
Abstract
This systematic review aimed to identify and compare instruments measuring nurses’ organizational well-being, summarise the dimensions measured by these instruments, the statistical analysis performed for validity evidence and identify an instrument that comprehensively investigates nurses’ organizational well-being. The JBI Manual for Evidence Synthesis and the PRISMA checklist were used as guidelines. The search was conducted on Medline, CINAHL, Cochrane Library and Scopus. Critical appraisal and data extraction were drawn on the COSMIN checklist. Dimensions were conceptually synthesized by the measurement concepts' similarity. Twenty-two articles were retrieved and they included 21 instruments that measured nurses’ organizational well-being. The instruments vary by dimension number (range 2–19), items (range 12–118) and concept elicitation. A plurality of methodologies has been used in instrument development and assessments of evidence for validity. Only four instruments reported a concurrent criterion validity or a measurement comparison with an already tested-for-validity instrument. Similar dimensions were leadership and support, relationships and communication, work-family balance, work demands, violence, control and autonomy, satisfaction and motivation, work environment and resources, careers, and organizational policy. This review underlines the core areas of the instruments that measure nursing organizational well-being. It allows administrators and researchers to choose the appropriate instruments for monitoring this multidimensional concept.
Introduction
The concept of organizational well-being refers to the set of cultural bases, organizational processes and practices that coexist in a working context and influence the quality of life and physical, psychological and social well-being of workers (Avallone & Bonaretti, 2003). Ensuring the organizational well-being of healthcare professionals has become one of the main objectives of healthcare organizations over recent years (DellaBella et al., 2022). Attention to this topic has grown in particular during the COVID-19 pandemic, which has noticeably affected aspects of the working context of healthcare professionals such as workloads, patient demands and work-family balance, impacting consequently their physical, social and emotional well-being (Piredda et al., 2022; Zaghini et al., 2021).
Research conducted in different healthcare contexts has noted that organizational well-being influences the performance of professionals, and consequently, the quality of care given and the safety of patients (Fiorini et al., 2022; Wong & Spence Laschinger, 2015; Zaghini et al., 2020). In a positive work environment, nurses appear to be more dedicated to their work (Zaghini et al., 2015), staff turnover is reduced (Bae et al., 2010; Mohamadzadeh Nojehdehi et al., 2015) and the intention of nurses to leave the profession (Perry et al., 2017), in both public and private health facilities (García et al., 2014). Creating and promoting a positive working climate, in which nurses report good organizational well-being, may be key to ensuring the success of a healthcare organization, in improving the quality of care (Bahrami et al., 2016; Kassem & Gaber, 2015), and therefore clinical outcomes (Al-ghraiybah et al., 2021). Considering this, it becomes essential to measure and study nurses’ organizational well-being with instruments that demonstrate validity and reliability to implement interventions that will maintain and improve nurses’ well-being and indirectly improve patient outcomes.
Numerous studies in the literature have been designed to measure organizational well-being (Avallone & Paplomatas, 2005), including studies specific to the nursing profession (Sili et al., 2010). However, the multiplicity of these instruments makes it difficult to compare outcomes in the scientific community, leading to some uncertainty and incoherency. For example, authors have drawn on the generical organizational well-being conceptual models and have included variables related to the physical context of the organization, such as workloads and resources, applying models such as the job demands-resource (JD-R) model (Bakker & Demerouti, 2007). Others have considered occupational psychology models and focused on the relational and emotional aspects of work and the workplace (Elfering et al., 2017). Similarly, other instruments have focused on how work activities influence the time available for one’s family (Ogata et al., 2021). The Nursing Context Index (NCI) encourage consideration of work and social life balance in instrument development as it is associated with work-related stress and ultimately with nurses’ organizational well-being (Slater et al., 2009) These different methods used to measure nurses’ organizational well-being and the different methodological approaches used in their validation make it difficult for the scientific community to compare the results obtained from the research, and therefore to have comparable measurements of the degree of organizational well-being in the nursing sector.
Although a literature review has summarised the conceptual models developed for nurses’ organizational well-being, and suggested the creation of an all-encompassing model (DellaBella et al., 2022), to date there is still no complete, valid and reliable instrument in the literature for measuring nurses’ organizational well-being in all its aspects. Considering this, this systematic review aimed to identify and compare the instruments for measuring nurses’ organizational well-being, and, as secondary objectives, to summarise the dimensions measured by these instruments and if possible, identify an instrument that comprehensively investigates nurses’ organizational well-being. The research questions of this systematic literature review were: 1. What instruments are there that measure nurses’ organizational well-being? 2. What dimensions are investigated by existing instruments? 3. Which of the identified instruments comprehensively investigates nurses’ organizational well-being? 4. Which statistical analysis are used in the examination for evidence of the validity of instruments?
