
Abstract
Falling is a major health-related risk among older adults due to injuries, disability, and even death. Although physical activity (PA) can prevent falls, most older adults are inactive due to limited motivation. The purpose was to examine a motivational framework whereby the stages of change (SOC) and PA mediated the relations between the theory of planned behavior constructs and falls risks among 172 diverse older adults (M age = 72.36). The participants were assessed using standardized scales. Based on the path analysis, the hypothesized framework fit the sample data. The SOC and perceived control had significant path coefficients for PA (.48 and .43, respectively), and PA was linked to falls risks (−.54). Subjective norm was mostly associated with the SOC followed by attitude and perceived control. The variance explained in the SOC, PA, and falls risks were 28%, 59%, and 29%, respectively. Health promoters can use the proposed framework to promote PA and decrease falls risk.
Introduction
One of the most severe, health-related risks for older adults is falling and its related consequences, such as nonfatal and fatal injuries, limited independence in activities of daily living, hospitalization, disability, and psychosocial conditions, such as postfall anxiety syndrome and fear of falling (Centers for Disease Control and Prevention [CDC], 2010; Sterling, O'Connor, & Bonadies, 2001; Tinetti, 1994; Tinetti & Williams, 1997).
Physical activity (PA) is one important way to prevent falls, increase independence in activities of daily living, reduce stress and depression, and improve quality of life among older adults (American College of Sports Medicine, 1998; Blake, Mo, Malik, & Thomas, 2009; Cairney, Faulkner, Veldhuizen, & Wade, 2009; Freiberger, Menz, Abu-Omar, & Rütten, 2007; Morey et al., 2008). Although a major focus of the article is on the effects of PA on falls risks, it is important to report other important predictors of falls risks among older adults. There are intrinsic (health history and biological factors) and extrinsic falls risk factors. Intrinsic falls risk factors include gender, age, race/ethnicity, medical conditions (e.g., cognitive and psychological impairments), physical fitness and function, and history of falls (Campbell, Borrie, & Spears, 1989; Tinetti, Speechley, & Ginter, 1988). Extrinsic falls risk factors include substance abuse, environmental factors (such as difficulty to navigate one’s home due to cluttered setting), medication types, number of medications (the higher the number of medications the higher the falls risk), and adverse medication effects (e.g., sense of dizziness and loss of balance; Cumming, 1998; Leipzig, Cumming, & Tinetti, 1999; Ray, Griffin, & Shorr, 1990; Tinetti et al., 1994). Although to our knowledge there are no studies differentiating the importance of extrinsic and intrinsic falls-risk factors, some extrinsic (e.g., environmental hazards) and intrinsic falls-risk factors (e.g., physical fitness and function) can be decreased or eliminated via health promotion programs, such as increased PA participation (Fabre, Ellis, Kosma, & Wood, 2010).
Based on the American College of Sports Medicine guidelines (Haskell et al., 2007), older adults need to exercise 5 days/week at moderate levels of intensity for 30 min/day or 3 days/week at vigorous levels of intensity for 20 min/day. Although the benefits of PA for older adults have been well documented, the Federal Interagency Forum on Aging-Related Statistics (2008) reported that in 2007–2008 only 22% of people over 65 years old were regularly active. In particular, only 25% of those between 65 and 74 years old and 11% of those over 85 years of age exercised regularly. Additionally, one of the main goals of the United States Department of Health and Human Services (2000) is to identify ways to increase the number of older adults who participate in regular exercise levels of moderate or higher intensity by 2020 (Healthy People, 2020).
One of the reasons for the high inactivity levels among older adults is limited motivation; therefore, identifying theory-based PA motivational strategies for health and wellness is of paramount importance (Grodesky, Kosma, & Solmon, 2006). However, PA behavior is a complex phenomenon and cannot be sufficiently explained using only one theory. It is rather recommended to use integrative theoretical frameworks, such as one derived from the integration of the stages of change (SOC) in the transtheoretical model (TTM; Prochaska & DiClemente, 1983) and the theory of planned behavior (TPB; Ajzen, 1991; Grodesky et al., 2006; Kosma, Ellis, Cardinal, Bauer, & McCubbin, 2007).
Advances in the SOC
With regard to PA, five SOC have been primarily studied: the precontemplation, contemplation, preparation, action, and maintenance stages (Reed, Velicer, Prochaska, Rossi, & Marcus, 1997). Precontemplators are not active and they do not intend to be active in the next 6 months. In the contemplation stage, individuals are also not active, but they intend to be active in the next 6 months. In preparation, people are inactive or irregularly active (e.g., once or twice per month), but they have the intention to be active within 30 days. In action, people are regularly engaging in certain forms of physical activities for less than 6 months. Finally, in the maintenance stage, people are participating in regular PA for more than 6 months (Kosma, Cardinal, & McCubbin, 2004; Reed et al., 1997).
