
Abstract
The current study assesses the relationship between continuing education (CE) with a focus on pediatrics and children with special heath care needs and how CE influences the knowledge and comfort levels of prehospital providers who treat these cases. Data are survey responses provided by paramedic and emergency medical technician (EMT) level providers (N = 575) in Los Angeles County. Regression models assessed the relationship between pediatric-focused continuing education and EMTs’ knowledge of and comfort with pediatric cases, adjusting for relevant covariates. EMTs’ participation in continuing education focusing on pediatrics and special health care needs was significantly associated with an increase in perceived comfort and knowledge. Among EMTs who did not receive continuing education focused on either pediatrics or special health care needs, the most frequently reported barrier to education was a perceived lack of availability. The impact of continuing education on perceived comfort and knowledge was more pronounced than the effect of prior experience, especially considering the limited prevalence of provider exposure to pediatric and childhood special health care needs cases compared to adult cases. Expanding educational opportunities is a promising approach to increasing the comfort and knowledge of EMTs who transport and care for pediatric cases.
Introduction
Pediatric patients constitute approximately 17%–27% of all United States (U.S.) emergency department visits (CDC, 2016; Shah et al., 2008) and 13% of all emergency medical service (EMS) transports (CDC, 2016; National Center for Health Statistics, 2017; Shah et al., 2008). Although the volume of pediatric emergency calls is lower than that of adults, pediatric patients transported by EMS often have an injury or illness with a higher level of acuity, and they need significant acute care (Shah et al., 2008). These cases may require specialized equipment, treatment, or even different modes of transport (Gausche-Hill et al., 2007; Lee et al., 2019; Rzońca et al., 2020). When an ambulance is called, a prehospital provider, either an emergency medical technician (EMT) or a paramedic, will be the first point of contact within the health care system (Sholokhova & Sviatoslav, 2019). For EMS workers to effectively respond and treat a diverse patient population (e.g., age, health status, and ability level), appropriate knowledge regarding health conditions and treatments at all stages of development is required (Lee et al., 2019). Although there has been a reduction in pediatric emergency department visits as a result of the COVID-19 pandemic, some hospitals are noting that the proportion of high-acuity, pediatric patients has increased in 2020 (Chaiyachati et al., 2020). Given the lack of overall experience with critically ill or injured children, comfort in working with and treating pediatric cases becomes challenging and requires ongoing education and training to ensure optimal pediatric prehospital care. Studies have shown that many prehospital providers are uncomfortable or unfamiliar with how to safely transport pediatric cases (Fidacaro et al., 2020), treat pediatric cases (Fowler et al., 2018; Hansen et al., 2016; Schroter et al., 2020), and pediatric patients are even at increased risk of lacking proper documentation during prehospital transports (Ramgopal et al., 2018). This is further complicated by interaction with parents, who may have conflicting priorities and could refuse transport against medical advice (Hartka & Vaca, 2020). Research has shown that a critical step to increasing knowledge and comfort in prehospital providers is continuing training that focuses on pediatric care (Stevens & Alexander, 2005).
It is estimated that 15% of children in the U.S. are children with special health care needs (CSHCN), defined as having chronic physical, developmental, behavioral, or emotional conditions that may require health-related services beyond those generally required by typical children (Boyle et al., 2011; Houtrow et al., 2014; Newschaffer et al., 2005; U.S. Department of Health and Human Services, 2013; Van Naarden Braun et al., 2015). Trends also suggest that there is an increase in the prevalence of pediatric disability, predominantly neurodevelopmental or mental health conditions (Houtrow et al., 2014; Van Naarden Braun et al., 2015; Zablotsky et al., 2019). Developmental disability and special health care needs in children have been linked to poorer overall health, comorbid conditions, mental illness, chronic health problems, and preventable premature death (Altman & Bernstein, 2008; Billstedt, 2000; Bradley & Lofchy, 2005; Einfeld et al., 2011; Gurney et al., 2006; Krahn et al., 2015; Pasic et al., 2005). Additionally, CSHCN are noted to have disproportionately high rates of EMS and interfacility transport usage, suggesting higher incidents of interaction with prehospital providers including EMTs and paramedics (Fratta & Fishe, 2019).
