
Abstract
The objective of this study was to observe the immediate effect of a knee brace with a patellar hole versus without a patellar hole on pain perception in patients with knee osteoarthritis. To accomplish this, a double-blind, randomized controlled trial enrolled 108 patients divided into two groups (knee brace with a patellar hole or without a patellar hole). Patients were evaluated by the Visual Analogue Scale (VAS) in order to measure their pain sensation, the Timed Up and Go (TUG) test was used to evaluate their ability to walk, and the 8-m walking test (8MWT) was used to estimate their walking speed. Both groups presented significant reduction in pain perception, higher function of the lower extremities, and greater mobility while wearing a knee brace. However, the patients who wore a knee brace without a patellar hole presented more favorable results than those who wore a knee brace with a patellar hole: a 1.6-point reduction was found versus 1.1 points in the VAS, the patients presented 0.7 s less time versus 0.4 s in the TUG, and the speed was reduced by 1.4 s versus 0.8 s in the 8MWT. Therefore, the knee brace without a patellar hole presented more favorable results when compared with the knee brace with a patellar hole.
Osteoarthritis (OA) is the most prevalent cause of knee injury. It affects around 10% of men and 18% of women worldwide. Knee OA is most likely to occur in older people, and the prevalence may increase to 50% in people aged over 65 years (The Royal Australian College of General Practitioners, 2009; April et al., 2013). The most common knee OA symptoms are pain, joint stiffness, joint instability, muscular weakness, and edema. Individuals who suffer from this condition experience a decrease in daily activities, as they have difficulties remaining in a standing position, rising from a sitting position, climbing stairs, or even walking, all of which make them more vulnerable to falling and injury (Bennell, Hunter, & Hinman, 2012; The Royal Australian College of General Practitioners, 2009; April et al., 2013).
Prior research has examined different effective approaches for the treatment of individuals with knee OA, including pharmacological treatments (Hochberg et al., 2012), more invasive treatments such as surgery (Richmond, 2008), and conservative treatments (Iwamoto, Sato, Takeda, & Matsumoto, 2011). Among these resources, the treatment choice is evaluated by considering the advantages and disadvantages for each patient, while accounting for patients with contraindications for surgery. Physical therapy is generally recommended as beneficial and also considered to be a conservative first-line treatment in an attempt to reduce pain, stiffness, and swelling. It improves joint mobility and flexibility by increasing the strength of the lower extremities and the functional framework in patients’ daily activities (Abbott et al., 2009; Iwamoto et al., 2011; April et al., 2013).
Moreover, in physical therapy, clinical practice elastic knee braces are commonly prescribed to decrease pain and increase muscle strength in the knee joint (Bennell & Hinman, 2011; The Royal Australian College of General Practitioners, 2009). An elastic knee brace is a low-cost resource that knee OA sufferers can easily and independently use in their daily activities; it is an important tool for reducing pain and improving functional levels (Bryk et al., 2011). It also helps to promote joint stability; however, the size of the knee brace has to be adjusted to each individual to promote comfort during activities and not to be too tight or harm the patient (Bryk et al., 2011; Mazzuca, Page, Meldrum, Brandt, & Petty-Saphon, 2004; Tiggelen, Coorevits, & Witvrouw, 2008).
There are basically two models of knee brace: the model with a patellar hole and the model without a patellar hole. The difference between them is that the patellar hole promotes patella stability within the knee’s range of motion (Petersen et al., 2014). However, the question of which one promotes the best clinical results persists in clinical practice. To the best of our knowledge, there are currently no published clinical trials that were designed to compare the effects of different types of knee braces in patients with OA.
This study addresses a question that is the subject of many clinical discussions: Is there a clinical difference in the effects of the different types of knee brace recommended for patients with knee OA? Currently, only one systematic review (Brouwer, Jakma, Verhagen, Verhaar, & Bierma-Zeinstra, 2005) has assessed the effect of braces and orthoses, including knee braces, in patients with knee OA. This systematic review analyzed a total of 13 studies (n = 1,356), which included studies that compared the effect of braces and orthoses in different forms of treatment. However, it is noteworthy that 10 of the studies included in this systematic review were considered to have a high risk of bias; furthermore, three of the studies were considered to have a low risk. Thus, the authors concluded that the use of these pieces of equipment is still inconclusive and that more studies are needed.
Therefore, the primary objective of the present study was to observe the immediate effect of a knee brace with a hole versus without a hole on pain perception in patients with knee OA. The secondary objective was to evaluate function and mobility when using a knee brace with and without a hole.
