
Abstract
The optimal provision of pharmaceutical care services requires an adequate number of pharmacists, satellite pharmacies and service units at healthcare facilities. We examined the availability of these requirements at Nigerian hospitals using the 2016 nationwide inspection reports of hospital pharmacies conducted by the Pharmacists Council of Nigeria. Records of 254 hospitals inspected were retrieved, of which 171 (67.3%) were public. The total number of pharmacists across facilities was 753. The most common satellite pharmacy units recorded were antiretroviral 80 (31.5%) and emergency departments 48 (18.8%). The most common service units were drug revolving funds 176 (69.3%) and drug information 112 (44.1%) units. These findings suggest the availability of pharmacists, satellite pharmacies and service units are inadequate for the optimal delivery of pharmaceutical care services at healthcare facilities in Nigeria. Therefore, there is a need for interventions to improve the provision of pharmaceutical care services at health care facilities in Nigeria.
Introduction
The optimal provision of pharmaceutical care (PC) services is fundamental to any healthcare system (WHO, 2011). PC is the responsible provision of drug therapy to achieve definite outcomes that improve the patient’s quality of life (Al-Quteimat & Amer, 2016). Achieving these outcomes in the hospital depends on the availability of the pharmacists, service units and other pharmaceutical care services. The minimum requirements for these standards are determined and regulated by the Pharmacists Council of Nigeria (PCN). The PCN is a statutory agency of the Federal Government of Nigeria, saddled with the responsibilities for the regulation of pharmacy in all its aspect and ramifications (PCN, 2020).
The PCN conducts nationwide inspections of hospital pharmacies in Nigeria every 2 years to ensure compliance with the minimum requirements for hospital pharmacy practice in Nigeria (PCN, 2009). Over the past few years, the PCN has been performing these inspections across the country. However, the findings from this exercise have not been published. The study aimed to evaluate the availability of service units and satellite pharmacies at hospitals in Nigeria, drawing on the PCN reports on nationwide hospital pharmacy inspections. Specifically, we examined the distribution of facilities, the types of facilities, the numbers of pharmacists and the services provided.
Method
This study utilized reports of the 2016 PCN nationwide inspection of hospital pharmacies in Nigeria. The inspection involved interviewing the head of the pharmacy department of each facility visited and assessing their services using the PCN-scoring format. This assessment contains questions pertaining to the availability of facilities, personnel and services in the facility. Other information in the facility was collected based on physical observations. Facilities were then graded as “full,” “provisional” or “not recommended” for registration based on their final score.
In this study, the results from these assessments were extracted from PCN inspection reports. Data pertaining to the hospital pharmacies inspected from 12 states of the 6 geographical zones of Nigeria was included. Information regarding the type of facility (public, private, faith-based and staff clinic of corporate organizations), the number of pharmacists in the facility, the availability of satellite pharmacies (such as emergency, pediatric, geriatric, antiretroviral therapy units, in-patient, and intensive care unit), and service units (such as drug revolving funds (DRF)—a funding scheme for the provision of essential drugs and medical consumables, research laboratory, drug information unit, drug procurement unit and pharmacovigilance unit) were collected. The operational definitions of the service units and satellite pharmacies are provided in Appendix A. The PCN’s Four-Part Compendium Of Minimum Standards Form The Assurance Of Pharmaceutical Care In Nigeria was used to determine the minimum number of service units, satellite pharmacies and pharmacists required in the facilities visited (PCN, 2012).
Ethical Approval
The study was approved by the PCN. However, the protocol was exempted from formal review and approval by the Council research ethics committee as it did not involve the use of identifiable information of the participants or facilities.
Results
The records of 254 hospitals visited during the inspection period were retrieved, of which 171 (67.3%) were public, 62 (24.4%) were private, 17 (6.7%) were faith-based, and 4 (1.6%) were staff clinics. Most of the facilities visited were in the South-West region 94 (37.0%), followed by North-West 41 (16.1%) and then North-Central 40 (15.7%). The total number of pharmacists in the facilities visited was 753. These pharmacists were predominantly based in the South-West 116 (45.6%), North-Central 46 (18.2%) and North-West 40 (15.9%) regions. None of the hospitals met the required number of pharmacists based on the PCN minimum standards of pharmacy practice in Nigeria. Table 1 illustrates the distribution of pharmacists in the facilities by region.
