
Abstract
The authors examine the roles of social connectedness in mediating the relation between the loss of loved ones and life satisfaction in older residents living in a retirement community. Data were collected through a mail survey on a random sample of 734 older residents (M age = 67 years, SD = 9.6 years) in a retirement community in the Southwest. Analyses were conducted using SPSS macros for estimating the indirect effects through multiple mediators. Participants who experienced the loss of loved ones in life reported statistically significantly higher life dissatisfaction scores than those who reported no such loss. The effects of loss on perceived life dissatisfaction were partially mediated by individual connectedness and satisfaction with received social support but not by support network size or collective connectedness. Interventions with older adults who experienced loss in life need to help alleviate their loneliness and increase their satisfaction with social support.
A large number of Americans aged 55 years and older choose to live in age-restricted retirement communities in the United States. For example, a retirement community in central Florida houses 36,000 residents (Snyder, 2004); three Sun City, Arizona, communities provide housing for more than 80,000 older adults, and most of them live in freestanding homes (Waldron, Gitelson, Kelley, & Regalado, 2005). The number of retirement community residents will continue to increase as 76 million baby boomers approach retirement age. A report from the housing industry found that 26% of baby boomers would consider living in “age-qualified” adult communities after their retirement (Del Webb Corporation, 2004), which is consistent with a recent finding on the basis of government housing data suggesting that roughly 29% of 55-and-older households choose to live among similarly aged persons (Metlife Mature Market Institute, 2009). For these reasons, the social dynamics of planned, same-age communities continue to interest social gerontologists, housing specialists, and community designers.
The concentration of older adults in certain communities creates both opportunities and challenges. We are particularly concerned with the social relationships within these communities and their roles in helping older persons maintain satisfying lives after experiencing the loss of loved ones. In a recent study, older adults were found to have expanded their social networks by making new friends after relocating to retirement communities (e.g., Waldron, Gitelson, & Kelley, 2005). However, because the homogeneous demographics of age-restricted communities increase exposure to loss, members of one’s immediate social network are more likely to experience loss due to serious illness. The effects of this likelihood on life satisfaction are not well understood. Furthermore, several features of retirement community living are potentially noteworthy. For example, these communities typically provide a considerable set of social activities, some of which might help a bereaved resident sustain satisfying social connections after the death of a spouse or close friend. However, in some communities, social participation is easier for married couples than it is for widowed persons (Waldron, Gitelson, & Kelley, 2005).
In addition, the move to a retirement community can complicate relationships with long-time friends and family members, often creating geographic or psychological distance in these relationships (Williams & Guendouzi, 2000). As a result, bereaved retirement community residents may be more vulnerable to feelings of loneliness and dissatisfaction. For this reason, in this study we focus on the effects of the loss of loved ones on the life satisfaction of residents of a large retirement community and how social connectedness mediates such effects.
Loss of Loved Ones and Life Satisfaction in Older Adults
Life satisfaction is conceptualized as elders’ sense that they are living meaningful and satisfying lives, which could range from utter dissatisfaction to complete life satisfaction. Predicting the life satisfaction of older adults has been a consistent objective of gerontological research (Depp & Jeste 2006; Strawbridge, Wallhagen, & Cohen, 2002). Literature suggests that the loss of a spouse, family members, or close friends is a significant risk factor for individuals’ life satisfaction, and it can be particularly harsh for adults at later life stages (e.g., Williams, 2003). According to socioemotional selectivity theory (Carstensen, 1992; Lang & Carstensen 1994), older people tend to have smaller yet closer support networks compared with younger adults. The theory posits that as older adults perceive that the life span is diminishing, they focus their emotional investments on the most meaningful relationships. Consequently, the loss of one of these valued relationships can directly affect life satisfaction, not to mention secondary stressors associated with loss, such as diminished meaningful social roles and lost connections to mutual friends.
Abundant empirical evidence has underscored the close relations between spousal loss and declines in social and psychosocial well-being. The loss of a spouse can trigger a decrease in social participation (Utz, Carr, Nesse, & Wortman, 2002) and cause depression, anxiety, and lost passion for life (Wilcox et al., 2003). Although a relatively small number of studies have focused on the impacts of the loss of close friends or family members other than a spouse, it is obvious that friendships and family ties are key ingredients to life satisfaction of people across the life span (Pinquart & Sörensen, 2000) and are particularly important for older adults as a means to buffer life stress (Lang & Carstensen, 1994). For this reason, we examined the life satisfaction of those who lost a spouse, a family member, or a close friend.
Social Connectedness and Life Satisfaction in Older Adults
Supportive social connections appear to be an important factor for older adults’ mental and physical well-being (Bourque, Pushkar, Bonneville, & Béland, 2005; Depp & Jeste, 2006). Cavanaugh (1998) commented that having a group of people to whom older adults can relate is essential in their dealing with life challenges associated with older age. Baxter et al. (1998) found that supportive network size and contact were positively associated with perceived quality of life in a sample of Caucasian and Hispanic older adults in southern Colorado. Social connectedness can be a broad term; for our purposes, it is defined as the extent to which a person participates in relationships with others.
