
Abstract
This study investigated whether transitioning into the role of activities of daily living (ADL) spousal caregiver is associated with increased depressive symptoms for older husbands and wives among a sample of coresiding community-dwelling older couples. Using data from the Health and Retirement Study, we estimated a two-level linear model to examine the association between change in caregiver status and respondents’ depressive symptoms at follow-up, controlling for other factors identified in Pearlin’s stress process model (PSPM). Results indicate that both husbands and wives who become ADL caregivers have more follow-up depressive symptoms than noncaregivers. Furthermore, wives continuing as caregivers have more follow-up depressive symptoms than wives who do not provide care. Finally, the physical health of the spousal caregiver is related to depressive symptoms at follow-up. We conclude with policy and practice implications of these three main findings.
Introduction
Nearly 20% of all caregivers aged 65 and older are husbands and wives who provide care to their spouse (National Alliance for Caregiving and American Association of Retired Persons [AARP], 2009), so it is important to consider issues related to their well-being, particularly depression. Depression not only affects the spousal caregiver but can result in negative outcomes for their care recipient, such as nursing home placement (Mittelman, Haley, Clay, & Roth, 2006). There is considerable evidence that those who provide care to a spouse have more depressive symptoms than their noncaregiving counterparts (Adams, 2008; Pinquart & Sörensen, 2003). Furthermore, providing care for activities of daily living (ADL) has clearer negative mental health consequences than does providing care for instrumental ADL (IADL; Burton, Zdaniuk, Schulz, Jackson, & Hirsch, 2003), and the likelihood that spouses are the main providers of ADL care is great (Wolff & Kasper, 2006). However, the majority of prior studies on the consequences of providing ADL care to a spouse typically examine those who are already a caregiver, and therefore it is unclear whether those transitioning into the ADL caregiving role may be at an increased risk for depressive symptoms. Better understanding is needed of the potential effects of transitioning into the caregiving role on depressive symptoms to provide information to those who design services to meet caregivers’ mental health needs. The purpose of our study is to examine whether transitioning into the role of an ADL spousal caregiver over a 2-year period is associated with increased depressive symptoms for husbands and wives among a representative sample of coresiding community-dwelling older American couples.
Background
The majority of older Americans experiencing limitations in ADLs live in the community and receive informal care from family members (National Center for Health Statistics, 2006; Wolff & Kasper, 2006), most often from a spouse when he or she is present (Lima, Allen, Goldscheider, & Intrator, 2008; Wolff & Kasper, 2006). Previous research has found that spousal caregivers have more depressive symptoms than their noncaregiving counterparts (Adams, 2008; Pinquart & Sörensen, 2003). Typically, however, these studies do not report when the caregiving activities began, so they cannot distinguish between those transitioning into care and those continuing care. Furthermore, few studies have examined the mental health effects of stopping caregiving for a spouse who is still alive and living in the community. Previous research suggests that the effects of caregiving are not static (Seltzer & Li, 2000) and individuals in different stages of the caregiving process are likely to adapt differently to care demands (Aneshensel, Pearlin, Mullan, Zarit, & Whitlatch, 1995; Cannuscio et al., 2002). An important area needing further attention is whether ADL spousal caregiving status (i.e., noncaregiving, transitioning, continuing, or stopping care) influences depressive symptoms.
Currently, there is very limited evidence regarding the effects on well-being of transitioning into the caregiving role. We located four studies (Burton et al., 2003; Cannuscio et al., 2002; Marks, Lambert, & Choi, 2002; Seltzer & Li, 2000) that have examined the depressive symptoms of those entering spousal caregiving over 3- to 5-year periods. Two of these studies (Burton et al., 2003; Marks et al., 2002) found that both husbands and wives transitioning to spousal care experienced more depressive symptoms than their noncaregiving counterparts. Cannuscio and colleagues (2002) reported similar differences among older married women transitioning into the spousal caregiving role. While Seltzer and Li (2000) did not find significant changes over time in depressive symptoms of wives who became new caregivers, wives did experience decline in other measures of well-being (e.g., lower marital satisfaction). There is a need for additional work in this area, however, because these studies compared new caregivers to noncaregivers, they could not distinguish between the effects of transitioning versus providing care in general. In addition, these studies used data from samples that were not nationally representative (Burton et al., 2003; Cannuscio et al., 2002; Seltzer & Li, 2000) or were collected more than two decades ago (Marks et al., 2002).
Few studies have focused on depressive symptoms of spouses continuing in the caregiver role. Some research has documented that an increase in care demands among those continuing spousal care is associated with a concurrent increase in depressive symptoms (Aneshensel et al., 1995; Li, Seltzer, & Greenberg, 1999). Cannuscio and colleagues (2002) did not find a significant difference in depressive symptoms between continuing caregivers and noncaregivers but examined only wives without serious mental or physical health problems at baseline.