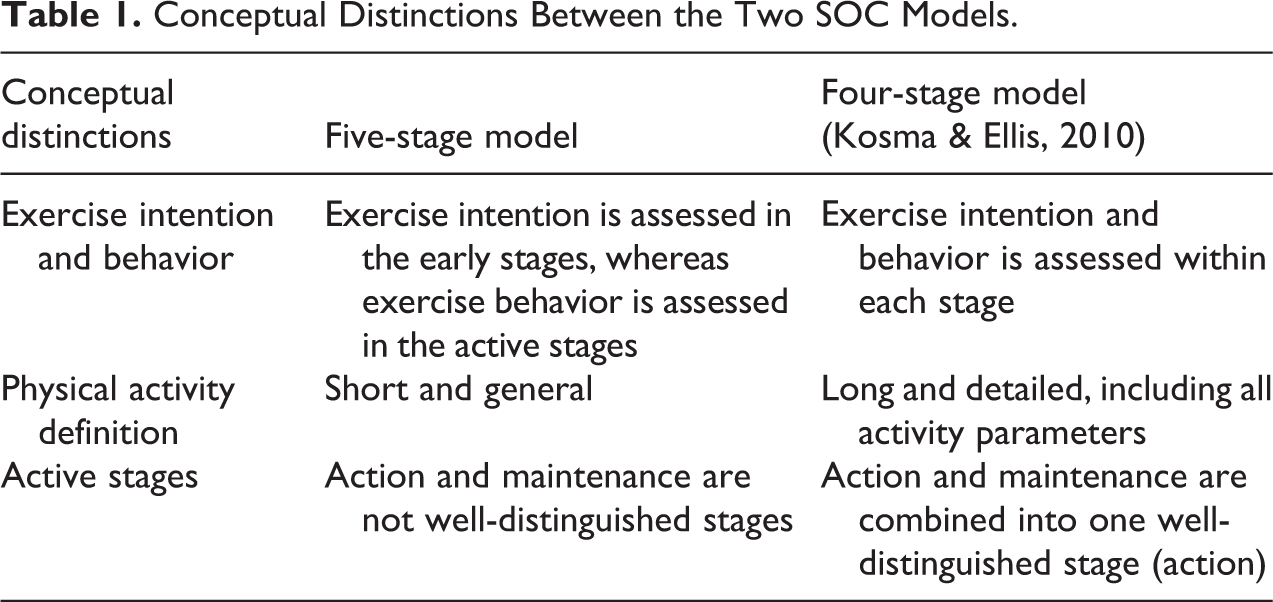
Although the aforementioned, five SOC have been used extensively in the PA literature, they have several conceptual drawbacks, such as lack of the measure of PA intention and behavior within each stage, brief and general exercise description, and limited distinction of the two active stages (action and maintenance; Godin, Lambert, Owen, Nolin, & Prud’homme, 2004; Kosma, 2007; Kosma & Ellis, 2010; Kosma, Ellis Gardner, Cardinal, Bauer, & McCubbin, 2006; Reed et al., 1997). Given the aforementioned, conceptual limitations, Kosma and Ellis (2010) developed and validated an improved SOC scale, which was applied to adults with physical disabilities (Kosma & Ellis, 2010) and was recently used among also older adults (Kim & Kosma, 2010). Instead of five SOC, this scale consists of four SOC, precontemplation, contemplation, preparation, and action (combination of action and maintenance into one stage). PA intention and behavior are assessed within each stage and exercise includes a long and detailed definition of PA (Kosma, 2007; Reed et al., 1997). The exercise definition is based on the American College of Sports Medicine guidelines by Haskell and colleagues (2007) and it includes all activity parameters, providing activity examples specific to the population of interest, such as walking with or without assistive devices, wheeling, dancing, and swimming. In this study, the improved SOC scale by Kosma and Ellis (2010) was used. In Table 1, the differences in the two SOC models are presented.
Conceptual Distinctions Between the Two SOC Models.
The Theory of Planned Behavior and Older Adults
The TPB (Ajzen, 1991) is a social cognitive theory and assumes that individuals will evaluate the consequences of a behavior and their attitudes toward those consequences before they engage in the behavior (Ajzen, 1991). Below, the TPB will be described in the domain of exercise behavior. The first main construct of TPB is intention, which reflects one’s motivation and willingness to participate in exercise behavior. In other words, it is hypothesized that people will be active if they have strong positive intentions toward the behavior, and thus it is a direct determinant of the behavior. Intention in turn is affected by attitude, subjective norm, and perceived behavioral control. Attitude reflects the perceived positive or negative consequences of PA, such as PA will improve one’s health or it will take time away from family and friends. Subjective norm is perceived social pressure to be active and it reflects two forms: injunctive subjective norm (how significant others’ perceptions about one’s exercise affect one’s exercise behavior) and descriptive norm (how significant others’ exercise behavior affect one’s exercise participation). Perceived behavioral control is a combination of one’s confidence to be active (self-efficacy) and perceived control over the behavior (controllability; Ajzen, 2002). Beyond the indirect effects of perceived behavioral control on PA via intention, perceived behavioral control has also a direct effect on intention (Ajzen, 1991).