Materials and Methods
A systematic review was conducted between April and September 2022, following the guidelines of the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis (Aromataris & Munn, 2020). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., 2009) have been used for reporting this review. The protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under record number CRD42022379289 (Gioiello et al., 2022).
The evidence-based framework of population, investigated condition, comparison condition and outcome (PICO) was used as follows: P) nurses; I) instruments, questionnaires, surveys, validation; C)/; O) nurses’ organizational well-being, organizational health, organizational climate, organizational wellness, job satisfaction, work environment.
The main keywords were identified as validation, instrument, survey, questionnaire, instrument, organizational health, organizational climate, organizational wellness, organizational well-being, job satisfaction, work environment, and nurses. A search strategy was designed for the purpose of this review (see Supplementary File 1), to search, from the databases inception up to and including the 29th of May 2022, the following databases: Medline (via PubMed); Cochrane Library; Cumulative Index of Nursing and Allied Health Literature (CINAHL); and Scopus.
Eligibility Criteria
Studies were deemed eligible for inclusion if they: (a) focused on the development and/or examination for evidence of validity of instruments; (b) recruited only nurses as participants; and (c) developed the instrument for measuring nurses’ organizational well-being or occupational health. In the case of published manuscripts reporting an instrument’s development separately from its validation, both of the respective studies were included.
Unpublished studies, published only in an abstract form, published in non-peer-reviewed journals, conducted on other healthcare professionals (e.g. physicians, nursing students, technicians, or mixed samples) or published in another language from Italian, English or Spanish were excluded. Manuscripts reporting an instrument’s validation in another language from that of its development, such as for the purpose of cross-cultural adaptation, were excluded from this review. Before starting the review process, initial research was conducted for pre-testing and discussion of the inclusion and exclusion criteria by all the researchers involved.
Selection of the Studies
Three researchers (GG, FZ and JF) conducted the database search and the selection of the studies was performed blindly using Rayyan (https://www.rayyan.ai/) after duplicates had been removed. The researchers read all the titles and abstracts separately and agreed on their selection. All the selected texts were then read in full by the researchers, and the decision on the final selection was unanimous. In the case of any dispute, another researcher (AS) was designated to make the final decision.
Data collection Process and Data Items
A data extraction table was developed to summarise the data from the final sample, reporting for each included study: author(s); year and country; study design; study setting; sample; results; and conclusion.
Quality Appraisal
The articles included in this review were assessed by two independent reviewers (JF, FZ) for their methodological validity using the COnsensus-based Standards for the selection of Health Measurement INstruments (COSMIN) checklist (Prinsen et al., 2018). The COSMIN checklist is a standardized instrument recommended for use in systematic reviews of measurement properties. This modular checklist consists of 12 boxes, with 5–18 items per box. Given the lack of a comparable or gold-standard measurement of nurses’ organizational well-being, and the COSMIN checklist being specifically developed for patient-reported outcome measures, we used, for our review, only the boxes evaluating general psychometric properties, namely: the instrument design, content and structural validity; internal consistency; reliability; measurement error; criterion and construct validity; convergent validity; and responsiveness. As per COSMIN guidance, each item of the checklist was assessed on the following response scale: very good; adequate; doubtful; inadequate; or not reported. Content validity was evaluated on a four-point scale: sufficient; insufficient; indeterminate; or inconsistent. According to Terwee et al., (2011), the lowest score of any box should be the overall score of the reviewed study, as the rating system appears to severely inhibit differentiation between studies and instrument development and validation. Therefore, a revised scoring was used (Speyer et al., 2019). The final quality ratings were calculated as a percentage using the following formula

The total percentage scores were then categorised as poor (0%–25%); fair (25.1%–50%); good (50.1%–75%); or excellent (75.1%–100%). Studies with a poor-quality score were deemed to have a low methodological quality and were thus excluded from the review, following the indications of Speyer et al. (2019). All disagreements arising between the reviewers were resolved through discussion, or by the involvement of a third reviewer (GG).
Data Extraction and Synthesis
Once the methodological quality of the included studies had been evaluated, data on the characteristics of the research were extracted and summarised by title, authors, years, aim, instrument name, research method, population and context, dimensions, and related items. According to the JBI Manual for Evidence Synthesis (Aromataris & Munn, 2020) and COSMIN guidance (Prinsen et al., 2018), the instrument’s measurement properties were tabulated, reporting the dimensions, items, response rate, content validity index, Cronbach’s alpha, Confirmatory Factor Analysis (CFA), and concurrent or convergent validity. The research data and instrument characteristics were extracted and tabulated by two reviewers independently (GG and FZ), and any disagreements were resolved by discussion. Instruments analyses were performed comparing dimensions and psychometric characteristics. Similarities and differences regarding instrument development and validation were summarised and analysed. Finally, the dimensions/variables reported in each instrument were categorized and summarised using the affinity of measurement concepts as the main criterion.