Elevated levels of required care, in conjunction with difficulties associated with CSHCN, create a unique challenge to treatment. In addition, the baseline levels of orientation and communication such as the Glasgow Coma Scale and many other metrics used in prehospital assessments may be different for CSHCN (Owley, 2004). Specialized knowledge and technical skills are necessary for effective management of these cases, yet because there are less frequent CSHCN cases in proportion to total call volume and insufficient EMS continuing education (CE) emphasizing pediatric or special needs skills (Davis & Mincin, 2005; Engelman et al., 2013; Glaeser et al., 2000; Seidel et al., 1984; Shah et al., 2008; Wolf-Fordham et al., 2014), practice, exposure, and experience can be limited (Meckler et al., 2014; Shah et al., 2008). Identification of disability can be crucial in determining whether a case is a medical or psychiatric crisis (American Academy of Pediatrics et al., 2006; Bradley & Lofchy, 2005). Children with developmental disabilities and special health care needs have a wide spectrum of ability and understanding and they may not be able to communicate their needs and concerns in a medical emergency (Bradley & Lofchy, 2005). Severe and pronounced disabilities may be easily identified; however, many pediatric special health care needs patients with mild or less obvious impairments can be difficult to recognize (Bradley & Lofchy, 2005). Given that EMS workers will be a child’s first health care contact in an emergency medical situation and the responder’s ability to assess and treat appropriately is paramount, it is critical to the care of both general pediatric cases and CSHCN cases that EMS receive sufficient training.
The level of knowledge and comfort in working with pediatric or CSHCN patients exhibited by prehospital care providers may have an influence on treatment decisions and could affect critical points of intervention. This can be demonstrated by evidence that shows EMS providers less frequently apply advanced life support skills to pediatric patients when compared to adults, with EMS workers more likely to use a “scoop and run” approach with children (Kumar et al., 1997). Some investigators hypothesize that this may be related to provider comfort levels regarding pediatric skills (Jo Su et al., 1997; Kumar et al., 1997; Smith et al., 1997; Spaite et al., 2001). Conditions may present differently in pediatric or CSHCN patients, when compared with adults and typical children, making it more difficult to accurately evaluate these cases. For example, research has shown that prehospital providers have had more difficulty in recognizing active pediatric seizures compared to adults experiencing seizures (Abramson et al., 2020). Pediatric patients have unique needs that can become exacerbated when the child’s ailment is serious or life-threatening and providing high-quality out-of-hospital care is critical to increasing the likelihood of favorable outcomes (Owusu-Ansah et al., 2020). The deterioration of infrequently performed skills related to pediatric cases and CSHCN may result in a decline in provider knowledge and comfort which can lead to increased anxiety with providing care (Gausche et al., 1990; Spaite et al., 2000, 2001). To address these issues, comfort and knowledge can be increased with continued training and exposure (Gausche et al., 1990; Smith et al., 1997; Spaite et al., 2001).
Continuing education has been shown to increase EMTs’ knowledge regarding pediatric and CSHCN patients as well as their comfort level in working with them (Spaite et al., 2000, 2001). This training does not need to be costly or provide a tremendous burden to the prehospital providers. Research has shown that online pediatric continuing education programs can effectively increase cognitive knowledge (Warren et al., 2008), and web-based training can be a cost-effective alternative for achieving instructional objectives (Jerin & Rea, 2005). More research has shown that expanding mobile technologies may provide unique learning opportunities in addition to both e-learning and instructor-led courses (Leszczyński et al., 2018; Sobolewska & Pinet Peralta, 2019). In addition to the low cost and efficacy, many EMTs prefer web-based modules (Jerin & Rea, 2005), and inclusion of quality didactic videos and interactive video instruction can be impactful in developing future continuing education opportunities in both pediatric and CSHCN subjects (Lindquist et al., 2020). Although training and continuing education requirements differ by state and local jurisdictions within the U.S., new technologies, procedures, and treatment processes for pediatric patients and CSHCN are continuing to change and regular updates to provider education are needed, The COVID-19 pandemic has highlighted the need for evolving educational opportunities across medical disciplines (Al-Jabir et al., 2020), as well as for specific procedures such as a pediatric resuscitation process that mitigates infection spread during a pandemic (Diaz & Dawson, 2020).
