
Abstract
This study had a dual purpose (1) to identify variables associated with perceived work role performance (WRP) among 315 mental health professionals (MHPs) in Quebec and (2) to compare variables related to WRP in MH primary care teams (PCTs) and specialized service teams (SSTs), respectively. WRP was measured using an adapted version of the work role questionnaire. Variables were organized within five areas: individual characteristics, perceived team attributes, perceived team processes, perceived team emergent states, and geographical and organizational context. Half of the WRP variables were linked to team processes. Knowledge sharing correlated with WRP in both MH PCTs and SSTs. Team attributes had more impact on MH PCTs, while team processes and team emergent states played a larger role among SSTs. The association between WRP and knowledge sharing confirms the need for a systematic training program to promote interdisciplinary collaboration. Integration strategies (e.g., service agreements) could improve collaboration between MH PCTs and SSTs and help MHPs perform more effectively within PCTs.
Keywords
Biopsychosocial causes of mental health disorders (MHDs) affect many facets of patients’ lives. Hence, multidisciplinary teams are essential (van der Feltz-Cornelis, 2011) for providing holistic and complementary services that meet patient needs (Nancarrow et al., 2013). Recent MH reforms were designed to improve interdisciplinary teamwork, and ultimately services, by consolidating primary care teams (PCTs) and integrating them with specialized services (Commonwealth of Australia, 2009; Nicaise, Dubois, & Lorant, 2014). The integration of MH care into PCTs has had a profound impact on MH professionals (MHPs; Harris et al., 2016), especially those working previously within specialized service teams (SSTs). PCTs mainly serve patients with common MHDs, while SSTs address serious MHDs or complex cases (e.g., cooccurring MHDs and substance use disorders). Consultations and treatments in PCTs are more time limited (Kisely & Campbell, 2007; Thielke, Vannoy, & Unutzer, 2007), and PCTs operate with more limited expertise (Thiebaut, Farand, & Fleury, 2014), sometimes lacking psychiatrists and substance use disorder specialists (Thiebaut et al., 2014). MHPs working in new PCTs must surrender part of their autonomy to collaborate with new colleagues, such as general practitioners (GPs), who may have different values, experiences, and practices in MH (Kilpatrick, Lavoie-Tremblay, Ritchie, & Lamothe, 2011). GPs and other primary care providers have limited ability to diagnose and treat MHDs (Fleury, Grenier, & Robitaille, 2016; Thielke et al., 2007; Walters, Tylee, & Goldberg, 2008). Working effectively with new MH PCTs, as well as SSTs, requires that team members have a good understanding of their tasks (perceived work role performance [WRP]), both as individuals and as members of their teams and organizations (Mathieu, Maynard, Rapp, & Gilson, 2008).
A positive WRP improves satisfaction among both professionals (S. W. J. Kozlowski & Bell, 2003; Lemieux-Charles & McGuire, 2006) and patients, attenuates the risk of negative events (Kilpatrick et al., 2011; Manser, 2009), and reduces health costs (Quaschning, Korner, & Wirtz, 2013). WRP is thus a proximal outcome worthy of attention. This concept comprises behaviors over which individual team members may have control and which are in themselves predictive of results expected from health teams such as healthier patients.
Some models have identified variables associated with WRP. Under the Input–Mediator–Outcome–Input (IMOI) model (Ilgen, Hollenbeck, Johnson, & Jundt, 2005), individual characteristics, along with team and organizational attributes (input), act on two kinds of mediators: perceived team processes (i.e., actions affecting team performance such as knowledge sharing) and team emergent states (i.e., motivation, cognition, and commitment; Mathieu et al., 2008). These mediators then impact outcomes such as patient satisfaction (Jaca, Viles, Tanco, Mateo, & Santos, 2013). Interaction with other teams also comes into play (Ilgen et al., 2005; Perlow, Gittel, & Katz, 2004).
Similarly, in the heuristic Integrated (Health Care) Team Effectiveness Model (ITEM), the organizational and external environment (social and policy context) may influence task design variables (setting, nature and composition of the team, rules and procedures, and quality standards). All these factors may be directed by teams to improve effectiveness (Lemieux-Charles & McGuire, 2006). Several studies have assessed determinants of health team effectiveness (Kilpatrick et al., 2011; Lemieux-Charles & McGuire, 2006), but few have looked at variables influencing WRP and more particularly in MH (Wholey et al., 2012).
