-consuming problems. Restraining contextual factors were changes or increases in program fees resulting in loss of the most vulnerable participants and poor exercise trainer employment conditions, usually freelance, whereby additional tasks in support of the target group were excluded from payment. In some cases, legal contracts and organizational support were lacking. Additional restraining contextual factors were participant related, such as cultural dispositions and habits and lack of sport or PA experiences over the life span. Diversification of groups in terms of age and ethnic or cultural background was, interestingly enough, identified as a supportive as well as restraining mechanism. Group contexts, such as cultural habits or sense of community, may be decisive for the effectiveness of this mechanism (Figure 1).
Becoming visible in, and familiar with, the communities (O2)
Respondents identified CBHEPA programs as a strategy for organizational visibility within communities and neighborhoods. Key supportive mechanisms were the mobilization of passionate and committed actors and making oneself noticed in the community, for example, by attending community meetings or activities. Use of (social) media and other communication strategies, as well as accountability efforts (writing reports), was also mentioned. Contextual factors in support of these mechanisms were actors’ enthusiasm and shared ambition at the start of the program, reinforced by access to funding. Being part of, or aligned with, related community-based initiatives contributed to organizational visibility at community level, indicating a joint impact of the different initiatives.
Restraining mechanisms were discontinuity of actor commitment and involvement, not being able to get the right people around the table, and negligence about communicating about the program within one’s own organization. Restraining contextual factors were poor operational conditions, such as the time needed to mobilize relevant actors and discontinuity in representation of formal organizations in the community, resulting in change or abandonment of commitments and ownership (Figure 1).
CMO Configurations That Matter in Program Sustainability
Program sustainability was identified as a main outcome domain at program level, pursued by setting up ownership in established community-based organizations and by making efforts to meet contingent conditions regarding group size or number of groups. Generic contextual factors in support of program sustainability were past experiences, based on lessons learned from different projects, and alignment with related community-based initiatives in the area.
Generic contextual factors restraining program sustainability related to the lack of a shared belief in the added value of CBHEPA programs for organizational objectives, for example, because PA programs did not fit into core businesses. Furthermore, restrictions of subsidy schemes in place (in terms of goals, time frame, or content), lack of clarity on budgets available, and poor exercise trainer employment conditions were restraining factors. In particular, municipal or organizational policies focusing on pilot projects were found to restrain program sustainability. It was difficult to consolidate the activities developed in the pilot project because, in most cases, the expertize built up during the pilot phase (personnel, knowledge, and funds) moved away to a new area, leaving the pilot area empty (Figure 2). The need to be able to respond to contextual dynamics, in particular with reference to local and national policy developments and legislation on sport and PA promotion, was generally underlined.

Context–mechanism–outcome configurations on program sustainability: Setup ownership (O3) and expanding group(size)s (O4).
CBHEPA program F—Program coordinator: [Local] sports policy is very much financed in bits and pieces from different schemes. […] This runs from one scheme to the next. [This requires] connecting things and linking the dots, and becoming skilful in writing successful grant applications.
Setup of ownership in community-based organizations (O3)
Key supportive mechanisms for setting up ownership were a strong personal engagement and determination of the initiator (generally a project coordinator or exercise trainer), advocating for ownership in community-based organizations, and someone who is active and resourceful and involved in related community-based initiatives. Contextual factors in support of setting up ownership were national and/or local polices and arrangements for sport and PA promotion, justifying advocacy strategies used, and established collaborative structures at municipal level, underpinning trustful relationships among community-based actors involved.
Restraining mechanisms for setting up ownership were lack of arrangements for structural financing, withdrawal of available expertize and funding once a pilot had stopped, and policy uncertainties regarding the future for the programs.
CBHEPA program F—Exercise trainer: So they went to another area. They said like, okay, over there they need it more than over here […]. That is just a top-down decision that they made […] and I took it from there of my own accord and that all went well. But you should further build on at that point, really. But no, then it goes to someplace else and there it starts again.
Expanding group size or number of groups (O4)
Key mechanisms in support of expanding groups or group sizes were mainly personal communication (word-of-mouth spreading among participants’ social networks) and organizing joint activities with related community-based initiatives so as to link education or health themes with exercise classes. Other supportive mechanisms were the use of regular communication means and (social) media, extension of the area of recruitment beyond the original neighborhood or community targeted, and smart use of available funding and other resources. Supportive contextual factors were alignment with related community-based initiatives and a strong sense of community within neighborhoods usually based on sociocultural or ethnic background, family relations, or sport clubs connections.
