
Abstract
Placental weight (PW) is a measure commonly used to summarize growth and aspects of placental function. In a normal pregnancy, it is reasonable to assume that PW is related to aspects of the functional capacity of the placenta. The placenta, as the site for all maternal–fetal oxygen and nutrient exchange, influences birth weight and is thus central to a successful pregnancy outcome. PW is the most common way to characterize placental growth, which relates to placental function. With physical exercise becoming an integral part of life for many women, the question of whether exercise during pregnancy has an adverse effect on the growing fetus is very important. The aim was to examine the influence of an aerobic exercise program throughout pregnancy on PW among healthy pregnant women. A randomized control trial was used (registration trial number: NCT02420288). Women were randomized into an exercise group (EG; n = 33) or a control group (CG; n = 32) that received standard care. The EG trained 3 days/week (55–60 min/session) from gestational Weeks 9–11 until Weeks 38–39. The 85 training sessions involved aerobic, muscular and pelvic floor strength, and flexibility exercises. PW and other pregnancy outcomes were measured. There was high attendance to the exercise program, and no differences in the PW at delivery were observed between study groups (CG = 493.2 ± 119.6 g vs. EG = 495.4 ± 150 g, p = .95). A regular, supervised exercise program throughout pregnancy does not affect the PW in healthy pregnant women.
In the past three decades, an increasing amount of evidence has been published on the clinical significance of placental weight (PW) and its long-term effects on health and disease in adult life (Almog et al., 2011; Naeye, 1987; Pardi, Marconi, & Cetin, 1997; Thornburg, O’Tierney, & Louey, 2010). Furthermore, the placenta metabolizes and absorbs nutrients; thus, it is more than a passive conduit. Nutrient transport should be considered a staple of the normal exchange between the maternal body and fetal environment (Hay, 1994).
PW is a measure commonly used to summarize growth and aspects of placental function. In a normal pregnancy, it is reasonable to assume that PW is related to aspects of the functional capacity of the placenta (Salafia, Charles, & Maas, 2006). In fact, to a large degree, the placenta translates how the fetus experiences the maternal environment and, genetic influences aside, is the principal influence on one of the most important pregnancy outcomes: the weight of the newborn (Godfrey, 2002; Salafia et al., 2008; Thame, Osmond, Bennett, Wilks, & Forrester, 2004; Thame, Osmond, Wilks, Bennett, & Forrester, 2001).
Many studies indicated that PW was related to pregnancy outcome (Eskild, Romundstad, & Vatten, 2009; Roland et al., 2012; Shehata et al., 2011). High placenta weight was associated with a poor perinatal outcome, a low Apgar score, respiratory distress, and perinatal death, whereas a low PW was associated with medical complications of the mother. To determine high and low PW, above and below the 10th and the 90th percentiles, respectively, are used (Janthanaphan, Kor-Anantakul, & Geater, 2006). Placentas over 750 g and less than 350 g are unlikely to be normal (Kaplan, 2008). Also, both small and large placentas relative to birth weight (BW) were associated with fetal death in preterm births (Haavaldsen, Samuelsen, & Eskild, 2013).
The idea that PW is an expression of the intrauterine environment is supported by numerous studies (Godfrey, 2002; Haavaldsen et al., 2013; Hendricks, 1964; Salafia et al., 2008). Environmental challenges that disrupt maternal life will impact the fetal environment and transmit across the placenta. The placenta responds to alterations in the maternal–fetal exchange with a wide range of structural and functional changes such as race, socioeconomic problems, or health problems (Perry, Beevers, Whincup, & Bareford, 1995), including changes in PW (Baptiste-Roberts et al., 2008; Fowden, Forhead, Coan, & Burton, 2008; Jansson & Powell, 2007; McNamara, Hutcheon, Platt, Benjamin, & Kramer, 2014).
Thus, maternal factors known to influence fetal growth, BW, and neonatal body composition are also important determinants of PW (Roland et al., 2012). Because certain studies have shown that physical exercise could influence BW (Baciuk, Pereira, Cecatti, Braga, & Cavalcante, 2008; Barakat et al. 2016; Hopkins, Baldi, Cutfield, McCowan, & Hofman, 2010; Ruiz et al, 2013), it is interesting from the scientific point of view to examine the effects of supervised and regular exercise throughout pregnancy on PW.
In this sense, although many studies about the impact of exercise during pregnancy on PW exist (Bergmann, Zygmunt, & Clapp, 2004; Clapp, 2003; Clapp, Kim, Burciu, & Lopez, 2000; Hilde, Eskild, Owe, Bø, & Bjelland, 2017), this relationship has not yet been studied by any Randomized Clinical Trial (RCT).