In previous studies, individual characteristics (e.g., age and gender) had little influence on WRP or presented mixed results (Mathieu et al., 2008; Webber & Donahue, 2001). Concerning team attributes, studies found associations between WRP and familiarity between coworkers (Chiocchio, Grenier, O’Neill, Savaria, & Willms, 2012), team interdependence (Mathieu et al., 2008), and team support (Mathieu et al., 2008). Type of profession affects WRP; professionals with higher employment status (e.g., physicians) have more positive perceptions of their WRP than nurses (Lichtenstein, Alexander, McCarthy, & Wells, 2004). The relationship between WRP and the use of standardized clinical approaches or tools has yet to be assessed, although these practices are acknowledged as improving MH team effectiveness (Blackmore & Persaud, 2012; Buljac-Samardzic, Dekker-van Doorn, van Wijngaarden, & van Wijk, 2010; Lemieux-Charles & McGuire, 2006). Given that a heavy workload may hinder performance (Chiocchio, 2012), perceived work role among MHPs may be influenced by the high rate of complex cases (e.g., heavy service users and personality disorders).
In addition, several team processes are acknowledged as affecting WRP and team effectiveness: collaboration (Chiocchio, Forgues, Paradis, & Iordanova, 2011), autonomy (Langfred & Moye, 2004), conflict (De Dreu & Weingart, 2003), informational role self-efficacy (Sonnentag & Frese, 2002), knowledge sharing (Bock & Kim, 2002; Quigley, Tesluk, Locke, & Bartol, 2007), integration (Korner et al., 2016), and participation in decision-making (Chiocchio, 2012). WRP was also linked to several team emergent states: trust (Kirkman, Rosen, Tesluk, & Gibson, 2006), team climate (Mathieu et al., 2008), job satisfaction (Manser, 2009; Maynard, 2007), and belief in the advantages of interdisciplinary collaboration (S. W. Kozlowski & Ilgen, 2006). Finally, the impact on WRP of the geographical and organizational context has received little attention (Lemieux-Charles & McGuire, 2006), except for organizational culture (Gerowitz, Lemieux-Charles, Heginbothan, & Johnson, 1996; Scott, Mannion, Marshall, & Davies, 2003; Shortell et al., 2001). The clan culture (e.g., flexibility and internal focus) is reported to be linked with WRP and job satisfaction (Hartnell, Ou, & Kinicki, 2011; Scammon et al., 2014).
To our knowledge, no research has compared WRP among professionals in MH PCTs and SSTs. As both kinds of teams differ in terms of role, activities, composition, and clientele served, it is conceivable that different variables could also influence their WRP. The international trend toward consolidating MH and primary care justifies a comparative study of MH PCTs and SSTs.
This study had two distinct purposes. First, it identified variables associated with WRP among 315 MHPs working in MH PCTs (n = 101) and SSTs (n = 214). Consistent with the IMOI (Ilgen et al., 2005) model and the ITEM (Lemieux-Charles & McGuire, 2006), we hypothesized that overall WRP would most likely proceed from team processes rather than from individual characteristics, team attributes, team emergent states, or geographical and organizational context. Second, the study compared variables associated with WRP among MHPs from MH PCTs and SSTs, respectively. Considering that PCTs and SSTs perform different roles and tasks, we hypothesized that variables related to WRP would be significantly different for each type of team.
Method
Study Context and Design
This study emanated from a larger evaluation of local health service networks (LHSNs) implemented under the 2005–2015 MH care reform (Ministère de la santé et des services sociaux [MSSS], 2005a) in Quebec (Canada). As part of a global reform of the Quebec health-care system (MSSS, 2005b), general hospitals, local community health centers, and nursing homes were merged to create 93 health and social service centers (HSSCs). These centers oversee health service organization in their respective LHSNs and coordinate other health service providers (e.g., psychiatric hospitals, community-based organizations, and medical clinics). The reform (MSSS, 2005a) required that at least one MH PCT be established within each HSSC to treat patients with common MHDs and provide follow-up services to stabilized users with severe MHDs. Furthermore, MH PCTs and SSTs were urged to consolidate their efforts through service agreements, liaison officers, shared staff, and the like to improve continuity of care for users with severe MHDs living in the community.
