
Abstract
The main objective of this study was to evaluate the effects of interactive video games on functional balance and mobility in poststroke individuals. The Health Science databases accessed included Medline via PubMed, LILACS, SciELO, and PEDro. The inclusion criteria were as follows: clinical studies evaluating the use of interactive video games as a treatment to improve functional balance and mobility in individuals poststroke and studies published in the Brazilian Portuguese, English, or Spanish language between 2005 and April 2016. PEDro Scale was used to analyze the methodological quality of the studies. The Berg Balance Scale and Timed Up and Go Test (TUGT) data were evaluated using a meta-analysis, the publication bias was assessed by funnel plots, and the heterogeneity of the studies by I 2 statistic. Eleven studies were included in the final analysis. Functional balance improved in individuals treated using interactive video games (mean difference = 2.24, 95% confidence interval [0.45, 4.04], p = .01), but no improvement was observed in mobility as measured by TUGT. The studies presented low heterogeneity (24%). The mean score on the PEDro Scale was 6.2 ± 1.9. Interactive video games were effective in improving functional balance but did not influence the mobility of individuals poststroke.
World Health Organization defines stroke as a rapidly developing syndrome caused by vascular involvement of encephalic arteries, of ischemic or hemorrhagic origin, that may lead to focal disturbance of encephalic function (WHO, 2006). In the United States, about 795,000 people are diagnosed with stroke annually, with 1 in 20 deaths being from stroke resulting in 130,000 deaths per year (Centers for Disease Control and Prevention [CDC], 2017; Mozaffarian et al., 2015).
Stroke can be detrimental to speech as well as sensorimotor and cognitive functions. Among the sensorimotor alterations, impairment of functional balance and mobility (Da, Física, Pacientes, & Acidente, 2013; Mc, Kelly, Godwin, Enderby, & Campbell, 2016; Morelato, Pinto, Regina, & Oliveira, 2015) are the most limiting to the activities of daily living (Soares, Santos, Costa, & Melo, 2015; Veerbeek et al., 2014; Webster & Celik, 2014). Several studies have analyzed the effects of different interventions such as functional electrical stimulation, robotic therapy, and virtual reality (Veerbeek et al., 2014) on improving the functional balance and mobility of individuals poststroke.
Improved functional balance and mobility in individuals with stroke have been associated with reduced risk of mortality (Callaly et al., 2015). After stroke, individuals who experienced at least one fall or presented functional dependence had a higher risk of death within 2 years compared to functionally independent individuals or those with mild/moderate disability (OR = 6.5, p = .001; Callaly et al., 2015).
Virtual reality is defined as the projection of a scenario with which individuals can interact through their sensory channels and body movements (da Silva Ribeiro et al., 2015). Accordingly, interactive video games can be considered a form of virtual reality. Several studies have shown the potential of this new intervention for rehabilitation of individuals poststroke (Laver, George, Thomas, Deutsch, & Crotty, 2015; Li, Han, Sheng, & Ma, 2015; Lloréns, Gil-Gómez, Alcañiz, Colomer, & Noé, 2015).
Among the interactive commercial video game consoles, Nintendo Wii and Xbox with Kinect sensors have been used for the rehabilitation of individuals with neurological impairment. The Nintendo Wii system detects movement using accelerometers, infrared signals, or a platform with pressure sensors. The Xbox with Kinect sensors detects movements through a camera that captures infrared signals from anatomical landmarks, creates an avatar, and projects the reproduced movements of the player on the game screen. This enables interaction without the need of a game controller (Soares et al., 2015; Webster & Celik, 2014).
Systematic reviews have verified the positive effects of virtual reality in poststroke individuals on upper limb function (Laver et al., 2015); gait (Li et al., 2015; Rooij, van de Port, & Meijer, 2016); perception of the affected side of the body; and cognition such as attention, planning, and executive functions (Pompeu et al., 2014). However, the results of these systematic reviews are controversial, given the heterogeneity of the virtual reality systems and study populations between the studies. Therefore, it is important to specifically evaluate the effects of interactive video games, with and without conventional physical therapy, on functional balance and mobility rehabilitation in individuals poststroke.