The aim of the present study was to examine the influence of an exercise program throughout pregnancy on PW among healthy pregnant women.
Based on a previous study (Juhl, Olsen, Andersen, Nøhr, & Andersen, 2010), we hypothesized that maternal exercise would decrease PW.
Material and Method
The present RCT (registration trial number: NCT02420288) was conducted between January 2014 and January 2016 following the ethical guidelines of the Declaration of Helsinki that was last modified in 2000. The research protocol was reviewed and approved by the Hospital Universitario de Torrejón (Madrid, Spain).
We contacted a total of 92 Spanish pregnant women (who descended from three or more generations of Caucasians) from the consultant obstetrician hospital. Only women without any obstetric complications according to the American College of Obstetricians and Gynecologists guidelines (ACOG, 2015) with a singleton gestation and who were not participating in any other trials or exercise programs at the moment of inclusion and throughout pregnancy were invited to participate in this study.
For practical reasons, women who were not planning to give birth at the same obstetric hospital department (Hospital Universitario de Torrejón, Madrid, Spain) and who did not receive medical follow-ups throughout the entire pregnancy period were not included in the study. We also excluded women who had any serious medical conditions that would have prevented them from exercising safely (i.e., long-term muscle injuries). All of the participants provided signed written informed consent prior to participating in the study.
A simple randomization process was used to allocate the study participants. A computer-generated list of random numbers was used to allocate the participants into two groups: exercise and control. The randomization and blinding (sequence generation, allocation concealment, and implementation) were performed by three different authors.
Exercise Intervention
The exercise program was designed following the ACOG (2015) guidelines to ensure that it was safe and effective for pregnant women and included a total of three 55–60 min sessions, performed 3 times per week on alternate days, which lasted from the beginning of the pregnancy (Weeks 8–11) until the end of the third trimester (Weeks 38–39). An average of 85 training sessions was planned. Each exercise session was preceded and followed by a gradual warm-up and cooldown period (both 10- and 12-min duration) and consisted of walking and light static stretching of most muscle groups. The cooldown period included relaxation exercises.
The women wore heart rate monitors (Accurex Plus, Polar Electro OY, Finland) during all sessions to meet the intensity target of 55–60% of their heart rate reserve using the Karvonen equation (Goldberg, Elliot, & Kuehl, 1988). Borg’s Rate of Perceived Exertion Scale was also used and ranged from 10 to 12 (fairly light to somewhat hard, respectively; O’Neill, Cooper, Mills, Boyce, & Hunyor, 1992). During the first week of the program, the pregnant women received a complete explanation and practice of the Borg’s scale in order to gain familiarity with this instrument.
After the warm-up, the women participated in different activities, the main objective of which was to reach and hold 55–60% heart rate reserve of intensity for 20–25 min. To achieve this goal, aerobic exercises consisted of low-impact aerobic dance, involving the upper and lower limbs using different musical style choreography. Some specific exercises were then performed to increase muscle strength and to improve balance and to prevent some muscle imbalances that are common among pregnant women (pectoral, back, shoulder, and upper and lower limb muscles). Exercises were performed through the full range of motion. One set (10–12 repetitions) was conducted using barbells (2 kg/exercise) or low-to-medium resistance (elastic) bands (Therabands) and included biceps curls, arm extensions, arm side lifts, shoulder elevations, bench presses, seated lateral row, lateral leg elevations, leg circles, knee extensions, knee (hamstring) curls, and ankle flexions and extensions. The session also included 10 min of pelvic floor muscle training to prevent urinary incontinence.
Extreme stretching, joint overextension, the Valsalva maneuver, ballistic movements, and jumps were avoided, and exercises performed in the supine position on the mat were not performed for more than 2 min.
To maximize program safety, adherence, and efficacy, all sessions were (i) supervised by a qualified fitness specialist (working with groups of 10–12 subjects) and with an obstetrician’s assistance, (ii) accompanied by music, and (iii) performed in the Health Care Center in a spacious, well-lit room under favorable environmental conditions (altitude = 600 m, temperature = 19–21°C, and humidity = 50–60%). An adequate intake of calories and nutrients was confirmed before the start of each exercise session.
Usual Care (Control) Group
Women randomly assigned to the usual care (control) group received general advice from their midwife about the positive effects of physical activity. Participants in the usual care group had their usual visits with health-care providers (midwives, obstetricians, and family doctors) during pregnancy at a frequency equal to the exercise group (EG). The women were not discouraged from exercising on their own. They reported no regular exercise during their pregnancies (telephone interviews).
