
Abstract
Medical researchers frequently need to collect blood samples from study participants. The determination of whether and how much compensation to provide to the participants is challenging. Institutional review boards typically allow researchers to provide a compensation that reimburses participants for their time and effort but is not so large as to be coercive. Using a randomized controlled trial, we estimate parents’ responsiveness to financial compensation in terms of their willingness to provide their child’s blood sample. We find that an additional dollar of compensation raises the willingness to provide a child’s blood sample by about 0.5 percentage point at a base of 65%. This corresponds to an elasticity of .33. Using the findings, we provide general guidance on how compensation can be structured to strike a balance between appropriate compensation for participation and coercion.
Background
The practice of compensating research participants for their participation in scientific research in the United States goes as far back as the early 19th century (Grady, 2005). In the past few decades, various approaches for determining appropriate compensation have been documented (Dickert & Grady, 1999; Grady, 2005; Saunders & Sugar, 1999), as has the evidence on the motivational effect of financial compensation (see Tishler & Bartholomae, 2002, for a review). Dickert and Grady (1999) evaluate three models on the determination of compensation for research participation. In the first model, the market model, researchers provide incentives to the participants in exchange for complying with the study protocols such as tests and procedures. In the second model, the wage-payment model, compensation is provided to offset the participant’s cost of time and effort. According to this model, participants should be paid a low, standardized hourly wage that can be increased if the participants need to endure uncomfortable procedures or possible adverse side effects. Finally, in the reimbursement model, participants should be reimbursed for expenses they incur, such as the cost of transportation. There is no consensus on which model is the most ethically appropriate (Tishler & Bartholomae, 2002).
The ethical issues surrounding whether to and how much financial compensation to provide have also been documented. Although an extensive discussion of the debates is beyond the scope of this article, we summarize the key points here (see Permuth-Wey and Borenstein 2009; Ripley 2006, for a review). Briefly, the primary reasons in favor of offering financial compensation to research participants include ensuring an adequate number and types of participants and offsetting the costs of participation the participants face (Dunn & Gordon, 2005). Arguments against financial compensation mainly relate to the effect the compensation may have on the participant. For example, compensation may exert undue influence (Bentley & Thacker, 2004), may be coercive, and perpetuate inequity by adversely affecting the economically disadvantaged population disproportionately (McNeill, 1997; Wilkinson & Moore, 1999).
Despite the extensive documentation of the ethical issues to determine compensation, the amount paid to research participants varies widely. Grady, Dickert, Jawetz, Gensler, and Emanuel (2005) review 467 studies offering compensation to research participants and find that the amount of compensation ranged from US$5 to US$2,000. Variation in amounts occurred in similar studies, in the same multisite study at different sites, and for similar procedures across studies sometimes even within one site. Such variation has been reported in other studies as well (Borzekowski, Rickert, Ipp, & Fortenberry, 2003; Latterman & Merz, 2001).
In response, there have been efforts to establish benchmarks for the amount of compensation. For example, Dominguez, Jawara, Martino, Sinaii, and Grady (2012) make use of data from research conducted at the National Institutes of Health Clinical Center and the “inconvenience units” assigned to each study by the investigators and estimate the amount of compensation that researchers should provide research participants for a number of procedures such as a blood draw, MRI scan, or clinic visit.
Research involving children require additional considerations beyond those required for research on adults (Diekema, 2006, 2009). In addition to ensuring ethical standards, identifying an appropriate amount of compensation in research involving children is difficult. Researchers need to seek consent from their parents and provide compensation to them. However, participation in the research requires both parents’ and children’s time and effort and both may experience discomfort. The parents’ decision on whether to agree to participate on behalf of the child depends on the relative weights that they place on these costs and the compensation. For the children, money is an important measure of importance and independence and can cloud judgment (Ramsey, 2006). Adolescents may be less risk averse than adults and may minimize the potentially harmful consequences of a risk-taking behavior (Cohn, Macfarlane, Yanez, & Imai, 1995). Scherer et al. (2005) provided seven different research protocols to adolescents with asthma and their parents and asked them to provide estimates of a fair compensation for their participation in those studies. They find that the estimates were lower for adolescents than their parents. In general, several studies (Abramovitch, Freedman, Henry, & Van Brunschot, 1995; Susman, Dorn, & Fletcher, 1992) suggest that adolescents are limited in their ability to correctly identify risks and benefits from participation in a research.