Results
From the database search, 3473 articles were retrieved. After removing duplicates (N = 261), the articles were screened by reading the title and abstract, and 3027 articles were subsequently removed for not validating any instrument (Figure 1). The remaining 185 articles were assessed for eligibility, excluding 162 because they had been conducted on other healthcare professionals than nurses (n = 35), 70 because the instrument did not measure nurses’ organizational well-being, 56 because they were identified as cross-cultural adaptations, and 1 due to copyright infringement. At the end of the selection process, 23 articles had been identified and methodologically evaluated. PRISMA 2020 Flow Diagram for New Systematic Reviews Which Included Searches of Databases and Registers Only.
Quality Appraisal Assessment
COSMIN Quality Assessment of the Included Manuscripts
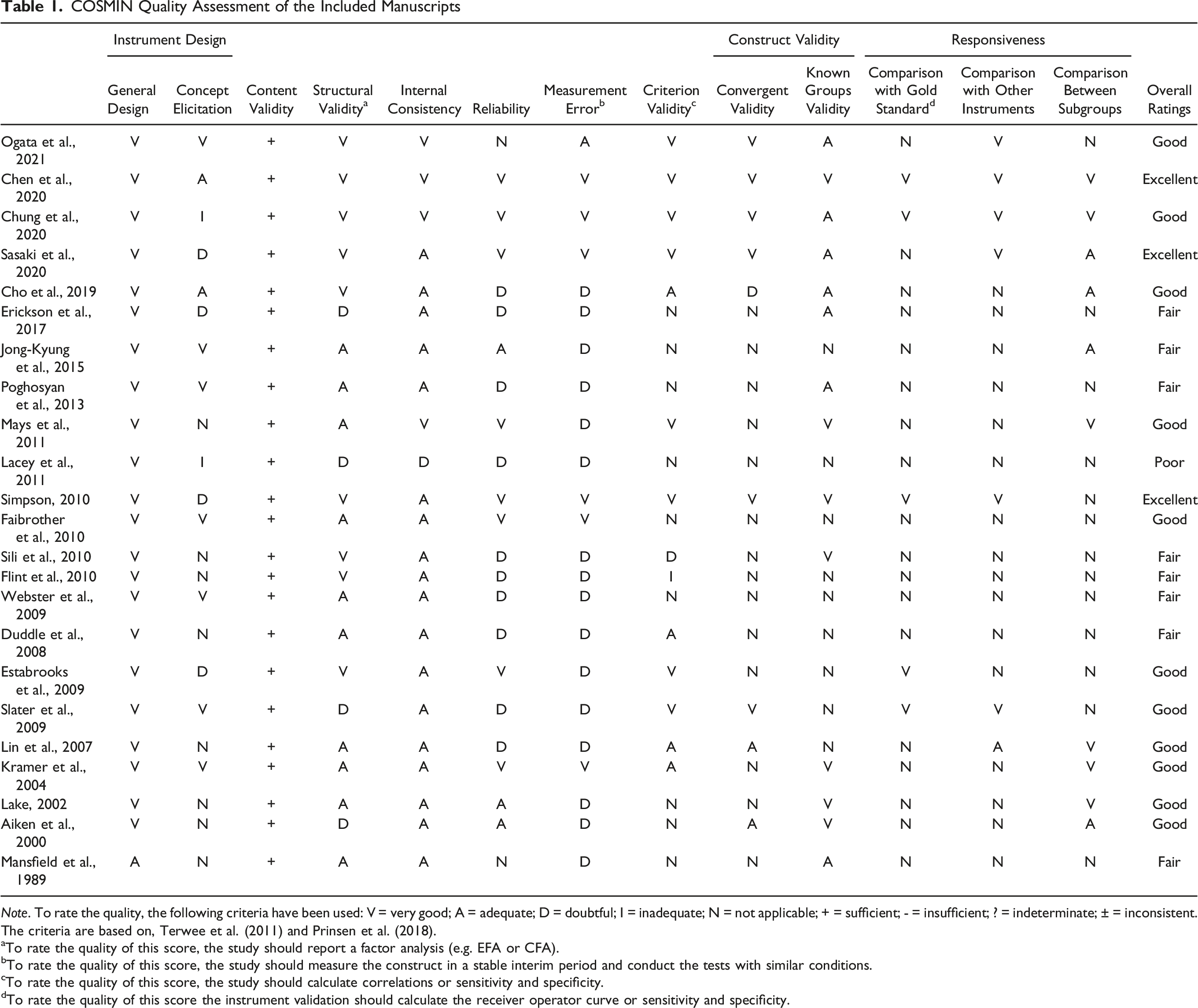
Note. To rate the quality, the following criteria have been used: V = very good; A = adequate; D = doubtful; I = inadequate; N = not applicable; + = sufficient; - = insufficient; ? = indeterminate; ± = inconsistent.
