
Abstract
Using data from the 2007 National Home and Hospice Care Survey, this study provides an update of nursing staff turnover at U.S. home health and hospice agencies and explores correlates of nursing staff turnover. Results show that the three-month turnover rates of registered nurses (RNs), licensed practice nurses (LPNs), home health aides (HHAs), and certified nursing assistants (CNAs) in 2007 were 10.2%, 14.3%, 12.5%, and 12.9%, respectively. A higher nurse staffing level reduced the odds of RN and HHA turnover; the availability of communication aids reduced the odds of LPN turnover. Moreover, among benefit programs, the provision of partial insurance for family reduced the odds of HHA turnover; dental or vision health insurance reduced the odds of RN turnover; mileage reimbursement or agency car reduced the odds of LPN turnover. The provision of a 401k plan and a paid-time-off program increased the odds of RN turnover. The study results suggest that high staffing levels and benefit programs (e.g., health insurance) may reduce the odds of experiencing nursing staff turnover. Initiatives to minimize nursing staff turnover should consider these factors.
Nursing staff turnover has several adverse consequences, including high costs (Jones 2004, 2005), lower staff morale, and compromised patient care (Castle and Engberg 2005; Cavanagh and Coffin 1992). Amid a continuing nursing shortage (Buerhaus, Staiger, and Auerbach 2003), retaining nurses has become an important issue for many health care organizations in the United States and other parts of the world (Oulton 2006). The nursing shortage in the United States could grow to more than one million nurses by 2020 (American Association of Colleges of Nursing 2011).
Among all health care settings, home health care agencies are projected to be the most strongly affected by the nursing shortage (Carter 2009). Moreover, home health care has become a more popular option for the chronically ill and those needing postacute care. For example, from 2000 to 2007 the total number of home health care patients increased by 7.4% (Centers for Disease Control and Prevention 2010), while the total expenditures on home health care increased by 93% (Hartman et al. 2009). Thus, it is important that home health care managers be able to identify typical factors of nurse turnover and design policies to retain nursing staff and improve the quality of care for clients. In 2007, about 69% of the home health patients were 65 years or older (National Center for Health Statistics 2011). Although much research has been done to examine nurse satisfaction, intent to stay, and retention in home health care providers (Ellenbecker 2004; Ellenbecker, Boylan, and Samia 2006; Ellenbecker and Byleckie 2005; Ellenbecker and Cushman 2001; Ellenbecker et al. 2007; Ellenbecker et al. 2008; Flynn 2003, 2005; O’Brien-Pallas, Duffield, and Hayes 2006; Smith-Stoner 2002, 2004), there is a dearth of national data on nursing staff turnover and its correlates in home health and hospice care agencies. Using the most recent data from a national survey, this study presents an update of nursing staff turnover and explores factors that are associated with nursing staff turnover in home health and hospice agencies.
Theoretical Framework
Several theoretical models have been developed to explain individual behaviors of nursing staff turnover (Alexander et al. 1998; Ellenbecker et al. 2008; Hinshaw and Atwood 1983; Liou 2009; Wagner 2010). In this study, we investigated organizational factors of nursing turnover in home health and hospice care agencies using Halbur’s (1983:383) structural model. In Halbur’s model, there are three factors that influence turnover: “the opportunity structure in which organization competes for workers, organizational structure in which individuals work, and control structure by which workers are rewarded for continued participation.” The opportunity structure refers to the organization’s exterior market, such as the community’s unemployment rate and the availability of alternative employment; the organizational structure is the particular setting where individuals work, including organizational characteristics such as ownership and size; and the control structure refers to the approaches by which individuals are rewarded for continued participation, including pay, benefits, promotion opportunities, and involvement in decision making. Halbur’s model of turnover was first tested in a study of nursing personnel in 122 nursing homes in one southern U.S. state. The study demonstrated that all three factors of nursing homes are important to explain nursing personnel turnover (Halbur 1983). Recently, Temple and colleagues applied this model to investigate organizational and control structure characteristics related to nursing assistant turnover in a sample of U.S. nursing homes (Temple, Dobbs, and Andel 2009).