Prior research on individuals who stop caregiving typically focuses on those whose care recipient died or moved into a long-term care facility. Among these studies, there is evidence suggesting that stopping care may have positive effects on family caregivers’ mental health, as they experience a decline in depressive symptoms following the care recipient’s death (Haley et al., 2008; Li, 2005; Schulz et al., 2003) or institutionalization (Gaugler, Mittelman, Hepburn, & Newcomer, 2009). However, this literature rarely examines the effects of ceasing spousal caregiving while the care recipient is alive and continues to live in the community. Cannuscio and colleagues (2002) did find a significant difference in depressive symptoms between wives stopping spousal caregiving and those not having provided spousal care, but it is unclear whether caregiving was stopped due to the death, institutionalization, or other reasons.
In addition to spousal caregiving status, there are other potential contributors to depressive symptoms. First, prior research focusing specifically on those transitioning into care or on caregivers in general often does not consider baseline and follow-up physical and mental health characteristics of the caregiver, important concerns when evaluating the effects of caregiving on depressive symptoms over time. Spouses of elders in need of ADL care are likely to be old and frail themselves, given the similarities in the health and well-being of married couples (Meyler, Stimpson, & Peek, 2007), which could limit their ability to enter or sustain the caregiving role. In numerous studies, spouses who do provide care experience detrimental effects on both their physical and mental health (Schulz & Beach, 1999; Vitaliano, Zhang, & Scanlan, 2003). Second, the caregiver’s gender may also influence the effects of caregiving on well-being. Prior research indicates that caregiving wives have more depressive symptoms than caregiving husbands (Sugiura, Ito, Kutsumi, & Mikami, 2009; Thompson et al., 2004). However, there are a number of plausible explanations for these gender differences, including (1) higher levels of caregiving stressors and utilization of different social resources by women and men, (2) gender differences in the general population’s mental health, with women twice as likely as men to experience depression (Pinquart & Sörensen, 2006), and (3) gender differences in the reporting of depressive symptoms (Gijsbers van Wijk, Huisman, & Kolk, 1999; Spinhoven & Kooiman, 1997). In their meta-analysis, Pinquart and Sörensen (2006) found that when differences in caregiver stressors and social resources are taken into account, gender differences in depression among caregivers were similar to those found in the general population. Taken together, these studies suggest the importance of including measures of baseline health and depressive symptoms of the potential caregiver, as well as examining the effects of caregiver status and other relevant factors in men and women separately.
Conceptual Framework
We adapted Pearlin, Mullan, Semple, and Skaff’s (1990) stress process model (PSPM; Aneshensel et al., 1995) to guide our interest in changes in the caregiver role among coresiding spouses living in the community. According to this model, caregiving is a career with a history of onset and progression. Our primary interest is whether becoming a spousal caregiver places an older adult at risk for higher depressive symptoms than being a noncaregiver once possible differences prior to transition into caregiving are taken into account. We also considered whether continuing or stopping caregiving increases the risk for depressive symptoms compared to not providing spousal care, as well as differences among these groups. The PSPM’s identification of four key dimensions helped differentiate the impact of caregiver status change from the effects of these other factors.
The background and context for caregiving in the PSPM represents the sociodemographic characteristics and baseline health of care recipients and caregivers. Numerous studies underscore the importance of these factors in well-being and depression. For example, disability, functional impairment, and prior depression are important risk factors for depression among older community residents (Cole & Dendukuri, 2003; Steffens, Bosworth, Provenzale, & MacFall, 2002).
Primary stressors in the PSPM reflect the objective and subjective aspects of recipient care needs and are viewed as the driving force influencing caregiver stress outcomes (Pearlin, Mullan, Semple, & Skaff, 1990). We focused on indicators of change in the health of the potential care recipient from baseline to follow-up. For example, previous research on changes in care recipients’ ADL dependencies showed that these changes affect care demands of the caregiver and subsequent adaptation of the caregiver (Gaugler, Kane, & Langlois, 2000).
Secondary stressors in the PSPM potentially result from the demands of caregiving, flowing directly from difficulties caregivers experience in responding to primary stressors. We conceptualized this dimension as spillover effect from providing care on changes in the health of potential caregivers. This decision was based on previous evidence that (1) spousal caregivers may have their own physical health problems that can be exacerbated while providing care (Pinquart & Sörensen, 2011, 2007) and make providing physical care especially stressful and (2) the chronic stress of caregiving leads to negative health outcomes such as more illness days (Son et al., 2007), chronic health conditions (Capistrant, Moon, & Glymour, 2012), insufficient time to exercise, failure to take prescription medications (Burton, Newsom, Schulz, Hirsch, & German, 1997), and greater mortality risk (Schulz & Beach, 1999).