Hypotheses regarding the effects of interactive games state that the constant self-correction during a series of motor tasks is beneficial to the effected individuals in promoting neuroplasticity as motor planning and motor control abilities are continuously stimulated through visual biofeedback. Studies have demonstrated that mirror neurons activity is modulated to imitate the neural activation pattern of an observed motor task. This improves movement performance and, consequently, the functional balance and mobility of the patient (Brunner, Skouen, Ersland, & Grüner, 2014; Wang et al., 2015). Hence, the objective of this study was to evaluate the effects of interactive video games on functional balance and mobility in individuals poststroke.
Method
This review was registered on the PROSPERO site (http://www.crd.york.ac.uk/prospero/): CRD42015024685. The present study followed the methodological recommendations proposed by Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (Padula et al., 2012).
Eligibility Criteria
Studies with the following characteristics were included in this systematic review: randomized clinical trials involving individuals poststroke, analyzed the effects of interactive video games, such as Nintendo Wii and Xbox with Kinect sensors, on functional balance and mobility outcomes, and published between 2005 and April 2016 in Brazilian Portuguese, English, or Spanish.
Search Strategies
The search strategy termed “PICO” was used where “P” represents patient, “I” intervention, “C” comparison, and “O” outcome. The search strategy utilized Descriptors in Health Sciences and Medical Subject Headings, which were combined with the Boolean operators (AND, OR). The terms used were “Stroke,” “Virtual Reality Exposure Therapy,” “Video Games,” “Feedback Sensory,” “Postural Balance,” “Postural Equilibrium,” “Virtual Reality,” and “Visual Biofeedback.” These terms were used in the following combinations: “Stroke” AND (“Virtual Reality Exposure Therapy” OR “Video Games” OR “Feedback Sensory” OR “Virtual Reality” OR “Visual Biofeedback”) AND “Postural Balance” as well as “Stroke” AND “Video Games” AND “Postural Equilibrium.” The search strategy was applied in the following databases: PubMed, Latin-American and Caribbean Literature in Health Sciences, Scientific Electronic Library On-line, and Physiotherapy Evidence Database.
Selection of Studies and Extraction of Data
The selection and methodological evaluation of the articles were carried out by two independent reviewers (K.T.K. and V.F.), and a third reviewer (M.C.A.) was consulted in case of a disagreement regarding a study’s eligibility. Initially, the titles and abstracts were screened to identify studies that analyzed the effects of interactive video games (e.g., Nintendo Wii and Xbox with Kinect sensors) on functional balance (evaluated by the Berg Balance Scale [BBS]) and mobility (evaluated by the Timed Up and Go Test [TUGT]) in individuals poststroke. Articles with a study population other than individuals poststroke (e.g., elderly or those with Parkinson’s disease) were excluded by screening the titles and abstracts. Subsequently, full-text articles of eligible studies were accessed to establish whether they meet all the inclusion criteria. To ensure that all potentially eligible scientific articles in the literature were considered, a manual search was performed in the bibliographic references of the selected studies.
Description of Methodological Quality
The included randomized clinical trials were evaluated methodologically using the PEDro Scale (Shiwa, Costa, Moser, Aguiar, & Oliveira, 2011), which consists of 11 items, all based on the Delphi list, except for Criteria 8 and 10. The evaluation criteria of the methodological quality were as follows: (1) specification of the origin of the subjects and requirements for the study, (2) random allocation of subjects to groups, (3) person who determined eligibility of subjects was unaware of their group allocation, (4) study groups presented similar prognoses at the beginning of the study, (5) the study subjects participated “blindly,” (6) therapists administered the study “blindly,” (7) the evaluators measured the key results “blindly,” (8) key results were attributed to 85% of the subjects distributed in the groups, (9) all subjects included in the results received the treatment or control condition according to the group, if not, the data were analyzed for intention to treat, (10) the results of the statistical comparisons were described by the key result, and (11) measures of precision and variability in the key result were presented (Shiwa et al., 2011).
The PEDro Scale uses a procedure that evaluates an article according to its score on the 11 criteria. The article is allocated 1 point for each of the 11 criteria met and 0 points for each criterion not met. Thereafter, the score is summed with the maximum score being 10 as criterion number 1 is not included in the final score. Evaluated articles with a total score close to the maximum (10) are considered to have high methodological quality, while articles with a total score close to the minimum (0) are considered to have low quality.
The PEDro Scale was chosen to assess clinical trials because it is appropriate for assessing methodological quality of studies with an intervention in addition to being quick and easy with high reliability (de Morton, 2009; Shiwa et al., 2011).