The criteria are based on, Terwee et al. (2011) and Prinsen et al. (2018).
aTo rate the quality of this score, the study should report a factor analysis (e.g. EFA or CFA).
bTo rate the quality of this score, the study should measure the construct in a stable interim period and conduct the tests with similar conditions.
cTo rate the quality of this score, the study should calculate correlations or sensitivity and specificity.
dTo rate the quality of this score the instrument validation should calculate the receiver operator curve or sensitivity and specificity.
All the studies had sufficient content validity, and most had a very good general instrument design and structural reliability, as well as adequate internal consistency. Limited information was retrieved on construct validity and responsiveness. Convergent validity was not reported in 14 of the studies, and no comparisons with a gold standard were reported in 18 studies, nor with other instruments in 16 studies, nor between subgroups in 13 studies. Scores assessed as inadequate in terms of concept elicitation were due to missing or incomplete qualitative data collection methods or analysis to identify relevant items for the development of the instrument (Lacey et al., 2011).
Instrument Characteristics and Statistical Methods
The final 22 included manuscripts were published from 1989 to 2021 and reported 21 instruments since the Brisbane Practice Environment Measure (B-PEM) was developed by Webster et al. (2009) and tested its validity separately by Flint et al. (2010). The instruments had between 2 (Mays et al., 2011) and 19 (Slater et al., 2009) dimensions, and between 12 (Mays et al., 2011) and 118 (Sili et al., 2010) items.
Psychometric Characteristics of the Instruments

Another relevant noted aspect concerned the concurrent criterion validity or the comparison of the newly developed instrument measure with one obtained by an instrument already tested for validity. Only 4 studies reported this assessment and comparison. Among these 4, Ogata et al. (2021) compared their instrument score with nurses’ intention to leave the profession, job satisfaction, and quality of care; Chen et al. (2020) associated the new instrument results with a previous version of the same; Sasaki et al. (2020) compared the Job Content Questionnaire results with overwork, depression, anxiety, and stress; Simpson (2010) equated the results of the core nurse resource scale with work engagement; and, lastly, Slater et al. (2009) used staffing, nurses’ relationships with head nurses, physicians and empowerment as terms of comparison.
Identified Dimension/Variable for Affinity and Measured by the Instrument

Note. X = dimension/variables identified and measured by the instrument.
Leadership and Support
The most common dimension was the leadership provided by head nurses and managers and the support they provided to work teams. Indeed, the presence of a leader with effective leadership styles and support for their professionals appeared to improve nurses’ perception of organizational well-being. This assessment of leadership appeared in many instruments (Aiken & Patrician, 2000; Chen et al., 2020; Cho et al., 2019; Estabrooks et al., 2009; Ives Erickson et al., 2017; J.-K. Kim et al., 2015; Kramer & Schmalenberg, 2004; Lake, 2002; Ogata et al., 2021; Poghosyan et al., 2013; Sasaki et al., 2020; Slater et al., 2009). For example, the Korean Work Environment Scales for Clinical Nurses (KWES-CN; Kim et al., 2015) investigated, in particular, the head nurse’s behaviour, role, vision, and character. The theoretical assumption that supports the inclusion of this dimension in the instruments lies in the relationship between organizational well-being and nurses’ perception of their head nurse, managers and organization. Accordingly, the instruments evaluated how nurses perceive the choices, work behaviours, management of interpersonal conflicts, support and gratification of their head nurses and managers. Another example is the Nursing Practice Environment Scale in Home Health Care (NPES-HHC; Ogata et al., 2021), which evaluated the leader’s ability to transform mistakes into opportunities and to monitor the work of staff and their development of skills.