This article focuses on the organizational structures and control structures contained in Halbur’s model, similar to Temple and colleagues’ (2009) study, and explores the association of organizational structures (measured by organizational characteristics) and control structures (measured by job characteristics) to the turnover of registered nurses (RNs), licensed practice nurses (LPNs), home health aides (HHAs), and certified nursing assistants (CNAs) in home health and hospice agencies.
Method
Data
Data for this analysis came from the National Home and Hospice Care Survey (NHHCS). NHHCS is a national probability sample survey that collects data on U.S. home health and hospice care agencies, including information related to their staff, services, and people they serve. NHHCS was conducted in 1992, 1993, 1994, 1996, 1998, 2000 and, most recently, in 2007. The 2007 NHHCS used a stratified two-stage probability sampling design and was conducted between August 2007 and February 2008. A sample of 1,545 agencies was selected, and 1,036 participated in the survey, for a response rate of 71% (Dwyer et al. 2010). The variables used in this analysis were collected as part of the 2007 NHHCS agency questionnaire and staffing questionnaire. The combined data set was downloaded from the NHHCS website (www.cdc.gov/nchs/nhhcs/nhhcs_questionnaires.htm).
Measures
Turnover rates
In the 2007 NHHCS, agencies were surveyed on the number of four types of nursing staff who left in the past 3 months: RNs, LPNs, HHAs, and CNAs, including both full- and part-time, but excluding contract workers. The reason for job termination included both voluntarily and involuntary terminations (retired, dismissed, resigned). To calculate the turnover rates for RNs, LPNs, HHAs, and CNAs, we first aggregated the number of RN, LPN, HHA, and CNA full-time equivalents (FTEs) in each agency to get the total number of nursing FTEs in the agency. Then, for each type of nursing staff, we calculated the turnover rate by dividing the number who left in the past 3 months by the aggregated total number of nursing staff FTEs in the agency. This measurement is consistent with a standard turnover rate definition in nursing homes (Castle 2006). In the study sample, the 3-month turnover rate among agencies for RNs ranged from 0% to 400%, for LPNs from 0% to 900%, for HHAs from 0% to 500%, and for CNAs from 0% to 800%. Because 54.4% of the agencies did not have RN turnover, 75.4% had no LPN turnover, 67.7% had no HHA turnover, and 68.2% had no CNA turnover, in multivariate analysis we measured turnover for each staff type as a binary measure: agencies with turnover (1) versus agencies without turnover (0).
Organizational characteristics (organizational structure variables)
We included the following organizational characteristics in this analysis: type of agency (home health agency, hospice agency, and dual agency), ownership (for-profit vs. nonprofit), chain affiliation (member of a chain vs. independent facility), agency director’s tenure (in months at the agency), agency size (the aggregated total FTEs of RNs, LPNs, HHAs, and CNAs, not including contract workers), and nurse staffing levels (the aggregated nursing staff FTEs divided by total current number of home health and/or hospice patients).
Job characteristics (control structure variables)
Following prior research on nursing staff turnover (Castle and Engberg 2006; Kash, Castle, and Phillips 2007; Temple et al. 2009), we included the following job characteristics available in the 2007 NHHCS in this analysis. Wage is the current entry-level hourly wage for an RN, LPN, HHA, or CNA at the agency. The provision of 16 benefit programs were assessed separately for the RNs/LPNs group and for the HHAs/CNAs group in the 2007 NHHCS, including health insurance (either full or partial), retirement benefits, paid time off, bonus, and tuition reimbursement. We combined the survey response for the provision of full health insurance for family members with the provision of full health insurance benefits for the employee only because very few facilities provided full health insurance for family members. All these benefit programs were binary measures (provided vs. not provided by the agency).