Research assessing the perceptions of emergency responders who assist on pediatric calls is limited, especially calls that involve CSHCN. Much of the existing research has focused on general pediatric cases (Glaeser et al., 2000) or specific providers such as emergency room physicians (Simon & Sullivan, 1996), nurses (Fredrickson et al., 1994), or paramedics (Spaite et al., 2000, 2001) but not EMTs. Broadly, EMTs and paramedics feel that their training has prepared them less for pediatric patient management compared to adults (Bentley et al., 2016). The studies that have assessed perceptions of prehospital providers have found that confidence and knowledge were related to providers’ abilities to assess and treat pediatric cases (Gulli et al., 2011) and CSHCN (Spaite et al., 2000, 2001). To our knowledge, there are few studies that broadly assess EMS providers’ (both emergency medical technicians and paramedics) perceived knowledge and comfort with general pediatric as well as CSHCN cases. This study assessed prehospital EMS workers’ (both EMTs and paramedic) levels of perceived knowledge and comfort in working with general pediatric and CSHCN cases. We hypothesized that 1) prior pediatric CE and prior CSHCN CE would be associated with an increase in perceived knowledge; and 2) prior pediatric CE and prior CSHCN CE would be associated with an increase in perceived comfort level in working with general pediatric and CSHCN cases.
Materials and Methods
Study Design and Population
These data are survey responses from a convenience sample of certified EMTs and paramedics in the Los Angeles County area collected in the Fall of 2018. The 24-item electronic survey was distributed via email to public and private emergency providers via Emergency Medical Services Agency listserv that included public and private providers operating in Los Angeles County. Public and private providers were asked to forward the survey to certified EMTs and paramedics who worked within their organization. After the initial email, two follow-up emails were sent, one per month for 2 months, requesting participation. The survey included items related to the respondents’ demographics, case history, continuing education, and comfort and knowledge related to pediatric and CSHCN cases. Inclusion criteria required either an EMT or paramedic certification and being at least 18 years of age. To incentivize participation, respondents were given the option to be included in a drawing for one of two $250 gift cards. Entry into the raffle was not contingent on providing complete responses. Respondent email addresses were reviewed for duplication and the survey links were restricted to one IP address to control duplicate responses. Considering the voluntary nature of the study and the desire not to pressure participants, a lower response rate was anticipated; however, this study presents an important preliminary assessment of EMS provider’s knowledge and comfort regarding CSHCN cases. All participants were informed of the minimal risks related to the study and only responses with a positive consent were included in the data. The study, including the research design, incentives, and questionnaire, was approved by the Institutional Review Board of the California State University, Northridge (IRB Number 1718-079). Funding for the two gift cards was provided by the Richie’s Fund (grant number SCG011312) in partnership with Children’s Hospital Los Angeles.
Measurements
In conjunction with items adapted from previous studies, several questions were developed using a process similar to the Delphi method by collaborating with in-field and out-of-field experts in EMT and paramedic education (Dalkey & Helmer, 1963). Demographic covariates included: age (measured in years), gender, and racial/ethnic makeup. Additional covariates included respondents’ average number of pediatric cases per month, monthly average of CSHCN cases, and number of years that the respondent worked or volunteered in EMS. One question, “since receiving my certification, I have taken a continuing education or refresher course that covered materials about…” was used to assess pediatric CE and CSHCN CE.
Key Outcome Measures
There were no indices adapted to both EMTs and paramedics designed to assess their comfort and knowledge in working with pediatric and CSHCN cases. To measure these components, items were drawn from EMT and paramedic textbooks (Gulli et al., 2011; Wertz & Wertz, 2002) in addition to modeling questions after prior studies that were conducted among medical and first responder populations, including nurses (Fredrickson et al., 1994), paramedics (Spaite et al., 2000, 2001), and law enforcement (Lew et al., 2014). Selected items were presented in a questionnaire to a panel of seven EMT and paramedic educators. They chose items most relevant to both EMTs and paramedics and provided suggestions for additional items where needed. The panel was then presented with a list based on the first round of recommendations. The panel met to discuss the items, and each were considered for inclusion or exclusion. The final measures were also reviewed by medical staff in direct clinical care and were piloted among a group of 10 active EMS personnel to assess consistency and content.