A major gap in the current literature—on research involving children in particular but also on the use of financial compensation generally—is on the effect of a change in financial compensation offered to research participants on their decision to participate. Economic theory dictates that a higher compensation increases participation as it helps offset the opportunity cost of time and other barriers such as discomfort from participation. But we know little about the magnitude of this effect. For blood draw, for example, the benchmark that Dominguez et al. (2012) provide is US$20. We do not know how the participation rate would change, if the researchers provided, say, US$15 or US$30.
To fill this gap, we conducted a randomized controlled trial (RCT), which allows us to draw a causal link from financial compensation to research participation. Specifically, we varied the amount of financial compensation offered to prospective research participants. A measure of the response to an additional dollar—the elasticity—derived from this study is critical from a practical point of view. For example, researchers can use the number to determine the amount of compensation they should provide to obtain a certain participation rate or the number of participants they need to approach in order to ensure their required sample size at a given amount of compensation. Likewise, the institutional review boards (IRBs) can use the information to set limits on the amount of compensation for common interventions such as a blood draw that was used in this study.
Study Design
Our RCT was a part of a larger study: the University of Michigan Healthy Families Project (Healthy Families). Healthy Families was an interdisciplinary project that explored multiple aspects of a child’s biology, diet, physical activity, and environment. The goal was to better understand the biological, behavioral, and environmental contributors to child obesity risk, which in turn would help generate tailored interventions for parents to better guide their children through healthy growth and development. The project collected data from 132 parent–child dyads (only one child from each family) within a 1-hr driving radius of Ann Arbor, MI.
Families were recruited from the community through an obstetrics registry, a university-affiliated clinical research website, and flyers in community sites and pediatric primary care clinics. Interested families contacted the research team to complete a phone screening to determine eligibility. Inclusion criteria were that children were between the ages of 12–24 months (toddler), 3–5 years (preschool), and 10–12 years old (school age) and were not outside of the parents’ direct care for greater than 15 hr per week (toddler and preschool age-group); at least one biological parent lived in the home with child; child lived in only one home at least 5 of 7 days of the week; family spoke English at home most of the time; child did not have any major medical problems or developmental delays; child had no significant dietary restrictions that could impact growth or eating; and child was born at gestational age of 36 weeks or more. The University of Michigan’s IRB approved the study (HUM00079730).
When the research staff visited the families during a 6-month follow-up of the Healthy Families study, they offered the family the opportunity to volunteer for an ancillary study requiring that the child’s blood be drawn. Ensuring that the study complied with the University of Michigan’s IRB, the researchers offered the compensation to the families in a noncoercive manner and used a standardized text. We sought to draw blood samples from children in the three age-groups. The child’s age determined whether and what type of assent was obtained. Of course, the 12- to 24-month-old children were not able to provide assent. Preschool children provided verbal assent after the research assistant explained what would happen in an age-appropriate manner. Documented, written assent was obtained from the school-age children. The research assistant reviewed the assent document with the child and explained all that it entailed. The child’s signature on the assent document indicated his or her agreement to participate in the study. In all cases, parents also provided written informed consent.
Compensation was primarily provided to the parents, except in case of school-age children in which case it were offered either to the parents or to the child. We randomized the amount of the compensation and the recipient as shown in Figure 1. Parents were offered US$15, US$30, or US$60. Parents of toddlers and preschool children were also provided a teddy bear (costing US$7). In families with a child in the school-age group, we further randomized the recipient in a subset of families, we offered the compensation directly to the child instead of the parent (after seeking the parents’ approval first). The compensation provided to the families and the family’s responses constitute, respectively, the key explanatory variable and the outcome variable of interest in answering the research question.
