
Abstract
Valid and reliable measurement tools are necessary for pain assessment among the elderly with dementia. This study aimed to translate the Mahoney Pain Scale (MPS) into Persian and evaluate its psychometric properties among Iranian elderly with dementia. In this methodological study, after translating and assessing the face and content validity of MPS, 100 elderly with dementia were selected via convenience sampling from nursing homes and clinics in Kashan in 2018–19; then, MPS was completed for them both at rest and during a movement pain protocol. MPS was assessed by exploratory factor analysis, known-group comparison, convergent validity, internal consistency, equivalence, and stability. The factor analysis revealed a one-factor structure, which explained 57.11% of the total variance. The Persian MPS differentiated patients with and without known painful conditions, as well as pain at rest and during the movement pain protocol (p < .0001). There was a significant positive correlation between the scores of MPS and PACSLAC-II (r = .87, p < .0001). The Cronbach’s α, intraclass correlation coefficient and standard error of measurement of MPS were .91, .79, and ±1.37, respectively. As a valid and reliable tool, the Persian MPS can be used for pain assessment among Iranian elderly with dementia.
Introduction
Pain is a common problem among the elderly with dementia, with a prevalence of ∼28%–83% (Li et al., 2015; Makino et al., 2019). Studies in Iran on the community-dwelling elderly reported a pain prevalence rate of 79.8%–82.4%, though no specific rate has been reported for pain among the elderly with dementia (Nouhi et al., 2012; Taghipour et al., 2013).
Pain among the elderly with dementia has numerous consequences (Lichtner et al., 2014). It can alter the physiological rhythms of the body, cause functional impairment and depression, reduce the quality of life, increase the need for healthcare services, and thus increase healthcare-related costs (Zwakhalen et al., 2018).
An absolute prerequisite to effective pain management is an accurate pain assessment (Mahoney & Peters, 2008). Yet, due to misconceptions about pain and its management among the elderly, most healthcare providers pay limited attention, if any, to pain assessment (Schofield & Abdulla, 2018). Moreover, problems such as advanced cognitive, agitation, aggression, mood disorders, and pain make pain assessment among the elderly with dementia very difficult and may result in erroneous clinical decision-making (Lichtner et al., 2014; Schofield & Abdulla, 2018). Most healthcare providers attribute pain-related agitation to dementia, consider it inevitable and, hence, take no measure for pain management or inaccurately use antipsychotic agents to manage pain-related agitation (Husebo et al., 2010). The use of antipsychotic agents for agitation management is associated with different side effects, while pain and pain-related agitation can easily and effectively be managed using simple and safe measures (Corbett et al., 2012).
Pain assessment among the elderly with dementia needs an appropriate assessment tool (Mahoney & Peters, 2008). The gold standard for pain assessment is the self-report method. However, the use of this method for the elderly with dementia produces no reliable results due to problems such as aphasia, apraxia, and agnosia (Zwakhalen et al., 2018). Therefore, behavioral manifestations should be considered in pain assessment among these patients (Lichtner et al., 2014). The American Geriatrics Society determined six main groups of behaviors as the behavioral manifestations of pain among the elderly with dementia, based on which different tools were developed for pain assessment among these patients (Lichtner et al., 2014). However, pain assessment among these patients in Iran is still performed using non-specific tools (Nouhi et al., 2012; Taghipour et al., 2013). The only measure employed in this country for pain assessment among patients with dementia is the translated and psychometrically evaluated version of the Pain Assessment Checklist for Seniors with Limited Ability to Communicate II (PACSLAC-II). However, this checklist has some limitations, such as having too many items and complex concepts (Haghi et al., 2019).
In Iran, the elderly with dementia are mostly cared for in homes and nursing homes by non-professional caregivers who have a low literacy level; therefore, in addition to covering a wide range of pain-related behavioral manifestations and having the acceptable psychometric characteristics, the appropriate tool for measuring pain should be short and clear and have simple words so that this group of caregivers can easily use it (Lichtner et al., 2014).