Method
Study Design
This is a double-blind, parallel study design with a 1:1 ratio; it is a randomized controlled trial. It was approved by Santa Casa de Misericórdia de São Paulo’s (ISCMSP) ethics review board and is registered at www.clinicaltrials.gov (registration no.: NCT02706106).
Inclusion and Exclusion Criteria
All participants were admitted to the Rehabilitation Department at ISCMSP, Brazil, with a medical diagnosis of knee OA. The research was conducted between March and April 2016. Patients were of both genders, were between 40 and 60 years of age, and had been diagnosed with knee OA. Patients with a minimum of 4 items from the knee OA diagnosis criteria according to the American College of Rheumatology (Altman et al., 1986), patients with a pain perception higher than four points on the Visual Analogue Scale (VAS), and patients seeking physiotherapy treatment were considered eligible to participate in this research.
Patients with a neurological disease, total or partial knee prosthesis, or cardiorespiratory disease; pregnant women; and patients unable to perform the proposed tests were excluded.
Outcomes
Two researchers (M.A.N.A. and D.G.F.) conducted the data collection. The first researcher (R1) collected data regarding the patients’ clinical characteristics. The VAS was used to evaluate patients’ pain sensation (Price, McGrath, Rafii, & Buckingham, 1983); it was evaluated by an 11-point scale, ranging from 0 (no pain) to 10 (worst possible pain), and the participants were asked to indicate their level of pain. The Timed Up and Go (TUG) test (Gan, Large, Basic, & Jennings, 2006) was used to evaluate the time a participant takes to get up from a chair, walk a distance of 3 m, make a turn around a cone, and return to the chair that they were originally sitting in. The 8-m walking test (8MWT; Fransen, Crosbie, & Edmonds, 1997) was used to estimate the walking speed per second over the 8 m without running. To minimize risks, especially the risk of falling, one of the researchers (D.G.F.) observed the study participants closely for the duration of all tests that were performed as part of the study. All data collection was performed before patient randomization and allocation to the knee brace with a hole group and the knee brace without a hole group.
Randomization and Intervention
The randomization process was developed by the computer software Microsoft Excel, Version 19.0 (Microsoft Corporation, Redmond, Washington), and opaque envelopes were sealed by an external researcher not involved in this study. After this first evaluation, R1 revealed the patient allocation and opened a randomized envelope before performing the second evaluation.
Patients were divided into two groups: the knee brace with a patellar hole group and the knee brace without a patellar hole group. Once a patient was allocated to a particular group, R1 chose an appropriate knee brace, which was sized to fit the patient’s knee according to knee circumference measured by perimetry, 27–31 cm (extra small), 31–35 cm (small), 35–39 cm (medium), 39–43 cm (large), and 43–47 cm (extra large). All devices were Neoprene knee braces from Mercur® (registered at Agência Nacional de Vigilância Sanitária [ANVISA]: no. 1034044001) and provided to the participants by the researchers.
The patients’ eyes were covered, so they would be blinded and would not know which knee brace they were wearing. R1 covered the knee brace with a black cloth bag, so that the second researcher (R2), who performed the tests, was also blinded to the type of knee brace that the patients were wearing. The patients’ eyes were uncovered once the knee brace was hidden.
During the entire data collection process performed by R2, R1 waited in another room. R2 evaluated the patients’ VAS, TUG, and 8MWT, while they were wearing their respective knee braces with or without a patellar hole. The duration of the data collection was approximately 45–60 min.
Blinding
In this double-blind study, the participants and R2 were blinded regarding the type of knee brace. It was not possible to blind R1, so R1 was chosen to perform the first evaluation before randomization, and R2 was chosen to perform the final evaluation.
Sample Size Calculation
The sample size calculation was based on the detection of one point of difference on the pain outcome, according to the Pain Perception Scale (the VAS). The statistical power was considered to be 80%, with calculations for a 5% α and the possibility of 15% of patients dropping out (in the case that patients reported pain during test performance). Therefore, the sample size calculation was 54 patients in each group and 108 patients in total.
Statistical Analysis
All the statistical analyses were performed by a group of researchers not directly involved in this research. The Kolmogorov–Smirnov test was used to determine the distribution normality of the variables. The Wilcoxon test was used to analyze pretest (no knee brace) versus posttest (wearing a knee brace) measurements in both groups (knee brace with a hole and knee brace without a hole), and the Mann–Whitney U test was used to evaluate differences between the groups. Differences were considered statistically significant when p < .05, and the Statistical Package for Social Sciences software, Version 19.0, was used for analysis.