The final measures assessing how comfortable and knowledgeable EMTs and paramedics are with general pediatric cases were divided into two sections, one for comfort and one for knowledge, each comprised of 15 questions. Through each set of questions, respondents were asked to rate either comfort or knowledge on a 4-point scale. The two sets of questions all assessed the same 15 skills for pediatric care: 1) managing a pediatric airway; 2) recognizing respiratory illness and the appropriate treatment in pediatric cases; 3) identifying and treating the early signs of respiratory failure in a pediatric patient; 4) managing pediatric trauma; 5) recognizing cardiac arrest and arrhythmia in pediatric patients; 6) recognizing and treating pediatric shock; 7) performing cardiopulmonary resuscitation (CPR) on a newborn; 8) determining an APGAR (appearance, pulse, grimace, activity, and respirations) score for a newborn; 9) determining the Glasgow Coma Scale score for a child; 10) recognizing and managing pediatric seizures; 11) recognizing signs of child abuse/non-accidental trauma and neglect; 12) distinguishing normal from abnormal vital signs for a child; 13) performing a pediatric pain assessment; 14) giving bad news to parents of pediatric patients; and 15) dealing with a sudden infant death syndrome case. To assess comfort, the question the stem stated, “Please rate your comfort with pediatric patients in the following areas” and the response options included “very uncomfortable,” “somewhat uncomfortable,” “somewhat comfortable,” and “very comfortable.” To assess knowledge, the question stem stated, “Please rate your knowledge with pediatric patients in the following areas” and the response options included “very unknowledgeable,” “somewhat unknowledgeable,” “somewhat knowledgeable,” and “very knowledgeable.” The final measures of pediatric comfort and knowledge were computed by summing responses on all 15 skill areas for each section.
The final measures of CSHCN comfort and knowledge also consisted of two separate sections, each with 11 questions. Through each set of questions, respondents were asked to rate either comfort or knowledge on a 4-point scale. The two sets of questions all used the same 11 skills for CSHCN care: 1) recognizing signs of child abuse and neglect on a pediatric special needs case; 2) determining the Glasgow Coma Scale score for a pediatric special needs case; 3) performing CPR on a child with a tracheostomy; 4) providing ventilation with a bag-valve-mask on a pediatric tracheostomy patient; 5) suctioning a child’s tracheostomy tube to clear an obstruction; 6) recognizing and managing seizures on a pediatric special health care needs case; 7) recognizing signs of an allergic reaction; 8) communicating with a developmentally disabled pediatric patient; 9) recognizing the differences between a behavioral emergency and a developmental disability; 10) performing a pain assessment on a pediatric special health care needs case; and 11) determining the most appropriate receiving facility for a pediatric special needs case. To assess comfort, the questions the stem stated, “Please rate your
All four measures (general pediatric comfort, general pediatric knowledge, CSHCN comfort, and CSHCN knowledge) were assessed for face validity by an expert panel and reported high internal consistency with Cronbach’s αs: pediatric comfort 0.940, pediatric knowledge 0.953, CSHCN comfort 0.935, CSHCN knowledge 0.941.
Analytical Methods
To test hypothesized relationships, four separate linear regression models assessed the association between experience, pediatric continuing education, and the respondent’s knowledge or comfort for general pediatric cases, controlling for covariates including respondent age, sex, ethnicity, status as a parent, time working/volunteering in EMS, and whether they were an EMT or paramedic. Two additional models were built to assess the relationship between experience, CSHCN continuing education, and the respondent’s knowledge of or comfort with CSHCN cases, while controlling for covariates including respondent age, sex, ethnicity, status as a parent, time working/volunteering in EMS, and whether they were an EMT or paramedic. Model diagnostics indicate appropriate fit and adherence to assumptions. Initial CSHCN models also controlled for general pediatric knowledge or comfort; however, due to a strong significant correlation with other variables in the models, the cross over comfort and knowledge were removed from the final models. There was no change in directionality and no major changes in significance when these variables were removed. Finally, among those who did not participate in general pediatric CE or CSHCN CE, statements about barriers to receipt of CE were ranked according to percentage of agreement. Analyses were completed at a statistical significance level of 0.05 using SPSS version 24 (IBM Corp, 2016).