Other job characteristics included the use of an electronic medical record (EMR) system at the agency (yes–no; whether the agency uses a computerized patient medical record information in management of patients’ health care), the use of telemedicine (yes–no; whether the agency uses electronic communication and information technologies to provide or support clinical care at a distance), the presence of a staff or contract physician (yes–no), the availability of communication aid (yes–no; whether the agency used one or more of the following communication practices with patients, including interpretation services, translated material, and multilingual staff), and flexible scheduling/job sharing (yes–no; whether agency allowed flexible scheduling/job sharing). These variables were included to reflect the working environment characteristics. Prior research has shown working environment is an important factor for nursing turnover (Spetz and Adams 2006).
Statistical Analysis
Descriptive statistics were used to characterize home health and hospice agencies. Because the outcome variable in this study is binary (i.e., whether the agency had nursing staff turnover or not), we ran three separate multiple logistic regression models to estimate the association of organizational and job characteristics to RN, LPN, and HHA turnover, respectively. Because of missing values, the final sample size for the RN, LPN, and CNA turnover model was reduced to 876, 641, and 778 agencies, respectively, out of the total sample of 1,036 agencies. We did not estimate the model for CNA turnover because of the limited sample size (n = 123 agencies) as a result of missing values. Analysis was conducted using SAS version 9.2. The procedures SURVEYFREQ, SURVEYMEANS, and SURVEYLOGISTIC were used to account for the stratified sampling designs and associated sampling weights. We checked for multicollinearity among the independent variables before conducting multiple regression model analyses. We did not detect significant collinearity as all variance inflation factors were less than 2.5 (Allison 1999). We report the adjusted odds ratios (AORs) and 95% confidence intervals (CI) and note significance levels less than p = .05.
