
Abstract
A single undiagnosed COVID-19 positive patient admitted in the green zone has the potential to infect many Health Care Workers (HCWs) and other patients at any given time with resultant spread of infection and reduction in the available workforce. Despite the existing triaging strategy at the Obstetric unit of a tertiary hospital in New Delhi, where all COVID-19 suspects obstetric patients were tested and admitted in orange zone and non-suspects in green zone, asymptomatic COVID-19 positive patients were found admitted in the green zone. This was the trigger to undertake a quality improvement (QI) initiative to prevent the admission of asymptomatic COVID-19 positive patients in green zones. The QI project aimed at reducing the admission of COVID-19 positive patients in the green zone of the unit from 20% to 10% in 4 weeks’ time starting 13/6/2020 by means of dynamic triaging. A COVID-19 action team was made and after an initial analysis of the problem multiple Plan-Do-Study-Act (PDSA) cycles were run to test the change ideas. The main change ideas were revised testing strategies and creating gray Zones for patients awaiting COVID-19 test results. The admission of unsuspected COVID-19 positive cases in the green zone of the unit reduced from 20% to 0% during the stipulated period. There was a significant reduction in the number of HCWs, posted in the green zone, being quarantined or test positive for COVID-19 infection as well. The authors conclude that Quality Improvement methods have the potential to develop effective strategies to prevent spread of the deadly Corona virus.
Introduction
Knowledge of the modes of transmission of the novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is limited and is still evolving. This, along with shortage of Personal Protective Equipment (PPE) and testing capacity, puts Health Care Workers (HCWs) at risk of getting infected by this virus (Jin et al., 2020; Lai et al., 2020).
The Obstetrics unit within our tertiary care hospital in New Delhi, India completes approximately 1,000 deliveries per month. With the advent of the Coronavirus pandemic in India, the Obstetric unit, was divided into red, orange, and green zones for COVID-19 confirmed, COVID-19 suspect, and COVID-19 non-suspect patients, respectively. Unfortunately, we found that a significant number of health care workers in the unit were being diagnosed with the COVID-19 infection consequent to the presence of unsuspected asymptomatic COVID-19 positive patients in the green zone. On collection of baseline data, COVID-19 positive cases were found to contribute to 20% of all green zone admissions. We found that 40 out of 502 HCWs (7.9%) had tested positive for COVID-19 infection over a period of 9 weeks out of which 24 (60%) were those who were posted in the green zones of the unit. This was a stimulus to initiate a quality improvement project to more carefully triage patients at admission and reduce the number of asymptomatic COVID-19 positive patients admitted in the green zone. The project goal was to reduce the occurrence of COVID-19 positive cases in the green zone of the obstetrics unit from 20% to 10% by 4 weeks’ time by means of dynamic triaging. The secondary objective was to reduce the COVID-19 infection rates in health care workers working in the unit.
Methods
A COVID-19 action Quality Improvement (QI) team was created with QI champions (people who inspire others to adopt QI practices) selected from the cohort of nursing officers, faculty members and residents. The problem was analyzed using Fish Bone analysis (Harel et al., 2016), which revealed that an inadequate triaging policy, based only on the history and symptoms at presentation, was the most important cause of inadvertent admission of positive patients to green zone. A dynamic improvement process was adopted where the team conducted and analyzed many change ideas via multiple Plan-Do-Study-Act (PDSA) cycles (Taylor et al., 2014) as shown in Table 1. A proforma was developed which included the daily statistics of patients detected positive from the green zone in the unit. The consultant on duty for 24 hours was assigned to get this proforma filled, check its accuracy and submit it to the QI team at the end of the shift. These data were analyzed weekly to calculate the number of patients admitted in the green zone who became positive for the COVID-19 infection. The impact of the intervention was evaluated by the following indicators: percentage of patients detected to have COVID-19 infection from the green zone among the total patients admitted in green zone (process indicator) and the percentage of HCWs posted in the green zone getting infected out of the total HCWs posted in green zone (outcome indicator). The team members met every week to follow progress made and identify issues that needed to be addressed to achieve the desired results. The progress of the project and the dynamic changes in triaging were shared with all the staff members through Whatsapp messages.
Implementation of the Change Ideas.

* The figures reflect the average of cases in 1 week.
Results
The percentage of patients who became positive for COVID-19 infection from the green zone gradually decreased from 20% in the 1st week to 0% at the end of the 4th week. A time series chart was plotted for the collected data (Figure 1). The most effective intervention was in PDSA cycle 4 which involved the creation of a designated segregation area (gray zone) in each ward. However, data collected at the end of 5th, 6th and 7th week again showed a positivity percentage of 9.7%, 8.5% &2.8% respectively from the green zone which, although within our target range, warranted further evaluation and monitoring to sustain the results and ensure that no COVID-19 positive cases were admitted in the green zones.