The PSPM recognizes that not all caregivers are affected by caregiving in the same way because various psychosocial resources can influence stress (Goode, Haley, Roth, & Ford, 1998; Pearlin et al., 1990). Pearlin et al. (1990) originally used the word mediator, but Anshenshel et al.’s (1995) test of resources’ independent, mediating and moderating affects found only independent consequences. We therefore conceptualized social and financial resources of the couple as directly affecting caregiver stress. For instance, income inadequacy often results in greater depression (Beach, Schulz, Yee, & Jackson, 2000; Sun, Hilgeman, Durkin, Allen, & Burgio, 2009), especially for women (Elliott, 2001). Additionally, supportive social relationships have been shown to be negatively associated with depression, especially for men (Elliott, 2001).
Purpose of the Study
Previous research on the relationship between spousal caregiving and depressive symptoms has a number of limitations. First, few studies have examined the potential differential effects of caregiver status, particularly transitioning to the spousal caregiving role. Second, the limited work focused on those entering the spousal caregiving role (e.g., Burton et al., 2003; Marks et al., 2002) has not fully considered the possibility that baseline depressive symptoms and health status may differ between those who subsequently do and do not later transition into the spousal caregiving role. In studies where baseline health and depressive symptoms were not considered, it would be inappropriate to conclude that differences in depressive symptoms observed at follow-up between those who have and have not transitioned into the spousal caregiving role only reflect the effects of becoming a caregiver. Third, most of the prior research has not used nationally representative or recent samples.
Given these limitations in the caregiving literature, we explored three research questions using a nationally representative sample of coresiding community-dwelling spouses: (1) Is transitioning into a spousal caregiving role for ADL limitations associated with more depressive symptoms than being a noncaregiver? (2) Is continuing as a caregiver or stopping caregiving associated with more depressive symptoms than being a noncaregiver? (3) Do the depressive symptoms differ among those transitioning into, continuing, and stopping the caregiving role? For each of these research questions, we take into account baseline and follow-up characteristics of the potential spousal caregiver and care receiver.
Method
Data
We used data from the 2000 to 2006 Health and Retirement Study (HRS, 2011), based on both raw HRS data files and those prepared by the RAND Center for the Study of Aging (RAND-HRS). The HRS is an ongoing longitudinal panel study, surveying representative samples of Americans 50 years and older and their spouses or partners every 2 years. The HRS started in 1992 with 12,652 respondents (the 1931–1941 birth cohorts), adding new cohorts every 6 years and oversampling non-Hispanic Blacks, Hispanics, and residents of Florida. Collected information includes basic demographic characteristics, physical and mental health status, and who provided care for ADL limitations.
Because we focused on the influence of spousal caregiving status change on potential spousal caregiver’s depressive symptoms over each 2-year period, we limited our sample to those who (1) participated in all sections of the HRS survey for at least two consecutive waves, (2) were married or partnered to the same person throughout our study period, (3) had a spouse or partner who also participated in HRS during that period, (4) lived in the community with their spouses at both waves, and (5) met the original HRS sample criteria (i.e., 50 years of age or older and community residents) in order to maintain nationally representative data. We excluded those proxy respondents (n = 389) who indicated that the original respondent could not be interviewed due to cognitive limitations because proxy respondents were not asked about a respondent’s depressive symptoms, and we expected such symptoms might be different for these individuals. We also dropped respondents in same-sex couples (n = 8) as both would appear in the same model (i.e., as both husbands or both wives). We also dropped those with zero personal weight (n = 2). These sample selection criteria resulted in a panel data set with 26,982 observations from 5,837 unique husbands and 5,837 wives.
Each respondent could have at most three possible observations based on three possible 2-year periods (2000–2002; 2002–2004; 2004–2006). In each period, the first year was considered the baseline and the second year the follow-up. This approach enabled us to examine how spousal caregiving status changed over the 2 years and how these changes affected the potential spousal caregiver’s depressive symptoms at follow-up once other factors were taken into account. Overall, 10.51, 17.59, and 71.90% of respondents had one, two, and three observations in the data set, respectively.