The Mahoney Pain Scale (MPS) has all these criteria and seems appropriate for pain assessment among the elderly, particularly in nursing homes. This scale, based on the claims of the tool developers (Mahoney & Peters, 2008), helps differentiate between pain and dementia-related agitation in the elderly with dementia. Also, the nature of the items is such that they can be used in all cultures. MPS was developed by Mahoney and Peters in 2008 in Australia for pain assessment among patients with advanced dementia. Despite its acceptable psychometric properties (Mahoney & Peters, 2008), MPS had not yet been translated from English into other languages, including Persian. Given the strengths of the scale, the present study was conducted to translate MPS into Persian and evaluate its psychometric properties among the elderly with dementia in Iran.
Method
This methodological study was conducted in 2018–2019 in two main phases.
Phase One: MPS Translation
MPS was translated into Persian following Wild et al.’s approach (Wild et al., 2005). Initially, permission for MPS use was obtained from its developers; then, the translation steps, including “Preparation,” “Forward Translation,” “Reconciliation,” “Back Translation,” “Back Translation Review,” “Harmonization,” “Cognitive Debriefing,” “Review of Cognitive Debriefing Results and Finalization,” and “Proofreading” were performed. In the finalization step, the Persian MPS was assessed in a panel comprising the researchers and a Persian literature expert, and the final Persian translation of MPS was prepared for psychometric evaluation.
Phase Two: MPS Psychometric Evaluation
Face and content validity assessments
For face and content validity assessments, the Persian MPS was given to 10 experts in gerontology, psychology, psychiatric nursing, neurology, and psychometric evaluation. For qualitative content validity assessment, they were asked to comment on the understandability, grammar, wording, scoring, adequacy, clarity, and simplicity of the items (Ebadi et al., 2016). Their comments were used to revise the scale. Quantitative content validity assessment was performed through calculating the strict content validity ratio (CVR), content validity index (CVI), average scale-level CVI (S-CVIAverage), and modified κ statistic. For quantitative face validity assessment, the same experts were asked to rate the importance of each item and, then, based on the scores, the impact score was calculated (Almanasreh et al., 2019).
Regardless of the review conducted by the experts, to perform face validity assessment qualitatively, the first author held face-to-face interviews with 10 non-professional caregivers who varied from one another with respect to their age, sex, work experience, and educational level, and their perception of each item was compared with the actual item content (Mohammadbeigi et al., 2015).
Data collection for assessment of construct validity, reliability, and floor and ceiling effects
Due to the difficulty of the sampling process in this study, the minimum sample size was considered to be 100 cases. In this regard, Klein also notes that irrespective of the number of the items of the intended tool, a sample of 100 people is adequate for explanatory factor analysis (Kline, 2013).
The target population was the elderly with dementia. The eligibility criteria were age more than 60 years, a definite diagnosis of dementia by a neurologist based on interviews and computerized tomography data, not having intellectual disabilities, having a normal hearing ability, giving consent for participation (by the patient, his/her legal guardian, or authorities of the research setting), no intake of drugs with sedative effects during the 6 hours before the assessment, residence in the nursing home for at least 1 month before the study for residents, and having an eligible caregiver. The eligibility criteria for caregivers who gave care to the patients with dementia at home were caregiving for at least 4 days a week for one whole month, and the eligibility criteria for caregivers in nursing homes were caregiving for at least four work shifts a week for 1 month. The exclusion criterion was the voluntary withdrawal of the participant or his/her caregiver/guardian from the study. Sampling was conveniently done from December 2018 to June 2019 in two nursing homes and a private neurology clinic in Kashan, Iran.
For data collection, permissions and letters of introduction were obtained from the Vice-Chancellor of Research and Technology of Kashan University of Medical Sciences, Kashan, Iran, and given to the authorities of the research setting. A list of the elderly was created and their guardians were invited over the telephone for participation and eligibility assessment. An appointment for assessment was made with each participant’s guardian. Then, the researchers attended the appointment for data collection. The first author collected the data through observation of participants, interviewing them and their caregivers, and referring to their medical records. Four measurement tools were used.