Results
Demographics
Of the 754 responses to the survey, 29 respondents declined to participate and 113 were excluded because of incomplete data, resulting in an analytic sample with data from 612 respondents. The majority of respondents were male (87%) and the most frequently reported racial ethnic background was non-Hispanic White (60%), followed by Hispanic/Latino/Latina (24%), Asian/Pacific Islander (11%), and Multi-ethnic/Other (5%). There was an approximately equal number of EMTs (51%) and paramedics (49%). Over half of respondents reported having a position within the fire department (62%) followed by non-fire positions (38%), 911 responding ambulance services (n = 124), non-911 responding ambulance services/interfacility transfer services (n = 96), and other (n = 12) which included hospital service, event first aid, and EMS education. Nearly 53% of respondents reported being a parent and 2% reported being a parent of a CSHCN. More than three quarters of respondents (84%) reported taking CE related to pediatric cases and only (40%) reported CE related to CSHCN cases. The average age of the sample was 36 years and the average amount of time respondents worked in EMS was 11.3 (SD = 9.8) years. When asked about cases, a majority (80%) of both EMTs and paramedics reported having at least one pediatric case per month, with a self-reported median caseload of three pediatric cases per month. Slightly over one quarter (27.6%) of respondents reported having at least one CSHCN case per month with a self-reported median caseload of one CSHCN case per month. Demographic characteristics of the sample are similar to that of national EMS provider demographics that show a majority male, non-Hispanic white, and an average age between 34 and 39 years (Bentley et al., 2016).
Differences Across EMTs and Paramedics
When assessing differences between responses of EMTs compared to paramedics, paramedics tended to be older (p < 0.001, 95%CI = −9.5, −6.2), have longer care provider histories (p < 0.001, 95%CI = −7.0, −3.9), higher levels of pediatric comfort (p = 0.001, 95%CI = −4.4, −1.1) and knowledge (p < 0.001, 95%CI = −4.6, −1.5) and CSHCN comfort (p = 0.047, 95%CI = −2.4, −0.1) and knowledge (p = 0.005, 95%CI = −2.9, −0.5). When comparing the responses between EMTs and paramedics, there were no significant differences in the mean number of pediatric cases or CSHCN cases either certification level treated per month. However, paramedics had more pediatric CE (p < 0.001, 95%CI = −0.3, −0.2) than EMTs.
Provider Comfort and Knowledge
Regression analysis indicated that participating in pediatric CE was associated with an increase in perceived comfort related to pediatric cases (β = 4.5, 95%CI = 2.0, 7.0, p < 0.001), controlling for all other covariates (e.g., parenthood/guardianship, age, gender, race/ethnicity, estimated number of pediatric cases seen per month, and years with certification) (Table 1). Similarly, taking pediatric CE (β = 4.2, 95%CI = 1., 6.5, p < 0.001) was associated with an increase in perceived knowledge related to pediatric cases (Table 1). For CSHCN cases, taking CSHCN CE was associated with an increase in perceived comfort related to CSHCN cases (β = 3.0, 95%CI = 1.8, 4.3, p < 0.001), controlling for all other covariates (e.g., parenthood/guardianship, age, gender, race/ethnicity, estimated number of CSHCN cases seen per month, and years with certification) (Table 1). Similarly, taking CSHCN CE was associated with an increase in perceived knowledge related to CSHCN cases (β = 3.4, 95%CI = 2.1, 4.7, p < 0.001), controlling for all other covariates (Table 1).
Multivariable Regression Analysis of Factors Associated With Increases in Comfort and Knowledge.