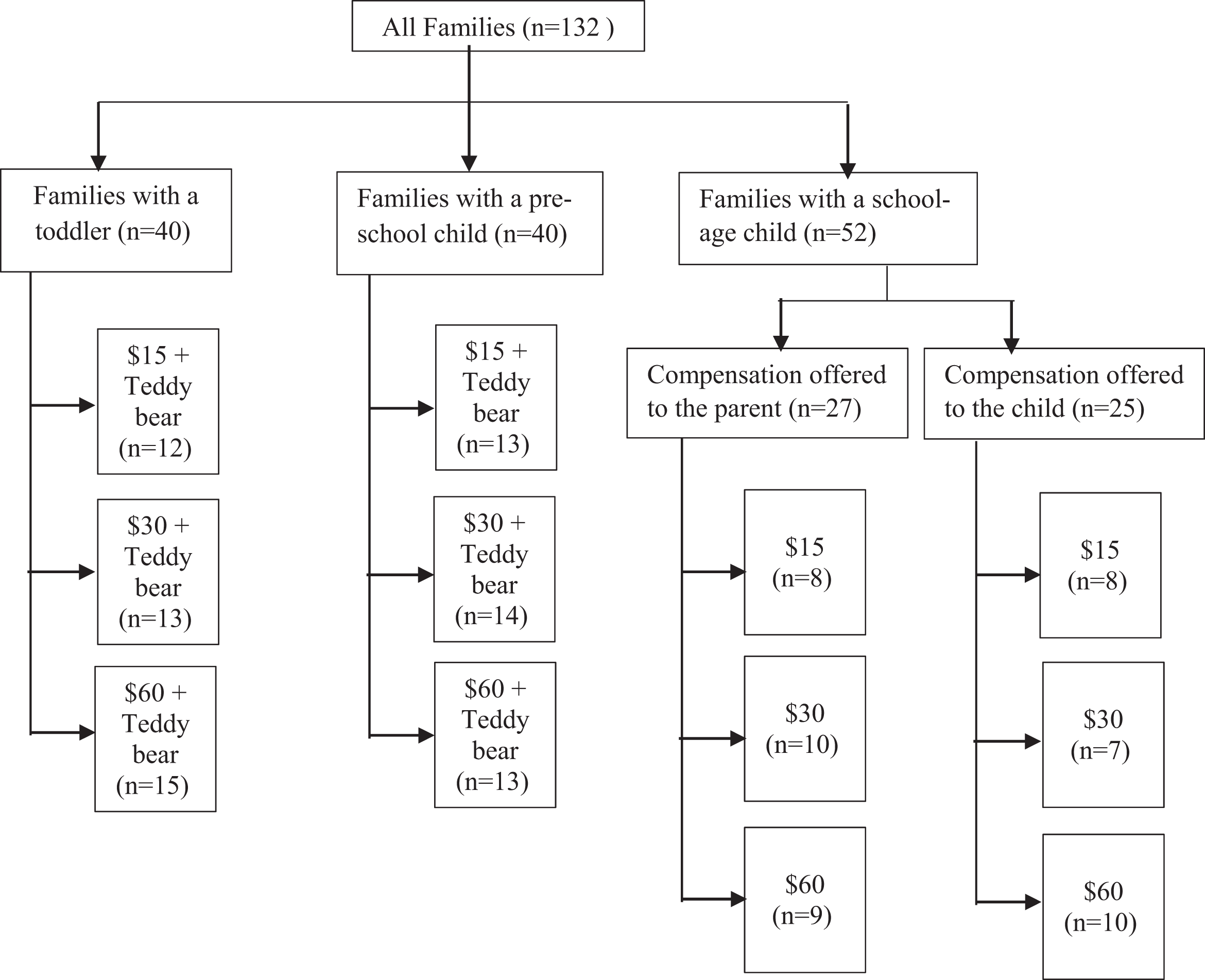
The study design. N and n represent the number of families. This is the same as the number of children since only one child was recruited per household. As explained in the text, the final analytic sample consists of 121 families.