Results
During the recruitment period, 129 patients were evaluated at the Rehabilitation Department. In total, 21 subjects were not considered for final inclusion for the following reasons: aged over 65 (n = 7), total or partial knee prosthesis (n = 6), pain lower than four points according to the VAS (n = 4), and inability to complete the tests (n = 4). During the data collection process, no patients dropped out of the study.
Most of the patients included in the study were women with an average age of 49 years and a knee pain sensation with a duration of 54 months. Table 1 presents all patients’ sociodemographic characteristics, followed by their respective assigned group. According to the patients’ characteristics, the knee brace with a patellar hole group and the knee brace without a patellar hole group were considered homogeneous.
Patients With Osteoarthritis Characteristics.

Note. Categorical variables are represented in numbers and percentage and continuous variables are represented as mean and standard deviation.
Considering the difference of patients’ performance before and after wearing the knee brace, both groups were evaluated by their pain intensity, functionality, and mobility levels (Table 2). Patients wearing the knee brace with a patellar hole presented with a significant reduction in pain intensity (p = .03), higher leg function measured by the TUG (p = .02), and greater mobility evaluated by the 8MWT (p = .03). In the same way, the other group (patients who wore the knee brace without a patellar hole) showed significant results in pain relief (p = .01), function (p = .02), and mobility (p = .04) when comparing before and after wearing the knee brace.
Pre- and Postintervention Values (Mean and Confidence Interval) at Baseline and After Intervention for Pain Intensity, Disability, and Mobility.
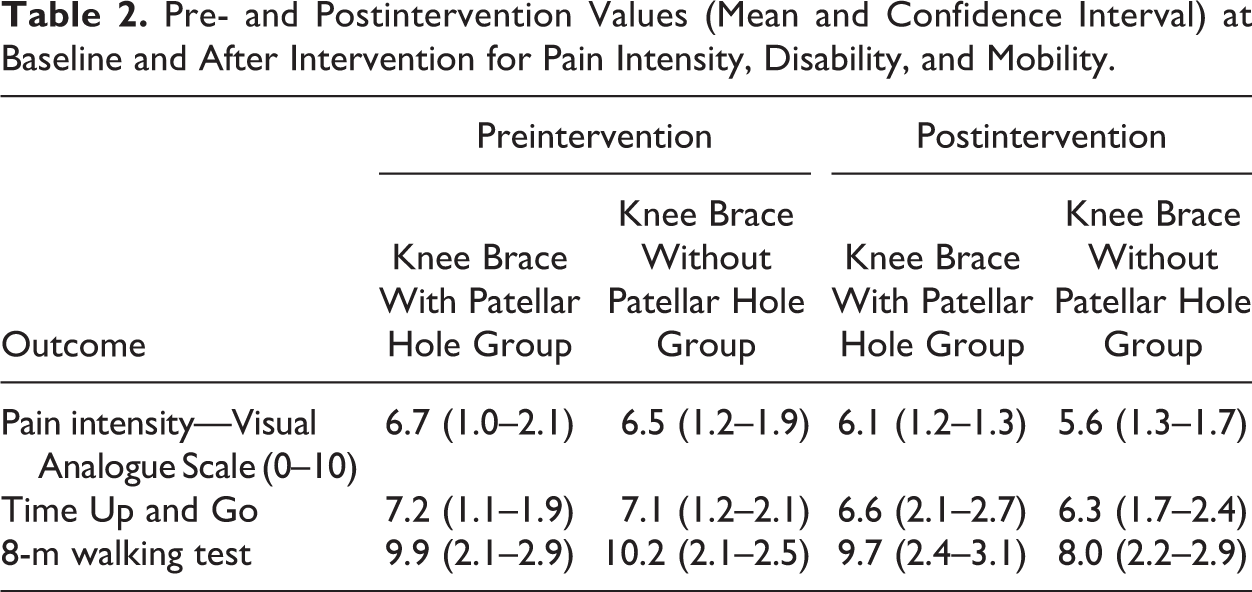
Comparing the two groups, patients who wore a knee brace without a patellar hole presented more favorable results than patients who wore a knee brace with a patellar hole. With regard to pain sensation, the knee brace without a patellar hole group presented a greater effect on reducing the pain sensation; these patients presented a reduction of 1.6 points versus 1.1 points in the knee brace with a patellar hole group. Moreover, the group wearing the knee brace without a patellar hole had greater leg functionality; the patients took 0.7 s less to perform the TUG test compared to 0.4 s less for the knee brace with a patellar hole group. They also presented greater mobility, which was evaluated by the 8MWT speed, which was reduced by 1.4 s compared to 0.8 s for the knee brace with a patellar hole group.