Results
As shown in Table 1, the 3-month turnover rates for RNs, LPNs, HHAs, and CNAs in U.S. home and hospice care agencies in 2007 were 10.16% (95% CI = 7.67–12.64), 14.32% (95% CI = 5.82–22.08), 12.51% (95% CI = 8.01–17.00), and 12.91% (95% CI = 5.83–20.00), respectively.
Descriptive Statistics.
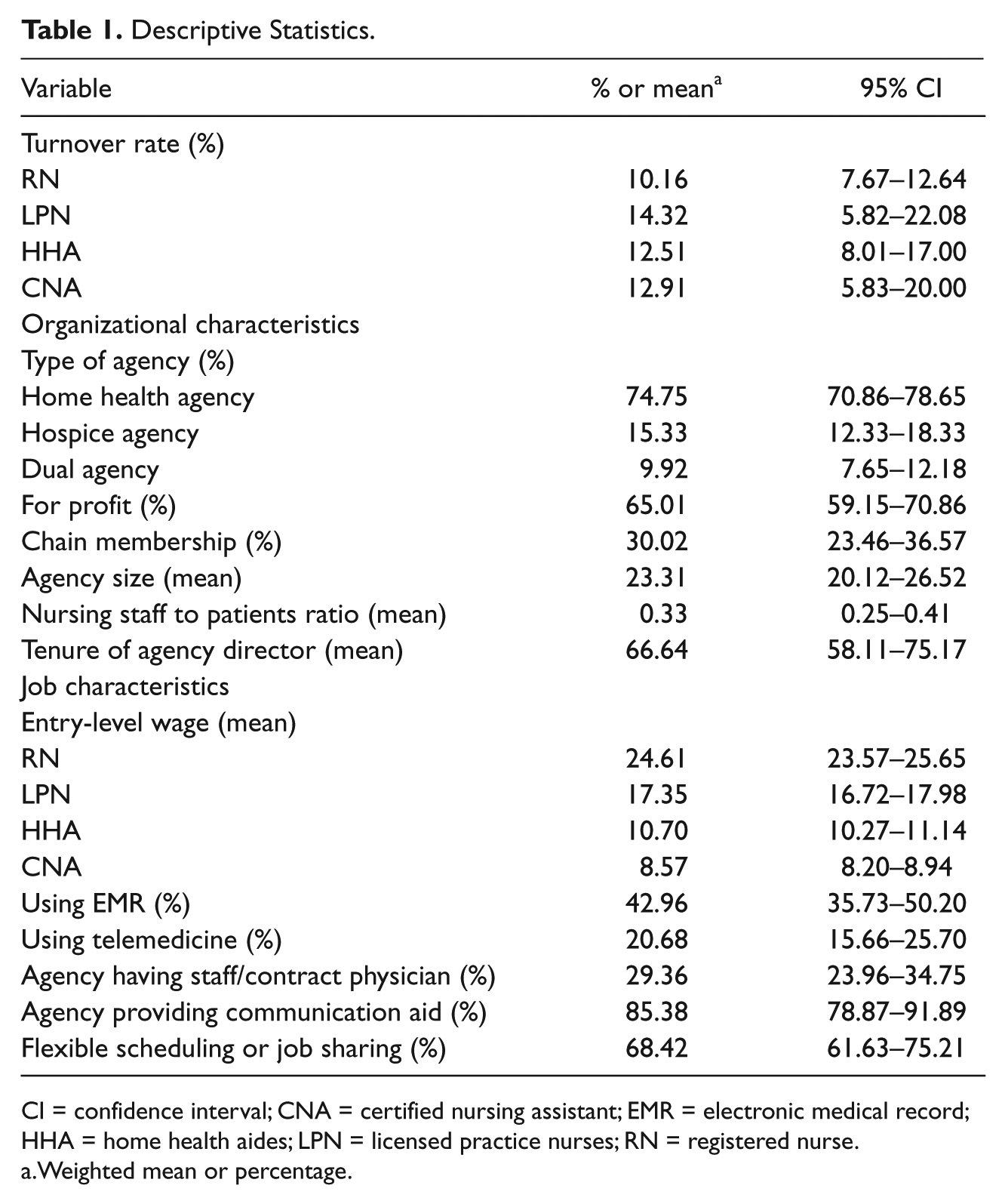
CI = confidence interval; CNA = certified nursing assistant; EMR = electronic medical record; HHA = home health aides; LPN = licensed practice nurses; RN = registered nurse.
Weighted mean or percentage.
In 2007, about 75% of the agencies were home health care only, 15% were hospice, and 10% were dual agencies. Of the agencies, 65% were for-profit, and 30% belonged to a chain. The average size was 23.31 FTEs per agency (ranging from 0 to 602). The average FTEs to patient ratio was 0.33. On average, a director’s tenure at the current agency was about 5.5 years (67 months; see Table 1).
The average entry-level hourly wages for RNs, LPNs, HHAs, and CNAs were $24.61, $17.35, $10.70, and $8.57, respectively. About 43.0% of the agencies used an EMR for patient health care, 20.7% used telemedicine, 85.4% provided communication or interpretation assistance, and 68.4% allowed flexible scheduling or job sharing (see Table 1).
Moreover, overall, in 2007, 43.9% (95% CI = 36.73–51.03) of U.S. home and hospice care agencies reported they experienced RN turnover in the past 3 months, 24.0% (95% CI = 16.45–31.47) had LPN turnover, 28.9% (95% CI = 22.04–35.72) had HHA turnover, and 36.6% (95% CI = 18.46–54.70) had CNA turnover.
The two most commonly provided benefit programs by home health and hospice agencies for both the RN/LPN group and the HHA/CNA group are paid vacation, 92.6% and 91.2%, respectively, and mileage reimbursement, 84.3% and 81.3%, respectively. The least frequently provided programs were provision of uniforms (10.7% and 12.6%) and full health insurance for the employee or family members (19.38% and 16.5%; see Table 2). On average, an RN/LPN was provided 8 benefit programs, whereas an HHA/CNA was provided 7 out of the 16 items (data not shown in the table).