Relationships and Communication
Relationships/communication with physicians and other professionals were investigated by various instruments (Cho et al., 2019; Duddle & Boughton, 2008; Estabrooks et al., 2009; Fairbrother et al., 2010; Ives Erickson et al., 2017; Kim et al., 2015; Kramer & Schmalenberg, 2004; Lake, 2002; Lin et al., 2007; Mansfield et al., 1989; Mays et al., 2011; Ogata et al., 2021; Poghosyan et al., 2013; Sili et al., 2010; Simpson, 2010; Slater et al., 2009). In particular, these instruments focused on the ability of staff to work together (Ives Erickson et al., 2017), and on the collaborative relationships between physicians and nursing staff (Kramer & Schmalenberg, 2004; Ogata et al., 2021; Poghosyan et al., 2013). For example, the Nursing Workplace Relational Environment Scale (NWRES) emphasises the dimension of “collegial behaviours”, referring to the types of behaviours that characterize a collegial workplace, including respect, support, the valuing of opinions, the exchange of ideas, open communication, and effective resolution of conflicts (Duddle & Boughton, 2008). Further underlining the importance of relationships for measuring organizational well-being, the same instrument included the “relational atmosphere” dimension, specifically concerning emerging behaviours of team members, both positive and negative, within work groups (Duddle & Boughton, 2008). In this regard, a supportive, encouraging and welcoming environment, as well as team spirit, would be associated with a positive relational atmosphere. Contrariwise, aggressive behaviour, resulting from a marked disaffection, would inhibit the good relationships in the team, or more generally in the same organization, and therefore degrade the perception of organizational well-being. This distinction between positive and negative indicators of organizational contexts in determining nurses’ organizational well-being was also found in the Nursing Questionnaire on Organizational Health (QISO; Sili et al., 2010). In this latter instrument, an entire dimension was dedicated to the assessment of nurses’ satisfaction with the relationships they have in the organization, including managers, head nurses and the team in which they work (Sili et al., 2010).
Work-Family Balance
The conflict between work and family commitments was another aspect measured (Chen et al., 2020; Ogata et al., 2021; Slater et al., 2009). The Nurses’ Occupational Stressor Scale dedicated a dimension to home-work conflicts, to globally measure nurses’ organizational well-being, while trying to understand how difficult it is to reconcile work and family demands (Chen et al., 2020). Similarly, the Nursing Practice Environment Scale in Home Health Care (NPES-HHC) measured nurses’ organizational well-being by focusing on how much work activities influenced time dedicated to one’s family (Ogata et al., 2021). Finally, the Nursing Context Index (NCI) considered it essential to measure work and social life balance, assuming it is closely associated with work-related stress, and therefore with nurses’ organizational well-being (Slater et al., 2009).
Work Demands
Work demands were examined as they influence nurses’ organizational well-being and were quantitatively assessed in terms of workload, but also time pressure and performance (Chen et al., 2020; Mansfield et al., 1989; Sasaki et al., 2020; Sili et al., 2010; Slater et al., 2009). In the Nurse Job Context Scale, the authors identified a first dimension that they called “general pressure/uncertainty”, to analyse pressures relating to numerous unpredictable situations that nurses in a hospital environment may have to face (Mansfield et al., 1989). Other authors of the studies included in this review agreed to consider excessive requests made by an organization to their nurses as a fundamental factor in nurses’ organizational well-being. Chen et al. (2020) dedicated a dimension to work demands, while in the Nursing Context Index (NCI; Slater et al., 2009) and the Nurse Job Satisfaction Scale (NJSS; Lin et al., 2007), authors referred to the specific construct of workloads. Sili and colleagues, on the other hand, studied the phenomenon from another point of view, explicitly including the demands made by an organization to their nurses in the work-related stress dimension of the QISO (Sili et al., 2010).
Violence
Violence is an emerging problem in healthcare systems and a dimension measured by Chen (2020) and Kim (2015). The Nurses’ Occupational Stressor Scale (NOSS) investigates verbal, psychological and physical abuse that nurses may suffer in the workplace, whether it comes from professionals, such as superiors or colleagues, patients, or their caregivers or family (Chen et al., 2020). The Korean Work Environment Scales for Clinical Nurses (KWES-CN; Kim et al., 2015) also included items regarding verbal and physical violence experienced by patients, caregivers, and other members of the care team, such as physicians and other professionals.
Control and Autonomy
The control and autonomy that nurses have in their workplace is an additional dimension measured in the instruments. For example, the Nursing Work Index (Aiken & Patrician, 2000) measured nurses’ autonomy and control over their work environment. Similarly, Kramer and Schmalenberg (2004), in the Essentials of Magnetism (EOM) tool validation study, dedicated two whole dimensions to measuring these aspects. Finally, the Job Content Questionnaire (JCQ) validation study (Sasaki et al., 2020) dedicated one dimension to the control that nurses have over their activities.