Restraining mechanisms were the time and money required for ongoing recruitment actions and dropout of (groups of) participants for personal, programmatic, or financial reasons. Restraining contextual factors were organizational policies, stipulating a minimum number of participants per group for cost-recovery reasons, project-based way of working at the municipal level, implementing organization requiring ongoing efforts to raise funds, and increase in program fees or competing sport and PA initiatives in the area (Figure 2).
CMO Configurations That Matter in Intersectoral Collaboration
Intersectoral collaboration was found as a common denominator across CBHEPA programs and turned out to be a fluid concept in terms of CMO configurations. In all programs, intersectoral collaboration was identified as an overall mechanism to reach socially vulnerable groups of interest, to unite skills and resources to tailor programs to their needs, and as a strategy to actually find and bind participants. At the same time, intersectoral collaboration was identified as a time-related outcome, primarily in support of program sustainability. So, intersectoral collaboration is needed to get started but is perceived over time as a prominent outcome of a collective effort. We focused in our description of CMO configurations on the latter interpretation of intersectoral collaboration.
Generic contextual factors in support of intersectoral collaboration were integral community-oriented policy frameworks at municipal level to trigger and legitimize community-based action.
CBHEPA program D—Community actor: Why are we actually in this group together? That all has to do with the fact that we are involved in project X in H. For if we say: how do you rally these partners? Well, they have signed an agreement to develop activities in this neighbourhood, also with a view to exercise and healthy behaviour. So this has not just miraculously come about all by itself.
Generic contextual factors restraining intersectoral collaboration related mostly to national policies reshaping social welfare policies locally during the period of our investigation. The project-based approach to CBHEPA initiatives—found in most municipalities and implementing organizations—was mentioned as a restraining factor. This generated persistent program uncertainties and ongoing fund-raising efforts. These dynamic and uncertain conditions resulted in a lack of continuity in organizational representatives, a loss of qualified personnel, and poor exercise trainer employment conditions (Figure 3).
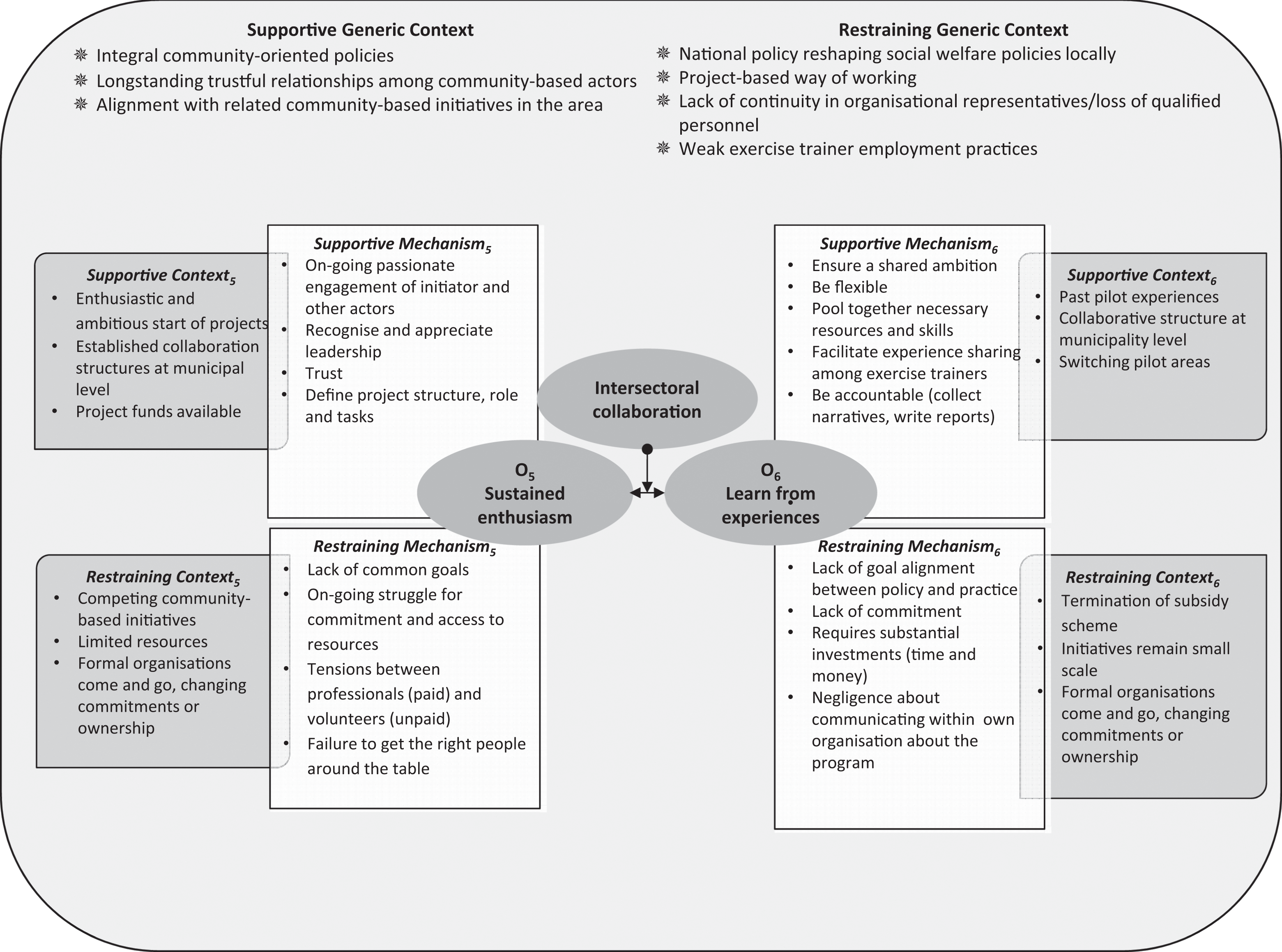
Context–mechanism–outcome configuration on intersectoral collaboration: Sustained enthusiasm (O5) and learn from experiences (O6).
Sustained enthusiasm of actors involved (O5)
Key supportive mechanisms to keep all actors enthusiastically involved were leadership—demonstrated by a respected and trusted enthusiastic and determined project coordinator or exercise trainer (or both)—and (taking) time to mobilize different parties in informal networks. Another supportive mechanism for the sustained enthusiasm of involved actors was defining together a more formalized project structure acknowledging different roles and tasks within the CBHEPA program. Supportive contextual factors related predominantly to the initial enthusiasm and ambition about the CBHEPA initiative, to existing and formalized collaborative structures (covenants), and to access to project funding.
