
Abstract
Dentists are healthcare professionals who are at high risk of infection and transmission of the coronavirus disease-19 (COVID-19). The primary objective of the present study was to evaluate the changes in clinical practice made by Brazilian dentists during the COVID-19 pandemic. From June 22 to July 13, 2020, an online questionnaire was sent to dentists using Google Forms. After providing consent, 1,178 dentists answered questions regarding their knowledge and clinical experiences related to COVID-19. Data were analyzed using Chi-square, Fisher’s exact, or Kruskal–Wallis tests, with a significance level of 5%. Brazilian dentists significantly changed their routine dental practices. Biosafety measures were added in their offices by 98% of the dentists, increasing operating costs for 88.3% of dentists. Greater discomfort due to the increase in personal protection equipment (PPE) worn during the pandemic was reported by 58.6%. Furthermore, 84.2% reduced heir hours of service. It was found that the dentists decreased their workload, used additional PPE, and took additional biosafety measures.
Introduction
Dentists, among other healthcare professionals, are at the highest risk for coronavirus disease-19 (COVID-19) transmission and contraction. This is because many routine dental procedures create aerosol particles, which have the potential to transmit the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19. Although it is important to offer treatment to patients who have dental situations that require immediate attention, it is important to prioritize the prevention of transmission to both patients and dental care personnel (Khader et al., 2020).
Considering the current rapid spread of COVID-19, the American Dental Association stated that in addition to following standard universal precautions, dentists should also ask patients about recent travel and assess for signs and symptoms of respiratory tract infections. Furthermore, patients’ body temperature should also be recorded, and the use of mouthwash with 1% hydrogen peroxide before starting any procedure should be recommended. Also, rubber dam isolation and high power suction should be used during procedures. Thorough cleaning and disinfection of public contact areas, including door handles, chairs, and bathrooms, should also be carried out (Ahmed et al., 2020; Khader et al., 2020; Vieira-Meyer et al., 2020).
While healthcare practitioners currently use personal protective equipment (PPE), including gloves, masks, and lab coats, when working with all patients, those working around potential aerial infections, such as SARS-CoV-2, require additional PPE, including goggles or face shields, N95 masks, and disposable outerwear, such as lab coats or coveralls and rubber boots (Odeh et al., 2020).
Due to the COVID-19 pandemic, dentists’ concerns regarding elective and urgent/emergent dental care have been reported (Faccini et al., 2020). It is important to better understand how dental professionals have altered their clinical practices during the ongoing COVID-19 pandemic, especially in countries with vast territorial extensions, such as Brazil (which now has the third-highest number of cases worldwide). In addition to the nonhomogeneous diffusion of the pandemic in each region, a wide representative sample from different locations is required to present the results substantially.
In light of the ongoing global COVID-19 pandemic and the lack of scientific reports regarding the changes in PPE usage by dentists and their routine dental practices during the pandemic, the present study aimed to evaluate how dentists had modified their clinical practices during this ongoing viral outbreak. Additional objectives included assessing workload changes, the use of PPE (the comfort and adverse reactions), and changes in relation to costs.
Materials and Methods
The present study was approved by the Research Ethics Committee of the University of North Parana (UNOPAR), with approval number 4.147.506. According to a previous study by Faccini et al. (2020), there are 338,000 dentists in Brazil; therefore, the sample should have been made up of at least 384 individuals, which would provide a confidence interval (CI) of 95% and a margin of error of 5% (Faccini et al., 2020). The inclusion criteria were as follows: dental school graduates, with or without a postgraduate degree, who were working in dental clinics. Participants who did not meet the inclusion criteria were excluded.
An online questionnaire was developed using Google Forms. Potential participants were contacted by e-mail by dissemination through postgraduate programs and professional councils as well as an active search of e-mails of dental offices. After providing consent, participants answered questions about their knowledge and clinical experiences regarding COVID-19. The questionnaire was administered from June to July 13, 2020.
In the Statistical Package for the Social Sciences (SPSS Statistics 22, IBM Corporation, 2013. JAVA), we performed descriptive statistics. Chi-square test was used to compare the working time before and during the pandemic. In addition, we performed Fisher’s exact test to compare the use of personal protection equipment and Kruskal–Wallis tests to compare biosafety between Brazil regions. A significance level of 5% and a CI of 95% was considered.