Satisfaction and Motivation
Many of the instruments measuring nurses’ organizational well-being investigated nurses’ satisfaction with various aspects of their work. For example, the Nursing Health and Job Satisfaction (NHJS) scale investigated various factors associated with job satisfaction (Chung et al., 2020). In particular, its “work environment satisfaction” dimension included five constructs: benefits, support, respect, security, and facilities. The QISO also analysed aspects of nurses’ satisfaction on a scale of positive and negative indicators of workplaces. This scale was composed of 4 different dimensions: overall satisfaction; overall dissatisfaction; satisfaction with management; and satisfaction with one’s operating unit (Sili et al., 2010). Furthermore, the Korean Work Environment Scales for Clinical Nurses (KWES-CN) explored the dimension of nurses’ satisfaction, particularly satisfaction with work hours and shifts (Kim et al., 2015). In the Professional Practice Work Environment Inventory (PPWEI), authors referred to motivation (Ives Erickson et al., 2017), while, in the Nursing Workplace Relational Environment Scale (NWRES), authors dedicated an entire dimension to satisfaction, intending to explore the connection between a person’s experiences in the work environment and job satisfaction or dissatisfaction (Duddle & Boughton, 2008). Finally, Slater et al. (2009) investigated the dimension of satisfaction in personal and professional aspects, referring to training, salary, and different job scenarios.
Work Environment and Resources
The work environment and available resources are additional variables measured by the included instruments (Chen et al., 2020; Cho et al., 2019; Chung et al., 2020; Estabrooks et al., 2009; Ives Erickson et al., 2017; S. Kim et al., 2017; Kramer & Schmalenberg, 2004; Lake, 2002; Lin et al., 2007; Mays et al., 2011; Sili et al., 2010; Simpson, 2010; Slater et al., 2009). The Nursing Questionnaire on Organizational Health (QISO; Sili et al., 2010) and the Professional Practice Work Environment Inventory (PPWEI; Ives Erickson et al., 2017) extensively investigated these variables. In particular, the QISO dimension called “comfort” measured the perception that nurses have of their working environment (Sili et al., 2010), including aspects included in similar instruments (Lin et al., 2007), such as cleanliness, lighting, temperature, silence, building conditions, satisfaction regarding rooms and accessories, available space per person (Estabrooks et al., 2009), and toilets. Instead, in the Professional Practice Work Environment Inventory (PPWEI), Erickson and colleagues (2017) focused on the particular resources provided by the organization to nurses, similar to other instruments (Chen et al., 2020; Cho et al., 2019; Chung et al., 2020; Estabrooks et al., 2009; Ives Erickson et al., 2017; Kim et al., 2015; Kramer & Schmalenberg, 2004; Lake, 2002; Ogata et al., 2021; Simpson, 2010; Slater et al., 2009). Specifically, the authors refer to the staffing (Cho et al., 2019; Estabrooks et al., 2009; Ives Erickson et al., 2017; Kramer & Schmalenberg, 2004; Lake, 2002), time (Estabrooks et al., 2009; Ives Erickson et al., 2017) and support services (Cho et al., 2019; Chung et al., 2020; Ives Erickson et al., 2017; Kramer & Schmalenberg, 2004; Lake, 2002; Ogata et al., 2021).
Careers
The possibility of career advancement or the existence of established career paths was a peculiarity measured by some instruments (Flint et al., 2010; Lin et al., 2007; Sili et al., 2010; Slater et al., 2009; Webster et al., 2009). For example, in the QISO, in the “perception of the enhancement of skills” dimension, Sili and colleagues analysed the perception that nurses have of the enhancement of their skills and their commitment to work (Sili et al., 2010). Similarly, a number of the instruments dedicated a dimension to measuring adequate acknowledgement and career and professional opportunities (Kramer & Schmalenberg, 2004), linking nurses’ organizational well-being to opportunities for professional development, both formally, through internal training programmes, and informally, through contact with more qualified personnel (Flint et al., 2010; Webster et al., 2009). The Brisbane Practice Environment Measure (B-PEM), for example, included a dimension called “professional development” to investigate opportunities for career advancement within the organization, and whether these opportunities were fair to all nursing staff (Flint et al., 2010).
Organizational Policy
Some instruments have measured also the organizational policy (Estabrooks et al., 2009; Ives Erickson et al., 2017; Kramer & Schmalenberg, 2004). The Essentials of Magnetism tool investigated the creation of a productive and satisfying work environment for nurses in “magnet” hospitals, measuring, in one of its 8 dimensions, “cultural values” (Kramer & Schmalenberg, 2004). Furthermore, the Alberta Context Tool included a dimension called “culture”, which the authors defined as “The way that ‘we do things’ in our organizations and work units, items generally reflecting a supportive work culture”, underlining attributed importance to the mission and vision of the organization (Estabrooks et al., 2009). In the Professional Practice Work Environment Inventory (PPWEI), one dimension measured “cultural sensitivity” to quantify organizational attitudes, practices and/or policies aimed at respecting and accepting cultural differences (Ives Erickson et al., 2017).