Mechanisms restraining sustained enthusiasm were withdrawal of supporting actors (e.g., municipality, welfare organization), lack of collaboration due to lack of shared ambition or tensions about payments for time invested, running out of steam struggling for commitment, access to facilities and funding, and a failure to get the right people around the table. Restraining contextual factors were the limited resources available for community-based activities and the presence of many community-based initiatives in the area, creating the risk of competing over resources rather than reinforcing one another.
CBHEPA program A—Community actor: And that you actually find out then, that there is no clear structural pot of money available to draw from. So, in other words: you share the responsibilities, you share the worries, also regarding the target group here in district L. But, oh, the feeling of powerlessness that you get …. Yes, okay, so I can stay involved, so I can advise, I can act as a consultant, I can help think about things, but I do not really have any resources that I can pull or that I can open.
Learn from experiences to apply them elsewhere (O6)
Key supportive mechanisms for learning from experiences in order to apply them elsewhere were flexibility, ensuring a shared ambition by bringing together necessary resources and skills, and facilitating sharing of lessons learned among actors and exercise trainers. Furthermore, generating accountability on learning experiences by collecting narratives of individual success stories and/or writing accountability reports was found as a supportive mechanism. Supportive contextual factors for learning from experiences were existing collaborative structures at municipal level, past pilot experiences, and switching pilot areas.
The main restraining mechanism in most programs was the stand-alone position of most exercise trainers, executing their tasks autonomously at community-based sports venues. Other restraining mechanisms were a perceived lack of goal alignment between policy and practice, organizations withdrawing their staff and other resources (e.g., municipality or welfare organization) whenever new policies came into force, lack of commitment, negligence about communicating about the program within one’s own organization, and a failure to get the right people around the table. Restraining contextual factors were termination of subsidy schemes, resulting in program uncertainties, and the relatively small scale of most CBHEPA initiatives (Figure 3).
CMO Configurations That Matter in Enhancing Active Lifestyles
Enhancing participants’ active lifestyles was identified as the main outcome domain across all CBHEPA programs. All CBHEPA programs defined the aim of improving their participants’ daily PA levels and program adherence (retaining participants in their groups and preventing dropout). Generic contextual factors in support of enhancing participants’ healthy and active lifestyles were a personal drive/enthusiasm for, and a strong personal belief in, the benefits and power of PA and sport as a means to improve health and personal development. Additional supportive contextual factors were related community-based initiatives and long-standing trustful relationships among community-based actors/professionals, a strong sense of community within neighborhoods (based on sociocultural or ethnic background, or sport clubs), and past experience with sport and PA projects.