Potential Barriers to the Receipt of Continuing Education
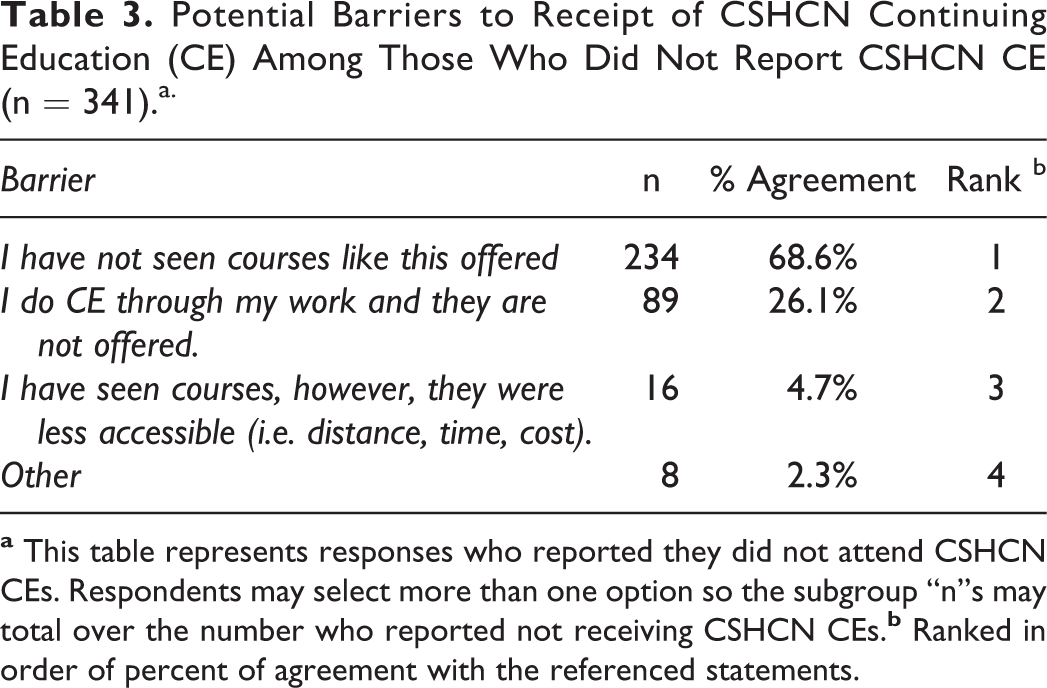
Among those who did not receive either pediatric CE (n = 90) or CSHCN CE (n = 341), statements regarding barriers to the receipt of CE were ranked by percent of agreement. The most frequently reported barrier related to both pediatric CE (Table 2) and CSHCN CE (Table 3) was not seeing courses like this offered (63% and 69% respectively), followed by employers not offering these CE (21% and 26% respectively), issues related to distance, time, or cost (17% and 5% respectively), and other specified issues (8% and 2% respectively). Percent of agreement did not significantly differ across gender, ethnicity, age, or year of undergraduate study.
Potential Barriers to Receipt of Pediatric Continuing Education (CE) Among Those Who Did Not Report Pediatric CE (n = 90).a

Potential Barriers to Receipt of CSHCN Continuing Education (CE) Among Those Who Did Not Report CSHCN CE (n = 341).a.
Discussion
It is important to evaluate an emergency responder’s level of comfort and knowledge in pediatric cases given that provider comfort and knowledge may influence treatment initiation and quality of care (Jo Su et al., 1997; Kumar et al., 1997; Smith et al., 1997; Spaite et al., 2001). The current study adds to the literature by assessing how comfort and knowledge, regarding both pediatric and CSHCN cases, are related to the receipt of CE. The study expands upon prior research by assessing these relationships among two types of EMS workers, paramedics and EMTs. Considering that a large majority of this sample is regularly treating and transporting pediatric cases each month and nearly half are involved in calls related to CSHCN, understanding providers’ perceptions may offer insight into the care of these critical cases. Although these data were based on self-reported information, the results were consistent with studies suggesting that EMS providers may have less frequent contact with pediatric cases compared to adult cases, thereby, having less opportunity to practice and refine pediatric skills (Gausche et al., 1990; Glaeser et al., 2000). Regardless of a lower frequency, a large majority of the sample reported encountering pediatric cases as well as CSHCN cases each month, highlighting that pediatric and CSHCN education and skill practice remain a priority. The prevalence of exposure to both pediatric and CSHCN cases among paramedics and EMTs suggests that education can increase perceived comfort among EMS providers.
Although paramedics reported greater comfort and knowledge regarding pediatric and CSHCN issues than EMT respondents, there was no significant difference in the average self-reported number of pediatric and CSHCN cases seen by paramedics or EMTs per month. This difference is most likely due to EMTs receiving less training, having less cumulative experiences, and fewer additional certifications than what is required of paramedics. Considering that both EMTs and paramedics report a similar number of average pediatric calls, additional training, and continuing education in relevant pediatric and CSHCN topics may help to close the gaps in knowledge and comfort between EMTs and paramedics. With much of the current pediatric CE research focus on EMS providers with paramedic certification, these data suggest that all levels of EMS providers may need to receive additional educational programs, particularly since EMTs on average have lower levels of self-reported knowledge and comfort regarding these cases.