Outcome Measurements
Demographic information was obtained at admission to the study. Medical history and pregnancy outcomes were obtained from medical records. The women’s weight and height were measured at admission following standard procedures. Body mass index (BMI) was calculated as weight (kg)/height (m2), and the women were classified as underweight (BMI < 18.5 kg/m2), normal weight (BMI ≥ 18.5–24.9 kg/m2), overweight (BMI ≥ 25–29.9 kg/m2), and obese (BMI ≥ 30 kg/m2; Institute of Medicine [IOM], 2009).
Primary outcome
The placentas were always weighed with the membranes and 1 cm of umbilical cord attached by the same specialists (three midwives). All the placentas were weighed during the first 30 min after delivery, an electronic scale was used (NAHITA 5041/5000, weight range 0–5,000 gr).
Secondary outcomes
Other maternal and fetal outcomes, such as gestational age, type of delivery (natural, instrumental, or caesarean), BW, Apgar score (at 1 and 5 min), gestational diabetes, and hypertension, were obtained from perinatal obstetric records. Gestational weight gain was classified according to the 2009 IOM guidelines. The recommended weight gain for underweight, normal weight, overweight, and obese women are 12.5–18 kg, 11.5–16 kg, 7–11.5 kg, and 5–9 kg, respectively (IOM, 2009).
Statistical Analysis
The comparison between treatment groups was performed with Student’s t test for unpaired data and the χ2 test for continuous and nominal data, respectively. We performed all of our analyses using the intention-to-treat principle (Detry & Lewis, 2014), if the outcome value was missing for a participant (lost to follow-up), then we inserted the mean value for that outcome.
Regarding the calculation of sample size, we used a conservative approach. We performed a power calculation for the primary outcome, PW, assuming a bilateral alternative and considering a standard deviation of 89 g based on a previous study (Janthanaphan et al., 2006). Additionally, we wanted to detect differences in PW of at least 70 g with a power of >80% and α of .05. Assuming a maximum loss at follow-up of 15%, we decided to recruit at least 30 participants for each study group.
The statistical analyses were performed with the Statistical Package for Social Sciences software (Version 20.0 for Windows; SPSS Inc., Chicago, IL). The level of significance was set to α = .05.
Results
There were no major adverse effects and no major health problems observed in the participants. In the control group (CG), a total of eight women were lost to follow-up due to the threat of a premature delivery (n = 2), a move to another hospital (n = 3), or personal reasons (n = 3). In the EG, a total of three women were lost to follow-up due to the threat of a premature delivery (n = 1), discontinued intervention (n = 1), or personal reasons (n = 1). However, due to the intention-to-treat, the final number of participants included in the analysis was 32 in the CG and 33 in the EG (Figure 1). No participants changed from one group to the other, and there were no protocol deviations from the study plans. Adherence to the training program was >85% in the experimental group that was measured by a qualified fitness specialist using a checklist of attendance for each session.

Flow chart of study participants.
The baseline maternal characteristics of both study groups are shown in Table 1. We found no significant differences (p > .05) between the groups in maternal characteristics that could potentially influence the main study outcome, PW.
Maternal Characteristics.

Note. Data are expressed as the mean ± standard deviation unless otherwise indicated. We analyzed continuous and nominal data with Student’s t test for unpaired data and the χ2 test, respectively. BMI = body mass index at the beginning of the study; EG = exercise group; CG = control group.
Table 2 shows no differences in the PW at delivery (CG = 493.2 ± 119.6 g vs. EG = 495.4 ± 150 g, p = .95) and other pregnancy outcomes between the study groups. In the CG, 5 (15.7%) women presented low, 26 (81.2%) women presented normal, and 1 (3.1%) presented with high PWs, respectively. In the EG, the number with low PW was 4 (12.1%), 26 (78.8%) had normal weight, and 3 (9.1%) had high PWs (p = .57). Also, regarding the PW:BW ratios, we found no differences between the groups (CG = 0.158 ± 0.03 vs. EG = 0.157 ± 0.03, p = .96). When we examined the maternal weight gain (MWG) during pregnancy, we also observed no statistical differences between the groups regarding total weight gain (CG = 11.8 ± 4.8 kg vs. EG = 10.9 ± 2.7 kg) and the number of women who exceeded their recommended weight gain during pregnancy according to their previous BMI (CG = 8/25% vs. EG = 4/12.1%; p = .43 and p = .18, respectively).