It is crucial to note the existence of the multiple and overlapping dimensions of social connectedness. It appears, for instance, that the perceived availability of supportive persons is more consequential to mental well-being than the amount of support actually received (for one comprehensive review, see Uchino, 2004). At the same time, satisfaction with social relationships is perhaps most important. Older adults may be satisfied when engagement in these relationships meets or exceeds their expectations, even if the levels seem quite low to others (see Sarason, Sarason, Shearin, & Pierce, 1987). Goldsmith (2004) argued that the literature on social connectedness lacks theoretical grounding and fails to consider how support is actually transacted through communication behaviors and social activity. She noted that a given kind of social connection can be helpful at one level of analysis (individual) but disruptive at others (romantic relationships, family). Thus, a widower’s forming of a new romantic relationship might be a source of personal satisfaction but also a cause of stress in the widower’s relationship with adult offspring.
Taking Goldsmith’s (2004) argument into account, we grounded our thinking in a larger theoretical perspective and acknowledged that social connectedness can function at individual, relational, and collective levels. We adopted Brewer and Gardner’s (1996) model of social identity, an approach that is grounded in the assumption that people possess a lifelong need for social connectedness. For Brewer and Gardner, social identity is how individuals define themselves in relationships to others or to social groups. In this formulation, identity is not a unitary concept. Rather, multiple identities emerge and are sustained through various kinds of social interaction.
Hawkley, Browne, and Cacioppo (2005) further used this notion of social identity as they studied social connectedness in samples of college students and older adults. The results supported a three-part conception of social connectedness. Individual connectedness referred to a person’s subjective psychological assessment of his or her identity as an isolated person or one who is linked closely with others. This assessment is quite different from more objective indicators of social network participation, such as the number of friends or family available to provide social support. Indeed, even people who report having many social contacts may feel that they lack close emotional connections to other people. Conversely, those with relatively small social networks may feel closely linked to others. In this way, individual connectedness matches closely with the emotional dimension of loneliness (Russell, 1996; Russell, Peplau, & Cutrona, 1980). Hawkley et al. used loneliness measures to operationalize individual connectedness. In contrast, relational connectedness was a person’s sense that he or she belonged to a network of friends and family members: people who were available and supportive. Reports of relational connectedness were predicted by the regularity of contact with friends and close relatives. Collective connectedness was an elder’s perception of social belonging. It was predicted by the number of group memberships (e.g., religious organizations, clubs) of older respondents and social activity engagement.
Impact of Loss on Social Connectedness in Older Adults
Loss, particularly traumatic loss such as the unexpected death of a spouse, disrupts social connectedness via multiple pathways. First, the victim of a loss often feels as if his or her personal identity has been shattered (Tedeschi & Calhoun, 2004) and his or her place in the world has been upended. For example, after the loss of a spouse, it is no longer possible to identify oneself as married, a valued aspect of identity for many older persons. In retirement communities, the identity derived from marriage can extend to certain social activities in which participation “as a couple” is the norm. The narratives told by those who have experienced major losses suggest that the fracturing of this joint identity is an important theme in a substantial number of cases (Keeley & Koenig Kellas, 2005). The result may be a sense of loneliness or lack of what we previously identified as individual connectedness.
The death of a spouse affects social connectedness at the relational level too. In addition to losing a valued partner and source of social support, the grieving spouse may find that certain kinds of relationships are no longer available. Connections to the spouse’s family may be reduced. Mutual friends may drift away. Supportive connections facilitated by the lost spouse may also be affected. He or she may have been the one to maintain connections with recreational partners (e.g., a golfing or card group), service providers (auto mechanics, tax specialists), and occupational communities (former coworkers, fellow union members).
The loss of a spouse may inhibit participation in community life. For example, if the spouse was a source of transportation, the remaining spouse may find it difficult to attend social events or to travel outside the boundaries of the retirement community. As implied above, some community activities such as dances or concerts may be designed and advertised for couples rather than individuals. Finally, the deceased spouse may have been an important advocate for a partner who was reticent, hampered by stroke-related communication difficulties, or intimidated by authority. As a result, the remaining spouse may avoid some encounters, choose not to seek the help he or she needs (e.g., subsidized transportation), and decide against participating in activities that require facile communication. In short, his or her participation in community life is curtailed by the lack of a supportive spouse.
On the basis of this reasoning and the three-part conceptualization of social identity (Brewer & Gardener, 1996; Hawkley et al., 1995), we argue that the loss of a loved one may have effects at the individual, relational, and collective levels of social identity. All of these levels of identity are likely affected, but the effects may not be uniform. For example, the loss of a spouse may be particularly devastating to an elder’s (individual-level) feeling of emotional isolation, even as it has limited effects on his or her collective identity as a member of various religious or civic organizations.