Generic contextual factors restraining enhancing participants’ healthy and active lifestyles, at organizational level, were a lack or loss of qualified personnel (e.g., resulting from organizational restructuring), poor exercise trainer employment conditions, and project-based approaches to CBHEPA programs. At participant level, cultural dispositions and habits played a role, for example, in migrant women’s groups, where male exercise trainers and/or professionals were not accepted (Figure 4).
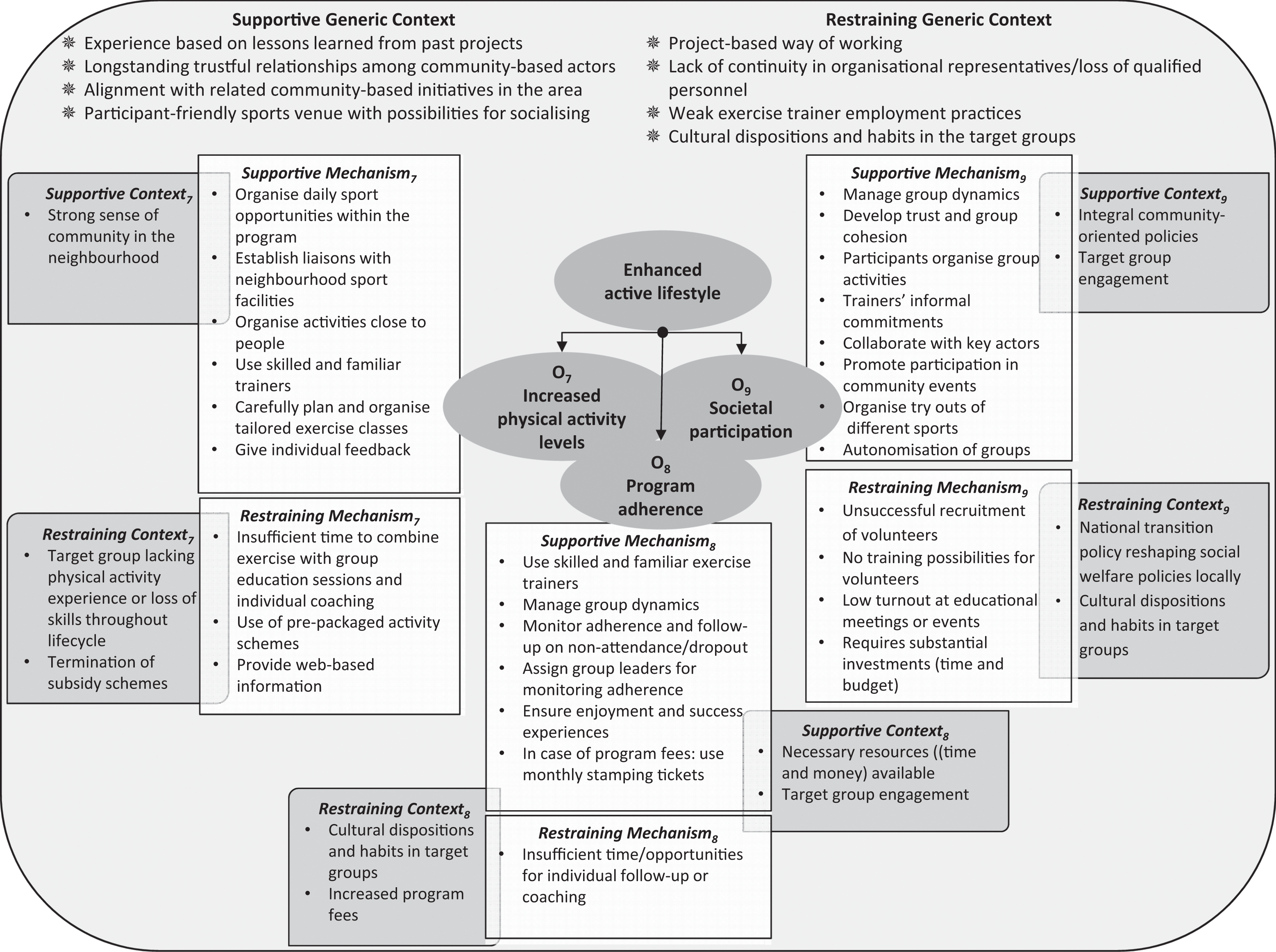
Context–mechanism–outcome configuration on enhanced active lifestyles: Increase physical activity (O7), program adherence (O8), and societal participation (O9).