Statistical Analysis
Functional balance was evaluated using the BBS and mobility using TUGT. The mean differences and 95% confidence intervals (CIs) were calculated by the inverse variance method (Dersimonian & Laird, 1986; Follmann, Elliott, Suh, & Cutler, 1992). The BBS has predictive validity and the ability to detect changes after interventions in individuals with stroke; a score from 0 to 19 on this scale indicates a high risk of falls, 19 to 24 a moderate risk of falls, and 24 to 28 a low risk of falls (Chou et al., 2006; Juneja, Czyrny, & Linn, 1998; Mao, Hsueh, & Tang, 2002). According to Gervasoni, Jonsdottir, Montesano, and Cattaneo (2017), the minimal clinically important difference for change on the of BBS is three points for patients with multiple sclerosis.
It has been documented that individuals with poor TUGT performance and longer duration since the onset of injury demonstrate particularly high fall rates (Pinto et al., 2014). In the TUGT, individuals with an accomplishment time of less than 10 s have a low risk of falls, 20–29 s an average risk of falls, and more than 30 s a high risk of falls (Barry et al., 2014; Bischoff et al., 2003).
The random effects model was utilized for analyses and to obtain summary effect measures (Kelley & Kelley, 2012). The heterogeneity between the studies was determined through T 2 and I 2 statistics, accompanied by visual inspection of the forest plot (Follmann et al., 1992). The publication bias was evaluated through analysis of the funnel plots. To adjust for possible publication bias, the trim and fill method was used. Analyses were performed using the R statistical software, Version 3.3.1. The α level was set at .05 for statistical significance.
Results
The search strategy yielded 118 studies and another 2 were found by manually searching the bibliographic references. Afterward, one study was excluded due to duplication and 119 articles remained. Of these, 25 articles were selected after screening the titles and abstracts and their full-text articles were read. Subsequently, 14 of the 25 studies were excluded for the following reasons: did not present a control group, did not use the Nintendo Wii or Xbox with Kinect sensors interactive game types, did not analyze the improvement in functional balance and mobility, or associated the use of interactive video games with interventions rather than conventional physiotherapy. Thus, 11 studies met the inclusion criteria and were included in this systematic review (Barcala, Grecco, Colella, Lucareli, & Oliveira, 2013; Bower, Clark, McGinley, Martin, & Miller, 2014; Cho & Lee, 2013; Cho, Lee, & Song, 2012; Fritz, Peters, Merlo, & Donley, 2013; Hung et al., 2014; Kim, Park, & Lee, 2015; Lloréns et al., 2015; McEwen, Taillon-Hobson, Bilodeau, Sveistrup, & Finestone, 2014; Morone et al., 2014; Rajaratnam et al., 2013). The complete flowchart of the studies’ selection for the meta-analysis is shown in Figure 1.