A phlebotomist visited the families that agreed to provide a blood sample in their homes. If the families preferred, the families drove to the University of Michigan to provide the blood sample. The sample was used to answer other research questions that are not directly relevant to this article. The teddy bear was given in person at the time of the draw to those families who agreed to participate. The compensation was paid within 2 weeks of completing the blood draw (or allowing two phlebotomist attempts at blood draw). All families were actually paid US$60 irrespective of what they were offered initially. As the families did not know that they would all receive US$60 after they provided the blood sample (or after the phlebotomist made two attempts to draw a sample), we can assume that their response is based on the amount they were offered not to the actual payment. In case of toddlers and preschool children, the response is based on the amount the families were offered and the teddy bear.
Data and Validity of Randomization
Of the 132 children from 132 families, information on the willingness to supply a blood sample—the outcome of interest—is missing for 11 children. These 11 families were lost during the 6-month follow-up of the larger study, either because the family moved from their initial location or decided not to continue its participation. Of the remaining 121 children, who constitute the final analytic sample, 54.5% are boys, 72% are White, the median family income is approximately US$42,500, and each household has 4.6 members on average (Table 1). The average age of the toddlers (12–24–month olds) in the sample is 18 months, that of preschool children (3- to 6-year olds) is 52 months, and that of school-age children (10- to 12-year olds) is about 11.5 years. Nearly two thirds of the families agreed to provide a blood sample.
Summary Statistics for the Analytic Sample.
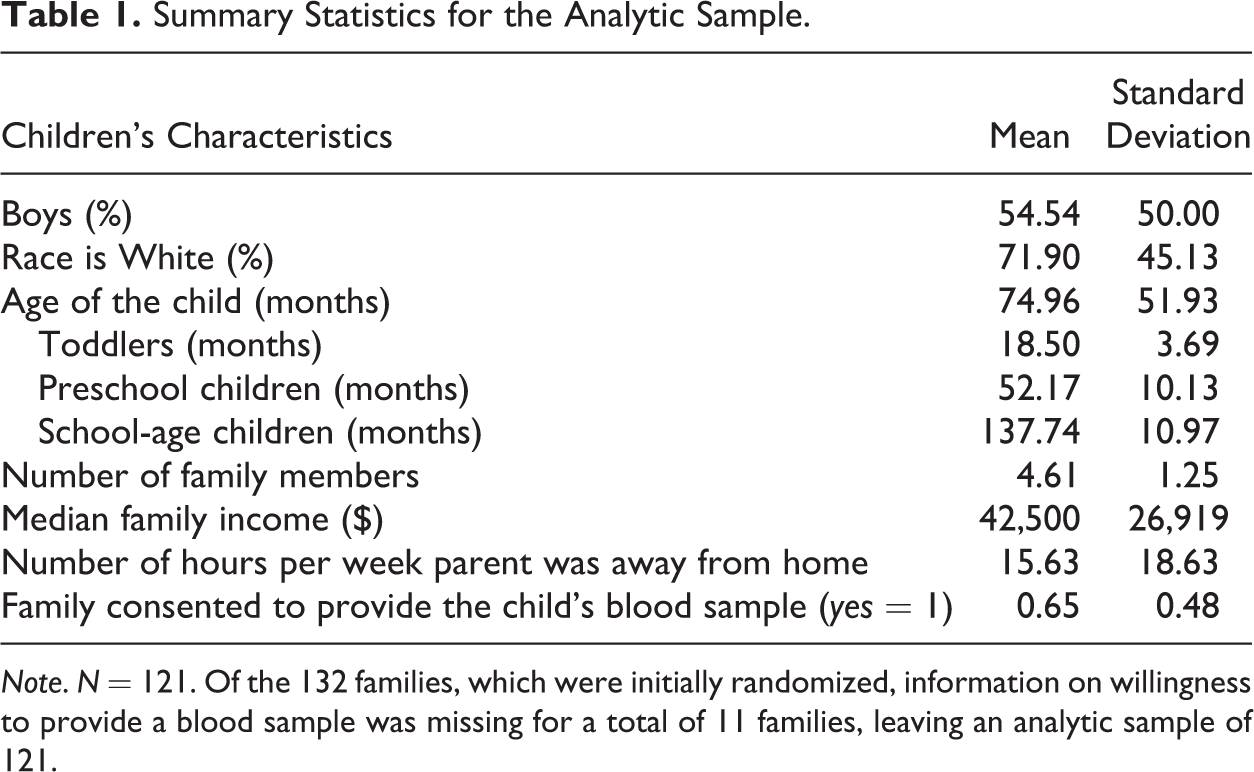
Note. N = 121. Of the 132 families, which were initially randomized, information on willingness to provide a blood sample was missing for a total of 11 families, leaving an analytic sample of 121.
Despite the relatively small sample size, randomization created subsamples that were generally balanced on the demographic characteristics mentioned above. Based on the conventional cutoff p value of .05, the arms offering different amounts of compensation are not different from one another in terms of most respondent characteristics. The average age of the child differs, but this difference is due to the younger children receiving a teddy bear; the average age of the children whose parents were offered US$15, US$30, or US$60 (i.e., compensation without the teddy bear) is similar, as is that of children whose parents were offered US$22, US$37, and US$67 (i.e., compensation plus the teddy bear).