Participants increase and maintain their daily PA levels (O7)
Key mechanisms supportive of participants’ increased and maintained daily PA level related to organizational aspects, such as organizing activities close to people, establishing liaisons with sport activities and facilities in the neighborhood, and providing for daily opportunities for sport and PA in the CBHEPA program. Other supportive mechanisms related to exercise trainer skills, such as use of experienced, professionally trained exercise trainers familiar with, and responsive to, the target groups’ vulnerabilities, and able to carefully plan and organize tailored exercise classes with a focus on enjoyment and individual feedback. Supportive contextual factors were a strong sense of community among participants and a participant-friendly sports venue with possibilities for socializing.
Mechanisms at program level restraining the increase and maintenance of daily PA levels were insufficient time to combine exercise with group education sessions and individual coaching, the use of prepackaged activity schemes, and the use of web-based information, which was perceived as expensive and not suited to the target group. Restraining contextual factors related to participant backgrounds, that is, lack of sport or PA experiences over their life span (e.g., in migrant groups) or loss of PA skills (e.g., the chronically ill or the elderly). Other restraining contextual factors related to sustainability issues such as the termination of subsidy schemes causing insecurities for future program activities (Figure 4).
Program adherence (O8)
Key mechanisms in support of program adherence were found mainly at the exercise trainer level. These involved actively monitoring adherence and undertaking actions in the event of nonattendance or dropout (e.g., phone call and home visit). Other supportive mechanisms were the assignment of group leaders in exercise groups to monitor adherence, active management of group dynamics (e.g., splitting groups according to PA skills), and ensuring enjoyment in PA and participants’ success experiences by supporting personal performance and body awareness in class. Use of a familiar, experienced, and professionally trained exercise trainer supports program adherence. In case of payment of membership fees, educating people to pay for sport and exercise and to use monthly stamping tickets to facilitate increased attendance were identified as supportive mechanisms.
CBHEPA program E—Exercise trainer: I think that [the reason] why people come to us is, that we are not really a gym, but rather a bit of welfare. We have combined things. The women are noted, we know them by name. You give them a ring if someone has not attended for a while, there is a great deal of care and attention around it all. More than, I do believe, at a usual, average gym.
Restraining mechanisms were insufficient time and opportunities for personal follow-up or coaching and lack of qualified personnel. Restraining contextual factors were increases in program fees and participants’ cultural dispositions and habits.
Societal participation through group exercise (O9)
Key mechanisms in support of societal participation through group exercise were also found mainly at the exercise trainer level. These involved actions at group level, such as managing group dynamics in order to develop trust and group cohesion and giving (moral) support to participation in community-based activities (e.g., neighborhood walks or sports events). Exercise trainers were also actively seeking collaboration with key actors in the community, organizing try outs of different sports, and helping groups to organize more autonomous group activities on their own initiative. Last but not least, exercise trainers often provided individual advice and material support. Supportive contextual factors were a participant-friendly sports venue with possibilities for socializing, integral community-oriented policies, and the exercise trainer’s commitment to, and engagement with, the target group.
Restraining mechanisms were a lack of volunteers and of possibilities for training volunteers on the one hand and a low turnout at community (educational) meetings or events on the other, resulting in a loss of interest in investing in these trajectories. Contextual factors restraining societal participation, at participant level, were differences in cultural dispositions and habits within groups and communities. At program level, competing interests between community-based organizations were mentioned, at times aggravated by policies reshaping local social welfare policies (Figure 4).
Discussion
In this study, we used realist synthesis to explore key combinations of contextual factors and mechanisms triggering outcomes of interest identified by CBHEPA program representatives. Using a realist protocol contributes to the clarification and elucidation of the multilevel nature of CBHEPA programs dealing with the everyday complexities of PA behavior within its socioecological contexts. Our findings indicate that outcomes of interest reach beyond enhancing participants’ active lifestyles; they also encompass a range of organizational and programmatic aims, such as improved community outreach, intersectoral collaboration, and program sustainability.
CBHEPA initiatives do not start from scratch; rather, they are generally entangled with related projects or collaborative structures. The key CMO configurations identified indicate that past experiences with sport and PA projects and commitment to the target group are strong supportive contextual factors, alongside the drive and responsiveness of competent exercise trainers as dominant mechanisms in sustained programs. Restraining factors relate mainly to lack of actor involvement, lack of project continuity, and trainers’ stand-alone position. On the basis of our findings, the program theory of CBHEPA programs is advanced by showing how passion for, and past experiences with, sport and PA as well as commitment to the target group are key contextualized factors triggering outcomes.