Primary and Secondary Outcomes of the Study Groups.
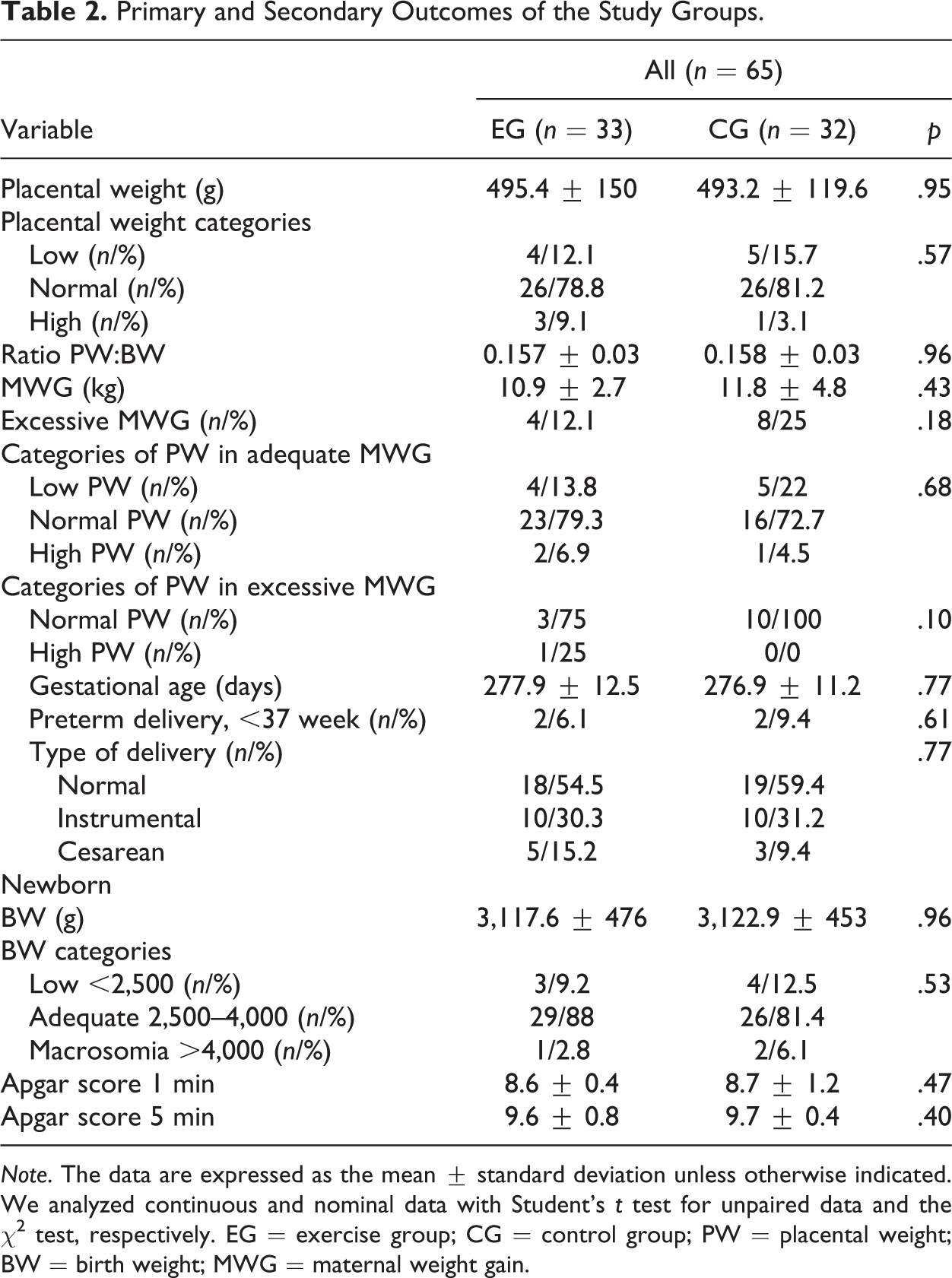
Note. The data are expressed as the mean ± standard deviation unless otherwise indicated. We analyzed continuous and nominal data with Student’s t test for unpaired data and the χ2 test, respectively. EG = exercise group; CG = control group; PW = placental weight; BW = birth weight; MWG = maternal weight gain.
Additional analysis examining the placenta weight categories (low/normal/high) in relation to MWG during pregnancy (adequate/excessive) also showed no significant differences.