This study included MHPs from four Quebec LHSNs selected in consultation with an advisory committee composed of key decision makers in the Quebec MH care system. Three LHSNs were served by a psychiatric hospital: two in the province’s largest city and one in the capital. The fourth, located in a semiurban area, relied on the services of a psychiatric department in a general hospital. Populations ranged from 135,000 for the semiurban area to 300,000 for the LHSN located in the capital.
To be eligible for the study, MHPs had to work in one of the LHSNs as a member of a MH PCT or SST composed of three or more MHPs from at least two distinct disciplines (e.g., psychologist, nurse, and social worker). A psychiatric research ethics board approved the multisite study protocol.
Data Collection and Definition of Variables
An advisory committee composed of representatives from each of the four LHSNs identified team managers, each of whom provided a list of MHPs eligible for the study. Consent forms and self-administered questionnaires requiring approximately 45 min to complete were mailed to designated MHPs. Data collection extended from May to November 2013.
Another questionnaire requiring approximately 120 min was sent to team managers (N = 49) of the individual MHPs between October 2013 and June 2014. This questionnaire covered patient characteristics, team profiles, clinical activities, network integration strategies, and frequency of and satisfaction with interactions with network teams/organizations.
The dependent variable, perceived WRP, was measured with the work role questionnaire (Griffin, Neal, & Parker, 2007), translated into French by Chiocchio et al. (2012). This 27-item measurement tool covers three different aspects: individual behaviors impacting individual performance (e.g., “I carry out the core parts of my job well”), individual behaviors impacting team performance (e.g., “I coordinate my work with my coworkers”), and individual behaviors impacting organizational performance (e.g., “I present a positive image of the organization to other people”). Each aspect under study comprised three elements of WRP: task proficiency, adaptability, and proactivity. Items linked to organizational performance were omitted, as the variables of interest were limited to determinants of team WRP, which include behaviors that focus on the respective performance of the team and the individual. Items were rated using a 5-point scale. The aggregated Cronbach’s α for the original questionnaire was .91 (Griffin et al., 2007).