The Mediating Roles of Social Connectedness Between Loss and Life Satisfaction
Evidence reviewed in previous sections has established the relationships between loss of loved one, social connectedness, and life dissatisfaction, suggesting meeting assumptions for a possible mediation (Baron & Kenny, 1986). Thus, we pose causal relationships among these variables, as noted in Figure 1. We conceptualize that the loss of loved ones would have a direct effect on life dissatisfaction and an indirect effect through social connectedness.
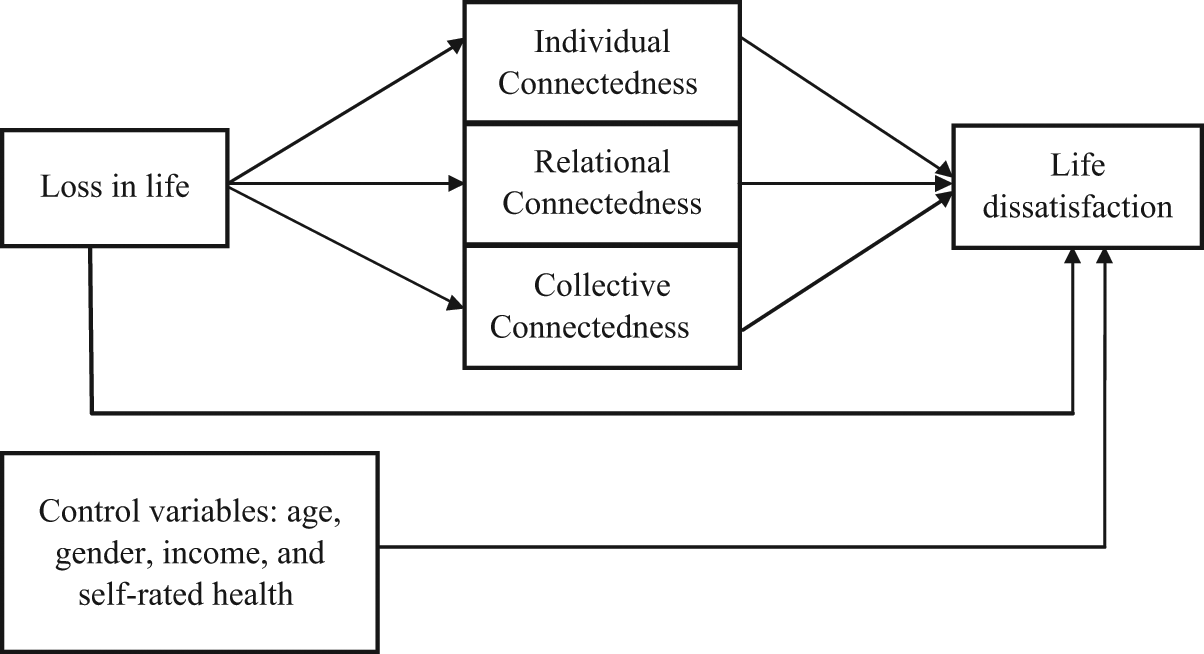
A conceptual model of social connectedness mediating loss on life dissatisfaction.
We began by establishing that the loss of loved ones often leads to increased dissatisfaction with life (Hypothesis 1). The loss of loved ones could result in the loss of financial resources, intimacy, and social support, which would likely result in life dissatisfaction. Research has established that for elders, social connectedness has potentially strong effects on their self-reported feelings of life satisfaction and dissatisfaction. Therefore, we posited that the three distinct forms of social connectedness presented earlier should mediate the effects of loss.
First, drawing from the work of Hawkley et al. (2005), we expected that the effect of loss of loved ones on life dissatisfaction would be mediated by individual connectedness (Hypothesis 2). Loss may affect individual connectedness, which in turn affects life dissatisfaction. Higher levels of individual connectedness retained should reduce the effect of loss on life dissatisfaction.
Second, measures of relational connectedness should have mediating effects on the association between the loss of loved ones and life dissatisfaction (Hypothesis 3). This variable involves measures of the social support network rather than individual feelings of loneliness (see Hays & DiMatteo, 1987). The loss of loved ones would impair relational connectedness, and elders who have networks of supportive friends or family members should feel less dissatisfaction with life following the loss of beloved individuals, because they can more easily access help and emotional support (Ha, 2008). Both the quantity and quality of the social relationships contribute to relational connectedness, but the key factor may be the degree to which an elder feels satisfied with his or her network of connections (Adams & Blieszner, 1995; Ingersoll-Dayton, Morgan, & Antonucci, 1997). Consistent with this idea, a recent longitudinal study of older caregivers found that the support of caring persons predicted overall life satisfaction over the 5-year period following the death of an important person (Clay, Roth, Wadley, & Haley, 2008). In addition to providing emotional or tangible support, friends or relatives often encourage bereaved persons to increase their participation in potentially satisfying life activities (Gallagher, 1994).
Finally, collective connectedness may mediate the effects of loss on dissatisfaction with life (Hypothesis 4). This may be particularly true in planned retirement communities, where residents typically report membership in numerous social groups and attend a variety of activities. The social connectivity provided by membership in these groups may be helpful as elders attempt to preserve social identity after the loss of a spouse, family member, or close friend. As mentioned earlier, the loss of a spouse may make it difficult to participate in activities such as dance lessons or couples-oriented social clubs. Thus, the loss of a loved one may influence dissatisfaction with life via collective connectedness.