The TPB has been successfully applied in the PA area among mainly healthy adults (Symons Downs & Hausenblas, 2005) and to a lesser extent among understudied populations, such as older adults (e.g., Wankel, Mummery, Stephens, & Craig, 1994) and adults with physical disabilities (e.g., Ellis, Kosma, Cardinal, Bauer, & McCubbin, 2009). Based on the TPB studies among healthy adults, the most important predictor of PA is intention and to a lesser extent perceived behavior control. Additionally, the most important predictors of intention tend to be attitude and perceived behavioral control, whereas subjective norm is not a strong predictor of intention. Similar findings have been reported among adults with physical disabilities (Ellis et al., 2009).
The results of the limited TPB studies among older adults are somewhat different from the aforementioned findings. Although intention still remains the major predictor of exercise behavior, with increased age subjective norm and perceived behavioral control tend to be more important predictors of intention than attitude (Dean, Farrell, Kelley, Taylor, & Rhodes, 2006; Wankel et al., 1994). Specifically, in the study by Dean and colleagues, subjective norm was the most important determinant of intention to participate in strength training exercises followed by perceived behavioral control among older adults. In the study by Wankel and colleagues, perceived behavioral control was the most important predictor of intention to engage in vigorous exercise behavior followed by subjective norm and attitude. In both aforementioned studies, multiple regressions were used to analyze the data and some of the psychosocial measures used were either indirect (e.g., subjective norm in Wankel et al study) or they did not comprise the recent recommendations by Ajzen (2006), assessing for example both injunctive and descriptive subjective norm. Additionally, the studies referred to strength training and vigorous exercise rather than leisure-time PA participation, which was the focus of this study.
An Expanded Framework for PA and Falls Risks
In their 6-month prospective study, Kosma et al. (2007) compared the TPB with an integrative framework (TPB/SOC) among adults with physical disabilities. In the integrative framework, the construct of intention in the TPB was replaced by the SOC in the TTM, which reflects both intention and behavior (Kosma, 2007; Rosen, 2000). This replacement took place because PA behavior is a complex behavior and it is hypothesized to be best predicted by both one’s exercise cognitions (e.g., intention) and exercise behavior (Ouellette & Wood, 1998).
The aforementioned hypothesis was supported in the study of Kosma et al. (2007), in that the integrative framework (TPB/SOC) was a stronger predictor of PA than the TPB alone. Additionally, the path analyses showed that the most important predictors of intention were attitude followed by perceived behavioral control in both the TPB and the TPB/SOC models. This integrative framework (Kosma et al., 2007) was expanded in another study, whereby the model predicted successfully not only future PA but also future health-related quality of life (physical and mental health) among adults with physical disabilities (Kosma, Ellis, Cardinal, Bauer, & McCubbin, 2009).
Purpose and Hypotheses
The purpose of the current study was to further expand the aforementioned, TPB/SOC integrative framework, and examine whether the TPB/SOC model affected not only PA but also falls risks among diverse older adults. To our knowledge, no other studies so far have linked the TPB or SOC to falls risks either directly or indirectly via exercise. In this expanded framework, the new, improved SOC scale of Kosma and Ellis (2010) was used and the recent recommendations by Ajzen (2006) were followed for the assessment of the TPB constructs. Additionally, a path analysis was conducted to test the model rather than regressions.
It was hypothesized that PA would affect falls risks and that both the SOC and the perceived behavioral control would affect PA. Given that this integrative framework has not been applied to older adults, it is difficult to ascertain a hypothesis about the most important determinants of the SOC. Regardless, following the results of the limited number of TPB-based studies among older adults (e.g., Dean et al., 2006 and Wankel et al., 1994), subjective norm was expected to be a stronger determinant of the SOC than attitude and perceived behavioral control, which were expected to also be associated with the SOC (see e.g. Kosma et al., 2007).
Method
Design and Procedures
This was a cross-sectional study, which was approved by the author’s Institutional Review Board. Informed consent was obtained from the participants. Data collection lasted 1 year and it took place in community settings in a Southeastern state. Using interviews, participants completed self-report, standardized measures of the TPB constructs (attitude, subjective norm, and perceived behavioral control), the SOC, and PA. Additionally, physical tests and interviews were performed to assess risk of falls. Finally, participants self-reported their age, race, gender, education level, and income level.