A conceptual framework (Figure 1), adapted from both the IMOI model and ITEM, and related literature on WRP and team effectiveness, guided the analysis. Variables were grouped into five categories: (1) individual characteristics, (2) perceived team attributes, (3) perceived team processes, (4) perceived team emergent states, and (5) geographical and organizational context. All standardized scales were translated into French and validated. Some variables (i.e., standardized clinical tools, clinical approaches, frequency and satisfaction of interaction with other services/teams, and integration strategies) were assessed using a 5-point Likert-type scale. A mean score was also calculated for each of these variables. A description of the scales appears in Table 1.

A conceptual framework.
Description of Standardized Instruments Included in the Study.
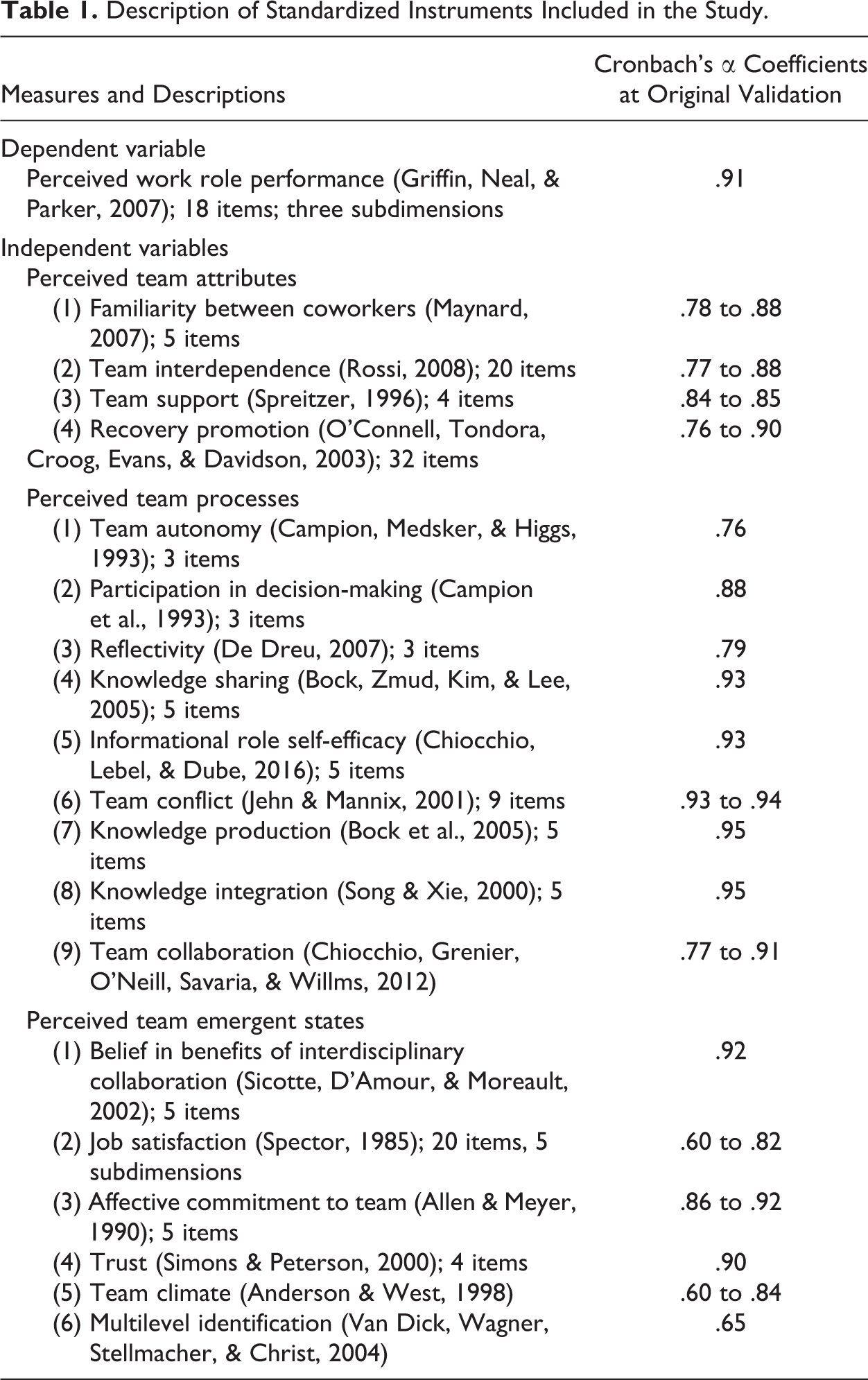
Four individual characteristics were identified: gender, age, seniority (in team and profession), and employment status (full-time and part-time). Perceived team attributes included type of professional (medical [e.g., pharmacist, nurse, and GP], psychosocial [e.g., social worker and psychologist], and general [e.g., technician and clerk]) and four standardized scales: familiarity between coworkers, team interdependence, team support, and recovery promotion. It also included four variables from the team manager questionnaire: (1) percentage of time allocated to treatment, interventions, or evaluation; (2) patient characteristics; (3) standardized clinical tools; and (4) clinical approaches.
Nine variables from the professional questionnaire covered perceived team processes: (1) team autonomy, (2) participation in decision-making, (3) reflexivity, (4) knowledge sharing, (5) informational role self-efficacy, (6) team conflict, (7) knowledge production, (8) knowledge integration, and (9) team collaboration.
Six variables from the MHP questionnaire covered perceived team emergent states: (1) belief in the benefits of interdisciplinary collaboration, (2) job satisfaction, (3) affective commitment to the team, (4) trust, (5) team climate, and (6) multilevel identification.
Geographical and organizational context included six variables from the team manager questionnaire: (1) percentage of time allocated to coordination with other teams, (2) frequency of intervention plan use, (3) frequency of interaction with other services/teams, (4) satisfaction with interactions with other services/teams, (5) integration strategies and organizational culture.
Organizational culture was measured using the Organizational Culture Assessment Instrument (Cameron & Quinn, 2006), which consisted of six questions where participants were asked to distribute a total of 100 points across four possible choices per question. Organizational culture was classified according to a four-factor model along two axes (flexibility vs. stability and internal vs. external focus): (1) clan (flexibility and internal focus), (2) adhocracy (flexibility and external focus), (3) market (stability and external focus), and (4) hierarchy (stability and internal focus; Scammon et al., 2014).