Satellite Pharmacies, Service Units and Pharmacists Available At The Hospitals Visited.
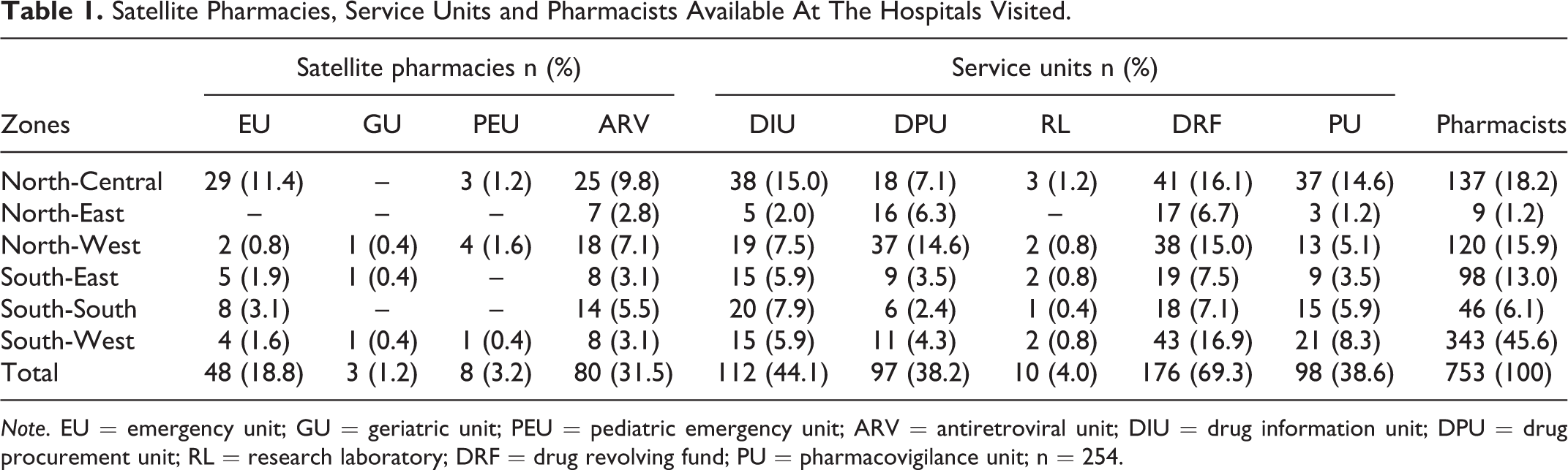
Note. EU = emergency unit; GU = geriatric unit; PEU = pediatric emergency unit; ARV = antiretroviral unit; DIU = drug information unit; DPU = drug procurement unit; RL = research laboratory; DRF = drug revolving fund; PU = pharmacovigilance unit; n = 254.
Satellite Pharmacies and Service Units in the Facilities Visited
The satellite pharmacies available at the facilities visited were antiretroviral, pediatric emergency, geriatric and emergency units. Antiretroviral units were available in 80 (31.5%) of the facilities visited, and these were the most common of all satellite units, followed by emergency units 48 (18.8%). Pediatric emergency and geriatric units were available at 8 (3.1%) and 3 (1.2%) hospitals, respectively.
In terms of the distribution of the most commonly available satellite pharmacies based on geopolitical regions, emergency, antiretroviral and paediatric emergency units were seen at the facilities visited in the North-Central region of Nigeria. An antiretroviral unit was the only satellite pharmacy observed at the inspected facilities in the North-East region. There were no geriatric units found at hospitals visited in the North-Central, North-East and South-South regions. Furthermore, there were no pediatric units seen at facilities inspected in the North-East, South-East and South-South geopolitical regions whereas at least one pediatric unit was noted in all satellite units inspected in the South-West region.
Service units were observed in almost all the facilities inspected. The most common service unit available among the facilities visited was the DRF 176 (69.3%), followed by drug information units 112 (44.1%). The availability of pharmacovigilance units was 98 (38.6%). Drug procurement unit availability was 97 (38.2%), and research laboratories were available in 10 (3.9%) facilities inspected.