Method
We used survey data collected between 2007 and 2008 from a sample of residents in a retirement community that was built in 1979 in Phoenix, Arizona. A stratified random sample (n = 1,268) on the basis of age and sex was first taken from the community’s recreation association database, which contains all the households in the retirement community. The data collection process involved four mailings. Respondents were sent a self-administered survey developed cooperatively between the recreation association and the study authors. A postcard reminder was sent 10 days after the first survey was mailed. A replacement survey was sent 2 weeks later to those who had not responded, and a final replacement survey was sent to nonrespondents 2 weeks after that.
The overall response rate was 63%. The final sample included 734 residents of the residential retirement community. Participants reported an average age of 67 years (SD = 9.6 years), 62.4% were women, and 96.5% were White. On average, they had lived in the community for about 7.4 years (SD = 5.9 years). The median household annual income interval for this sample was $50,000 to $75,000, and 61.4% had associate’s degrees or above. About one quarter of the sample reported at least one loss in the past 2 years. There were 22 participants who lost a spouse, 96 who lost family members, and 104 who lost close friends.
Measures
Dependent variable: life dissatisfaction
The level of life satisfaction was measured by a summed score of a five-item instrument designed to assess global judgments of life satisfaction (Pavot & Diener, 1993). The five questions are “In most ways my life is close to ideal,” “The conditions in my life are excellent,” “I am satisfied with my life,” “I have gotten the important things I want in life so far,” and “If I could live my life over, I would change almost nothing.” The scale was measured on a 7-point, Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). We reverse-coded the scores so that higher scores indicated higher levels of dissatisfaction or lack of satisfaction. The total score of the scale ranges from 7 to 35. The scale is available in the public domain and has exhibited acceptable psychometric properties in previous research. The internal consistency of this scale for this sample is .89.
Independent variable: loss of loved ones
Participants who reported at least one loss of a spouse, family member (child, sibling), or close friend in the past 2 years were categorized as the loss group and those who did not experience losses in the past 2 years as the nonloss group.
Mediating variables: social connectedness
Social connectedness was measured as individual, relational, and collective connectedness. Consistent with previous conceptualization (Hawkley et al., 2005), individual connectedness was measured by five questions from the UCLA Loneliness Scale (Russell, 1996). The items asked participants to rate the extent to which they agreed with a given statement on a 5-point scale ranging from 1 (almost always) to 5 (almost never). The five items are simple and valid measures of individual perception of social connectedness (i.e., “There are people that I talk to,” “There are people I can turn to,” “I feel alone,” “I feel I am no longer close to anybody,” and “I lack companionship”; Hawkley et al., 2005). The last three items were reverse coded, and a total score was calculated, ranging from 5 to 25, with higher scores indicating higher levels of individual connectedness. For this study, the internal consistency of the scale was .85.
Relational connectedness was measured by participant support network size and participant satisfaction with received social support. Support network size was measured by the average number of people from whom participants could receive assistance in eight different areas: financial assistance, technical advice, caregiving support, making new friends, helping with chores, sharing feelings, resolving family conflicts, and boosting confidence (Waldron, Gitelson, Kelley, & Regalado, 2005). The average support network size for this sample was 2.6 (SD = 2.8). Satisfaction with received support from friends and families was measured by a four-item scale adapted from the Social Support Questionnaire (Sarason et al., 1987) that asked participants to rate satisfaction with social support on a scale ranging from 1 (not at all) to 4 (very satisfied). Participants rated their satisfaction with the amount of emotional support, advice and information support, help received in times of health problems, and friends made in the retirement community. The summed score ranges from 4 to 16, with higher scores indicating higher levels of satisfaction. The internal consistency of the scale was .85.
Collective connectedness was measured by participants’ membership in organizations and their engagement in social activities. Participants were asked to respond “yes” (coded 1) or “no” (coded 0) to four questions: (a) “Do you belong to a social club?” (b) “Do you belong to a religious organization?” (c) “Do you currently engage in volunteer work within the retirement community?” and (d) “Do you currently volunteer in a setting outside of your retirement community?” The total score ranges from 0 to 4. Engagement in social activities was measured by the number of activities (i.e., sports, playing games, attending workshops, going to cultural events, working on crafts, and attending musical events) that participants did on a regular basis. It ranges from 0 to 6.
Control variables
We controlled for some known factors that influence life satisfaction: age, gender, income, and health (Ehrlich & Isaacowitz, 2002; Pinquart & Sörensen, 2000; Waddell & Jacobs-Lawson, 2010). Age was measured in years; female gender was coded 0 and male gender was coded 1. Household income was measured in dollar intervals. Self-rated health was measured by one question adapted from the SF-36 Health Survey (Ware, Snow, Kosinski, & Gandek, 1993) that asked participants to self-rate their physical health condition from poor (1) to excellent (5).