Although we dropped more than 8% of the sample (= 100 × 11/132) due to missing information on the outcome variable, this is unlikely to bias our estimates because the dropped observations were evenly distributed across the arms. A formal regression of whether information on willingness to provide blood samples was missing on the amount of compensation showed that missingness was not correlated with the compensation amount (p value of the coefficient on the compensation amount was .59).
Empirical Approach
To assess the overall effect of compensation on willingness to provide blood samples, we estimate a logistic regression model with the family’s willingness (binary; = 1 if the parent or the child—depending upon to whom the compensation was offered—agreed to provide the child’s blood sample) as the dependent variable. The amount of compensation is the key explanatory variable. The sample consists of all observations. We estimate the following logistic model:

In Equation 1, Y
j
is a binary variable indicating whether a family j agreed to provide the blood sample in response to the amount of compensation the family was offered. Because we are interested in the effect of an additional US$1 on the willingness to provide the blood sample, we enter the compensation amount as a continuous variable. We computed the total amount of compensation offered to a family by adding the compensation and the cost of the teddy bear (US$7). For school-age children and their parents, the total amount of compensation is just the monetary amount (US$15, US$30, or US$60) because they were not provided a teddy bear. Covariates
Given that the compensation was assigned randomly and the arms are generally balanced across the key characteristics, β1 in the equation above can be interpreted as the causal effect of an additional US$1 of compensation on the willingness to provide a blood sample even when we do not control for individual and household characteristics. Still, we estimate the model first without any covariates, then with covariates that describe the child (age and gender), and finally with covariates describing the child and the family (age and gender of child, race, family income, and the number of hours per week the parent is away from home). Controlling for the covariates helps improve the precision of the key coefficient and adding them gradually enables us to check the coefficient’s stability.
Key Findings
There are several ways to understand the effects obtained from estimating the equation above. In Table 2, we provide coefficients on the amount of compensation. With a goal to provide as much practical guidance as possible to future researchers, in this section, we also report the effect of raising the compensation from $15 (the lowest amount offered in this study) to $67 (the maximum amount offered) and the elasticity. The response to financial compensation obtained using the logistic models above is nonlinear; therefore, we report the elasticity at the mean of the compensation and other covariates. We computed this elasticity by estimating the equation and calculating the marginal effect of a percentage change in the compensation on the log of the predicted probability of being willing to provide a blood sample.