Participants were recruited through study advertisements and referrals made by the directors of community centers in a Southeastern state, such as Council of Aging Offices, retirement centers, and churches. Only ambulatory individuals without any known cognitive limitations that obstructed their understanding of the questionnaires were allowed to participate in the study. During data collection, participants were screened for their ability to understand the questionnaires based on their medical conditions, which were communicated with the participants via interviews when they provided a list of their current medications for the falls-risk screening. Lack of cognitive impairments was a requirement to participate in the study. Additionally, participants’ understanding of the consent form was another way to determine study eligibility. The consent form was personally discussed with the participants, who were encouraged to ask questions and reiterate the study purpose in order to ensure their understanding of the form. Finally, the study’s inclusion criteria and procedures were indicated in the advertised study flyer and consent form. Participants were not reimbursed for study participation.
Measures
Stages of change
An ordinal, modified, stages-of-change algorithm was used to assess participants’ SOC (Kosma & Ellis, 2010). The scale includes four stages, in that precontemplators are inactive or irregularly active and they do not intend to be regularly active within the next 6 months. Contemplators are inactive or irregularly active and they intend to be regularly active within the next 6 months. The PA pattern of preparators is the same as the one of the two former SOC, but preparators intend to be regularly active within the next month. Finally, the action and maintenance stages were combined into one stage, action, whereby people are regularly active and they intend to continue this behavior in the future. The scale’s content and construct validity (e.g., expected relations among the SOC, PA, and the TTM constructs) was supported among adults with physical disabilities (Kosma & Ellis, 2010), and was recently used among older adults (Kim & Kosma, 2010).
Attitude
A 7-point, 8-item Likert-type scale was used to assess attitude. The responses to the statement “for me to participate in regular physical activity is” reflect four adjective pairs of instrumental attitude (i.e., useless–useful, harmful–beneficial, foolish–wise, bad–good) and four adjective pairs of affective attitude (boring–interesting, unpleasant–pleasant, unenjoyable– enjoyable, stressful–relaxing). An average score was used to assess attitude. This scale is based on the renewed guidelines of Ajzen (2006), and it was successfully applied to adults with physical disabilities (Ellis et al., 2009; Kosma et al., 2007). In this study, the internal consistency of the scale was high (α = .91).
Self-efficacy and perceived control
Two questions on a 7-point Likert-type scale were used to assess self-efficacy: (a) “if I wanted to, I could easily participate in regular physical activity (1 = definitely false, 7 = definitely true)” and (b) “for me to participate in regular physical activity is (1 = impossible, 7 = possible).” Two items on a 7-point Likert-type scale were also used to assess perceived control: (a) “how much control do you have over participating in regular physical activity? (1 = no control, 7 = complete control),” and (b) “it is mostly up to me whether or not I participate in regular physical activity (1 = strongly disagree, 7 = strongly agree).” A mean score was used to assess perceived behavioral control (i.e., self-efficacy and perceived control). This scale is based on the updated guidelines of Ajzen (2006), and a similar version of the scale was used among adults with physical disabilities (Ellis et al., 2009; Kosma et al., 2007). In this study, the scale’s internal consistency was acceptable (α = .82).
Subjective norm
A 6-item, 7-point Likert-type scale was used to assess injunctive and descriptive subjective norm. The 3 items of injunctive subjective norm were the following: (a) “most people who are important to me think (1 = I should not, 7 = I should) participate in regular physical activity,” (b) “the people in my life whose opinion I value (1 = disapprove, 7 = approve) of my participating in regular physical activity,” and (c) “it is expected of me that I participate in regular physical activity (1 = strongly disagree, 7 = strongly agree).” The 3 items of descriptive subjective norm are the following: (a) “most people who are important to me participate in regular physical activity (1 = completely false, 7 = completely true),” (b) “the people in my life whose opinion I value (1 = do not participate, 7 = participate) in regular physical activity,” and (c) “many people like me participate in regular physical activity (1 = strongly disagree, 7 = strongly agree).” A mean score of the aforementioned items was used to assess subjective norm. Again, this measure is based on the updated guidelines of Ajzen (2006), and a similar version of the scale was used among adults with physical disabilities (Ellis et al., 2009; Kosma et al., 2007). The scale’s internal consistency in this study was acceptable (α = .80).
Physical activity
PA was measured using the Physical Activity Scale for the Elderly (PASE; Washburn, Smith, Jette, & Janney, 1993). PASE assesses the number of days per week and the average hours per day older adults participate in activities of different intensity levels, such as leisure, recreational, sport, household, and occupational activities. A composite scale score is used, which is the product of activity time and the respective weights (Metabolic (MET) values) for each activity. The scale developers reported PASE scores ranging between 0 and 360. They also supported the scale’s construct validity by exhibiting positive relations among PASE, grip and leg strength, and a negative correlation with the effect of disease on activities of daily living. In their study, the scale’s test–retest reliability was acceptable (r = .84), and its internal consistency was about the same as the one in the current study (α s = .69 and .65, respectively).