Analyses
After clearing the database of outliers and missing values, we completed univariate, bivariate, and multivariate analyses. Univariate analyses comprised frequency distributions (numbers and percentages) for categorical variables and central tendency measures (mean values and standard deviations) for continuous variables. We assessed normality assumptions for the three dependent variables: WRP of MHPs within MH PCTs, SSTs, and total sample. Multivariate tests for colinearity were performed to detect variables that were strongly correlated (tolerance, Variable Inflation Factor). Yet no likelihood of highly correlated variables was identified. The three dependent variables were found to be normally distributed. Bivariate analyses were performed using a simple linear regression analysis of variance t test, with an α value of .10. Variables significantly associated with each dependent variable were used to build multiple linear regression models, with the α value set at .05. The explained variance (R 2) and the goodness of fit (F test and p value) were calculated for each multiple regression model.
Results
A group of 315 MHPs of a possible 466 participated in the study (response rate: 68%). There were no significant differences between participants and nonparticipants with respect to the distribution for team type, χ2(1, N = 466) = 0.79; p = .68, and gender, χ2(1, N = 466) = 0.03; p = .87. With regard to health-care services, 32.1% of MHPs worked in MH PCTs and 67.9% in SSTs. Most MHPs were female: 70% in the total sample, 78% in MH PCTs, and 65% in SSTs. Most participants were psychosocial professionals (54.6%), while the rest were medical professionals (34.6%) or general professionals (10.8%).
Among team managers, 41 of a possible 49 participated in the study (response rate: 84%). There were no significant differences between respondent and nonrespondent managers for type of health-care setting, χ2(1, N = 49) = 1.86; p = .24, and gender, χ2(1, N = 49); p = .66. Most respondent managers (62%) worked in SSTs versus 38% in PCTs. Most respondent managers (70%) were female.