Analysis Strategies
Descriptive analysis was used to describe the sample characteristics broken down by those who experienced loss in life and those who did not. Correlation analysis was then conducted to reveal the bivariate relationships among mediators, controls, and outcome variables. Following the suggestions of Baron and Kenny (1986) for mediation analysis, we first tested the main effect of loss on life satisfaction by running a regression analysis controlling for demographics and self-rated health. We then conducted a multiple mediation analysis with three levels of social connectedness as mediators: individual connectedness, relational connectedness (support network size, satisfaction with received social support), and collective connectedness (memberships in organizations, social activity engagement). We ran this mediation analysis using SPSS macros for estimating and comparing indirect effects in multiple mediator models developed by Preacher and Hayes (2008). Their approach was developed from MacKinnon’s (2008) chapter on multiple mediator models and provides statistical estimates of indirect effects along with confidence intervals using a bootstrapping method. The total effects of loss in life on life satisfaction are composed of the direct effects of loss in life (effects controlling for mediators and covariates) on life satisfaction and the indirect effects of loss via mediators on life satisfaction. This mediation model involves testing the statistical significance of direct and indirect effects of loss in life and provides confidence intervals for the estimated effects so that researchers can determine the specific mediating effect for each mediator (Preacher & Hayes, 2008). Each test in this study used an α level of ≤.05 to determine statistical significance.
Results
Table 1 compares the characteristics of participants who experienced loss with the characteristics of those who did not. Participants who experienced loss reported statistically significant higher dissatisfaction scores than those who reported no loss (p < .01). In terms of social connectedness, those who experienced loss reported lower levels of individual connectedness (p < .01) and lower satisfaction with received support (p < .01) than those who had no loss. The two groups did not differ on the other three dimensions of social connectedness (i.e., support network size, membership in organizations, and social activity engagement) or on their age, gender, income, and health status.
Characteristics of Those Who Experienced Loss in Life and Those Who Did Not

Note: Data are expressed as M (SD) or as percentages.
Chi-square value (df = 1).
p < .01.
Table 2 presents the bivariate correlates of life dissatisfaction. Higher income, better health, and engagement in more types of activities were correlated with lower levels of life dissatisfaction. Age was not related to life dissatisfaction. Women reported statistically higher life dissatisfaction than men (p < .05). All five indicators of social connectedness were related to life dissatisfaction in the expected direction. Yet the magnitude of the relation varied among the four indicators. Individual connectedness was moderately related to life dissatisfaction (r = −.55), followed by satisfaction with social support (r = −.54), average support network size (r = −.17), and then social activity engagement (r = −.14). A weak though statistically significant correlation (r = −.08) was found between membership in organizations and life dissatisfaction.
Bivariate Correlates of Life Dissatisfaction
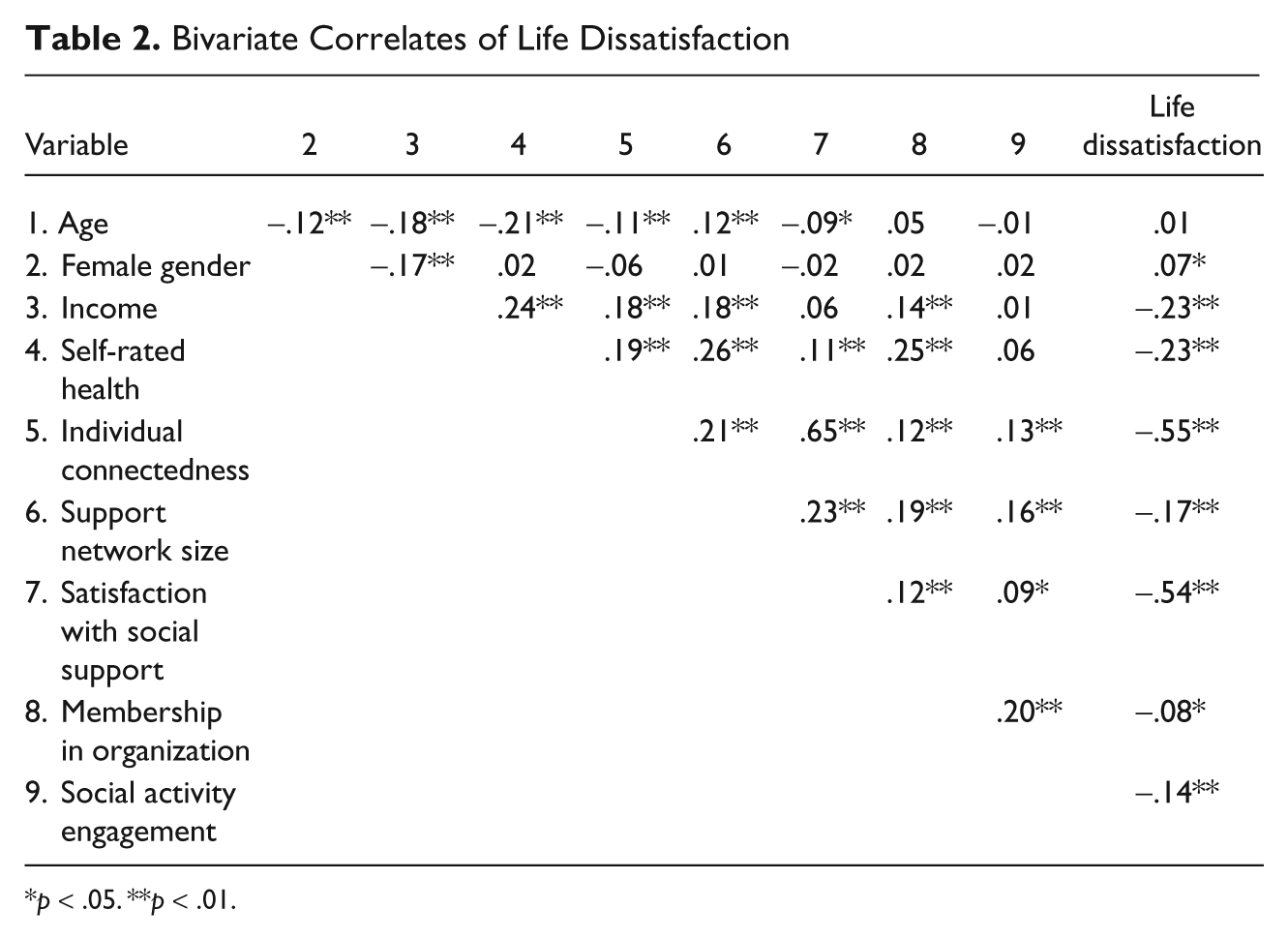
p < .05. **p < .01.