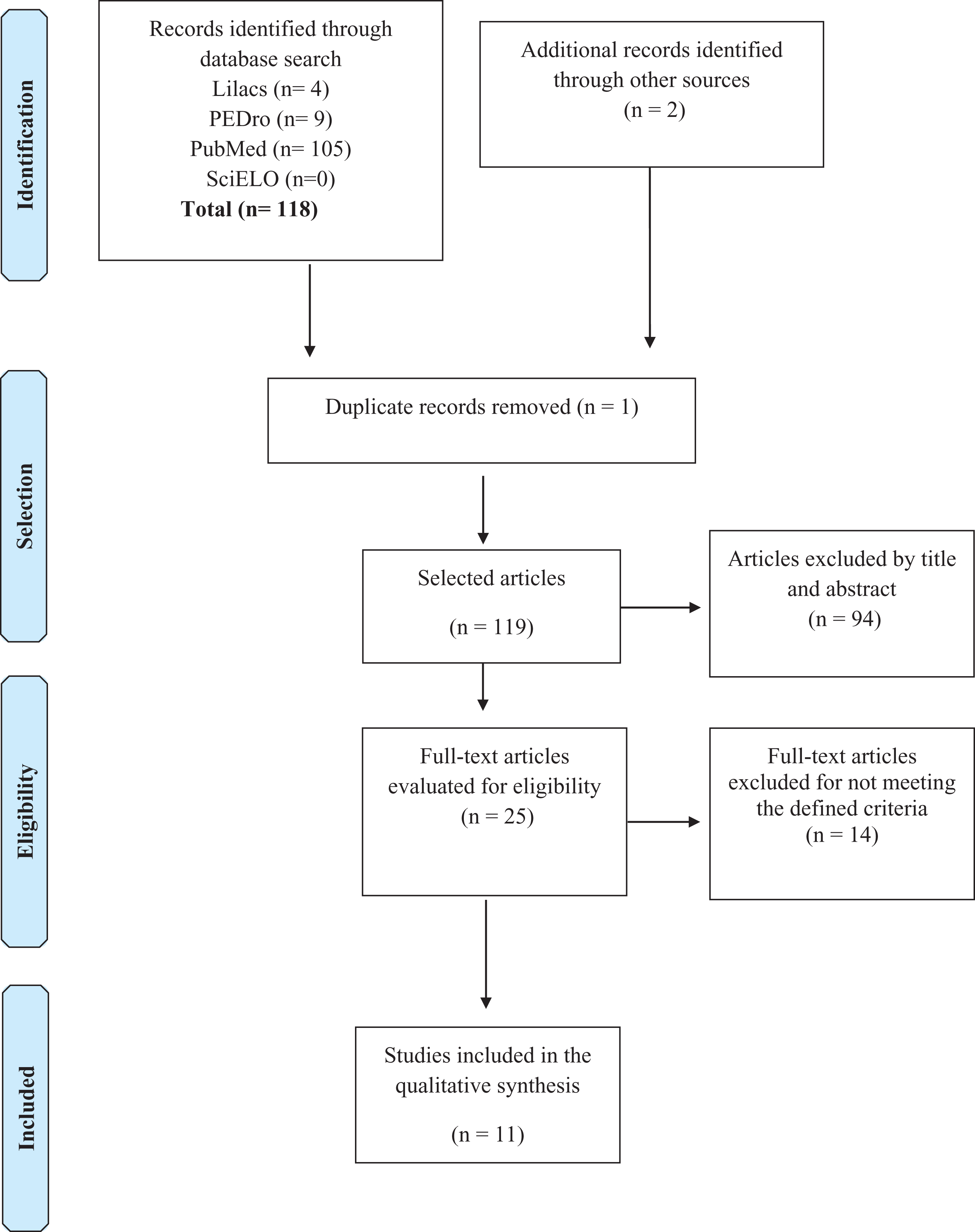
Flowchart of the selection of included studies.
The characteristics of the 11 selected studies are displayed in Table 1, outlining the names of the authors, number of participants per study, classification of injury time, outcome analyzed, type of intervention performed both in the study group and in the control group, duration of treatment, and the results.
Description of the Studies Included in the Systematic Review.
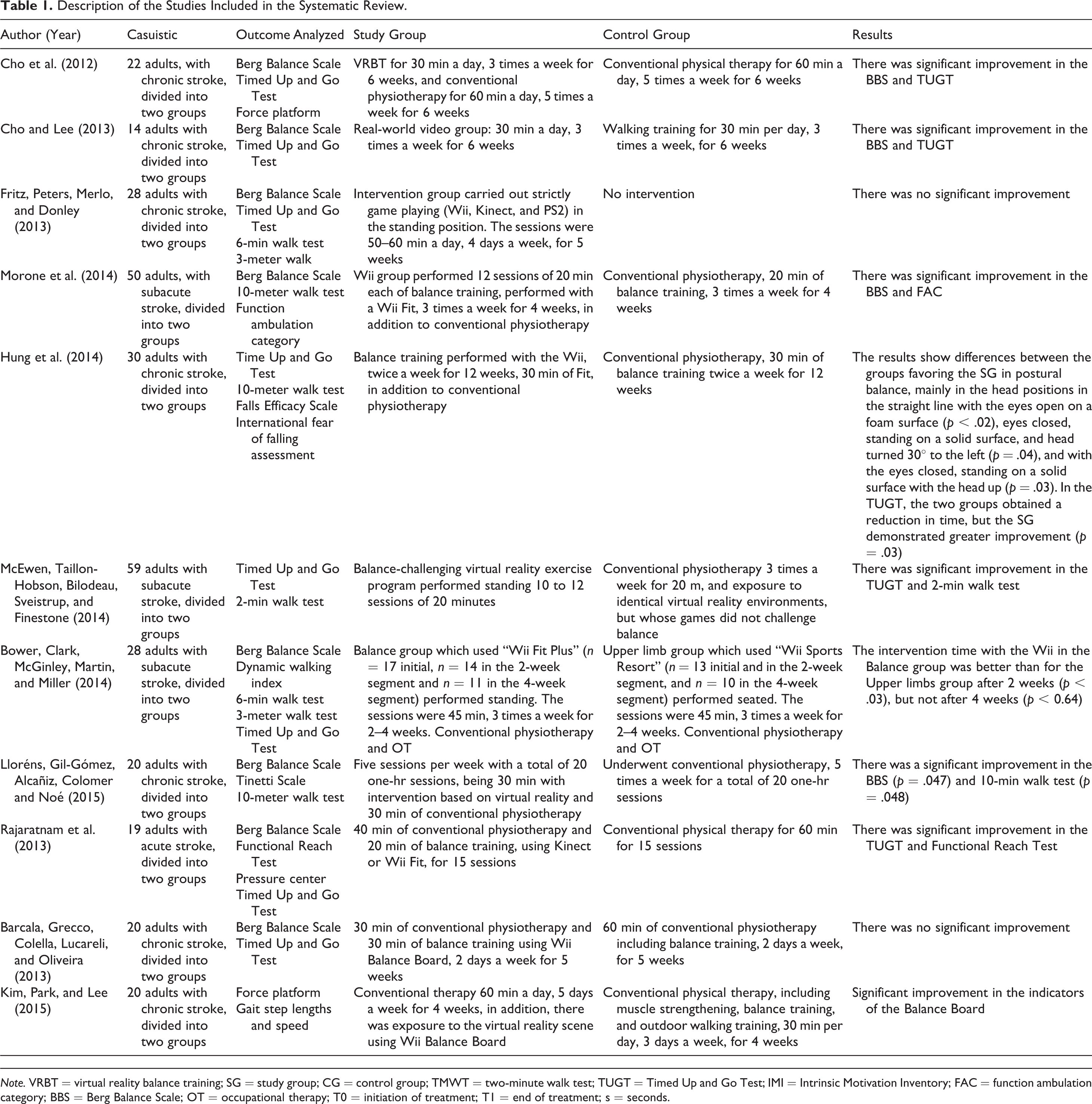
Note. VRBT = virtual reality balance training; SG = study group; CG = control group; TMWT = two-minute walk test; TUGT = Timed Up and Go Test; IMI = Intrinsic Motivation Inventory; FAC = function ambulation category; BBS = Berg Balance Scale; OT = occupational therapy; T0 = initiation of treatment; T1 = end of treatment; s = seconds.
The mean score of the methodological quality of the studies evaluated using the PEDro Scale was 6.2 ± 1.9, with only one study achieving a score of 3, two studies scoring 4, one study scoring 5, three studies scoring 7, and four studies scoring 8 (Table 2).
Description of the Methodological Quality of the Studies According to the PEDro Scale.