Discussion
The main purpose of this literature review was to identify and compare instruments for measuring nurses’ organizational well-being, and, as secondary objectives, to summarise the dimensions measured by these instruments and if possible, identify an instrument that comprehensively investigates nurses’ organizational well-being. Concerning the main aim, through this literature review, we have identified a total of 21 instruments to have been developed and tested for evidence of their validity in measuring nurses’ organizational well-being. Having read the manuscripts, this large number of different instruments could be due to the different interpretations and definitions of organizational well-being, leading to different concept constructions and consequently different instruments. In particular, some authors focused their attention on the context of organizations, analysing the demands on and resources provided to nurses (Chen et al., 2020; Cho et al., 2019; Chung et al., 2020; Estabrooks et al., 2009; Ives Erickson et al., 2017; S. Kim et al., 2017; Kramer & Schmalenberg, 2004; Lake, 2002; Lin et al., 2007; Mays et al., 2011; Sili et al., 2010; Simpson, 2010; Slater et al., 2009). Others, instead, concentrated on the working environment, investigating relational and communicative dynamics within work teams (Aiken & Patrician, 2000; Cho et al., 2019; Duddle & Boughton, 2008; Estabrooks et al., 2009; Fairbrother et al., 2010; Ives Erickson et al., 2017; S. Kim et al., 2017; Kramer & Schmalenberg, 2004; Lake, 2002; Lin et al., 2007; Mansfield et al., 1989; Mays et al., 2011; Ogata et al., 2021; Poghosyan et al., 2013; Sili et al., 2010; Simpson, 2010; Slater et al., 2009). For yet other authors, nurses’ organizational well-being could be measured through job satisfaction (Chung et al., 2020; Duddle & Boughton, 2008; Sili et al., 2010), or quality of life, referring to the balance between family and work demands or the amount of violence experienced in the workplace (Chen et al., 2020; S. Kim et al., 2017; Ogata et al., 2021; Slater et al., 2009).
To answer our secondary objectives, we have categorized and compared the dimensions of the existing tools for measuring nursing organizational well-being, according to their similarity. From the results appears that many aspects are studied in these instruments (second research question) and there is not a single instrument evaluating comprehensively this multidimensional concept, thus responding to the third research question. This heterogeneity might be explained by the lack of a single conceptual reference model for measuring nurses’ organizational well-being (DellaBella et al., 2022). In 2010, Sili et al. recognized the need for an adequate definition of organizational well-being in caring contexts, articulating it as “the set of managerial and coordination processes and practices aimed at caring for patients through the nurses’ involvement. A place of healthcare is a workplace in which professional integration and collaboration, the development, enhancement and consolidation of skills and the promotion of cultural growth are encouraged and ensured to build a sense of belonging to the profession and to the organization itself, which therefore ensures a work environment in which nurses feel they are promoters of health and motivated to pursue their professional mission” (Sili et al., 2010). Many instruments, however, were developed on the conceptual models used in organizational and occupational psychology and this review allows the identification of the core areas of an instrument that measures the nursing organizational well-being, such as the physical and organizational aspects, including workloads, working rhythms and shift work, and the nurses’ perceptions of their organization, managers, and work, referring to the autonomy in carrying out their work, or of supervisors exercising control over them, possibility of careers, and work-family balance. Many studies have already evaluated the repercussions of these two core areas on the single professional, his/her performance, and patients. Unsurprisingly, workloads are a source of physical and mental fatigue for professionals (Zaghini et al., 2020), as well as excessive pressure and control from superiors, which can generate stress and burnout (Liu et al., 2019). Under such conditions, nurses may negatively experience their organizational well-being, which, in turn, can negatively affect relations between nurses and patients and their caregivers. The leadership exercised by head nurses within operating units is crucial for improving not only motivation (Labrague et al., 2021) and satisfaction (De Moura et al., 2017), but also, importantly, patient outcomes (Fiorini et al., 2022) and safety (Farnese et al., 2019), and the quality of care given. A lack of autonomy and having to follow only the instructions of other team members are further possible sources of frustration and stress (Parizad et al., 2021) that can negatively affect organizational well-being. Nurses set specific objectives for their professional mandate, which may, in terms of times and methods, not coincide with what has been established by others. Having to limit oneself to following instructions may therefore lead to low motivation and job satisfaction (Chung-Yan, 2010). It is, furthermore, not surprising that a relational and communication dimension was present in almost all the instruments included in this review. Indeed, relational dynamics and interpersonal conflicts experienced by professionals can be a constant source of stress (Consiglio, 2014), which, if not carefully managed, can lead to the development of burnout syndrome (Safdar et al., 2020), especially in nurses (Zaghini et al., 2017).
Another element that emerged preponderantly from this literature review was career development. This result could be due to the lack of contractual and economic recognition, in certain countries, of nurses’ specialties, leading to the development of the phenomenon known in the literature as overeducation (Shahidan & Ismail, 2021). Carrying out a job that requires less training than you have or not being able to use your knowledge and skills in carrying out your work is a significant source of stress for professionals (Dudal & Bracke, 2019), associated with demotivation and job dissatisfaction (Satuf et al., 2018).