Discussion
The aim of the present study was to examine the effects of an exercise program during pregnancy on PW among healthy pregnant women. The main finding of our study was that supervised, moderate exercise training performed throughout pregnancy (85 training sessions in total) does not negatively affect PW. Furthermore, the overall health status of the newborn was unaffected as reflected by the results of the widely used Apgar score.
An additional novelty of our study was that the exercise program integrated light resistance, toning, aerobic dance, and pelvic floor exercises, which was easily incorporated into a structured exercise regime for pregnant women. The variety of activities of this program focuses its effects on the modifications that the pregnancy process generates and decreasing the discomforts of pregnant women. It seems that this program was highly liked by the pregnant women as indicated by the high rate of adherence. To our knowledge, this is the first controlled, randomized trial that objectively and specifically shows no cause–effect relationship between supervised, regular exercise and PW.
The main interest of this study was on the influence of exercise on PW because the placenta plays a major role in fetal nutrition and fetal growth, as nutrients from the maternal circulation need to be transported (across the placenta) to reach the fetal circulation environment (Baumann, Deborde, & Illsley, 2002).
In an observational and prospective study, Salafia et al. investigated seven maternal characteristics (age, height, weight, parity, socioeconomic status, smoking, and race) and determined whether their known associations with BW were mediated by placental markers. The authors reported that all of the maternal characteristics except smoking were mediated by placental characteristics (Salafia et al., 2008).
Other external factors, such as maternal life stress (Tegethoff, Greene, Olsen, Meyer, & Meinlschmidt, 2010) or prepregnancy nutritional status and maternal diet during pregnancy (Thornburg et al., 2010), have been associated with PW.
In a prospective longitudinal study, Roland et al. (2014) found that maternal factors known to influence fetal growth and newborn outcomes (BW and neonatal body composition), such as maternal BMI, gestational weight gain, or fasting glucose, are determinants of PW.
In an experimental study (in which the authors did not clarify whether it was an RCT), Ramirez-Velez et al. (2013) reported that during the second half of pregnancy, regular exercise increased endothelial nitric oxide synthases expression and nitric oxide production and decreased reactive oxygen species generation in the human placenta. The authors expressed that increased endothelial shear stress may contribute to the beneficial effects of exercise on the vascular and antioxidant system and, in turn, reduce the risk of preeclampsia, diabetes, or hypertension during pregnancy (Ramírez-Vélez, Bustamante, Czerniczyniec, Aguilar de Plata, & Lores-Arnaiz, 2013).
The known influence of exercise on maternal and fetal outcomes (Barakat et al., 2016; Perales et al., 2016; Ruiz et al., 2013) suggests that physical exercise during pregnancy would influence the weight of the placenta. In fact, the circulatory changes caused by exercise (i.e., redistribution) may disrupt the normal flow of maternal blood to the uteroplacental area (Mottola, 2013; Veille, 1996) and thereby alter the normal development of the placenta. However, our results regarding PW and PW:BW ratio do not support the idea of this disruption (or other effects) caused in theory by physical exercise and therefore informed the nonconfirmation of our initial hypothesis. This could be due to the disruptions mentioned above being generated by higher intensity exercise. Clapp, Kim, Burciu, & Lopez (2000) suggested that exercise performed at moderate to high intensity influences fetal–placental growth and the effects depend on the frequency, duration, and intensity of exercise sessions; moreover, the different types of maternal carbohydrate intake and the relative amount of exercise (in late pregnancy) influence late fetal growth (Clapp, 2003). In our study, the exercise was more of a moderate intensity throughout pregnancy, rather than high intensity, and this may have allowed the placenta to adapt to the exercise and thus no effects were seen that disrupted fetal or placental growth. Recent scientific evidence supports the idea of exercise of moderate intensity throughout pregnancy to achieve maternal and fetal benefits without associated risks (Perales, Artal, & Lucia, 2017).
The main limitation of the present study was that we were unable to measure factors that could influence the primary outcome, such as nutritional status, daily time in standing, or PW of previous deliveries (if any). We conclude that a regular, supervised exercise program throughout pregnancy does not affect the PW of healthy pregnant women.
We believe that there exists a significant gap in this scientific topic. Our results supplement an important portion of the scientific literature that studies the relationship between exercise and pregnancy. We believe that more clinical trials with large samples sizes are needed by examining other factors such as psychic, emotional, or nutritional. In addition, it would be interesting to study the relationship between the PW and the relationship between the PW and “child growth.”
Footnotes
Acknowledgments
The authors would like to acknowledge the technical assistance of the Gynecology and Obstetrics Service of Torrejón Hospital, Madrid, Spain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Technical University of Madrid (UPM), Spain (AL16-PID-15).