Benefit Programs Provided for RNs/LPNs and HHAs/CNAs in Home Health and Hospice agencies.

Weighted percentage.
CI = confidence interval; CNA = certified nursing assistant; HHA = home health aides; LPN = licensed practice nurses; RN = registered nurse.
Three multiple regression model results are presented in Table 3. Agency size was associated with experiencing RN turnover (AOR = 1.03, 95% CI = 1.02–1.05), LPN turnover (AOR = 1.02, 95% CI = 1.01–1.03), and HHA turnover (AOR = 1.03, 95% CI = 1.02–1.05). Moreover, model I results show that agencies with a higher nurse staffing level (AOR = 0.44, 95% CI = 0.28–0.70) and those providing other health insurance (e.g., dental and vision) were less likely (AOR = 0.29, 95% CI 0.12–0.70) to have RN turnover. Counterintuitively, agencies providing a 401k benefit program (AOR = 4.12, 95% CI = 1.94–8.74) or other paid bonus incentives (AOR = 2.86, 95% CI = 1.53–5.36) were more likely to have RN turnover.
Multiple Logistic Regression Results of Factors Associated With Nursing Staff Turnover.
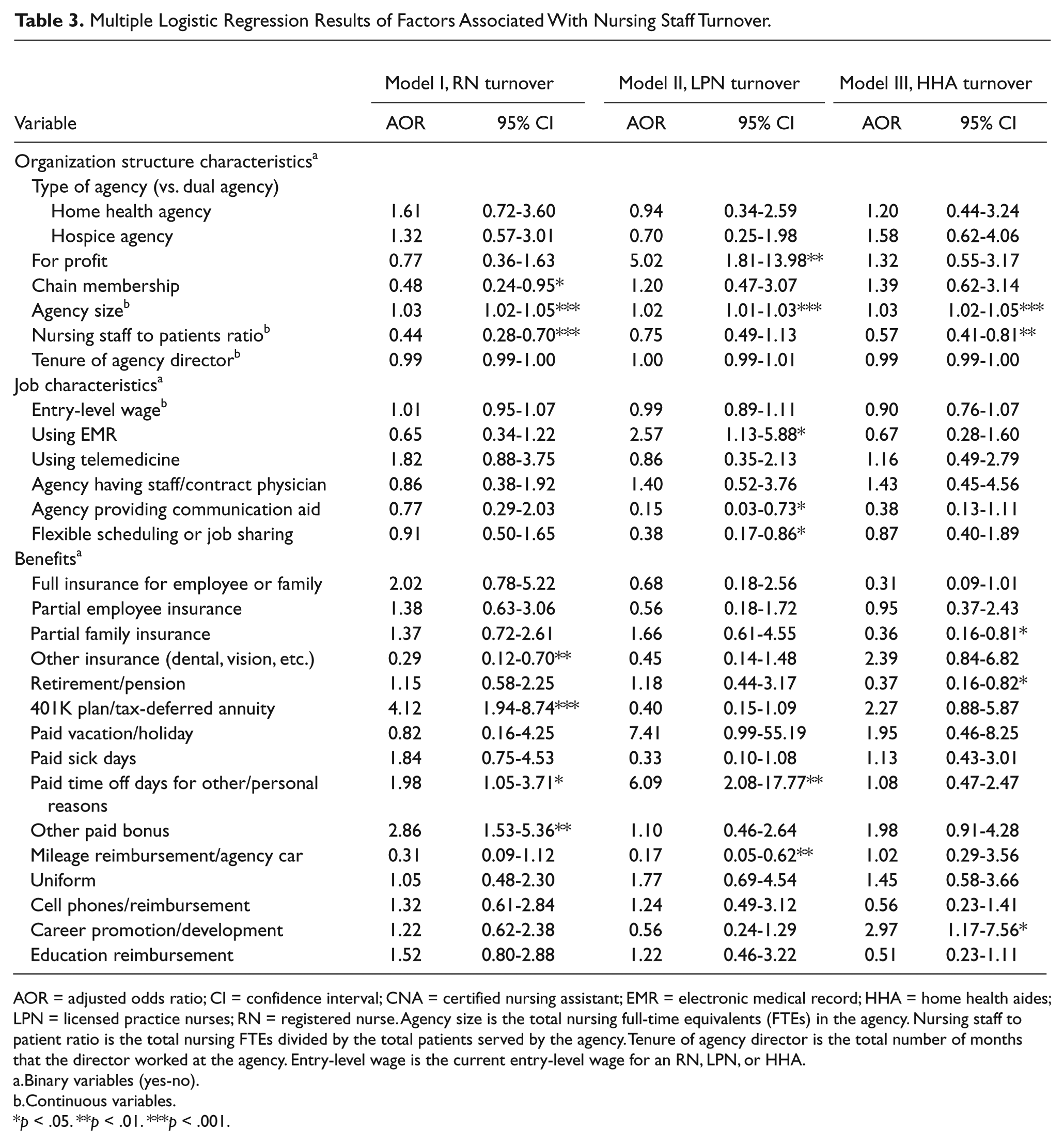
AOR = adjusted odds ratio; CI = confidence interval; CNA = certified nursing assistant; EMR = electronic medical record; HHA = home health aides; LPN = licensed practice nurses; RN = registered nurse. Agency size is the total nursing full-time equivalents (FTEs) in the agency. Nursing staff to patient ratio is the total nursing FTEs divided by the total patients served by the agency. Tenure of agency director is the total number of months that the director worked at the agency. Entry-level wage is the current entry-level wage for an RN, LPN, or HHA.
Binary variables (yes-no).
Continuous variables.
p < .05. **p < .01. ***p < .001.