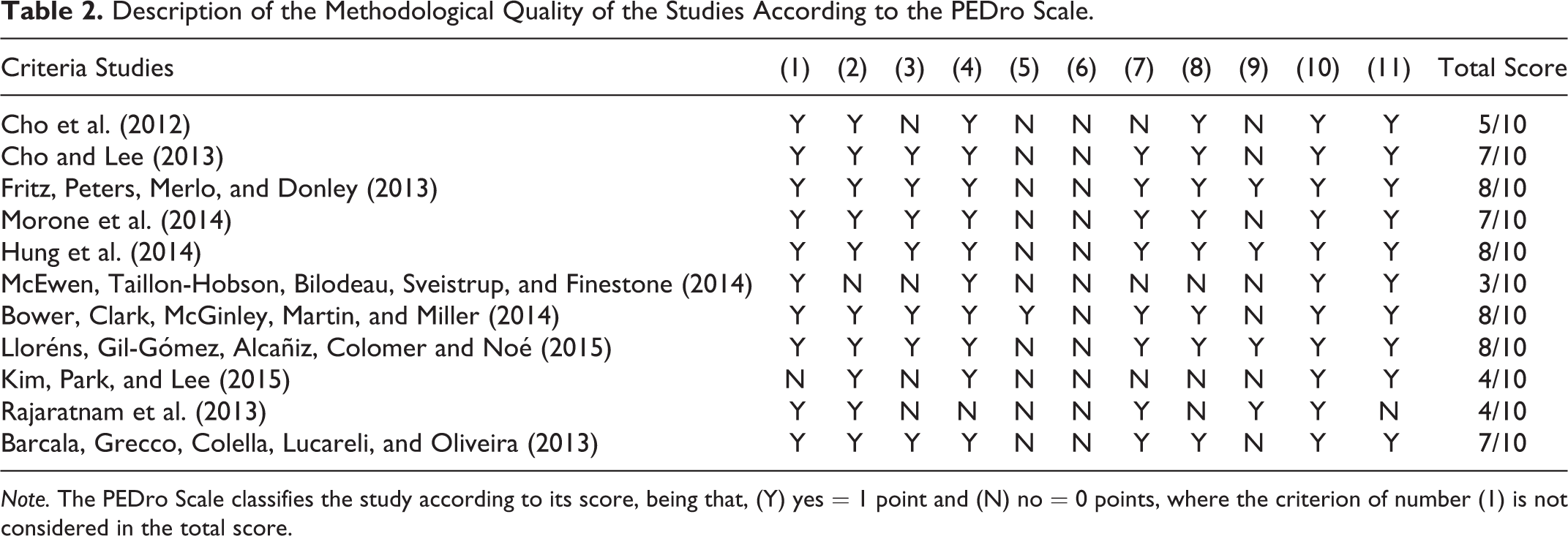
Note. The PEDro Scale classifies the study according to its score, being that, (Y) yes = 1 point and (N) no = 0 points, where the criterion of number (1) is not considered in the total score.
Meta-Analysis of the Effects of Interactive Video Games on the Functional Balance of Individuals Poststroke
The summary effect from the meta-analysis (Figure 2) indicated a mean difference of 2.24 (95% CI [0.45, 4.04], p = .01) demonstrating that the treatment with interactive video games improved functional balance of individuals with stroke compared to the control treatment. The heterogeneity (I 2) of 24% is considered low. Two studies showed a significant improvement in functional balance (3.33%) in the treatment groups with interactive video games compared to their respective controls (Figure 2). Additionally, the funnel plot did not suggest evidence of publication bias (Figure 3A).
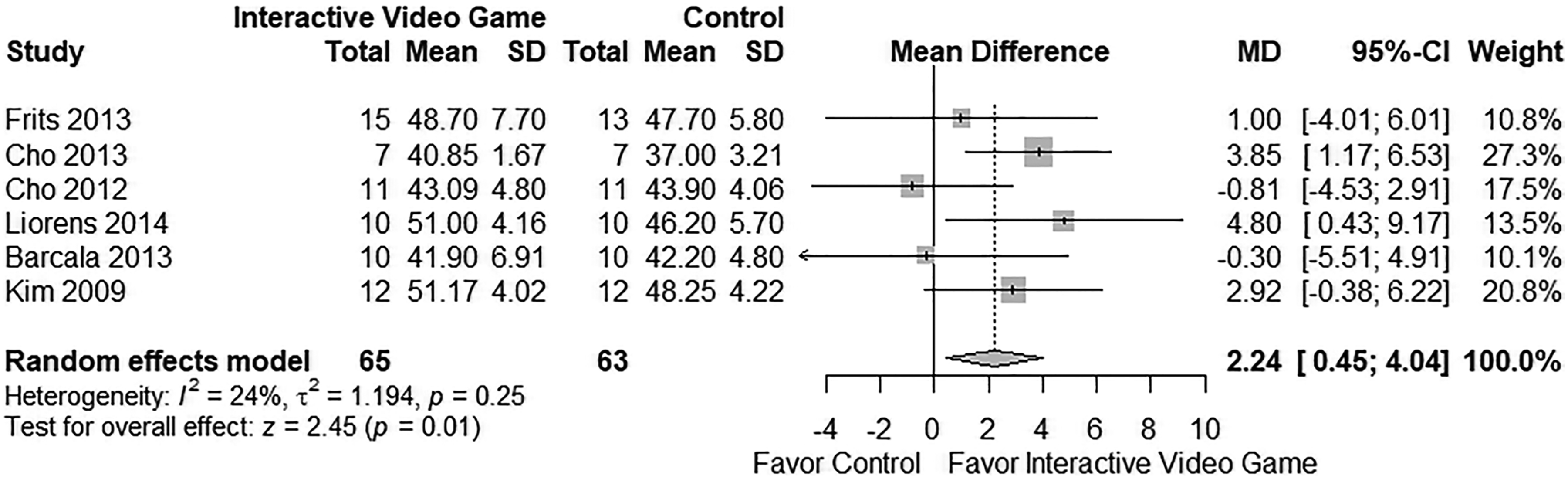
Forest graph of the rehabilitation effects of using interactive video games over the BERG Balance Scale. The effects to the right of the vertical line of the figure indicate favorable results for functional balance and mobility.