Results
A total of 1,357 questionnaires were returned. However, 168 were duplicates and 11 were respondents from other countries. A total of 1178 valid responses were obtained from all 26 Brazilian states. The overall response rate could not be calculated because the questionnaire was sent to various organizations in Brazil, which in turn forwarded it to their constituents. We received 339 responses during the first 24 hours. Respondents were mostly females (75.3%), who had been in practice for < 10 years (42.8%), and who had completed a continuous professional development course > 5 years (43.4%). The region with the highest number of participants was southern Brazil (39.6%). The mean age of the respondents was 37.97 ± 10.46 years, and 25.2% of respondents had at least one chronic disease (Table 1).
Sample Characterization, Work Practice Characteristics and Use of Personal Protection Equipment.

Note. SD: Standard Deviation; CI: Confidence interval.
The pandemic has required dentists to make some changes to their work routines, such as conducting COVID-19 testing (27.2%), reducing office hours (48.1%), or even temporarily suspending clinical services (7.7%), as seen in Tables 1 and 2. Only 10.8% of the respondents acknowledged having any flu symptoms, although 17% of the dentists declared that they had seen at least one patient with confirmed COVID-19. Screen and triage everyone entering the dental office for signs and symptoms of COVID-19 was conducted by 80.3% of dentists who kept working, as a new procedure.
Association of Working Time Before and During COVID-19 Pandemic.

Chi-Square test: (p < 0.001).
The dentists indicated that they had made changes in biosafety at the reception desk (97.8%) and had added biosafety measures in the office (98.0%). Improving biosafety because of the pandemic increased operating expenses for 88.3% of the dentists, but only 17.8% stated that they had transferred those increased costs to patients (Table 1).
Table 1 shows the changes in the weekly working hours. The majority (84.2%) changed their service hours during the pandemic. Of the dentists who stopped clinical practice during the pandemic, 24.1% had a lower workload (<10 hours/week). Out of the dentists with higher weekly workloads, 21–40 hours or > 40 hours, 50.6% and 65% reduced their working time, respectively. Only a few respondents (9.3%) who worked < 10 hours per week before the pandemic had to increase their workload. Of the dentists who worked 11–20 hours and 21–40 hours per week, their workloads increased by 1.5% and 0.9%, respectively (Table 2). A significant reduction in practice was reported by a majority of the dentists during the pandemic.
Various types of PPEs were added based on the airborne transmission of SARS-CoV-2 (Figure 1), with significant differences between their use before and their use during the pandemic. These additions included N95 masks, or those with similar particulate filtering (p < 0.001), disposable caps (p < 0.001), closed-toe shoes (p < 0.001), disposable lab coats/aprons (p < 0.001), protective goggles (p < 0.001), face shields (p < 0.001), and disposable shoe covers (p < 0.001). On the other hand, there was a significant reduction in the use of disposable gloves (p < 0.001), surgical masks (p < 0.001), fabric caps (p < 0.001), and fabric coats/aprons (p < 0.001). A large percentage of dentists reported greater discomfort due to the addition of PPE during the pandemic (58.6%), and 11.2% had allergic reactions due to the use of PPE (Table 1).