The mean score for WRP was 3.81 (SD = 0.51) for the total sample. The global mean score for MHPs from SSTs (3.88; SD = 0.52) was significantly higher than for MHPs from MH PCTs (3.65; SD = 0.47; t = −3.937, p < .001). This was also true regarding scores for proficiency (4.06; SD = 0.51 for SSTs vs. 3.82; SD = 0.49 for PCTs; t = −4.571, p < .001) and for proactivity (3.64; SD = 0.66 for SSTs vs. 3.35; SD = 0.65 for PCTs; t = −3.668, p < .001). The adaptivity score was marginally higher for SSTs versus PCTs: 3.93; SD = 0.59 vs. 3.79; SD = 0.56; t = −1.930, p = .055. Table 2 presents variables significantly associated with WRP in bivariate analyses for the total sample and for MHPs from PCTs and SSTs, respectively.
Participant Characteristics: Total Sample (Primary and Specialized Services).
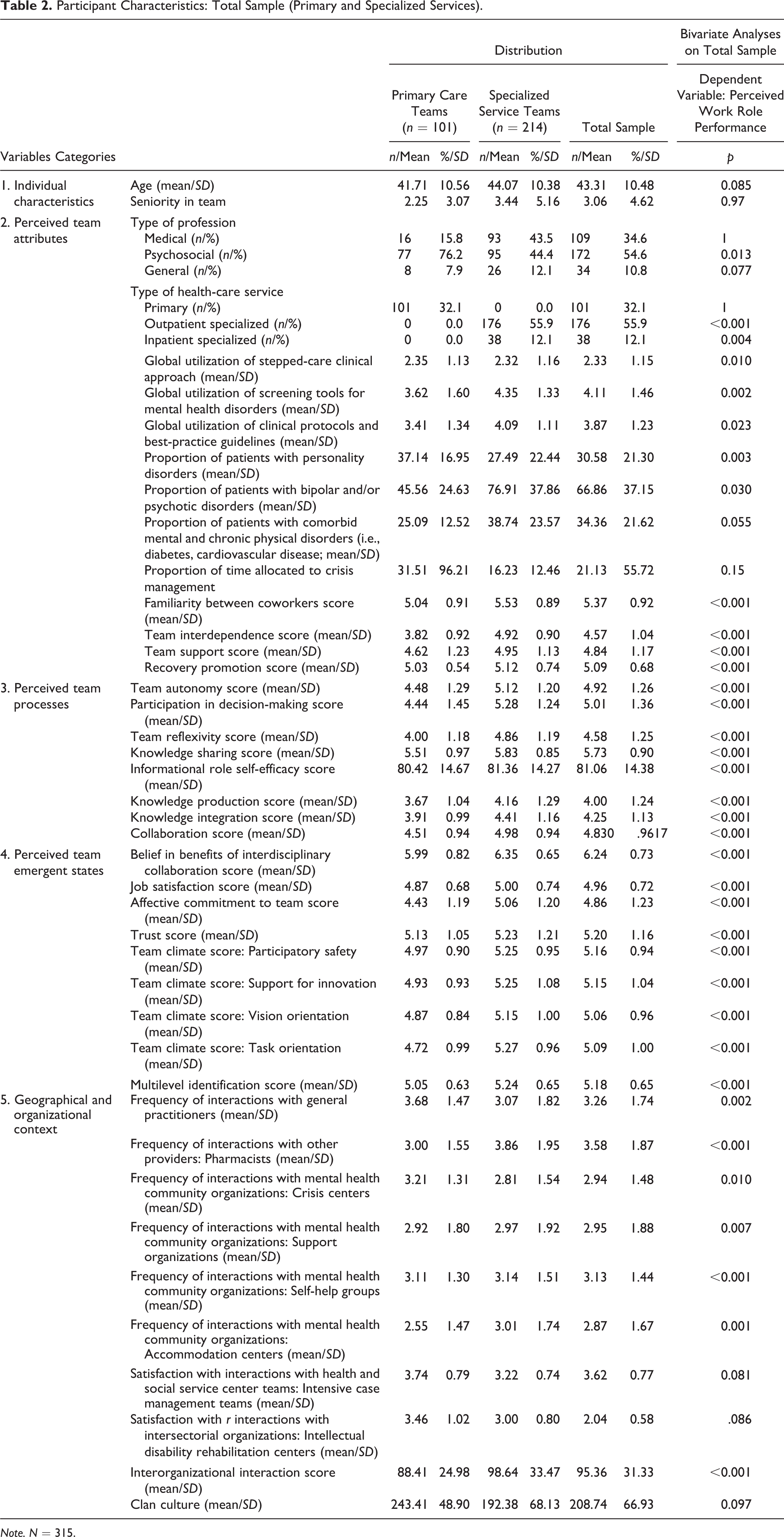
Note. N = 315.
WRP in the total sample (Table 3) had a strong link with recovery promotion and team interdependence (perceived team attributes); knowledge sharing, informational role self-efficacy, and team collaboration (perceived team processes); belief in the benefits of interdisciplinary collaboration (perceived team emergent states); and frequency of interactions with GPs (geographical and organizational context) and, marginally, with participation in decision-making (perceived team processes). This model explains 52% of the total variance and has an acceptable goodness of fit.
Variables Independently Associated With Perceived Work Role Performance.
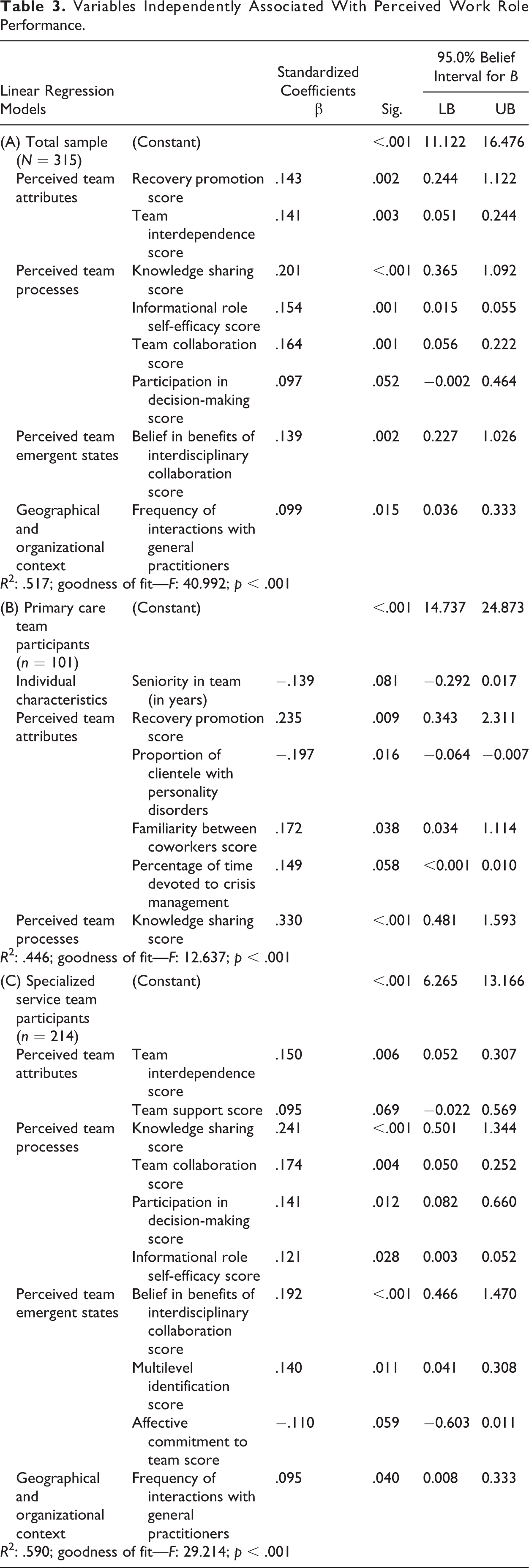
Within MH PCTs, WRP correlated significantly with knowledge sharing (perceived team processes) and with familiarity between coworkers and recovery promotion (perceived team attributes). There was a marginal link with the percentage of time allocated to crisis management, a low proportion of patients with personality disorders (perceived team attributes), and lower seniority on the team (individual characteristics). This model explains 45% of the total variance and has an acceptable goodness of fit.