Falls risks
Falls risks were assessed using the Comprehensive Falls Risk Screening Instrument (CFRSI; Fabre et al., 2010). The CFRSI encompasses the most common falls-risk subscales identified by the American Geriatrics Society (2001) and it was recently validated among ethnically and economically diverse older adults in Southeast LA (Fabre et al., 2010), which comprises the study’s population as well. The CFRSI was significantly related to physical activity (PASE), health-related quality of life, and physical function, supporting its construct validity. The five falls-risk domains/subscales of the CFRSI are falls history (e.g., past falling status, walking ability, and arthritis), physical functioning (mobility/balance), medications, vision, and environment (e.g., easy navigation of one’s home). The raw scores of the subscales are converted into continuous scores ranging between 0 and 100 with the higher scores indicating higher falls risks. The scores can also be interpreted as percentages because they are standardized on a 100-point scale. The percentages are compared to maximum falls risk. The average score of the subscales was used to assess total falls risks.
Statistical Analyses
Using SPSS (version 17.0), descriptive statistics and pairwise correlations were performed to report participants’ characteristics and variable relations, respectively. A path analysis was performed using LISREL (version 8.54) in order to test the hypothesized model (i.e., the mediating effects of the SOC and PA on falls risks). Path analysis belongs to the family tree of structural equation modeling, whereby path coefficients are used to determine predictive relations. It represents an observed-variable regression model where some variables are independent in some parts of the model and dependent in others. In this way, mediator and outcome effects can be simultaneously tested after taking into account disturbance (unexplained) variance in the endogenous (dependent) variables (Kline, 2005). In other words, path analysis has two major advantages over multiple regression analysis: (a) simultaneous examination of all parameter estimates and (b) consideration of disturbance variance in the endogenous variables (Kline, 2005).
Goodness-of-fit statistics (i.e., indices of fit) are used to determine the fit of the hypothesized model to the sample model. The χ2 statistic examines the goodness of fit of the sample matrix to the hypothesized model. A significant χ2 value indicates model misfit. However, the χ2 value can be affected by sample size and high variance, and thus it is considered a weak index of model fit (West, Finch, & Curran, 1995). Instead, the ratio of χ2/df is recommended to be used, among other fit indices that are described below. When the values of the χ2/df ratio are equal to or less than 3.0 the model is considered to have a good fit (MacCallum, Browne, & Sugawara, 1996).
The root mean square error of approximation (RMSEA) represents the amount of error when estimating the hypothesized matrix from the sample matrix (Byrne, 1998). Values between .05 and .08 indicate a good fit (MacCallum et al., 1996). The goodness-of-fit index (GFI) determines the amount of variance/covariance explained by the sample model. The comparative fit index (CFI) and normed fit index (NFI) compare the sample model to an independence model (i.e., a model of no relations). The values of these indices can range from 0 to 1 with values greater than .90 indicating a good fit (Byrne, 1998). The standardized root mean square residual (SRMR) represents the standardized, average residual value when comparing the hypothesized model to the sample model (Byrne, 1998). Values less than .10 indicate a good fit (Kline, 2005).
Results
Participants
Study participants' (n = 172) average age was 72.36 ± 8.44 years and most of them were women (n = 119). Participants’ race was almost equally split between Blacks (n = 93) and Whites (n = 77). Their income levels varied, whereby 62.6% of the reported income levels (n = 123) were below $20,000/year and the remaining income levels (37.4%) were $20,000/year or higher. Their education levels also varied, whereby 50% (n = 85) of them had a high school/general equivalency diploma or less and 47.1% (n = 91) had some college degree or higher. Participants’ distribution across the SOC was as follows: precontemplation = 23, contemplation = 18, preparation = 18 and action = 113. In Table 2, detailed information about participants’ characteristics is reported.
Description of the Participants.