A personal characteristics questionnaire: This questionnaire included items on age, sex, marital status, educational level, employment status, place of residence, history of known painful conditions, and the name of the afflicting painful conditions.
Persian-Clinical Dementia Rating (P-CDR): This valid and reliable scale was employed to determine dementia severity. It has 75 items in six dimensions. The possible total score of the scale is 0–18. Scores of 0, .5–2, 2.5–4, 4.5–9, 9.5–15.5, and 16–18 are considered as normal, suspected, very mild, mild, moderate, and severe cognitive impairment, respectively (Sadeghi et al., 2012).
MPS: This scale has eight items in two main dimensions. The first dimension evaluates four pain-related behavioral patterns, namely facial expression, breathing, vocalization, and body language. The second dimension evaluates behavioral changes, functional changes, physiological changes, and past and current medical status in order to evaluate and differentiate pain and agitation among patients with dementia. Each MPS item has four possible responses scored from 0 to 3. Scores 0–4, 4.5–8, 8.5–16, and 16.5–24 are considered as indicating no or limited pain, mild pain, moderate pain, and severe pain, respectively. The sum score of items 5–8 helps differentiate pain from dementia-related agitation (Mahoney & Peters, 2008).
PACSLAC-II: This checklist was utilized for convergent validity assessment (Chan et al., 2014). The Persian PACSLAC-II has 30 items scored either 0 or 1, resulting in a possible total score of 0–30 with higher scores showing severer pain. The validity and reliability of this scale were confirmed (Haghi et al., 2019). Reliability assessment in the present study revealed a Kuder-Richardson 21 statistic of .78 for the scale.
MPS and PACSLAC-II were completed for the participants both at rest and while performing Husebo et al.’s movement pain protocol (Husebo et al., 2010). This protocol was developed for pain assessment among patients with dementia and was successfully used in previous studies (Hadjistavropoulos et al., 2018). For precise pain assessment, the participants were filmed both at rest and during the protocol.
Assessment of construct validity and floor and ceiling effects
After data collection, construct validity was assessed through exploratory factor analysis, known-group comparison, and convergent validity assessment. Factor extraction in factor analysis was performed using the maximum likelihood method. The number of factors was determined using eigenvalue > 1 and the scree plot. The minimum factor loading value was estimated to be .52 based on this formula:
For construct validity assessment through the known-group comparison method, with the presumption that the movement pain protocol could probably cause or aggravate pain among the participants with known chronic painful conditions, MPS scores at rest were compared with MPS scores during the movement pain protocol. This comparison in the same group under different conditions can provide an opportunity to assess the responsiveness and capacity to detect pain changes, which is an important characteristic of pain assessment and is of utmost clinical relevance. Moreover, participants were divided into two groups, i.e. those with and those without known chronic painful conditions, and they were compared with each other with respect to their MPS scores during the movement pain protocol.
For convergent validity assessment, PACSLAC-II was completed for all the participants in addition to MPS during the protocol, and the correlation coefficient between their scores was calculated. The floor and ceiling effects were also assessed by calculating the frequency of the participants who had obtained the lowest and the highest possible scores of MPS (Ebadi et al., 2017).
Reliability assessment
The reliability of the Persian MPS was assessed via internal consistency, equivalence, and stability assessment methods. Internal consistency was assessed by calculating Cronbach’s α using the data collected from all the participants. For equivalence assessment, two raters (the first author and a qualified non-professional caregiver) simultaneously and independently assessed pain among 20 participants (selected from nursing homes) using MPS and, then, the inter-rater agreement value was calculated.
For stability assessment, the standard error of measurement (SEM) was calculated using this formula:
In all phases of this research, except for one method of construct validity assessment (i.e., comparing participants in two situations for known-group comparison), the data were collected during the movement pain protocol.
Data Analysis
The data were analyzed via SPSS (v.16). Numerical variables were described using mean and standard deviation, and categorical variables were described using absolute and relative frequencies. The Kolmogorov-Smirnov test was performed for normality testing. Moreover, the Spearman-Brown correlation analysis, Wilcoxon and Mann-Whitney U tests, Cronbach’s α, and intraclass correlation coefficient (ICC) and weighted κ were respectively used for correlation analysis between the scores of MPS and PACSLAC-II, known-group comparison, internal consistency assessment, and inter-rater reliability assessment. In all the analyses, the level of significance was set at < .05.