The first model in Table 3 provides the results using loss and controls as predictors for life dissatisfaction. We found that the experience of loss was positively related to life dissatisfaction (B = 2.26, p < .01). The explained R2 value was .24. The second model in Table 3 shows the results using SPSS macros for estimating multiple mediators. The loss of loved ones still predicted life dissatisfaction (B = 1.50, p < .01), but there were indirect effects of loss through individual connectedness (B = 0.43, 95% confidence interval = 0.12 to 0.91, p < .05) and through satisfaction with received social support (B = 0.49, 95% confidence interval = 0.17 to 0.92, p < .05). Because of these significant indirect effects, we can conclude that the reductions in the effects of loss (B from 2.26 to 1.50) on life dissatisfaction were due to individual connectedness and satisfaction with received social support. Because the direct effect of loss remained significant, the mediation was partial.
Direct and Indirect Effects of Loss on Life Dissatisfaction Scores via Social Connectedness

Note: The change in R2 value from Model 1 to Model 2 was significant (p < .01).
p < .05. **p < .01.
Support network size, membership in organizations, and activity engagement did not independently predict life dissatisfaction, and neither did they mediate the relationship between loss and life dissatisfaction. The adjusted R2 value in Model 2 is .45, indicating that a moderately large portion of the variance of life dissatisfaction was explained in the mediation model. To better illustrate, we constructed a path diagram including the estimates of direct effects of loss and mediators on life dissatisfaction on the basis of the output from our mediation analyses (see Figure 2).

Results of estimates of direct effects of loss and mediators in a path diagram.
Discussion
We examined the roles of different levels of social connectedness in mediating the stress of losing a loved one on life dissatisfaction for retirement community residents. Not surprisingly, our first hypothesis, that the loss of loved ones would negatively influence life satisfaction, was confirmed. This finding itself is in line with people’s common sense and corresponds to the bereavement literature (Stroebe, Abakoumkin, & Stroebe, 2010; Wisocki, 1998). Among the three mediation hypotheses, that individual connectedness would mediate the effect of loss on life satisfaction was supported (Hypothesis 2), that relational connectedness would mediate the effects of loss on life satisfaction was partially validated (Hypothesis 3), and that collective connectedness would mediate the effects of loss on life satisfaction was not supported (Hypothesis 4). In the following section, we provide explanations of our findings of the mediation analyses, address the limitations of this study, and conclude with a discussion of practical implications of our findings.
Individual connectedness was found to mediate between loss and life dissatisfaction. A lack of individual connectedness was conceptualized in this study as subjective feelings of loneliness or emotional isolation. Emotional isolation appears in the absence of desired companionship, which is not necessarily tied to physical isolation. Emotional isolation is a consistent risk factor for depressive symptoms (Blazer, 2002) and a strong correlate of poor physical health (Fees, Martin, & Poon, 1999) among community-dwelling older adults. Pinquart and Sörenson (2001) concluded from their meta-analysis on loneliness of older adults that the quality of a social network (e.g., having a confidant, feeling loved) rather than quantity is more central to loneliness. For those who live in retirement communities, disconnected from former homes and neighbors, the sense of companionship or emotional support would be more important during times of grief and loss. Consistent with the reasoning of socioemotional selectivity theory (Carstensen, 1992), our finding validates that emotional connectedness is important to life satisfaction in later adulthood. It is evident that loss could cause feelings of loneliness, but our findings add to the literature that the negative effects of loss on life satisfaction could be partially alleviated if the bereaved person perceives that desired emotional support is available. This is in line with Weiss’s (1975) argument that loneliness caused by the absence of a close emotional attachment due to bereavement can be compensated only by the integration of another emotional connection.