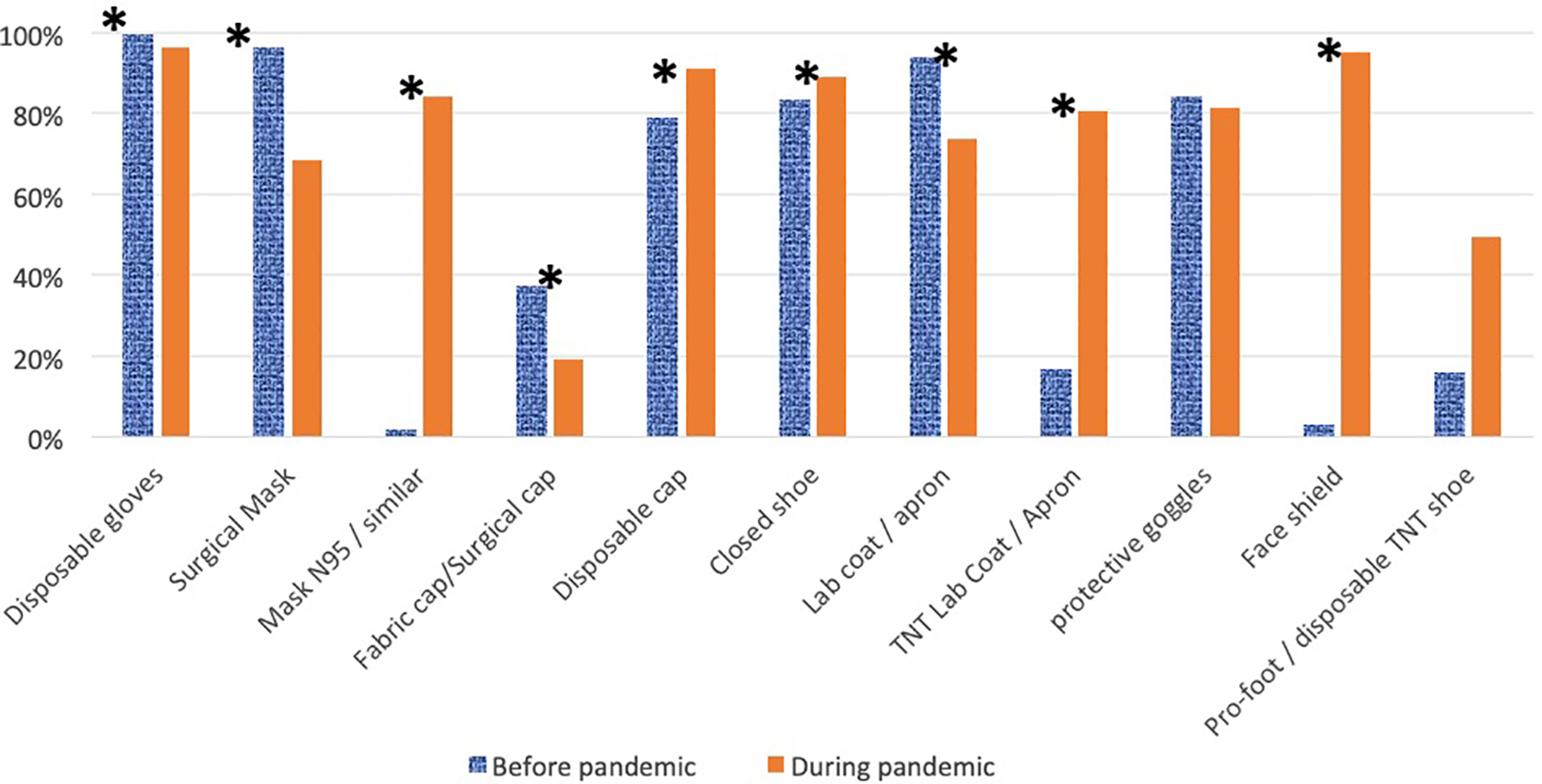
Use of personal protection equipment before and during COVID-19 pandemic.
Neither the educational level of the participants nor their years of experience affected the biosafety changes made in their dental offices. Even dentists who did not have chronic diseases were concerned with improving biosafety measures. Of the dentists who underwent COVID-19 testing, 52.10% worked with two or more patients with confirmed COVID-19 (p < 0.001).
When comparing regions, significant differences in changes to biosafety were not found between the regions (p = 0.385), as seen in Table 1. Additionally, all regions in Brazil had marked changes in relation to the workload (84.20%), with no statistically significant difference between the regions (Kruskal–Wallis = 0.416).
Discussion
The present study sought to collect information regarding changes in clinical practice by Brazilian dentists in response to the COVID-19 pandemic. The use of social media as a facilitator in the process of accessing and disseminating the questionnaire was fundamental to reaching and including dental professionals from all over Brazil. The majority of the responses were from dentists in southern Brazil, likely because that was where the research was generated, although dentists from all regions participated. Although some authors (Gelinas et al., 2017; Topolovec-Vranic & Natarajan, 2016; Weller, 2015) have indicated that social media has a greater range of recruitment in the younger population, in the present study, we were able to obtain responses from professionals between 21 and 74 years of age (Table 1), generating a broad representative sample of the Brazilian dentist population.