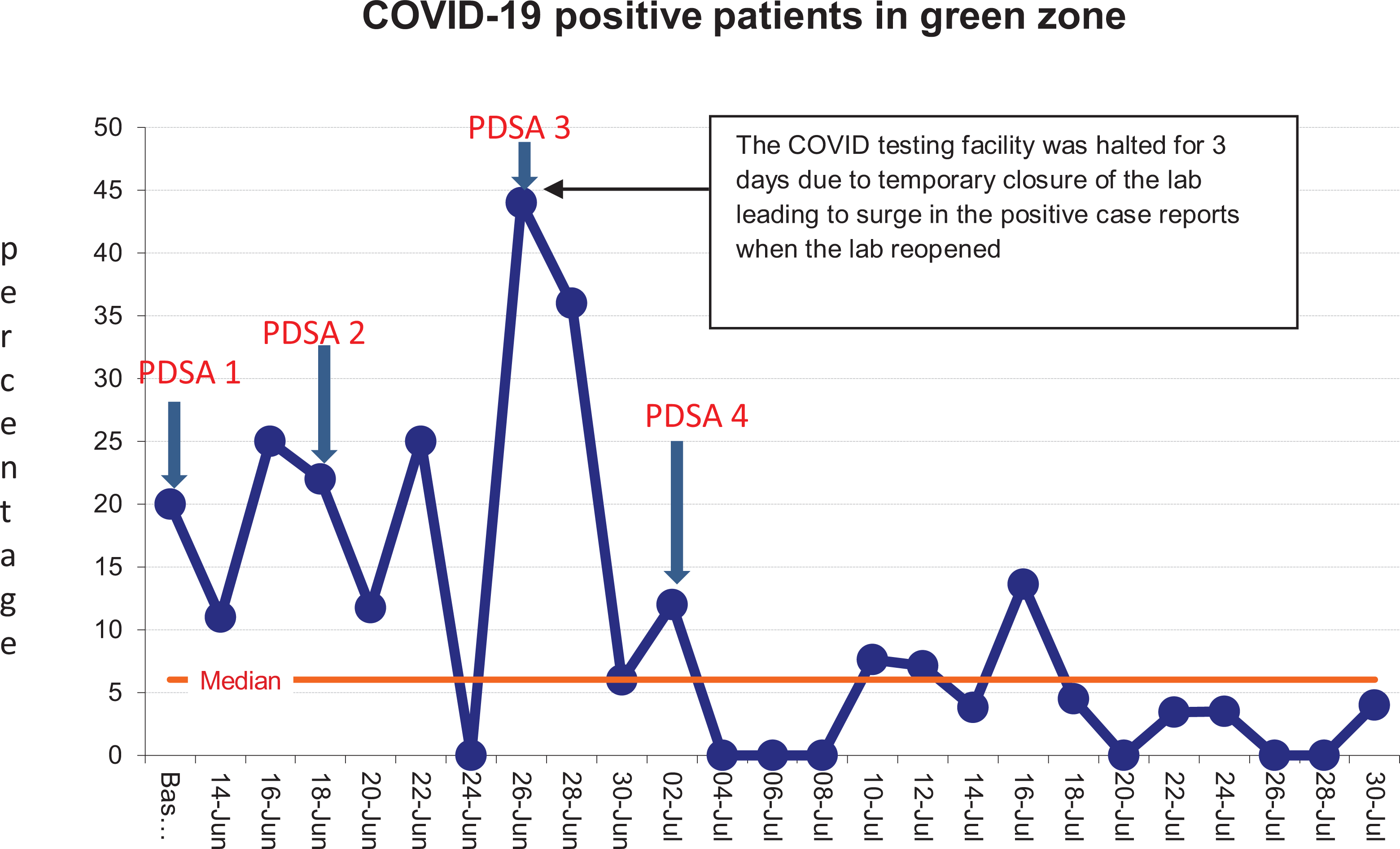
Time series chart of the percent of patients testing positive for COVID-19 infection out of total admissions in the green zone.
The percentage of HCWs in the unit who contracted COVID-19 infection among the total number of HCWs posted in the unit, after the project initiation, was found to be 23 out of 462 (4.9%) over a period of 9 weeks out of which 7 (30%) were from the green zone of the unit. Further, no HCW from the green zone of the Obstetric unit tested positive for COVID-19 infection for the last 1 month at the time of submission of this article.
Discussion
The key focus of all the interventions was to ensure effective and continued implementation by means of administrative support and active participation of all stakeholders, to devise a sustainable solution rather than a short-term quick-fix. The team members ensured participation of all stakeholders, namely concerned doctors, ward nurses and other HCWs, working in the green zone through communication via WhatsApp groups so that clear and uniform messages were conveyed to all. In addition, it helped the QI team devise new interventions based on suggestions received. By enhancing communication and facilitating teamwork, HCW’s were engaged and supported the sustainability of the new systems.
The project team was successful in achieving the desired target of reducing the occurrence of COVID-19 cases from the green zone with subsequent reduction in the percentage of HCWs getting infected while working in the green zone. However, the authors acknowledge that continued work is required to ensure that this improvement is sustained. To achieve this, the project team will continue to do weekly audits of the census so that any deviation can be analyzed and addressed proactively. The next challenge from this project will be extending this care pathway to achieve a “zero” infection rate for the HCWs working in the unit.
Footnotes
Acknowledgments
The authors wish to acknowledge Dr. Aparna Sharma, Additional Professor, Department of Obstetrics & Gynecology at All India Institute of Medical Sciences, New Delhi for her intellectual inputs to refine this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.