Coefficients From a Logistic Regression of Willingness on Compensation.

Note. Each column represents a separate regression. Standard errors are in parenthesis. Child characteristics include age and gender. Family characteristics include race, number of family members, the number of hours per week the parents are away from home, and income.
*p < .10. **p < .05. ***p < .01.
For the overall sample, as expected, higher compensation had a significant positive effect on the willingness to provide a blood sample. The coefficient on compensation is .025 (Table 2, Panel A). This means that a US$1 of additional compensation raises the log odds of the respondent agreeing to provide a blood sample by .025. This translates to a marginal effect of 0.5 percentage point—raising the compensation by US$1, increases the probability of a respondent agreeing to provide a blood sample by 0.5 percentage point. Limiting the analysis to only parents and excluding the school-age children does not change the results (Table 2, Panel B). Marginal effect calculations using the fully specified regression indicate that increasing the compensation from US$15 to US$67 raises the probability of providing a blood sample from 51% to 79%. At US$15, a researcher would need to approach approximately twice the number of research participants to obtain a given sample size. At a compensation of US$67, she would need to approach only about 30% more participants than the required sample size. The elasticity of the willingness to provide a blood sample is .33. If the compensation is increased by 10% from its mean, the probability that a respondent agrees to provide a blood sample increases by 3.3%. We are unaware of any prior study that specifically evaluates the elasticity of the willingness to participate in an invasive study, let alone for children’s blood sample. Therefore, we are unable to compare our finding with prior research in this area.
Discussion
Ethical issues related to the provision of financial compensation to research participants are complex, even more so when they involve children. Much of the available literature on compensation to research participants—both generally and when it relates to children’s participation—focuses on ethical concerns and rarely addresses guidelines, benchmarks, or formula to assist investigators (Dominguez, Jawara, Martino, Sinaii, & Grady, 2012). This study contributes to the emerging literature on providing practical guidance to investigators. More precisely, it provides an estimate of the elasticity of research participation to financial compensation—a critical piece of information that researchers can use when designing a study.
The first key finding of this study is that, consistent with economic theory, participation increases with higher compensation. This means that if budget is not a primary concern, researchers can obtain a larger sample size by offering a higher compensation to research participants, at least up to the point allowed by the IRB. This strategy may be useful in cases where the population from which the sample needs to be drawn is relatively small.
Second, when there are fears of coercion and the population from which the sample is to be drawn is large, researchers should choose to offer smaller compensation and reach out to a larger population to get the desired sample (as opposed to offering a high—and potentially coercive—compensation and reaching to a smaller population to get the same sample size). In our study, 51% of research participants offered a blood sample even at a compensation of US$15 (or less than 2 times the minimum hourly wage in Michigan).
These findings should be understood with two caveats. First, we have assumed that the teddy bear provided to the parents of toddlers and preschool children had the same effect as the effect of an equivalent monetary amount (US$7). This may or may not be true. In practice, a teddy bear brought to the door is likely worth more, as the recipient does not need to travel to the store and spend time choosing it. Second, as with many studies, one should exercise caution while extending the findings to other settings as the demographic composition of families in the study differs from the U.S. population. Caution should also be taken when extending the findings to nonhealthy research participants and those with special conditions. Limited but emerging literature on the effect of financial compensation to cancer patients, for example, suggests that an amount that is too low can be ineffective, even detrimental to participation (VanGeest & Johnson, 2012).
A natural next step in this area of research is to confirm the findings above using a larger sample size. A larger sample size would also allow us to answer additional questions, such as whether and how the response varies by the age and gender of the child and by the family’s socioeconomic status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data for this study were collected as a part of the Healthy Families Project, which was funded by the University of Michigan Momentum Center.