Our finding that EMS providers with pediatric or CSHCN CE are more confident and knowledgeable in caring for pediatric specific cases, suggests that pediatric education, including CE courses focusing on CSHCN, should be made available since an increase in comfort and knowledge in caring for children is associated with attendance in both pediatric and CSHCN courses. This increase in comfort extends beyond both experience and certification level and is consistent with other studies, suggesting that experience is not always related to increase in comfort with treating CSHCN (Simon & Sullivan, 1996). CSHCN CE may be the primary mechanism to ensure that providers have high levels of comfort and knowledge. These effects were significant even when controlling for other predictors such as being a parent and length of time working in EMS.
Compared to other studies, this study found a higher proportion of respondents taking pediatric CE; however, there were fewer who reported taking CE related to caring for CSHCN (Glaeser et al., 2000). Also, similar to findings from other investigators, a majority of respondents who did not take the CE appeared to value and desire CE related to both pediatric and CSHCN cases (Glaeser et al., 2000). In the context of barriers to either pediatric or CSHCN CE, the most frequently reported was a lack of knowledge about the existence of CE opportunities followed by concern about cost, time, and distance. Although anecdotal, it is likely that if offered, many of these providers would consider enrolling in pediatric and CSHCN CE. Although further research is needed, this suggests that informing providers of opportunities for pediatric or CSHCN CE, particularly ones that are inexpensive or allow for distance education, would encourage uptake.
Considering that many of these results align with previous work, one of the benefits of the present study is the creation of an assessment tool that gauges EMS perceived comfort and knowledge. Future studies could continue to study the impact of specific curriculum and trainings with pre- and post-curricular surveys.
Limitations
Results reported in this study are from a small survey of EMS providers that have several limitations inherent to survey methodology. First, although this is a small convenience sample, our work points toward the importance of improving knowledge and comfort through pediatric and CSHCH continuing education opportunities for EMTs and paramedics. Though nonprobability sampling was used, the respondents represent a diverse set of EMS personnel and demographics are similar to nationally representative samples (Bentley et al., 2016). Second, the small sample size and convenience sampling methodology limit the generalizability of the inferences made. Third, this cross-sectional study design cannot establish a temporal relationship and does not support causal inference. Future longitudinal studies assessing the direct implications of specific CE are needed to empirically tie CE directly to increase in EMS provider comfort and knowledge in caring for children. Third, although the pediatric and CSHCN measures were assessed for internal validity and reliability, additional studies are needed to assess these measures in different populations. Fourth, though the sample size was sufficient to power the models, future study should assess potential regional or national differences in results and whether there are specific patterns in respondents who do not take these CE, in order to improve understanding of how to provide targeted CE opportunity. Fifth, to ensure that only certified EMTs and paramedics were responding, the survey was sent out through a designated provider listserv and a screener question was asked about certification, however, no certification documentation was collected to prove current status. Sixth, perceptions of comfort and knowledge may be related to one another; however, to provide a parsimonious model and to limit modeling highly correlated variables, they were not modeled together. Eighth, in the survey the age grouping for pediatrics (defined as 0–14 in Los Angeles County EMS policy) was left for the EMTs and paramedics to interpret; however, all these prehospital providers would have received initial training defining pediatrics (Department of Health Services County of Los Angeles, 2020). Finally, the study was based on self-reported data and perceptions of comfort and knowledge. No knowledge tests or psychomotor tests were performed to assess either comfort or knowledge and as such, this study was based on perceived knowledge and comfort. Although this may be a potential limitation, prior studies have identified this as a useful and important way to assess providers (Lew et al., 2014; Seidel et al., 1984; Simon & Sullivan, 1996; Wolf-Fordham et al., 2014). Future studies should provide specific knowledge tests and even include CE interventions to both EMTs and paramedics to assess knowledge and comfort change and to determine if the effects last over time.
Conclusions
Access to educational opportunities may increase the comfort and knowledge of both paramedics and EMTs who treat pediatric and CSHCN cases. The impact of education was more pronounced than the effect of experience, an especially important finding considering the limited exposure of providers to pediatric and CSHCN cases compared to adult cases. Expanding educational opportunities may increase comfort and knowledge with treating pediatric and CSHCN cases, particularly for EMTs who have been shown to have lower levels of comfort in caring for children. Given that many providers seem to value CE despite not having taken them, increasing awareness of educational opportunities related to pediatric and CSHCN cases and prioritizing low-cost opportunities, as well as distance options may be promising approaches to enhancing provider comfort and knowledge.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the two gift cards was provided by the Richie’s Fund (grant number SCG011312) in partnership with Children’s Hospital Los Angeles.