With regard to SSTs, WRP was significantly associated with knowledge sharing, team collaboration, participation in decision-making, and informational role self-efficacy (perceived team processes); belief in the benefits of interdisciplinary collaboration and multilevel identification (perceived team emergent states); team interdependence (perceived team attributes); and frequency of interactions with GPs (geographical and organizational context). WRP was marginally associated with team support (perceived team attributes) and lower affective commitment to team (perceived team emergent states). This model explains 59% of the total variance and has an acceptable goodness of fit.
Discussion
Overall, the results confirmed our hypothesis that perceived team processes were the main determinants of WRP among MHPs, with four of the eight variables figuring into the final model. Among these variables, knowledge sharing had the closest correlation with WRP and was the only variable common to MH PCTs and SSTs. Organizational ability to share and use knowledge plays a significant role in team effectiveness (Bock & Kim, 2002; Quigley et al., 2007; Wang & Noe, 2010). The right conditions for knowledge sharing involve higher anticipated rewards, reciprocal relationships, a sense of self-worth, and an organizational climate favorable to innovation (Bock, Zmud, Kim, & Lee, 2005). The literature points to informational role self-efficacy as a major factor in performance (Sonnentag & Frese, 2002). Self-efficacy promotes adaptive and proactive behaviors among teams and facilitates both knowledge sharing and high-quality care (Chiocchio, Lebel, & Dube, 2016). Studies have also found that collaboration was a predictor of WRP, reducing conflict and promoting trust within teams (Chiocchio et al., 2011; S. W. J. Kozlowski & Bell, 2003; Lepine, Piccolo, Jackson, & Mathieu, 2008). Participation in decision-making enhances effectiveness by improving each team member’s sense of responsibility and ownership of the work (Campion, Medsker, & Higgs, 1993).
With two associated variables (team interdependence and recovery promotion), perceived team attributes were the second most important determinants of WRP among MHPs. Interdependence is usually the reason to create a team (Campion et al., 1993), as each team member depends on the others to some degree (Griffin et al., 2007). Studies have found that stronger interdependence is closely related to effectiveness (Kilpatrick et al., 2011; Lemieux-Charles & McGuire, 2006). Teamwork also enhances the quality of interdependence (Chiocchio, 2012; McIntyre & Salas, 1995). Regarding recovery promotion and WRP, reports indicate that more effective recovery-oriented services lead to less burnout and higher job satisfaction, two mediators of WRP among MHPs (Osborn & Stein, 2016). Other studies (Lakeman, 2010; Williams & Tufford, 2012) with service users have suggested that recovery-oriented care requires MHPs to possess specific knowledge (e.g., information about illness and treatment and access to services) and skills (e.g., teamwork, coordination, and collaboration). For example, a qualitative study involving patients with schizophrenia revealed that teamwork, knowledge sharing, and holistic care were key components of recovery-oriented services (Williams & Tufford, 2012).
It is logical that belief in the advantages of interdisciplinary collaboration would favor WRP since this perceived emergent state requires shared goals and responsibilities as well as the involvement of each professional in decision-making (Sicotte, D’Amour, & Moreault, 2002). Interdisciplinary collaboration enables global and integrated healthcare, which is a central objective of MH reforms (Sicotte et al., 2002).