Our findings support the notion of contextual interdependencies. While developing our CMO configurations, we identified generic contextual factors of influence on main outcome domains alongside specific contextual factors, generating specific mechanisms in relation to specific outcomes of interest. In pooling these contextual factors together, our findings suggest a strong influence of national policies shaping local policy contexts for CBHEPA programs. We also found that, generally, program implementation was weakly tied to local policy and hardly embedded in established organizations (Figure 5). From an ecological perspective, there is an apparent need for a more systemic and systematic approach to making (planning) processes explicit. Planning and organizing CBHEPA programs call for specifying and matching of interventions at multiple levels, using theories to map specific interventions from prior research and practice, and pooling together experiences from prior projects and community-preferred interventions so as to patch theory-based best practices and fill gaps in the evidence base with practice-informed insights on what works best, and how, in a particular community (Green & Kreuter, 2005).
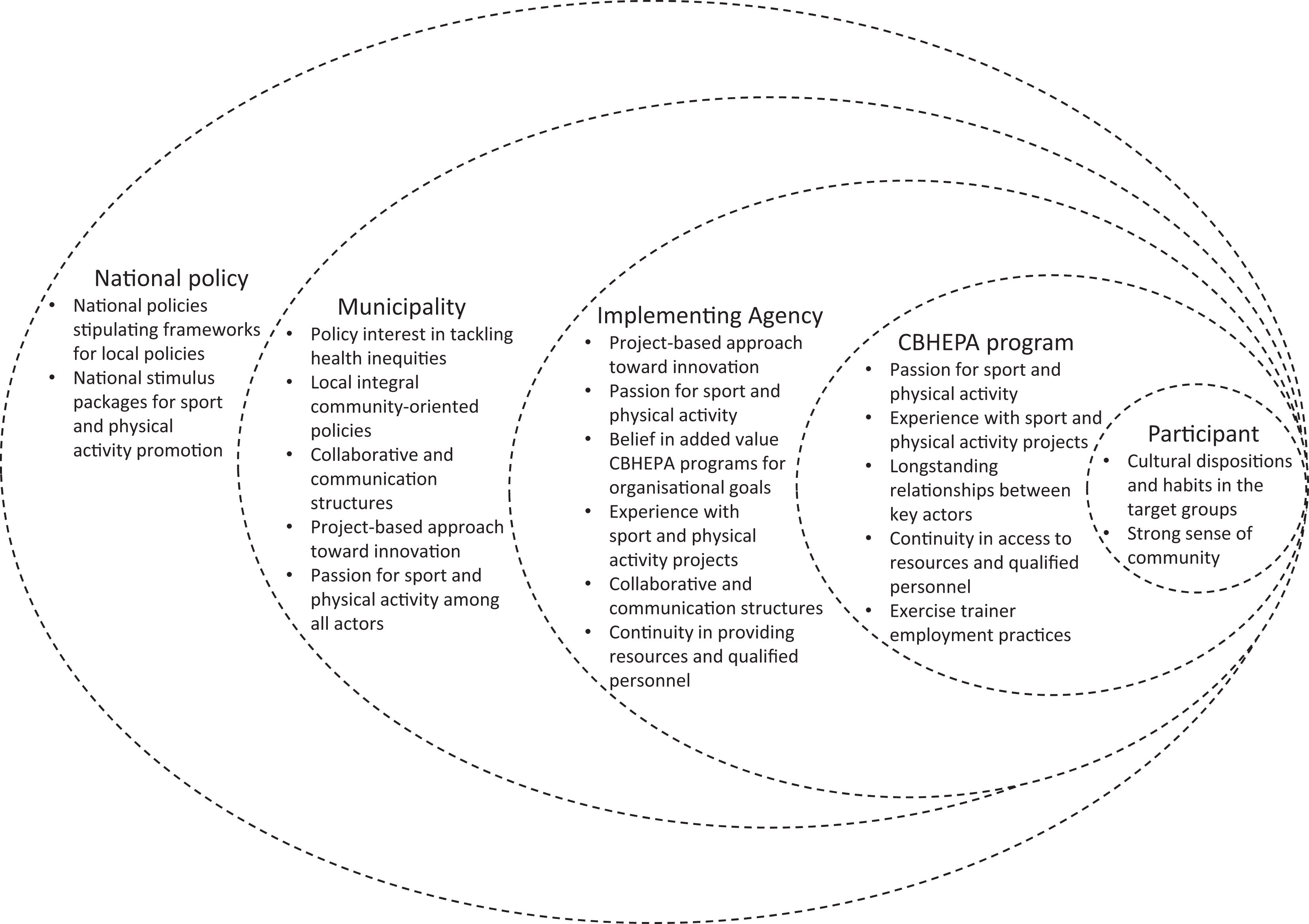
Contextual spheres of influence on community-based health-enhancing physical activity programs.