Variables and Measures
We use the term “respondent” for the person in the couple whose depressive symptoms at follow-up are the focus of our research questions and “spouse” for that person’s partner. Unless otherwise specified, all variables were assessed for the respondent. Coding details for variables are shown in Table 1. The dependent variable was respondent’s number of depressive symptoms at follow-up, measured with the Center for Epidemiologic Studies-Depression’s (CES-D) 8-item instrument (Radloff, 1977). Responses agreeing that the six “negative” indicators (depression, everything is an effort, sleep is restless, felt alone, felt sad, and could not get going ) were experienced “all or most of the time” and denying the two “positive” indicators (felt happy and enjoyed life) were summed yielding scores of 0–8, with higher values indicating more symptoms. The 8-item CES-D scale has been known to have good reliability and internal consistency (Steffick, 2000).
Sample Characteristics of Husbands and Wives in Health and Retirement Study (2000–2006).

Note. ADL = activities of daily living; IADL = instrumental activities of daily living.
Table entries are unweighted data prior to missing imputation for observations meeting the study selection criteria for any 2-year period. All change variables are based on changes over two consecutive waves of data collection: 2000–2002, 2002–2004, or 2004–2006. Percentages are shown for categorical variables; means are shown for continuous variables with standard errors in parentheses. For categorical variables, the first listed category is the reference group in subsequent tables. All variables were regarding each respondent’s characteristics unless specified as “spouse.”
For each observation, if a person with any ADL limitations (bathing, dressing, eating, walking across a room, getting in or out of bed, or using a toilet) reported that they got help from their spouse, we coded the partners as a spousal caregiver. Then, depending on caregiving status changes over 2 years, we created the four caregiving categories for respondents: remained not caregiving, transitioned to caregiving, continued caregiving, and stopped caregiving. Because our sample included only those residing in the community at both waves, we note that none of the respondents in the stopped caregiving category did so because their spouse died or was institutionalized.
As background/context variables, we included respondent’s baseline CES-D score and demographic characteristics (i.e., age, race/ethnicity, marital status, and education). Additionally, we included age-squared to take into account a U-shaped relationship between respondent’s age and follow-up CES-D score. We also included measures of respondent’s and spouse’s baseline number of ADL limitations and respondent’s provision of baseline spousal IADL care. To control for period effects, we included two dummy variables indicating the year of the follow-up observation.
Many of the variables assessing primary stressors, secondary stressors, and resources reflected changes over a 2-year period. For each of these measures, we created categorical change variables: (1) not present at baseline or follow-up, (2) present at follow-up only, (3) present at both baseline and follow-up, and (4) present at baseline only.
The five primary stressor variables measured change in spouse’s health status, including (1) change in spouse having any moderate to serious health condition (diabetes, chronic lung disease, arthritis, incontinence, cancer, heart problems, stroke, emotional/nervous/psychiatric problems, very poor eyesight, or legal blindness); (2) change in spouse having any moderate to serious cognitive impairment (self-respondents with a score of 10 or less in the HRS modified version of the Telephone Interview for Cognitive Status (Rodgers, Osfstedal, & Herzog, 2003) or proxy respondents reporting any serious cognitive problem for the original respondent (Freedman, Aykan, & Martin, 2001); (3) a dichotomous variable indicating the spouse had any nursing home stay between baseline and follow-up; (4) a dichotomous variable indicating the spouse had any hospital stay between baseline and follow-up; and (5) change in spouse’s number of ADL limitations.
Five secondary stressor variables measured change in respondent’s health status in the same manner as the five primary stressors (i.e., health conditions, cognitive impairment, nursing home stay, hospital stay, and ADL limitations). The sixth variable assessed change in a respondent’s paid work from baseline to follow-up.
The four resource variables included potential sources of support to reduce the stress of caregiving responsibilities. Three of these assessed change from baseline to follow-up: (1) the use of any other ADL caregivers for the spouse, (2) any sons residing with the couple or within 10 miles (called proximate sons hereafter), and (3) any proximate daughters. We also included the respondent’s household wealth at follow-up, measured in four categories due to the nonlinearity of the relationship of this measure with follow-up CES-D score. We separated those with zero or negative wealth because these respondents might have higher depressive symptoms (Lorant et al., 2003) and then divided those with positive wealth into tertiles.
Statistical Analyses
We estimated a two-level linear model using the STATA xtmixed procedure to predict a respondent’s depressive symptoms at follow-up. The model took into account multiple observations for a respondent and accounted for variations in observations across and within respondents. We centered each continuous predictor at its mean.
The depressive symptoms for a respondent i at time t are specified in the following equation:
where CESD
it
represents a CES-D score for an individual i at the follow-up interview (t). ΔCGstatusit refers to a vector regarding change in a respondent’s spousal ADL caregiving status between the baseline (t − 1) and follow-up interview (t). The coefficient of main interest π1 measures the effect of caregiving status change on an individual ’i’s depressive symptoms at follow-up.