WRP was linked with only one variable under geographical and organizational context: frequency of interaction with GPs. This result seems to reflect the hiring of respondent psychiatrists to consult with, and support, GPs in medical clinics with the implementation of “shared care” under the Quebec reform. GPs usually make initial clinical contact with patients affected by MHDs and take charge of their medical follow-up (Walters et al., 2008). The transfer and follow-up of patients with severe MHDs in the community require close collaboration between psychiatrists and GPs.
Of the eight variables significantly or marginally associated with WRP, only one (knowledge sharing) was common to MH PCTs and SSTs, while six variables correlated with SSTs only and one (recovery promotion) with MH PCTs only. The sample consisted mainly of MHPs working in SSTs (68%), which may explain why more variables associated with WRP were shared among SSTs than among MH PCTs.
The results confirm our second hypothesis that different variables influence WRP in MH PCTs and SSTs. Primary care is more accessible and less stigmatizing for patients, which may explain why recovery promotion impacted the WRP of MHPs within PCTs (Fleury, Imboua, Aube, Farand, & Lambert, 2012). The association between WRP and familiarity between coworkers in MH PCTs suggests that these teams were still in the first two phases described by Kozlowski and Bell (2003) as socialization and acquisition of task knowledge and new skills. Familiarity between coworkers allows better communication and understanding, thus reducing errors (Courtenay, Nancarrow, & Dawson, 2013). WRP should, therefore, improve when MHPs are used to working together. The marginal connection between WRP and lower level of seniority in MH PCTs seems to contradict the previous observation. One possible explanation would be that some MH PCTs include MHPs transferred from SSTs who have more experience in interprofessional collaboration. Newcomers to MH PCTs may have also received specific training to ensure proficiency in their new setting. The negative impact of high numbers of personality disorder cases on the WRP of MH PCTs, based on perceptions of team managers, could stem from patient interactions that are too limited to meet the needs of these heavy service users (Kisely & Campbell, 2007; Laugharne & Flynn, 2013). Finally, there was a marginal association between WRP and time allocated to crisis management. The fact that MH PCTs are responsible for crisis service delivery requiring immediate and concerted action by the entire team suggests that WRP would increase with the amount of time allocated to crisis management.
Concerning SSTs, the association between multilevel identification and WRP might indicate that MHPs identify more with their profession or discipline than their team. Their decision to remain with the team may stem from a sense of obligation or a recognition of the costs of leaving, rather than any affective commitment toward their coworkers (Allen & Meyer, 1990). The marginal impact of team support on WRP within SSTs may reflect the relative abundance of resources in psychiatric hospitals as compared with primary care institutions. Team support has been described as a group maintenance behavior (Campion et al., 1993).
Limitations
There are two important limitations to this study. First, the data are cross-sectional and as such cannot be used to infer cause and effect. Second, the results may not apply to jurisdictions with health-care systems or related services different than those in Quebec.
Conclusion
This study was innovative in including a broad sample of MHPs working in MH PCTs or SSTs. Moreover, the holistic model tested included many variables usually covered in the literature on WRP, but also others (e.g., clinical tools, clinical approach, and interactions with other teams) recognized for their strong impact on team effectiveness. Finally, the study identified variables associated with overall WRP, as well as some linked specifically to MH PCTs or SSTs. The overall results confirm the strong link between WRP and team processes, especially knowledge sharing. They indicate the importance of implementing a systematic training program for MHPs to promote interdisciplinary values and skills, as suggested by several international reforms. An interdisciplinary approach to training would facilitate communication and support between the various professions, helping to harmonize their visions and practices.
The results also show that WRP was mainly related to perceived team attributes among MH PCTs as well as perceived team processes and perceived team emergent states among SSTs. Since managers have more direct influence on perceived team attributes than perceived team processes (Campion et al., 1993), it is essential that they provide human and material support to new MH PCTs to improve the WRP of their MHPs. A more systematic implementation of integration strategies, such as shared care, service agreements, liaison activities, or joint training initiatives may ensure better alignment between MH PCTs and SSTs to the ultimate benefit of patients, especially those with complex profiles such as personality disorders.
Footnotes
Acknowledgment
We thank the individuals who participated in the research including our advisory committee and network respondents and our research team (Catherine Vallée, Denise Aubé, Lambert Farand, and Geneviève Cyr).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study came from the Fonds de recherche du Québec Santé and the Prends Soin de toi programs.