Support network size did not mediate the relations between loss and life dissatisfaction, which is not a surprising finding. Consistent with previous work (Pinquart & Sörenson, 2001), we concur that the size of support network might be relatively unimportant, as not all social relationships and interactions contribute to the well-being of older adults. We suspect that in times of bereavement, people need comfort and support from trusted sources, which might have little to do with the size of the support network. In contrast, we identified a significant mediating effect for the satisfaction with received social support. This finding once again validated the socioemotional selectivity theory, which suggests that for older adults the supportive ties that meet their expectations are more important than the mere number of contacts or network size (Carstensen, 1992; Sarason et al., 1987). For example, Pinquart and Sörensen (2001) found that older adults report more happiness than young adults in spite of their smaller support network sizes. Similarly, we conclude that even in times of grief, older adults who are satisfied with received support fare much better than those whose support fell below their expectations.
Guided by previous literature (Potts, 1997), we believe that connectedness to the community would be less important than the connectedness formed at individual and relational levels. We found no significant relations between collective connectedness and life dissatisfaction after adjusting for controls and other mediators. Residence in a retirement community provides social exposure but may not guarantee access to close relationships. By the same token, memberships in clubs or religious organizations and volunteering provide opportunities for older adults to socialize but may not ensure companionship or intimacy to follow. Another explanation could be heightened exposure to loss in retirement communities. People may join clubs or engage in community with their spouses and peers. After the death of a spouse or peers, participation in this activity may be curtailed. In this case, memberships in organizations might not relieve the person from the distress of loss but might instead cause more grief. Interestingly, social activity engagement, the other indicator of collective connectedness, was similarly insignificant in the multivariate mediation model. One explanation is that such engagement might influence life satisfaction through mechanisms such as reducing feelings of loneliness or increasing satisfaction with social support. When these two variables were included in the model, they likely removed the effects of social activity engagement.
It is worth noting that all the mediation effects identified in this study are partial, which means that only a portion of the influences of loss are mediated. This finding implies that the loss of loved ones has a substantive impact on older adults’ life satisfaction, which cannot be fully mediated by social connectedness. In light of this, a bereaved person may not experience life satisfaction to the same degree as he or she did prior to the loss, even when satisfying types of support were provided to assist readjustment and grief. It is understandable that lost relationships cannot be easily replaced. Longitudinal studies on bereavement found that people take up to 4 years or longer to recover from death of a loved one (Ferraro, 1984). Future studies need to examine other concepts (besides social connectedness) through which helping professionals can intervene to reduce the impacts of loss on older adults’ life satisfaction.
This study was limited in several ways. Because of the cross-sectional design, we did not examine the patterns of social connectedness over time. Related to this, we did not know whether the losses came after long illnesses, which might give people more time to prepare for the loss or build alternative forms of support. We also had little information about the quality of the lost relationships. These factors need to be examined in future studies. Our findings were based on a single retirement community population in the southwestern United States, which might have limited generalizability to other areas. Recalling the relatively young age (M = 67 years) of the participants, we note that loss might not be a prevalent experience for residents in this community, and the results might be different if we examined a retirement community dominated by residents who are much older. Because a relatively small percentage of participants in this sample experienced loss, we did not have sufficient statistical power to detect the differences for each relationship type. Future studies should examine the different impacts due to the loss of a spouse versus the loss of relatives or friends. Another limitation could be the measure of collective connectedness in the data set. Although membership in organizations and social activity engagement has been used in previous literature to indicate collective connectedness, we might have missed the evaluative aspect of collective connectedness (e.g., a sense of belonging to an organization, relationships within an organization).
Despite the above-mentioned limitations, our findings lend themselves to several theoretical and practice implications for gerontological researchers and service professionals. This study supports the conceptualization of social connectedness as a multiple-dimensional construct with different roles for each dimension in mediating loss effects on life dissatisfaction. Our study in an aging population in a retirement community suggests that the intimacy and quality of social relationships are more important than the size of the social network. Future researchers can expand our findings by examining the relations of loss, social connectedness, and life satisfaction using a national sample or a longitudinal design.
Implications
From a practice perspective, first, it is important to expand awareness about the effects of loss on aging residents who experience loss. We suspect that normal processes of grief may be amplified when many elders live in close proximity and the rate of loss is relatively high. One way would be to prepare the recreational and social infrastructure in the community to be alert to the needs of grieving residents for increased social support following the loss of a loved one. The infrastructure is composed of service providers such as pharmacists and neighborhood association representatives, who come in contact with grieving residents. Upon noticing that a resident has suffered a loss, these providers could refer the resident to mental health professionals, grief support groups, or social organizations depending on the situation. On subsequent contacts, they might inquire about the grieving person’s success at making these kinds of connections and encourage initial efforts to seek new sources of social support. In this way, the service provider becomes a new member of the support network and facilitates the resident in making the relational connections that seem to be so influential in our own study. In addition, a resident who is approached by others may find such activity incompatible with the identity of a lonely person. As our data suggest, this subjective evaluation of the self seems to mediate the effects of loss on life dissatisfaction.