In the analysis of the articles included in this review, other common dimensions of the instruments were organizational culture and policy (Kramer & Schmalenberg, 2004) and work-family balance (Chen et al., 2020; Ogata et al., 2021; Slater et al., 2009). The mission and vision of healthcare organizations inevitably condition the behaviours and performance of its professionals. The balance between work and family is also a widely recognized source of stress (Molina, 2021), especially for female workers (Navajas-Romero et al., 2020). Considering that the majority of nurses are female, the dimension of the balance of family and work demands is particularly decisive in influencing organizational well-being.
Finally, considering the fourth research question, an evident heterogeneity of statistical methodologies has been used for the examination for evidence of the validity of instruments. Certain authors limited themselves to performing a content validation and internal consistency analysis (Aiken & Patrician, 2000; Kramer & Schmalenberg, 2004; Mansfield et al., 1989), while others also performed Exploratory and/or Confirmatory Factor Analyses (Cho et al., 2019; Duddle & Boughton, 2008; Estabrooks et al., 2009; Fairbrother et al., 2010; Ives Erickson et al., 2017; S. Kim et al., 2017; Lake, 2002; Lin et al., 2007; Mays et al., 2011; Poghosyan et al., 2013; Sili et al., 2010). Only a few authors also evaluated the concurrent criterion validity of the instruments (Chen et al., 2020; Ogata et al., 2021; Sasaki et al., 2020; Simpson, 2010; Slater et al., 2009), through comparison with control items or dimensions measuring similar constructs. Such methodological heterogeneity did not make it possible to directly compare the results, therefore it is difficult to draw definitive conclusions on which instruments can be used globally and can be most recommended for measuring nurses’ organizational well-being.
Limitations
The findings of this systematic literature review are specific and unique but must be considered in light of certain limitations. First, the large number of identified instruments and dimensions that composed them did not make it possible to summarise individual results and individuate a restricted number of variables to measure nurses’ organizational well-being; on the contrary, given the working contexts heterogeneity, it could be useful choose different tools for capturing various aspects. Moreover, many of the analysed instruments were developed and tested for their validity with different processes and psychometric analyses, avoiding comparisons among them with specific tests, and therefore related syntheses and interpretations. Finally, the multiple models and definitions of organizational well-being used for developing the instruments, and influencing the creation and validation of the instruments, have made it difficult to synthesize the results and investigate certain aspects. These limitations may have influenced the overall representativeness of the results.
Implications for Nursing and Health Policy
Healthcare and nursing managers should consider the results of this review because it focuses on and summarises the dominant aspects of nurses’ organizational well-being and presents instruments that can be used for monitoring organizational well-being in their organizations. The existence of numerous instruments for measuring nurses’ organizational well-being and the heterogeneity of constructs used for the instruments developed highlight the need to create a single instrument that can be used internationally and contains most of the dimensions considered essential for evaluating nurses’ organizational well-being. Future research should underline which of the included instruments is better at evaluating nurses’ organizational well-being and propose the universal use of an instrument for the comparison of data collected from across the world.
Conclusions
This literature review study had the main objective of identifying and comparing instruments for measuring nurses’ organizational well-being, and, as secondary objectives, of summarising the dimensions measured by these instruments and the statistical analysis performed for examining the measurement validity evidence and if possible, identifying an instrument that comprehensively investigates nurses’ organizational well-being. 22 manuscripts have been identified and 21 instruments measuring nursing organizational well-being have been developed and examined for evidence of validity, varying in several dimensions, items, and concept elicitation. This result is an added value of this study for the scientific community, as it underlines the core areas of already published instruments and of the concept of nursing organizational well-being that may be integrated, depending on the clinical settings, and organizational and research needs.
Supplemental Material
Supplemental Material - Measuring Nurses’ Organizational Well-Being: A Systematic Review of Available Instruments
Supplemental Material for Measuring Nurses’ Organizational Well-Being: A Systematic Review of Available Instruments by Giovanni Gioiello, Francesco Zaghini, Valerio Della Bella, Jacopo Fiorini, and Alessandro Sili in Evaluation & the Health Professions
Supplemental Material
Supplemental Material - Measuring Nurses’ Organizational Well-Being: A Systematic Review of Available Instruments
Supplemental Material for Measuring Nurses’ Organizational Well-Being: A Systematic Review of Available Instruments by Giovanni Gioiello, Francesco Zaghini, Valerio Della Bella, Jacopo Fiorini, and Alessandro Sili in Evaluation & the Health Professions
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.