We used a time-variant personal weight for Level 1 variables and a time-invariant weight based on the year when each respondent was initially enrolled in the HRS study for Level 2 variables. After examining patterns of missing data and concluding that data were missing at random, we addressed missing data using the multiple imputations by chained equations procedure. This procedure constructed five complete data sets and then adjusted for the effects of missing data on statistical inference.
Because all data were from husband–wife pairs and each partner was both a respondent and a spouse, we fitted separate regression models for husbands and wives and therefore were unable to test for significant gender differences. This approach allowed us to understand the effects of caregiver status and variables reflecting the PSPM on depressive symptoms for husbands and wives.
Results
Sample Description
Table 1 presents descriptive statistics for this sample of husbands and wives. Caregiver status change was similar for wives and husbands, with more than 90% of both groups not providing ADL spousal care at either time. Nearly 3% of wives and husbands transitioned to caregiving over the 2-year period, more than 2% continued caregiving, and less than 2% stopped caregiving. This sample of community-dwelling husbands and wives was relatively healthy, as indicated by depressive symptoms, cognitive impairments, and ADL limitations at baseline and follow-up. Few husbands and wives had any other caregiver present at either time point. Nearly 30% of respondents had at least one proximate son or proximate daughter present at each time point.
Table 2 provides the baseline and follow-up CES-D scores by caregiver status among husbands and wives. As shown in the table, at baseline, wives had more depressive symptoms than husbands in all caregiving status groups, indicating the importance of taking into account depression at baseline. Furthermore, both husbands and wives who transitioned into spousal care and continued as caregivers had increases in depressive symptoms, while those who remained as noncaregivers showed stability in depressive symptoms. Among those who stopped caregiving, husbands decreased in depressive symptoms, whereas comparable wives showed increased symptoms.
Baseline and Follow-up C-ESD Scores by Caregiving Status Among Husbands and Wives.

Note. CES-D = Center for Epidemiologic Studies-Depression.
Table entries are means and standard deviations in parentheses, based on unweighted data prior to missing imputation for observations meeting the study selection criteria for any 2-year period. CES-D scores can vary between 0 and 8.
aWe used 13,491observations for each gender.
Transitioning to Care Versus Not Providing Care
As shown in Table 3, husbands and wives who became an ADL caregiver over a 2-year period had significantly more depressive symptoms at follow-up than those who remained as noncaregivers when all components of the PSPM were considered.
Multilevel Linear Models Predicting Respondent’s CES-D Score Among Husbands and Wives.

Note. ADL = activities of daily living; IADL = instrumental activities of daily living.
All change variables are based on changes over two consecutive waves of data collection: 2000–2002, 2002–2004, or 2004–2006. For categorical variables, the first listed category is the reference group. All variables were regarding each respondent’s characteristics unless specified as “spouse.”
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Aspects of each component of the PSPM also had significant independent effects on depressive symptoms at follow-up. The effects of background and context were largely similar for husbands and wives. Those with more depressive symptoms at baseline and fewer years of education had significantly higher depressive symptoms 2 years later. The significant age and age-squared coefficients indicated a U-shape relationship between age and depressive symptoms, with more depressive symptoms among younger and older respondents. Respondents with more baseline ADL limitations also had more depressive symptoms at follow-up. Husbands who provided IADL care at baseline had more follow-up depressive symptoms than those who did not.
A small number of the primary stressors had significant effects on follow-up depressive symptoms. For both genders, those whose spouse was hospitalized between baseline and follow-up had more depressive symptoms. For husbands only, those whose spouse had health conditions at both time points had more depressive symptoms than those whose spouse was free of such conditions at both times. Because change in spouse’s ADL limitations was highly correlated with caregiver status change, we were unable to include this variable in our final model.
Several of the secondary stressors were significant for both husbands and wives. Respondents whose ADL limitations increased or had any hospital stays over the 2-year period had significantly more follow-up depressive symptoms. Husbands who had a nursing home stay in the previous 2 years had significantly more depressive symptoms. Compared to those without any health conditions, respondents reporting health conditions at follow-up only or those with health conditions at both times had a higher number of depressive symptoms. Husbands and wives employed at both times or only at baseline had fewer depressive symptoms than those who worked neither time. Additionally, husbands who worked only at follow-up had more depressive symptoms than those not working either time.
Among the resources examined, only wealth was significantly related to depressive symptoms. Both husbands and wives with higher levels of positive wealth had fewer depressive symptoms than those with debt or lacking any assets. Changes in availability of other helpers or proximate children were not significant.