Discussion
To our knowledge, this is the first published notes from the field on the availability of satellite pharmacies, service units, and pharmacists at hospitals using data from PCN nationwide inspection of hospital pharmacies in Nigeria. Outcomes of this study will guide the design and implementation of strategies and policies for delivering quality pharmaceutical care services in Nigeria.
The facilities visited during the nationwide inspection of hospital pharmacies were predominantly public. This result is consistent with the distribution of health facilities in Nigeria (Makinde et al., 2018). Therefore, interventions to improve pharmaceutical care services in Nigeria should be mainly targeted toward public hospitals.
The PCN “4-part Compendium for the Minimum Standards of Pharmacy Practice in Nigeria” provides the minimum number of pharmacists for each hospital category based on the bed capacity of the facility (PCN, 2012). In this study, none of the facilities satisfied the minimum number of pharmacists required in hospitals. This human resource deficit is critical to address given the significant role of pharmacists in the provision of pharmaceutical care in hospitals. Therefore, there is a need for more hospital-based pharmacists for the optimal delivery of pharmaceutical care services in the healthcare facilities in the country.
An adequate enabling environment is necessary for achieving successful pharmaceutical care. Our study identified limited facilities, particularly the pharmacy service units, that are essential for the provision of pharmaceutical care. Drug revolving funds were the most common service units observed in the facilities visited, particularly in public hospitals. This high frequency may be related to compliance with the National Drug Policy of the Federal government of Nigeria (Ogbonna et al., 2015).
Approximately 44% of the total facilities visited had drug information and pharmacovigilance units. These units are fundamental in the provision of pharmaceutical care given the high prevalence of reported drug-related problems in Nigeria (Samaila et al., 2018). Research laboratories were the least available service unit observed among the hospitals visited. According to the provision of PCN, only tertiary and specialist hospitals are required to have research laboratories. This provision may be the reason for the lower percentage of research laboratories observed in these facilities. Given the increasing number of fake and counterfeit drugs in circulation in Nigeria (Erhun et al., 2001), there is a need for more facilities to have research laboratories in order to oversee the quality control of drugs supplied to the hospitals.
There was a shortage of satellite pharmacies in most of the facilities visited. The most commonly available satellite pharmacy was antiretroviral units. A possible explanation to this finding may be the influence of donor organisations towards HIV/AIDS management in Nigeria, with most of the antiretroviral units supported and funded by the Non-governmental Organizations (Adefemi et al., 2017).
Implication
Findings from this study could guide and inform policy direction towards improving healthcare in Nigeria, particularly in the hospital pharmaceutical care services. Our study has identified gaps in the pharmaceutical care service provision in Nigeria that could guide future studies, policies and interventions for improving patient outcomes.
Conclusion
The findings from the PCN nationwide inspection of hospital pharmacies suggest the need to improve the number of pharmacists, satellite pharmacies and pharmacy service units at healthcare facilities in Nigeria. Therefore, policies and intervention are needed in this direction when working toward improving pharmaceutical care services at these facilities in Nigeria.
Supplemental Material
Supplemental Material, 5_Appendix_A_-_Copy - Notes From the Field: Availability of Satellite Pharmacies and Pharmacy Service Units in Nigerian Hospitals—Implications for Pharmaceutical Care
Supplemental Material, 5_Appendix_A_-_Copy for Notes From the Field: Availability of Satellite Pharmacies and Pharmacy Service Units in Nigerian Hospitals—Implications for Pharmaceutical Care by Ene Daniel-Ebune, Abubakar Ibrahim Jatau, Sai’du Lawal Burji and Mustapha Mohammed in Evaluation & the Health Professions
Footnotes
Acknowledgments
The authors would like to thank and acknowledge the Registrar, Pharmacists Council of Nigeria (PCN) for the support in conducting this study. The efforts of the PCN inspection team and the Head of Pharmacy Practice PCN is highly appreciated. The authors would also like to thank and appreciate the efforts of Olive Schmid of the University of Tasmania for the English language editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.