Ethical Considerations
This study has the approvals of the Vice-Chancellor of Research and Technology and the Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (codes: 9728 and IR.KAUMS.HUHEPM.REC.1397.015, respectively). Informed consent for participation was obtained from the participants’ legal guardians and, if they were inaccessible, from the authorities of the research setting. Moreover, informed consent was obtained from the elderly if they were capacitated. The guardians and caregivers were provided with explanations about the reasons for filming the participants during the movement pain protocol and they were ensured that the films would be confidentially assessed. If the guardians did not consent to taking the films out of the research setting, we watched and assessed the films in the research setting and then deleted them. The guardians had the right to reject participation in the study.
Results
Phase One: MPS Translation
The draft of the Persian MPS had eight items scored on a 4-point Likert scale.
Phase Two: MPS Psychometric Evaluation
Face and content validity assessment
In qualitative content validity assessment, minor revisions were made to the scale. For example, “looking blank” was revised to “blank expression”. Moreover, Item 8 was clarified by considering the number of painful conditions in item options (e.g., several painful conditions were considered equal to three or four cases). In quantitative content validity assessment, CVR and CVI values of all items were .8–1, modified κ statistic values were .79–1, and S-CVIAverage was .95. In qualitative face validity assessment, no change was made to the scale. In quantitative face validity assessment, the impact scores of all the items were > 1.5 (in the range of 4.23–5).
Assessment of construct validity and floor and ceiling effects
In total, 127 elderly individuals with dementia were assessed for eligibility. Twenty-four of them did not give consent for participation, and two suffered from intellectual disabilities and, therefore, were not included. Moreover, one participant was excluded due to his guardian’s refusal to remain in the study. Finally, the data obtained from 100 elderly with dementia were analyzed. Participants’ age was in the range of 63–95 years, with a mean of 87.31 ± 8.70 years. Other demographic characteristics are given in Table 1.