Continuing and Stopping Caregiving Versus Noncaregiving
Table 3 also shows the effects of continuing or stopping ADL caregiving on depressive symptoms. Both husbands and wives who stopped providing care did not differ in their follow-up depressive symptoms from noncaregivers. Husbands continuing care did not have more depressive symptoms at follow-up than husbands who remained as noncaregivers. Wives who continued in the caregiving role, however, were significantly more likely to experience depressive symptoms at follow-up than noncaregivers.
Differences Between Transitioning, Continuing, and Stopping Care
To address our third research question, we reran the models for each gender using the same observations and variables in the analyses as given in Table 3 but changed the caregiver status reference group. The results from these models are shown in Table 4. When we focus on the continued caregiving group, we see that neither husbands nor wives who continued ADL caregiving differed in follow-up depressive symptoms from those who stopped caregiving or transitioned into caregiving. When we focus on those who transitioned to care, we see that both husbands and wives who transitioned into the caregiving role had significantly more depressive symptoms than those who stopped caregiving.
Additional Multilevel Linear Models Predicting Respondent’s CES-D Score Among Husbands and Wives Comparing Those Who Transitioned to Caregiving, Continued Caregiving, and Stopped Caregiving.
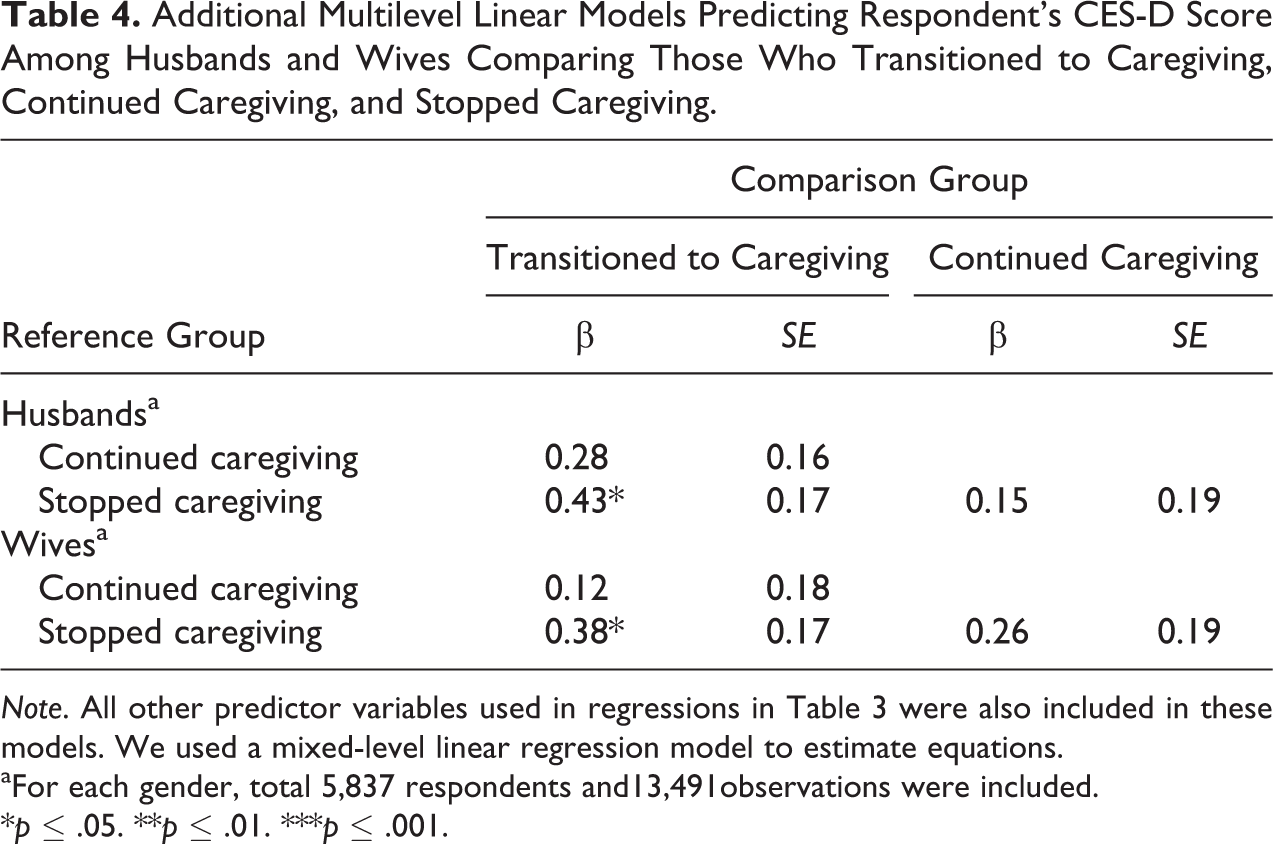
Note. All other predictor variables used in regressions in Table 3 were also included in these models. We used a mixed-level linear regression model to estimate equations.