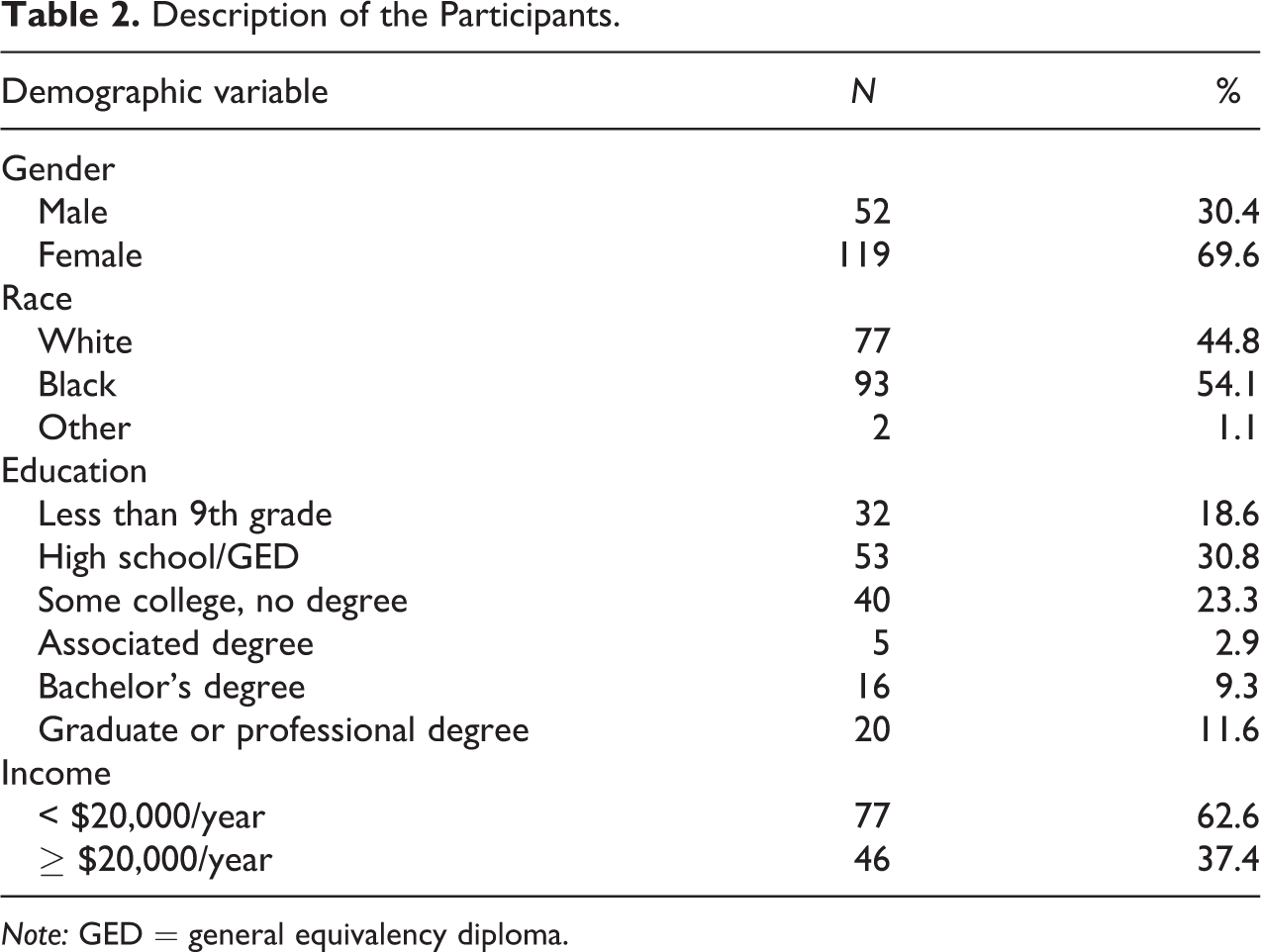
Note: GED = general equivalency diploma.
Variable Correlations and Descriptive Statistics
The correlation coefficients of the variables together with their Means and SDs are shown in Table 3. PA was correlated significantly with the studied variables and its highest correlation was with falls risks (r = −.47), whereby the higher the exercise levels the less the risk of falls. Additionally, participants had positive attitudes toward exercise, they were somewhat active, and their average risk of falls was below 50% of maximal risk.
Pearson Correlations, Means, and SD of Continuous Study Variables.

Note: ** p < .01. * p < .05.
aVariable study range: physical activity (MET-hrs./day): .00–313.92; falls risk: 9.29–62.40; attitude: 2.38–7; subjective norm: 2.17–7; and perceived behavioral control range: 2.25–7.
Expanded, Conceptual Framework
Based on the path analysis, the hypothesized, integrative framework overall fit the sample data well: RMSEA < .01, GFI = 1.0, NFI = 1.0, CFI = 1.0, SRMR = .08 (see Figure 1). Although the model’s χ2 value was statistically significant (χ2 = 19.45, p = .003), the ratio of χ2/df approached a good fit (19.45/6 = 3.24 ≈ 3; MacCallum et al., 1996).