Participants’ Demographic Characteristics.
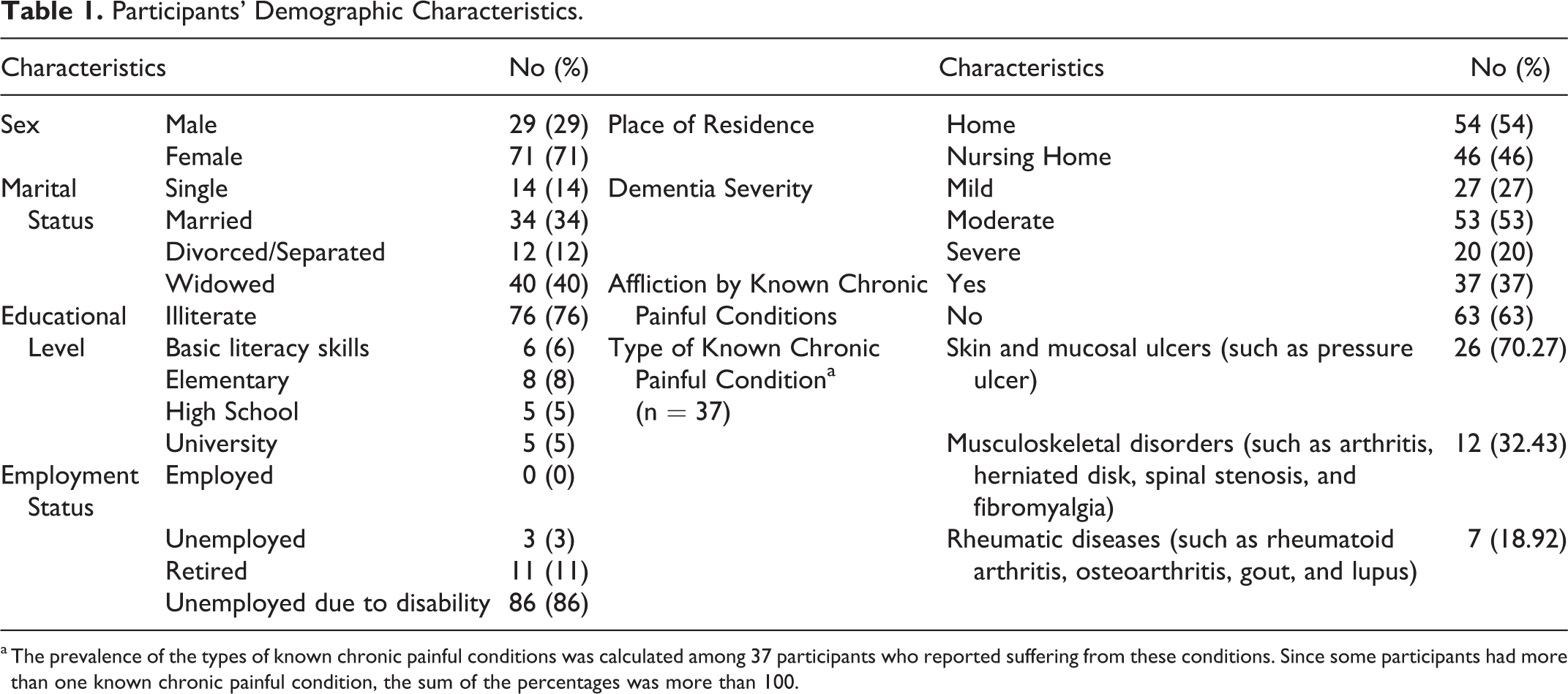
a The prevalence of the types of known chronic painful conditions was calculated among 37 participants who reported suffering from these conditions. Since some participants had more than one known chronic painful condition, the sum of the percentages was more than 100.
As for the appropriateness of factor analysis, the Kaiser-Meyer-Olkin statistic (= .87) confirmed the sampling adequacy, and Bartlett’s test showed that the correlation matrix was appropriate (χ2 = 505.88, p < .0001). During factor analysis, one factor with an eigenvalue of 4.57 was extracted, which explained 57.11% of the total variance (Figure 1 and Table 2).
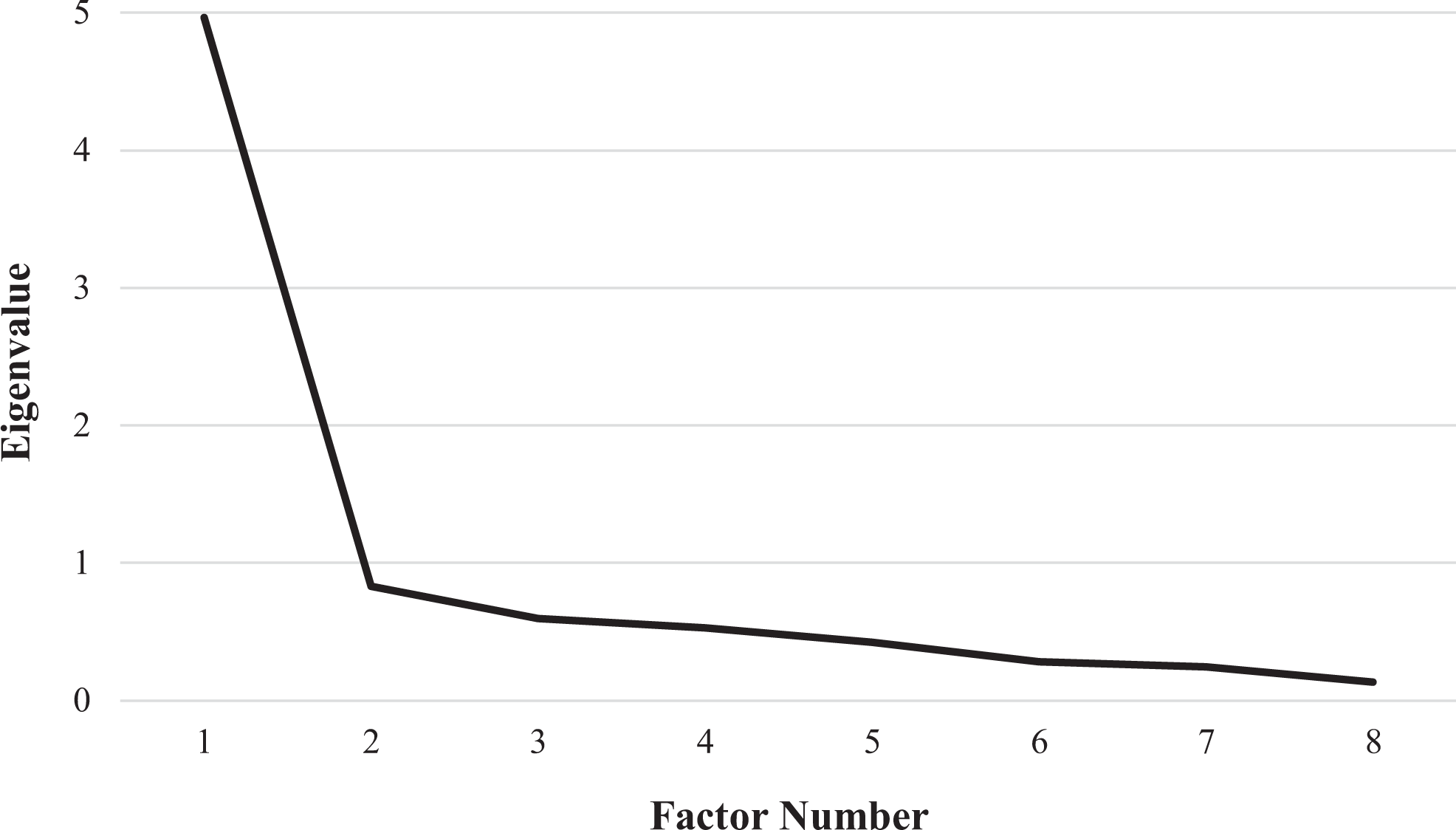
The scree plot of the Persian MPS.
Exploratory Factor Analysis (factor loadings and communalities) and Weighted κ values of the Persian MPS.
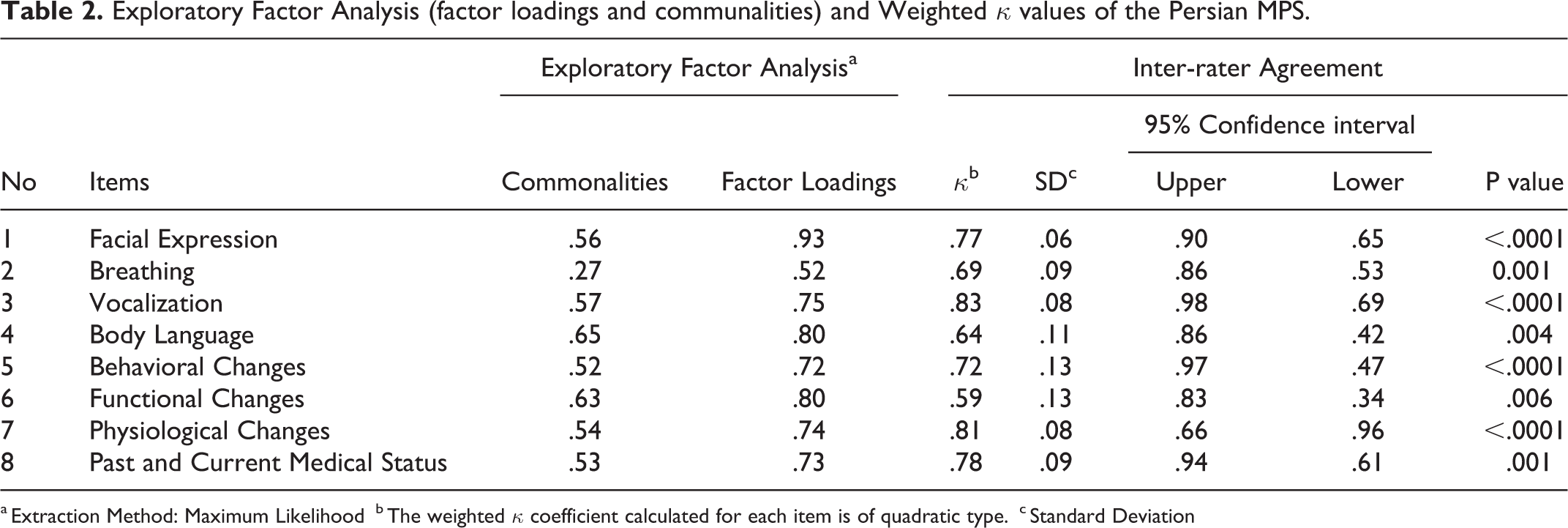
a Extraction Method: Maximum Likelihood
b The weighted κ coefficient calculated for each item is of quadratic type.