Second, community activity planners and staff members might supplement existing recreational activities and social organizations with initiatives designed to facilitate identity readjustment. A resilient response to loss may require a resident to replace or reimagine elements of his or her identity. A man who has traditionally attended dances with a spouse might learn to replace this “couple identity” with a new “single dancer” identity. Community staff members may help find venues in which single older people are appreciated and supported in their pursuit of social connection. In a different example, community staff members can play the role of brokers linking older persons in need of social connection to appropriate services. Consider a nondriving widow who is socially isolated by the death of her husband, who used to drive her to the library to meet with members of a valued book club. If a librarian or club member recognized her isolation and helped her find transportation, the widow could retain her mobility, affirm her identity as a book club member, and remain socially and intellectually engaged with valued peers. Here again, the stark effects of loss on the life satisfaction of an elderly person could be mediated by perceptions of individual and social connectedness, both of which should be responsive to this modest form of intervention. In this latter case, we note that it is not merely membership in the book club that should matter most. Our data suggest that simple membership is not enough. Rather, it is the resident’s identity as a person with meaningful connections to others and her perception that satisfying sources of social support remain accessible to her.
Third, our study has potentially important implications for counselors, social workers, and others who have therapeutic contact with grieving residents of retirement communities. One implication is that such professionals may conduct a kind of “audit” of a client’s social identity after a loss. It may not be enough to encourage a resident simply to “stay involved” in community life or “make new friends” as routes to improved life satisfaction. Rather, changes in the clients’ identities should be considered.
The audit might include a review of the kinds of relational connections that have been weakened by the loss, directly or indirectly. Some of these are obvious. The loss of a spouse may mean that a client’s single most important link to emotional support has been broken. But others disruptions may be less direct. To whom will a client talk when he or she needs to find a car repair service? If a client and his or her spouse socialized primarily with other couples, the client’s access to activity companions may be hindered. In this way, the audit should consider the different kinds of supportive connections, the degree to which they are now unsatisfying, and the means by which new or modified relationships can be formed.
A cautionary tale is found in the work of Heller, Thompson, Truba, Hogg, and Vlachos-Weber (1991), who experimented with an intervention in which elderly women with low perceived levels of support were paired (after an initial assessment) with peers who provided support via telephone conversations. A comparison group received friendly telephone support from mental health staff members. The results suggested no differences between the treatment groups on measures of loneliness and depression and no differences between those groups and a third control group. Although a number of explanations are possible, one possibility is that the interventions were not appropriately calibrated to the social identities of the participants. Although it is clear that the participants described themselves as low in individual connectedness, it seems unlikely that merely talking with another disconnected person would change that identity substantially. As Heller et al. noted, these women generally experienced low levels of support from their family members, and it may be this kind of support that is central to their social identities. Talking on the phone with relative strangers may be of little help in such instances. Perhaps assistance with the process of strengthening family ties would have been more effective. In the case of loss, interventions should be focused on rebuilding the kinds of social connections that have been most disrupted. Of course, as our data make clear, loss is a major influence on life satisfaction, one that will be only partly mediated by any form of social support.
Although exemplary intervention models in this regard are not yet available, additional commonsense strategies should work to the advantage of grieving community residents. Carstensen and Fremouw (1988) suggested that only intrinsically rewarding social interaction could sustain with the removal of external rewards. It might be important to create a vibrant recreational and social culture that are rewarding for single adults, supplementing that which develops around married pairs. Another idea is the use of Internet-based support groups, which might be particularly helpful to grieving residents with mobility limitations (Barrera, Glasgow, McKay, Boles, & Feil, 2002; Waldron, Gitelson, & Kelley, 2005). Finally, previous research suggests that opportunities to cross the physical and psychological boundaries that are often constructed around retirement communities can be helpful (Waldron, Gitelson, & Kelley, 2005). Residents who sustain friendships and supportive connections in the larger community may fare better when faced with stressful circumstances.
Conclusions
This study focuses on intricate relations between loss, social connectedness, and life satisfaction among a rapidly growing aging population living in retirement communities. Loss, related to aging and complicated by disconnection from previous support networks, challenges the well-being of retirement community residents. However, by considering the social identities of residents, human services professionals may devise interventions to help residents cope with the difficult experience of losing a loved one. The recreational and social infrastructure, including a variety of service professionals in the community, is a useful foundation on which to build such interventions. However, successful interventions are likely to be those that sustain or replenish satisfying relational connections while assisting residents with the identity work that accompanies the loss of valued social bonds.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article. Data collection was supported by a fund from the Sun City West Recreation Association.