Discussion
The objective of this randomized controlled trial was to analyze the effect of a knee brace with a patellar hole compared to a knee brace without a patellar hole in the immediate relief of pain in patients with knee OA. When performing pre- and postintervention tests, both groups showed significant results in relieving pain (primary endpoint) and in improving function and mobility (secondary outcomes). However, when comparing the results of both groups, the group that received the knee brace without a patellar hole showed more favorable results.
Some studies have shown that the use of knee braces promotes cutaneous and somatosensory stimuli around the joint, favoring equilibrium and, consequently, increasing the dynamic control of the knee (Barrett, Cobb, & Bentley, 1991; Chuang et al., 2007; Edin, 2001). Currently, the literature presents two clinical trials that correlate the use of knee braces in patients with knee OA. A study by Bryk et al. (2011) aimed to evaluate the intensity of pain, disability, and mobility of 74 individuals with knee OA after wearing knee braces. Patients were divided into two groups: one group performed the proposed tests with a knee brace and the other group performed the tests without any device. As in the present study, the results of Bryk et al.’s (2011) study showed significant differences that support the recommendation that patients with knee OA use knee braces.
The second clinical trial, which was conducted by Brouwer, van Raaij, Verhaar, Coene, and Bierma-Zeinstra (2006), aimed to evaluate the effect of a knee brace on pain relief and on functional improvement in patients with unicompartmental knee OA. In this trial, 117 subjects were divided into two groups: an intervention group (n = 60), in which the participants were instructed to perform daily activities with a knee brace, and a control group (n = 57), in which the subjects were instructed to maintain their daily activities. After 12 months, a follow-up was performed, and the researchers observed significant results in pain relief and functional improvement outcomes in individuals who used the knee brace; however, the same was not observed in the control group.
Moreover, as presented in this study, the group that received the knee brace without a patellar hole had more favorable results than the group that received the knee brace with a patellar hole. One of the hypotheses regarding these results is related to the promotion of greater dynamic control through skin and somatosensory stimulation (Barrett et al., 1991; Chuang et al., 2007; Edin, 2001) by wearing a knee brace. The fact that a knee brace does not have a patellar hole may lead to a greater compressive force between the patella and the femoral trochlea, increasing the contact area between these bones, which consequently reduces the pressure at a given point on the knee joint, reducing pain (McConnell, 1996). This phenomenon would be linked with the favorable results obtained in this study.
This study followed the steps of previously published studies without making any changes in the first draft of the study design. Unfortunately, it was not possible to blind R1 who allocated the patients into two groups and was aware of the type of knee brace worn by the patients. To minimize the risk of allocation concealment bias, R2 was designated to perform the second evaluation. Furthermore, the use of the knee brace was only evaluated in the therapeutic context; it was not possible to measure the effects of the knee brace without the patellar hole on patients’ daily activities. Therefore, future studies are needed to understand the mechanisms that lead to the knee brace without a patellar hole improving function and mobility in patients with knee OA. Based on published studies and our results, we can state that a knee brace is a low-cost resource that can help patients with knee OA.
Based on the results, we conclude that the use of a knee brace with or without a supporting patellar hole is important for patients with knee OA because the results of this equipment showed a significant reduction in pain and improvement in function and mobility. However, when the results for the two types of knee braces were analyzed, the knee brace without a patellar hole presented more favorable results when compared to the knee brace with a patellar hole.
Footnotes
Authors’ Note
M.A.N.A., C.A., and D.G.F. developed the study design. M.A.N.A., V.P.R., and D.G.F. performed the data collection and V.P.R. was responsible for the statistical analysis. K.T.K. participated on data interpretation and manuscript language translation. M.A.N.A., C.A., V.P.R., and K.T.K. wrote the first draft of the manuscript and D.G.F. revised and contributed to the manuscript content. All the authors approved the last version of the manuscript before submission.
Acknowledgment
We want to thank all the Department of Physical Therapy at Santa Casa of São Paulo staff for the assistance during the development of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.