Model II results show for-profit agencies (AOR = 5.02, 95% CI = 1.81–13.98) were more likely to experience LPN turnover, yet agencies providing communication aids (AOR = 0.15, 95% CI = 0.03–0.73), flexible scheduling or job sharing (AOR = 0.38, 95% CI = 0.17–0.86), and mileage reimbursement or an agency car (AOR = 0.17, 95% CI = 0.05–0.62) were less likely to have LPN turnover. Paradoxically, agencies using an EMR (AOR = 2.57, 95% CI = 1.13–5.88) and those providing paid time off for other or personal reasons (AOR = 6.09, 95% CI = 2.08–17.77) were more likely to have LPN turnover (see Table 3).
Last, the results of model III indicate that agencies with higher nurse staffing level (AOR = 0.57, 95% CI = 0.41–0.81) and those providing partial health insurance for family (AOR = 0.36, 95% CI = 0.16–0.81) were less likely to have HHA turnover. The provision of full health insurance for employee or family was marginally significant (AOR = 0.31, p = .058). In addition, agencies providing career promotion and development for HHAs (AOR = 2.97, 95% CI = 1.17–7.65) were more likely to have HHA turnover (Table 3).
Discussion
Using the 2007 NHHCS data, this study estimated the 3-month turnover rates of four types of nursing personnel in U.S. home health and hospice agencies and explored the correlates associated with each type of nursing staff turnover. The results of this study show that, in 2007, the 3-month turnover rates of LPNs (14.3%) and CNAs (12.9%) in U.S. home health and hospice care agencies were relatively higher than rates of turnover among HHAs (12.5%) and RNs (10.2%). Overall, this pattern is similar to that for nursing staff turnover in nursing homes, where the highest turnover rate is for nurse aides and the lowest is for RNs (American Health Care Association 2008; Castle 2006). Of note, we cannot partition these turnover rates into “beneficial turnover rates,” that is, turnover resulting from the weeding out of poor staff (i.e., termination by the agency), or “bad turnover rates” that may adversely influence factors such as quality of care. This is an important area for future research.