Funnel graph of publication bias. (A) Studies using interactive video games over the Berg Balance Scale. (B) Studies using interactive video games over the Timed Up and Go Test. Dark gray “.1 > p > .05”; gray “.05 > p > .1”; Light gray “<.01.”
Meta-Analysis of the Effects of Interactive Video Games on the Mobility of Individuals Poststroke
The summary effect from the meta-analysis (Figure 4) indicated a mean difference of 0.51 (95% CI [−2.66, 1.64], p = .74) demonstrating the absence of a significant rehabilitation effect of interactive video games on the mobility of individuals poststroke. The I 2 statistic (0%) indicated no heterogeneity. The funnel plot suggested publication bias; however, the trim and fill method adjusted for publication bias (Figure 3B).
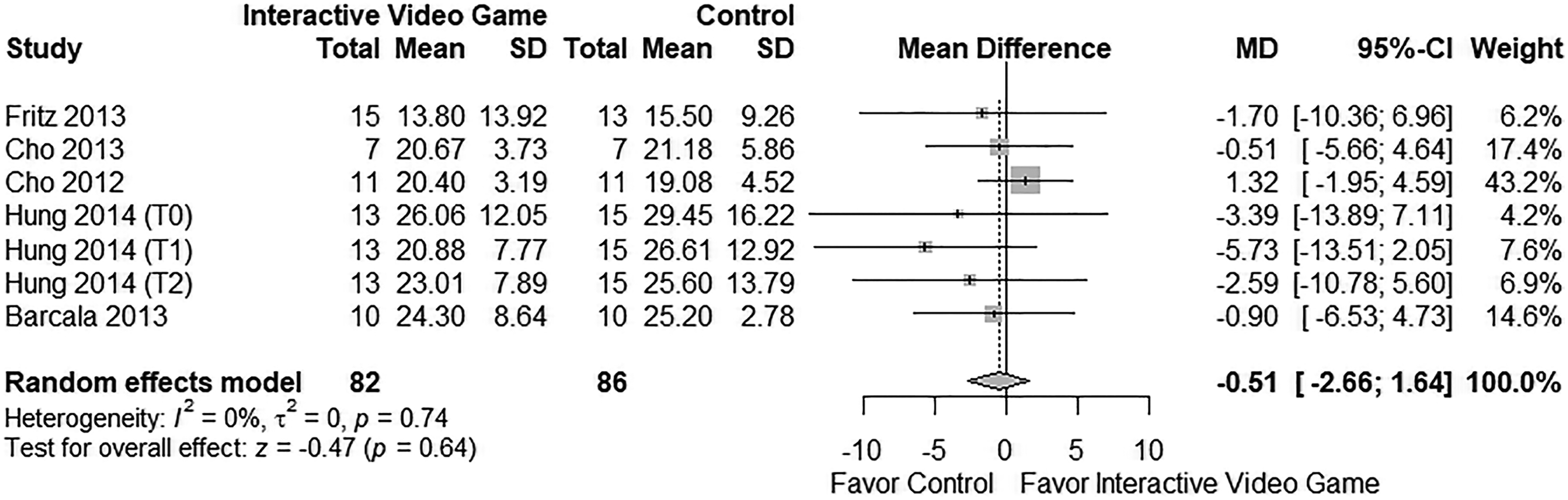
Forest graph of the rehabilitation effects of using interactive video games over the Timed Up and Go Test in individuals with stroke.