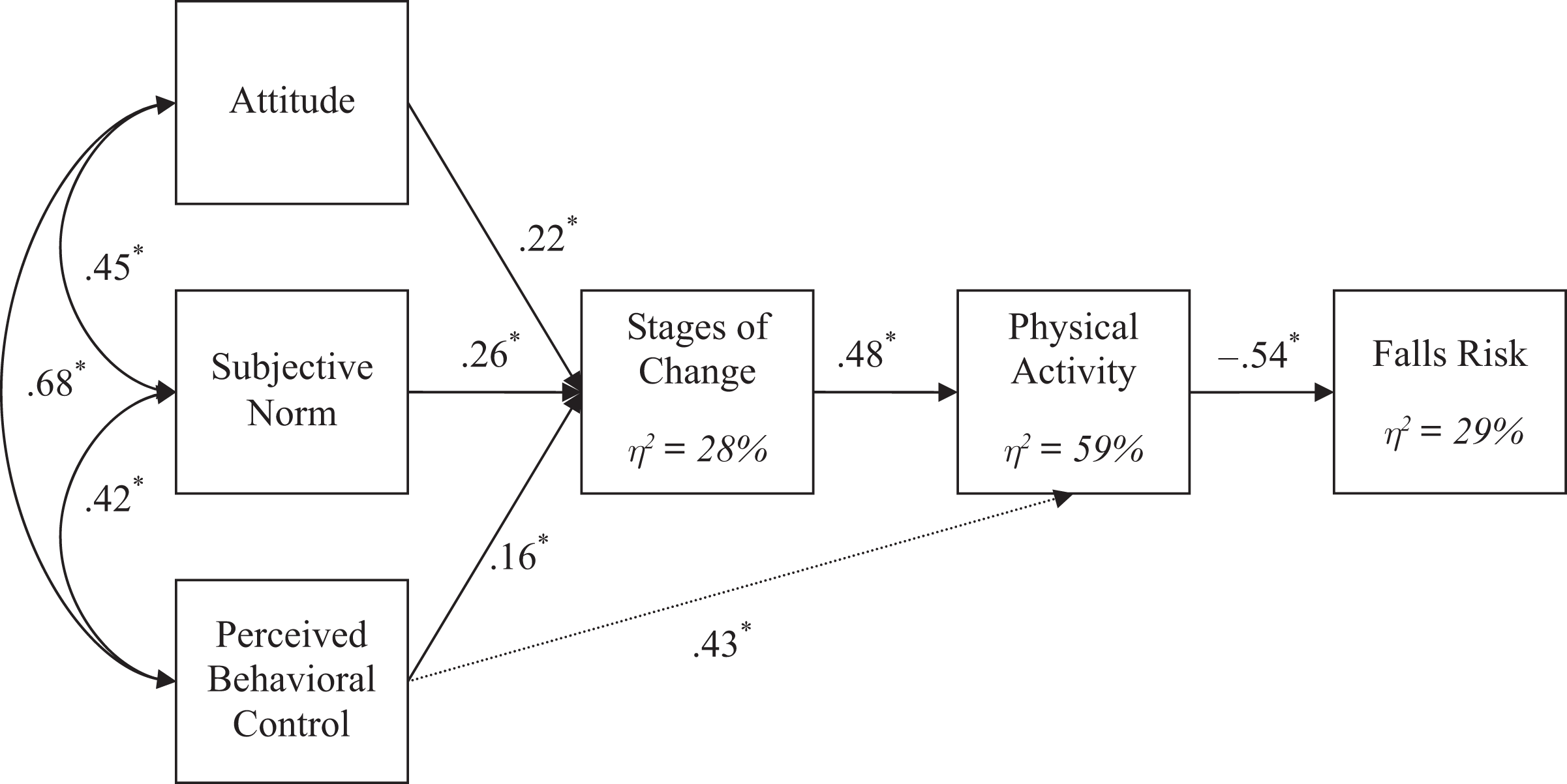
Predictors of physical activity and falls risks within an expanded, conceptual framework, * p < .05.
All path coefficients were statistically significant at p < .05 (see Figure 1). Standardized path coefficients with values less than .10 are considered small, whereas those with values around .30 and .50 or higher are considered medium and large, respectively (Cohen, 1988). The SOC and perceived behavioral control had medium to large direct positive effects (path coefficients) on PA (βs = .48 and .43, respectively). PA was significantly associated with lower falls risks (β = −.54 = large effect). Based on the values of the path coefficients, subjective norm had the strongest medium effect on the SOC (γ = .26) followed by the small to medium effects of attitude (γ = .22) and perceived behavioral control (γ = .16). The variance explained in the SOC, PA, and falls risks by the model were 28%, 59%, and 29%, respectively.
Discussion
The purpose of the study was to test an expanded, integrative framework by Kosma et al. (2007) whereby the SOC and PA mediated the relations between the TPB constructs and falls risks among diverse older adults. Based on the findings, the study hypotheses were supported. The hypothesized model fit the sample data well and explained moderate to high variances in the SOC, PA, and falls risks.