In open systems such as CBHEPA programs tackling PA inequities, the issue of context should not be interpreted as a purely external factor (Barnes et al., 2003). Context is both shaped by actors involved as much as it constrains their activities and refers to a “complex set of social actors intersect with socio-political structures to dynamically co-create contextual influences” (Edwards & Di Ruggiero, 2011, p. 43). George et al. (2015) indicate that contextual elements are dynamic and porous in nature, influencing programs as much as being influenced by programs (outcomes) because of the permeability of system boundaries (George et al., 2015). Therefore, in line with other studies, we found that there are multiple ways to define contexts, hence multiple ways of constructing CMO configurations (Byng et al., 2005). In addition, defining context in dialogue using narrative techniques contributed to a richness in retrospective and contextual understanding of developments in CBHEPA programs, highlighting how contextual factors have had an impact on program outcomes (Green & Kreuter, 2005; Naylor, Wharf-Higgins, Blair, Green, & O’Connor, 2002).
Our findings link up with ecological considerations in the scientific literature on the implementation of programs tackling health inequities. This literature highlights the importance of relationship development, collaborative problem solving, local knowledge and experience, and making community capacity development a goal (Trickett & Beehler, 2013). From an ecological perspective, implementation reflects a paradigm in which problem definition, intervention development, and implementation are viewed as emergent processes developed collaboratively and drawing on local history, culture, and resources. Consequently, program activities designed to affect specific health inequities are part of a broader, local, collaborative intervention process rather than merely putting an efficacious, predeveloped program into practice (Trickett & Beehler, 2013).
The outcomes of interest, identified by CBHEPA program representatives, reflect to a large extent the ecologic implementation paradigm. CBHEPA programs are generally profiled as a springboard to various neighborhoods and communities. Community outreach, in terms of reaching the target groups and organizational visibility, is usually perceived as an organizational responsibility legitimizing time, effort, and money spent on the program. According to a multilevel ecological rationale that underpins programs dealing with health inequities, however, community outreach as an outcome is about more than professional accountability only. It is a first indicator of developments in trust building and collaboration at community level. Intersectoral collaboration, defined as an outcome in terms of sustained enthusiasm and lessons learned, can also be viewed as a primary community-level outcome (Hawe, Shiell, & Riley, 2009). In dealing with health inequities, Trickett and Bheeler (2013) point out the importance of developing collaborative and empowering partnerships with relevant sectors of the community in intervention planning and implementation. This means including sectors not typically associated with health promotion but whose activities and policies may affect health inequities. They also point out the importance of setting community-level goals for capacity building as well as individual-level goals and highlight the value of making a long-term time commitment to local projects and communities involved (Trickett & Beehler, 2013).
Building and maintaining trustful relations were also key mechanisms in increasing output and anchoring program sustainability, in partnership longevity, in aligning with related projects or the launch of spin-off projects. This is in line with recent literature on realist synthesis in community-based participatory research (Jagosh et al., 2015). In conjunction with CMO configurations, Jagosh et al. (2015) show that spin-off projects, or ripple effects (Trickett & Beehler, 2013), serve as a framework to better understand how partnership activities accrue in stages, with the outcomes of one stage of the partnership life course informing or transforming the context for subsequent stages. The ripple effect concept is premised on the idea that community-based participatory (research) activity is a series of “events in the history of a system, leading to the evolution of new structures of interaction and new shared meanings” (Hawe et al., 2009, p. 267).
Our findings also indicate that there is ample support for program sustainability from formal policy or funding arrangements, aggravated by local policy preferring project-based approaches. There appears to be a tension between, on the one hand, municipal policies and administrative and/or legislative measures in place and, on the other, the ecological rationale of multilevel interventions necessary to tackle health inequities. In Dutch local politics and policies, the drive for accountability on expenditures becomes manifest in the preference for project-based approaches, suggesting well-defined value-for-money trajectories. Multilevel interventions addressing health inequity, however, require allowable resources for activities such as partnership and relationship building and plans for sustaining long-term support within communities (Trickett & Beehler, 2013) often not covered and hardly studied in the culture of local governance (Barten et al., 2011).