The results of this study show that agency size was the most consistent organizational characteristic associated with nursing staff turnover. That is, larger agencies were more likely to have turnover among RNs, LPNs, and HHAs. In addition, agency ownership (i.e., for-profit status) was a significant factor for experiencing LPN turnover, but was not significant for RN and HHA turnover. It is possible that large organizations are inherently a more difficult setting for nursing staff to establish kinship and commitment to the organization. In fact, we believe the organizational structure results of this national study are consistent with other research on nursing turnover (Banaszak-Holl and Hines 1996; Castle and Engberg 2006; Ellenbecker et al. 2008). For instance, a study of home health care nurses in six New England states shows that agency size and ownership affect nursing staff’s intent to stay and retention (Ellenbecker et al. 2008). Finally, the result that for-profit ownership is not significant for RN turnover (AOR = 0.77, p > .05) might be because of for-profit agencies employing fewer RNs. We are not able to determine why system affiliation is significant for RN turnover but not significant for LPN and HHA turnover.
Another important organizational characteristic associated with turnover is nurse staffing levels, as measured by the staff-to-patient ratio. A higher staff-to-patient ratio is associated with a lower likelihood of experiencing RN and HHA turnover. Since home health and hospice care is labor-intensive, a higher nurse staffing level would help to reduce workload. Prior research has identified that staffing levels are very important to nursing staff retention in home health care agencies (Flynn 2003). In nursing homes, higher nurse staffing levels have been found to be associated with lower NAs turnover (Castle and Engberg 2006; Donoghue and Castle 2007). Of note, accumulating research evidence suggests that increases in nurse staffing levels are associated with higher quality of care for patients in hospitals and nursing homes (Blegen et al. 2011; Centers for Medicare and Medicaid Services and U.S. Department of Health and Human Services 2001; Needleman et al. 2011). Yet during a period of nursing shortage, it may be prohibitively expensive to increase staffing levels. However, nurse turnover, in itself, has proven to be very costly because of the costs involved in searching for and training new employees (Jones 2005, 2008). Regarding other job characteristics, our results indicate that communication aids and flexible scheduling were associated with lower odds of having LPN turnover. The communication aids variable was also bordering on significance for HHAs (AOR = 0.38, p = .07). Thus, the availability of communication aids could be a viable strategy to help retain LPNs and HHAs, which is important because of their frontline role in delivering care to patients. Compared with RNs, LPNs and HHAs were interacting more often with patients. An earlier research study showed that home care nurses considered flexible work schedules, supportive administration, and participating in decision making as important to job satisfaction and professional work (Flynn and Deatrick 2003; Smith-Stoner 2004). Yet the results of this study show that agencies using an EMR were more likely to experience LPN turnover. And it is interesting that although not significant, the odds ratios for RN turnover (AOR = 0.65) and HHA turnover (AOR = 0.67) are actually in the opposite direction. One possible explanation for this finding is that it could be a challenge for LPNs to acquire the computer skills to use an EMR, and they might be more often asked to impute patients’ data into computers than RNs and HHAs. Some of them may prefer paper-based documentation. Nonetheless, agencies should ensure that nursing staff have adequate job training to reduce work-related frustration and turnover.
For benefit programs, our study results underscore the importance of providing benefit programs. First, the provision of other health insurance (e.g., vision and dental) reduced the likelihood of experiencing RN turnover, though it is not significant among LPNs and HHAs. Second, the provision of partial health insurance for family members and full insurance for the employee/family (marginally significant, p = .06) and retirement benefits reduced the likelihood of turnover among HHAs, but was not significant for RN and LPN turnover. Thus, not all health insurance benefit programs were significant across different types nursing staff. Our interpretation is that RNs may already have purchased general health insurance through their family plans, and thus they value supplemental insurance like vision or dental care, whereas HHAs may not have general health insurance through family plans, and thus the provision of this benefit would reduce the odds of HHA turnover. Overall, our findings are consistent with prior findings that medical insurance programs are important factors in nursing turnover (Anthony and Milone-Nuzzo 2005; Spetz and Adams 2006; Temple et al. 2009). Third, the provision of mileage reimbursement or an agency car reduced the likelihood of LPN turnover. Similar findings were reported in an earlier study of Connecticut home care nurses, where nurses considered dealing with inclement weather and wear on their personal automobile as the reasons to change jobs (Anthony and Milone-Nuzzo 2005).