aFor each gender, total 5,837 respondents and13,491observations were included.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Discussion
Guided by PSPM (Pearlin et al., 1990), this study examined the association between transitioning into the ADL spousal caregiving role and other changes in caregiver status on depressive symptoms. Using a nationally representative sample of community-dwelling couples, there were three main findings of our study that expand prior knowledge on depressive symptoms in spousal caregivers while also considering other aspects of the caregiving experience identified by the PSPM. First, both husbands and wives who transition to spousal caregiving over 2 years have more depressive symptoms than those who remain as noncaregivers. Second, some results suggest differential effects of continuing spousal care for husbands and wives. Third, our findings indicate the importance of considering baseline characteristics of caregivers and recipients and changes in those characteristics over time.
Because prior research typically examines the caregiving experience after it began, it has not been possible to understand the association of the transition to care on the caregiver’s depressive symptoms. By addressing some of the limitations of these earlier studies, our results expand previous evidence and show that transitioning into the ADL caregiving role is a stressful period for both husbands and wives. This is indicated by a greater number of depressive symptoms at follow-up for new caregivers than those remaining noncaregivers, supporting the limited prior work in this area (Burton et al., 2003; Cannuscio et al., 2002; Marks et al., 2002). Our results highlight the importance of interventions designed to address the stress associated with role entry.
Furthermore, we considered how the mental health of those who continue or stop ADL spousal caregiving differ from those who remain not providing care. Results show that among couples living in the community at both times, husbands and wives who stop providing spousal care do not differ from those continuing as noncaregivers. Wives continuing as caregivers have more depressive symptoms than those remaining as noncaregivers, while the depressive symptoms of husbands continuing care do not differ from those of husbands remaining as noncaregivers. Differing gender roles for husbands and wives could explain these findings. Because women are expected to take on caring tasks and responsibilities (Yee & Schulz, 2000), they may face more care demands as they continue caregiving. Additionally, it has been suggested that men are more likely than women to use problem-focused coping strategies rather than emotion-focused coping (Etters, Goodall, & Harrison, 2008; Sugiura et al., 2009), suggesting men may adapt faster to the caregiving role than women. There is also evidence that men focus on accomplishing tasks while women focus on the quality of their task performance (Calasanti & Bowen, 2006). Both of these strategies may serve as protective factors for husband’s mental health as they continue to provide spousal care. Furthermore, wives may have other caregiving responsibilities not shared by their husbands, such as raising grandchildren (Hayslip & Kaminski, 2005), which could negatively affect their mental health.
We also examined potential differences in follow-up depressive symptoms among those transitioning into, continuing, and stopping the caregiving role. Results demonstrating a significant difference between spouses who transition to care and spouses who stop care are consistent with prior research showing an improvement in the mental health of caregivers who stopped caregiving following the death (Haley et al., 2008; Li, 2005; Schulz et al., 2003) or institutionalization (Gaugler et al., 2009) of their care recipient. The majority of former care recipients had no ADL limitations at follow-up, whereas the spouses of persons transitioning into care had more ADL limitations at follow-up than baseline (data not shown). This suggests that the difference between stopping and transitioning caregivers may be due to changes in time spent in care tasks and feelings of overload, with those in the transitioning group experiencing an increase in overload over 2 years while those in the stopped caregiving group experiencing a decrease in overload.
We also found that husbands and wives who continue caregiving were not significantly different in depressive symptoms than those who stop or transition into spousal caregiving. The absence of significant differences between those who stopped and those who continued care is particularly puzzling, given the research cited previously demonstrating an improvement in mental health among former caregivers. One potential explanation is that those who stopped providing care to their spouse in our sample did so for a variety of reasons not often examined in research. Some may have stopped because their spouse’s health improved, while others may have stopped because someone else took over the caregiving responsibilities or because they were particularly stressed by providing spousal care. These reasons may have very different effects on depressive symptoms. Additional research is needed that focuses on the causes and consequences of stopping spousal care among those whose care recipient remains alive and in the community.
Our study also contributes to an understanding of PSPM. We examined measures reflecting background, primary stressors, secondary stressors, and resources identified in this model to separate the effects of changes in caregiver status from these other aspects of the caregiving experience. Reinforcing the PSPM, our results indicate that aspects of each of these dimensions are influential. One key finding relevant to the PSPM model was the discovery that the context in which ADL care is provided (i.e., baseline physical and mental health characteristics of the caregiver and provision of IADL care) affects caregiver mental health. Failure to take these into account in prior research has made it difficult to reach firm conclusions about the effects of changes in caregiver status.