The results of the present study found that neither the educational level nor the years of experience of the respondents affected the biosafety changes made in the dental office. This outcome differs from the results found by Kamate et al. (2020), in which questionnaires were administered to a worldwide sample of dentists and indicated that dentists with higher qualifications (postgraduates) had significantly higher knowledge scores than did the dental school graduates. (Kamate et al., 2020) Regardless of their chronic disease status, dentists were concerned about biosafety care and considered infection control measures to be essential for practice.
The COVID-19 pandemic has brought countless changes not only in the personal lives of individuals but also in the clinical routines of health professionals. Despite the fact that dentists are among the professionals with the highest risk of contamination and spread of the virus, Epstein et al. (2020) stated that no clusters of respiratory-transmitted diseases, including SARS-CoV-2, have been reported in dental providers or patients in a dental setting. Nonetheless, most dentists found it prudent to make changes to protect themselves, their team members, and their patients. The main changes reported in our study were workload changes, additional PPE, and additional biosafety measures which are similar to what was found by Faccini et al. (2020) wherein, 95.5% of the professionals reinforced biosafety improvements, such as the use of face shields and disposable PPE. A decrease in demand and use of emergency dental services was noted by Guo et al. (2020). This may also highlight the changing demands for dental services, as many patients have avoided leaving home because of the pandemic, and sought care only in urgent or emergent cases.
The additional expenses from the addition of PPE and biosafety measures can negatively impact the fiscal performance of dental offices (Table 1). In a study by Schwendicke et al. (2020) in Germany, the financial impact on dental clinics that have adopted additional preventive measures in response to COVID-19 was considerable. They noted that government financial aid may be required in the longer term, and practice owners may need to consider practice re-organization to reduce costs and maintain minimum profitability (Schwendicke et al., 2020)
A large number of dentists reported greater discomfort and some allergies due to the additional PPE (Table 1), consistent with the findings by Yuan et al. (2020), who found that a total of 94.57% of professionals surveyed reported discomfort regarding PPE use. The main complaints of adverse reactions and discomfort were adverse skin reactions, respiratory difficulties, heat stress, dizziness, and nausea (Yuan et al., 2020).
Although Brazil is a country with a vast territorial size with many regional and cultural differences, these differences were not very evident with regard to changes in dental office biosafety among professionals of different regions. Most dentists reported changes in biosafety measures, showing that the vast majority of these professionals were aware that the adoption of these infection prevention practices is essential to halt the spread of COVID-19.
One of the limitations of the present study was that no distinction was made between professionals from public and private clinics. There are likely differences inherent in the practices of each sector, including operating costs and access to PPE (Vieira-Meyer et al., 2020). Another limitation concerns gender, in response to which future studies should include proportional responses from women and men. The primary concerns of dentists all over the world during the ongoing COVID-19 pandemic are more than clinical practice modifications. These professionals, especially those who work in private clinics, are faced with the critical choice of stopping work to ensure their health or to continue working for the upkeep of their home and family. Therefore, it is up to each professional, based on their circumstances, to assess the risks and benefits when making their decisions.
Conclusion
Based on the results of the present study, we have concluded that most Brazilian dentists have altered their routine dental practices in response to the COVID-19 pandemic. The biggest changes reported were a decrease in the workload, the use of additional PPE, and the addition of biosafety measures.
Footnotes
Author Contributions
Mayara Delfino Sentone Rossato and Danielle Gregorio: Acquisition, analysis and interpretation of data, drafting, revision and final approval of the manuscript. Renata Rodrigues de Almeida-Pedrin and Thais Maria Freire Fernandes: Conception and design of the study, analysis and interpretation of data, revision and final approval of the manuscript. Luciana Prado Maia, Regina Celia Poli, and Sandrine Bittencourt Berger: Analysis and interpretation of data, revision and final approval of the manuscript.
Acknowledgements
The research team acknowledges Dr. Luiz Evaristo Ricci Volpato for his help in spreading the research to dentists.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.