It is interesting that our results of a few benefit program characteristics are counterintuitive. For example, provision of 40lk plan, other paid bonus, and paid time off increased the likelihood of RN turnover; paid time off increased the likelihood of LPN turnover; career promotion and development increased the likelihood of HHA turnover. However, prior research evidence shows that a paid-time-off benefit has been found to contribute to nurse satisfaction (Ellenbecker et al. 2008), and career development and lifelong learning activities have been shown to promote job satisfaction and increase the retention of nurses (Yoder 1995). It is not clear why these results are not consistent with prior findings. We suspect that it might be other organizational factors, such as working environment or organizational culture (Smith-Stoner and Markley 2007; Spetz and Adams 2006), that may be confounding our analyses; unfortunately, these variables are not available for evaluation in this study. This survey was administered during a period (2007–2008) when the stock market experienced considerable flux, and this could have dampen enthusiasm for 401k plans. We did additional analyses using existing variables to explicate these results. For example, our additional analyses show that those agencies that provided 401k plans offered a lower entry-level wage for RNs (p = .06) and LPNs (p = .02). More research is needed in this area. Last, our explanation for the positive association of career promotion or development with HHAs turnover is that a career promotion program, such as workshops, conferences, and certificate exams for HHAs, could help them to improve their competence and move up to higher positions in the organization or find other employment situations (e.g., hospital-based employment).
In summary, our study findings indicate that there is no one-size-fits-all benefits package. Some benefit programs might be effective for RNs, LPNs, or HHAs but not effective for all of them. Thus, effective benefit designs should accommodate the different demands and needs of different nursing staff.
Several limitations of this study should be noted. First, we did not include local market employment (i.e., the opportunity structure) and other job characteristics of turnover in our analyses, such as the work environment and patient acuity because of data unavailability. Second, the number of nursing staff who left was reported by agency staff and could be subject to reporting bias. Third, this study did not include characteristics of individual nurses, such as job satisfaction, tenure of service at the agency, or their particular job performance. Fourth, our study is a cross-sectional analysis, so no causality can be inferred. Fifth, we did not present the results separately for home health care and hospice care agencies. These results are available from the authors. The stratified analysis results for home health care agencies and hospice care agencies are similar to the results we presented above, except for minor differences with respect to HHA turnover.
Conclusion
There are philosophical differences that can exist in home health care and in hospice care that could influence nursing staff turnover. For example, hospice nursing staff may find greater fulfillment in their work providing end-of-life care, which could make them more likely to remain on the job longer than those employed only in home health care. On the other hand, hospice nursing staff may become burned out by the deaths of patients and the subsequent disenfranchised grief that they experience on the job (Hunnibell et al. 2008; Perry 2009). Yet in sensitivity analyses, few differences in turnover were identified between home health and hospice care agencies. Using the 2007 NHHCS data, this study presents the first national estimate of nursing staff turnover in home health and hospice agencies and explores factors that are associated with nursing staff turnover. In an era of increasing demands for home health care and a continuing nursing shortage, home health and hospice administrators and managers should enact evidence-based strategies to minimize turnover and enhance retention. Our study results demonstrate that nurse staffing levels, health insurance, and work-support programs for nurses are important factors for nursing staff turnover in home health and hospice agencies. These factors are modifiable by agencies. Initiatives to reduce nursing staff turnover should consider targeting these factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.