c Standard Deviation
Construct validity assessment through known-group comparison showed that the mean score of MPS at rest and during the protocol was 4.75 ± 4.29 and 6.66 ± 4.56, respectively. The Wilcoxon test showed that the difference between these two scores was statistically significant (p < .0001). Moreover, the mean score of MPS among participants with and without known chronic painful conditions was 11.11 ± 3.54 and 4.05 ± 2.69, respectively. The Mann-Whitney U test indicated that the difference between these two scores was statistically significant (p < .0001).
In convergent validity assessment, the mean scores of MPS and PACSLAC-II during the protocol were 6.66 ± 4.56 and 11.26 ± 5.43, respectively. There was a significant positive correlation between these scores (r = .87, p < .0001).
Assessment of floor and ceiling effects demonstrated that the relative frequencies of participants who had obtained the lowest and highest possible scores of MPS were 5% and 0%, respectively. As for pain severity, 40%, 26%, 32%, and 2% of the participants had no or limited pain (scores 0–4), mild pain (scores 5.4–8), moderate pain (8.5–16), and severe pain (16.5–24).
Reliability assessment
The Cronbach’s α of MPS was .91. Inter-rater ICC and inter-rater weighted κ values were respectively .79 (CI95%: .47–.92, p < .0001) and .59–.83 (p < .0001) (Table 2). The SEM, SDC, and MCID were ±1.37, 3.79, and 3.79, respectively.
Discussion
This study aimed to translate MPS into Persian and evaluate its psychometric properties among the elderly with dementia. The translation process was performed through a standard protocol that guaranteed the principles of cultural adaptation in the Persian version of the MPS and its understandable items (Tyupa & Wild, 2016).
The results of qualitative content validity assessment showed that the Persian MPS is comprehensive and adequately covers different aspects of the concept of pain among the elderly with dementia. Moreover, CVR, CVI, S-CVIAverage, and modified κ statistic values were higher than their minimum acceptable values, i.e. .8 (Ayre & Scally, 2014), .79 (Ebadi et al., 2016), .95, and .74 (Polit & Beck, 2017), respectively. Therefore, the content validity of the Persian MPS is confirmed.
No change was made to the Persian MPS during qualitative face validity assessment (Sousa & Rojjanasrirat, 2011). This finding may be due to the use of Wild et al.’s approach to translation, which includes cognitive assessment by the target population of the intended tool (Tyupa & Wild, 2016). Quantitative face validity assessment indicated that the item impact scores of all the items were > 1.5, which confirms the face validity of the scale (Ebadi et al., 2016).
Construct validity assessment through exploratory factor analysis revealed a one-factor structure for MPS, which included all MPS items and explained > 57% of the total variance. A variance of > 50% and high factor loadings are interpreted as an acceptable factor structure (Reio & Shuck, 2015). Therefore, the Persian MPS has acceptable construct validity.