This study has limitations that should be addressed in future research. While we examined ADL caregiver status change over a 2-year period, a shorter time period than prior studies, we lacked knowledge about spousal caregiving experiences before the years included in our study or the length of time within those 2 years transitioning caregivers were “new” to the caregiving role. On the other hand, the fact that we were able to evaluate the effects of transitioning to ADL caregiving over the relatively short period of 2 years may aid in capturing the influence of recent entry into the caregiver role on caregivers’ mental health. It also should be noted that we cannot generalize our findings to less healthy groups, as the sample we used reflects data from a nationally representative sample. Additionally, we could not examine the small sample in the “other” racial/ethnicity category, as it was less than 2% of the sample.
While other researchers (Aneshensel et al., 1995; Li, Seltzer, & Greenberg, 1999) report that increasing depressive symptoms are linked to increasing care demands, we found only limited evidence of this in our analyses, possibly because we were unable to include more traditional measures of burden. Specifically, we removed changes in the spouse’s ADL limitations from our regression models due to its high collinearity with changes in ADL caregiver status. It was not possible to disentangle the effects of change in caregiver status from those of change in spousal need for care on potential caregivers’ depressive symptoms. However, even with this limitation, other aspects of caregiver’s health and changes in caregiver’s health over time were important considerations in this study that have not been fully addressed to date. We could only assess significant differences in depressive symptoms associated with changes in caregiver status without indicating their clinical relevance, as there is no agreement about or a validated cutoff point used with the 8-item CES-D scale to describe respondents as clinically depressed (Steffick, 2000; Turvey, Wallace, & Herzog, 1999), We also could not consider other important and potentially explanatory variables such as provision of emotional assistance or quality of marriage which could influence commitment to the caregiving role and stress associated with it. Nor did available data permit us to consider whether the caregiver received emotional support from a child or anyone else, although instrumental support in providing care was taken into account.
Conclusion and Implications
This examination of change in ADL caregiver status with consideration of baseline and follow-up measures of health and mental health of both the potential caregiver and care receiver adds three key findings to the caregiving literature that can alert practitioners and policy makers to caregivers who may warrant special attention. First, both husbands and wives typically find transitioning into the caregiver role difficult, as they suffer from more depressive symptoms than noncaregiving spouses. Assessing the mental health of new caregivers might identify those who could benefit most from educational programs focused on basic caregiving techniques involved in bathing, toileting, and so on, and various aspects of taking on the caregiver role such as understanding the care needs of the care recipient and building a support network to help with caregiving over time. Second, it is important for practitioners to recognize potential variations in the way that the caregiver’s activities affect each gender both prior to and during ADL caregiving provision. Specifically, our findings suggest that wives who are providing spousal ADL care may need support for a longer duration than husbands providing such care. This support could include use of respite services and knowledge about community resources such as transportation and support groups. Finally, despite evidence that spousal caregivers often experience greater health problems compared to other caregivers because they are older (Barber & Pasley, 1994) and therefore may need more help in taking care of their own health needs, their physical health is often ignored in research examining predictors of caregiver mental health. Our results show that the poor health of husbands and wives providing ADL care is related to more depressive symptoms and highlight the importance of evaluating spousal caregivers’ health needs throughout the caregiving experience. This suggests practitioners could benefit from identifying and assisting spousal caregivers whose physical health is affecting their mental health, given established links between late life depressive scores and increased risk for physical functional decline as well as other health problems such as disability and mortality (Penninx et al., 1999). Providing such caregivers with support for their health behaviors including eating, sleeping, and exercise as well as regular doctor visits could help to maintain their well-being, support the caregiving relationship, and enhance their ability to continue in the caregiver role. This recommendation is supported by information demonstrating that targeting improvement in family caregivers’ health may result in lower levels of depression (Elliott, Burgio, & DeCoster, 2010). Burton, Newsom, Schulz, Hirsch, and German’s (1997) finding that living with a spouse with ADL impairment has a negative effect on caregivers’ own preventive health behaviors suggests that interventions need to focus on changes in caregivers’ health behaviors that place them at risk such as having time to rest, exercise, and recuperate. This may include respite periods from caregiving. Our results suggest the importance of considering all three findings from this study in order to address the mental health of spousal caregivers, and in particular, the mental health of those transitioning into the caregiver role. In considering all of these policy and practice implications, because not all people who provide care identify themselves as a caregiver, it is also important for practitioners to spread a broad net and identify spouses who provide care to their partners in order to offer help to them rather than just to those who label themselves as caregivers (AARP, 2001; O’Connor, 2007).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.