As expected, subjective norm was the most important determinant of the SOC followed by attitude and perceived behavioral control. Similarly, in the study by Dean and colleagues (2006), subjective norm was the most important determinant of older adults’ intention to participate in strength training activities. Contrary to these findings, subjective norm tends to be a weak predictor of exercise intention among healthy adults (Symons Downs & Hausenblas, 2005) and adults with physical disabilities (Ellis et al., 2009). Similarly, subjective norm tends to be a weak predictor of the SOC for exercise among adults with physical disabilities (Kosma et al., 2007). It seems that for older adults perceived social pressure to be active is an important determinant of their behavior and it may be linked to the increased awareness of the ameliorating effects of exercise on health risks associated with the aging process. This finding may also indicate the underlying need of older adults to exercise in highly supportive settings.
Beyond the importance of subjective norm on exercise participation, attitude and perceived behavioral control were also important exercise determinants. Similar findings were reported among older adults for vigorous exercise intentions (Wankel et al., 1994) and adults with physical disabilities for leisure-time PA intentions (Ellis et al., 2009) and the SOC (Kosma et al., 2007). Understanding the important benefits of regular exercise participation and gaining confidence toward one’s control over exercise behavior are linked to exercise participation.
The SOC was the most important determinant of exercise behavior followed by perceived behavioral control. Increased perceived control and positive exercise intentions and experiences (SOC) are linked to exercise participation (Kosma et al., 2007; 2009). Similar results were found for exercise intention and perceived control among healthy adults (Symons Downs & Hausenblas, 2005), adults with physical disabilities (Ellis et al., 2009), and older adults (Dean et al., 2006).
As hypothesized, PA behavior had a strong negative link to risk of falls, meaning that the higher the exercise levels the lower the risk of falls. Exercise programs tailored to older adults are linked to reduced number of falls (Freiberger et al., 2007) or falls risk factors (Shumway-Cook et al., 2007).
It is important to note the study’s limitations. This was a cross-sectional study, and thus cause-and-effect relations cannot be determined. Experimental designs are needed to identify the most important mediators of PA behavior change among older adults. Longitudinal designs are also important to understand the temporal effects of PA determinants. Another study limitation reflects the fact that there was an overrepresentation of people in the action stage (n = 113) compared with the earlier SOC (n = 59). As already indicated, the current SOC scale was validated and used only in one other, recent study among adults with physical disabilities, and the participants were well represented across the SOC (Kosma & Ellis, 2010). It is possible that adults with physical disabilities face more exercise barriers than older adults, and thus regular exercise participation is a challenging task. Although the falls-risk scale used in the study (CFRSI; Fabre et al, 2010) includes the most common falls-risk subscales identified by the American Geriatrics Society (2001), the list is not exhaustive and in future studies additional falls-risk factors need to be assessed, such as fear of falling. Fear of falling can be caused by prior falls, leading to restricted future PA participation due to decreased confidence to safely be active, and consequently can increase the risk of future falls (Jørstad, Hauer, Becker, & Lamb, 2005; Spano & Forstl, 1992; Yardley & Smith, 2002). As already indicated, study participants were somewhat active, community-dwelling, diverse older adults, and thus the study’s results cannot be generalized to inactive and dependent older adults. Additionally, about half of the participants were Black, and thus the study cannot be generalized to the majority of U.S. older adults who are Caucasian (Treas & Carreon, 2010). Although the study examined important psychosocial factors toward PA participation, environmental factors and additional social aspects need to be taken into consideration when examining exercise participation.
Beyond the study’s limitations, it is important to highlight the study’s strengths in relation to future research directions. To our knowledge, this was the first study to examine important psychosocial determinants of PA and falls risks within a theory-based, integrative framework using path analysis among diverse older adults. Improved measures for the SOC and TPB constructs were also used. The study utilized a community-dwelling and diverse older adult population that was comprised of both White and Black individuals of varying economic and education levels. Data collection took place in several community centers where older adults reside, function, and socialize; therefore, the results of this study provide important information for health care researchers and practitioners. As already stated, health promoters need to reinforce supportive exercise settings for older adults, highlighting exercise benefits and increased confidence and control over the behavior. One’s exercise intentions and experiences need to be taken into consideration when designing exercise motivational programs, which have numerous benefits, such as decreased risk of falls. In future studies, the well-fit integrative framework by Kosma and colleagues (2007) can be used as a basis to be further expanded in order to determine different health outcomes like weight control and cancer prevention.
Conclusion
Based on the study’s findings, falls-risk prevention programs among older adults can be informed by promoting successful exercise programs based on one’s views about PA participation. In particular, providing supportive exercise settings, reinforcing the positive outcomes of exercise programs, and identifying ways to overcome exercise barriers and increase one’s control over the behavior can increase older adults’ exercise intentions and behavior, and thus reduce their risk of falls.
Footnotes
Acknowledgment
The author would like to thank Mr. TaeEung Kim for his assistance with data collection and entry. Mr. TaeEung Kim was a graduate student at the time the data were collected.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.