Discussion
This systematic review with meta-analysis provided clinical evidence that treatment with interactive video games may be effective in improving functional balance of individuals poststroke. Clinically, the results indicated that interventions with interactive video games are more beneficial compared to the presence or absence of any other type of intervention. Improved functional balance is especially beneficial for individuals with stroke since they have impaired functional balance and a significant risk of falls (Subramaniam & Bhatt, 2015).
In addition, the I 2 statistic (24%) indicated that the studies are similar in methodological terms, making it possible to combine the data in the meta-analysis. These data attest to the similarity between the studies included in this systematic review, guaranteeing the absence of clinical and statistical heterogeneity and thus supporting the clinical evidence that interventions with interactive video games are beneficial for individuals poststroke to improve functional balance.
The lack of blinding of therapists or poststroke individuals in all but one study (Bower et al., 2014), may have introduced bias in the results of the meta-analysis. However, it is worth mentioning that the blinding of participants and therapists is often impractical in interventions that involve rehabilitation using interactive video games. Moreover, Fritz, Peters, Merlo, and Donley (2013) had no intervention in control groups which may also introduce possible bias and compromise the effect analysis of the interactive video games. On the other hand, despite the presence of some methodological limitations, the mean PEDro score was 6.2, which represents high methodological quality (Canadian Partnership for Stroke Recovery, n.d.—PEDRo score) of the studies included in the meta-analysis.
In regard to the populations of the 11 studies included in the analyses, seven articles studied individuals with chronic stroke with 6 months to at least 1 year of injury (Barcala et al., 2013; Cho & Lee, 2013; Cho et al., 2012; Fritz et al., 2013; Hung et al., 2014; Kim et al., 2015; Lloréns et al., 2015), three studied subacute stroke with 1 to 2 months of injury (Bower et al., 2014; McEwen et al., 2014; Morone et al., 2014), and one study included individuals with acute stroke with less than 16 days of injury (Rajaratnam et al., 2013). The differences in the poststroke periods appeared not to have influenced the potential recovery, since low heterogeneity was observed among the studies.
Conventional physical therapy treatment for patients poststroke may include different strategies and techniques for improving motor control, such as physical exercise and functional electric stimulation (Dobkin, 2004; Veerbeek et al., 2014). However, as an alternative to conventional therapy, the interactive video games presented promising results when comparing pre and posttreatment; moreover, some studies presented superior results for the treatment group compared to the control group treated with conventional therapy (Hung et al., 2014; Kim et al., 2015; Lloréns et al., 2015). These results may encourage clinicians to think about potentially incorporating commercial video gaming in rehabilitation programs, especially to increase motivation and adherence rate to conventional physical therapy treatments.
The present systematic review has several strengths: (1) a clearly defined objective, (2) a comprehensive and systematic study search, with explicit and reproducible eligibility criteria without language restrictions, and (3) selection of included studies by two independent authors. On the other hand, the low number of studies included in this review may limit the findings. An attempt to access additional data for inclusion in the meta-analysis was made by contacting the authors of another study (Morone et al., 2014), but no response was received.
This meta-analysis of randomized controlled trials provided clinical evidence on the efficacy of treatment with interactive video games aimed at improving functional balance in poststroke individuals when compared to other or absence of interventions but did not influence the mobility of individuals poststroke. Thus, clinical studies with high methodological quality are still necessary to establish whether interactive video games result in mobility improvement of individuals poststroke. Interactive video games represent a viable option for therapy to improve patient care, adopt available technology in rehabilitation therapy, and customize treatment of patients with neurological disorders using functional and dynamic exercises (Cho & Lee, 2013).
Footnotes
Authors’ Note
Vilma Ferreira and Karina Tamy Kasawara developed the research question and the study design. Two independent researchers, Vilma Ferreira and Karina Tamy Kasawara, performed the search strategy into scientific databases, whereas Mariana Cunha Artilheiro was consulted in cases of disagreements regarding inclusion of studies in this systematic review. Nelson Carvas performed all the statistical analysis. José Eduardo Pompeu substantially contributed to data interpretation and manuscript preparation. Vilma Ferreira and Karina Tamy Kasawara, Mariana Cunha Artilheiro and Nelson Carvas wrote the first draft of the manuscript. Syed Ahmed Hassan reviewed, edited, proofread, and provided feedback on the manuscript. All authors approved the last version of the manuscript before submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Systematic review registration number: PROSPERO CRD42015024685.