Construct validity assessment through known-group comparison showed that MPS could differentiate pain at rest from pain during the movement pain protocol. Moreover, findings revealed that it could differentiate the elderly with and without known chronic painful conditions with respect to their pain severity during the movement pain protocol. These findings affirm that this tool can detect pain and pain aggravation. In line with our findings, Mahoney and Peters confirmed the construct validity of the scale through the known-group comparison method by comparing pain scores at rest and during activity (Mahoney & Peters, 2008).
The results of convergent validity assessment showed a significant positive correlation between the scores of MPS and PACSLAC-II (r = .87). A correlation coefficient of .5 confirms acceptable convergent validity (Post, 2016). Therefore, it can be concluded that MPS and PACSLAC-II measure the same concept (Waltz et al., 2010). Yet, MPS has fewer items than PACSLAC-II (eight vs. 30) and can differentiate pain from dementia-related agitation and, hence, has superiority over PACSLAC-II in pain assessment in nursing homes, particularly by non-professional caregivers. In line with our findings, Mahoney and Peters also reported the acceptable convergent validity of the original MPS (Mahoney & Peters, 2008).
The relative frequencies of participants who obtained the lowest and the highest possible scores of MPS in the present study were < 15%. Therefore, the Persian MPS has no floor and ceiling effects. The absence of floor and ceiling effects indicates the appropriateness of the items of the scale and confirms its content validity and stability (Ebadi et al., 2017).
The Cronbach’s α of the Persian MPS was .91. Cronbach’s α values > .7 denote acceptable internal consistency (Serbetar & Sedlar, 2016). Therefore, the Persian MPS has acceptable internal consistency. The difference between the Cronbach’s α values of the Persian and the original versions of MPS (= .76) (Mahoney & Peters, 2008) may be due to the differences between the characteristics of the samples of these two studies, such as dementia severity and place of residence.
The findings showed that the inter-rater ICC of the Persian MPS was .79. Inter-rater ICC values > .6 confirm acceptable reliability (Koo & Li, 2016). The weighted κ values of the Persian MPS were .59–.83, confirming the moderate to excellent agreement of the Persian MPS items (Streiner et al., 2015). Mahoney and Peters reported that the inter-rater κ values of the original MPS were .43–.85 (Mahoney & Peters, 2008). The difference between these two studies with respect to inter-rater agreement values may be due to the use of different methods for agreement assessment, as well as providing education for the rater and the limited number of raters in the present study.
The assessment of the absolute reliability of the Persian MPS revealed a standard error of measurement of ±1.38. This value denotes that if the scale is recompleted for each of the participants, its score may change by ±1.38 points. As the range of the possible total score of MPS is 0–24, a change of ±1.38 is trivial. Therefore, the Persian MPS has acceptable stability and reliability (Streiner et al., 2015). Also, the SDC and the MCID were 3.79 and 3.79, respectively. A larger MCID than SDC can support scale responsiveness.
Strengths and Limitations
The diversity of participants in terms of their characteristics was one of the strengths of the present study. One of the limitations was its rather small sample size. Moreover, some participants might have had undiagnosed chronic painful conditions. There was also the possibility of bias in collecting data during the process of assessing known-group comparison. Future studies are recommended to replicate the present study on larger samples of the elderly who have dementia with different severities. Furthermore, studies are needed to determine the ability of the Persian MPS to differentiate pain from dementia-related agitation.
Conclusion
The eight-item Persian MPS is a valid and reliable tool for pain assessment and can, therefore, be used by both professional healthcare providers (in hospitals or health centers) and non-professional caregivers (in homes or elderly care centers), with a brief instruction on how to complete it, for pain assessment among the elderly with dementia.
Footnotes
Acknowledgments
We would like to thank the developers of MPS, all elderly people, caregivers, and family members who participated in the study, and the vice-chancellor of Research and Technology of Kashan University of Medical Sciences, Kashan, Iran.
Ethical Approval
This study has the approvals of the vice-chancellor of Research and Technology and the Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (codes: 9728 and IR.KAUMS.HUHEPM.REC.1397.015, respectively).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the vice-chancellor of Research and Technology of Kashan University of Medical Sciences, Kashan, Iran [grant number 9728]. This article came from a Master’s thesis in geriatric nursing approved and financially supported by the abovementioned.