Enhancing participants’ active lifestyles, defined in terms of increased PA levels, program adherence, and societal participation, is the ultimate outcome that CBHEPA programs seek to achieve. Serving socially vulnerable groups with PA programs tailored to their needs is perceived as their raison d’être. Our findings indicate that programs predominantly thrive on highly dedicated individuals. A key factor triggering outcomes is the crucial role of responsive leadership of the exercise trainer. This is in line with other studies indicating that professional qualifications, bonding with participants and managing group dynamics to demonstrate collective accomplishments, extend leadership requirements beyond the traditional technical performance and individual feedback in PA classes and include activities of social integration and societal participation (Estabrooks et al., 2004; Herens, Wagemakers, Vaandrager, & Koelen, 2015).
Methodological Reflections
Methodological issues in our study relate to data collection and analysis. Use of narrative techniques, in particular the timeline technique, generated actor-driven data. The timeline technique was particularly appreciated by participants—“much better than just talk”—and generated fruitful discussions on identifying what actually happened over time. The timeline technique builds on techniques for organizational and intercultural learning (Brunton & Jeffrey, 2010; Davis, 2006; Flanagan, 1954; McAllister, Whiteford, Hill, Thomas, & Fitzgerald, 2006). Participants often photographed the outcomes so as to take home a message, indicating that they valued the outcomes of the session. Conducting timeline sessions does, however, require good facilitating skills to manage the group dynamics and watch over the process of sense making of the actor-driven retrospective recollection of events and the determination of their significance. We cannot rule out the possibility that decisive events went unnoticed because of lack of knowledge or awareness or because of power imbalances within the focus groups.
Our study indicates that realist synthesis contributes to evidence-informed theorizing about how and in what circumstances CBHEPA programs work. The body of literature on the application of realist evaluation principles in health-related research is still relatively small and shows considerable diversity in its use (Coryn, Noakes, Westine, & Schröter, 2011; Marchal et al., 2012). We found that using a realist protocol in a longitudinal design was challenging for several reasons. In line with other authors (Astbury & Leeuw, 2010; Byng et al., 2005; Coryn et al., 2011; Jackson & Kolla, 2012; Jagosh et al., 2015; Marchal et al., 2012), we found that time, place, and actor perspective define CMO configurations and therefore are dynamic by nature. The question of what constitutes a mechanism was also a challenge (Astbury & Leeuw, 2010; Marchal et al., 2012). Our findings suggest that a mechanism can mutate over time and become a contextual factor. For example, enthusiasm and shared ambition were found as driving mechanisms to mobilize the necessary people, skills, and resources at the start of each CBHEPA program, whereas after some time, the efforts put into the maintenance of enthusiasm and involvement became the dominant mechanism. Jagosh et al. (2015, 2014) describe similar findings relating to the phenomenon of trust development.
In the literature, some argue that realist evaluation is useful for dealing with complexity issues in multilevel programs. Others believe that it is less suitable for evaluation of multisite programs made up of different interventions aiming at multiple outcomes because of the underlying reasoning of realist evaluation, in which contexts shape the conditions for mechanisms and outcomes to occur (Blamey & Mackenzie, 2007; Marchal et al., 2012). We acknowledge that our approach of synthesizing findings across multiple cases in favor of building conceptual robustness ties in with this dilemma. Nevertheless, we believe that, with reference to our findings on generic contextual factors, abstracting to some extent contributes to a better understanding and interpretability of identified CMO configurations.
Our sample consisted of actors involved in CBHEPA programs selected by local project leaders or initiators. Participation was on a voluntary basis. Consequently, we had to rely on the selection and recommendation of our local partners; this may have created bias in the sample in favor of participants most involved and enthusiastic about CBHEPA initiatives. Therefore, our findings relating to contextual factors, such as lack of continuity in actor involvement and mechanisms highlighting efforts to keep the right people around the table and actively involved, cannot simply be extrapolated to those actors who left the collaboration or (for whatever reason) refrained from participation, as we did not interview them.
Conclusion
CBHEPA programs do not start from scratch and are generally entangled with related community-based projects. Based on practice-informed theorizing using realist synthesis, our study provides an elaboration on existing program theories for CBHEPA programs, showing how actors’ passion for, and past experiences with, sport and PA as well as commitment to the target group were key factors triggering outcomes alongside exercise trainers’ responsive leadership skills. As of yet however, local governance structures appear often to lack the necessary adaptive capacity to accommodate the interactive processes and mobilize the resources needed at multiple levels to realize sustained CBHEPA program activities.
Footnotes
Acknowledgment
The authors would like to express their appreciation to the experts who peer reviewed this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by ZonMw, the Netherlands Organization for Health Research and Development (Project number: 50-51505-98-103) awarded to Annemarie Wagemakers. The Netherlands Institute for Sport and Physical Activity (NISB) developed the Communities on the Move program and is the collaborating agency.