
Abstract
Consistent with the weathering hypothesis, many studies have captured racial/ethnic disparities in average functional health trajectories. The same mechanisms of social inequality that contribute to worse average health among minority adults may also contribute to greater fluctuations in their physical function at upper ages. Using panel data from the Health and Retirement Study, we examine patterns of intraindividual variability over time in trajectories of functional limitations for White, Black, and Hispanic older adults. Intraindividual variability increases with age for both Whites and Blacks and such increase is greater for Blacks. Hispanics have the greatest intraindividual variability but there is no age-based pattern. Socioeconomic status and comorbidity are associated with intraindividual variability for all race/ethnicity yet do not explain the age-based increase in intraindividual variability for Whites or Blacks. The findings suggest further nuances to the weathering hypothesis—social disadvantage can generate instability in physical function as minority adults age.
Introduction
The existence of racial/ethnic disparities in health and functional outcomes among older adults has been clearly established (Angel & Angel, 2006; Mutchler & Burr, 2011; Williams & Wilson, 2001). A substantial body of research has documented a persistent Black/White disability gap during later life that cannot be fully explained by education, income, or poverty (Brown, O’Rand, & Adkins, 2012; Clark & Maddox, 1992; Haas & Rohlfsen, 2010; Kelley-Moore & Ferraro, 2004; Kim & Miech, 2009; Liao, McGee, Cao, & Cooper, 1999; Mendes de Leon, Barnes, Bienias, Skarupski, & Evans, 2005; Taylor, 2008; Thorpe et al., 2011). Similar disparities have been observed for Hispanic older adults who tend to have worse physical function (Brown et al., 2012; Dunlop, Song, Manheim, Daviglus, & Chang, 2007; Haas & Rohlfsen, 2010; Markides, Eschbach, Ray, & Peek, 2007) and spend more years functionally limited than do their non-Hispanic White and Black counterparts (Hayward, Warner, & Crimmins, 2007).
The weathering hypothesis provides an explanatory framework for the robust finding that racial/ethnic minorities, especially Black Americans, acquire health conditions at younger ages and experience health deterioration more rapidly than do White Americans, as a result of long-term exposure to social and environmental stressors over the life course (Geronimus, 1992, 2001). Emphasizing weathering-type explanations, a large body of empirical research has focused on capturing differences in the average rate of change in health and functional trajectories by race/ethnicity (Brown et al., 2012; Haas & Rohlfsen, 2010; Johnson, Schoeni, & Rogowski, 2012; Kelley-Moore & Ferraro, 2004; Kim & Durden, 2007; Kim & Miech, 2009; Shuey & Willson, 2008; Taylor, 2008; Warner & Brown, 2011; Wickrama, Mancini, Kwag, & Kwon, 2013; Yang & Lee, 2009). However, much less attention has been devoted to intraindividual variability over time in health measures, which has also been shown to increase with age and to be greater among racial/ethnic minorities (Callisaya, Blizzard, Schmidt, McGinley, & Srikanth, 2010 ; Christensen et al., 2005; Contoyannis, Jones, & Rice, 2004). Focusing exclusively on the average rate of change in health trajectories may obscure important health dynamics and patterning, especially for racial/ethnic minorities, since the same mechanisms of social inequality that contribute to worse average health among minority adults may also contribute to their greater within-person fluctuations at upper ages.
The purpose of this article is to contribute further to our understanding of weathering and, relatedly, the social mechanisms underlying observed health disparities, by examining the racial/ethnic patterning of intraindividual variability in late-life physical function. We begin by situating our work in a review of extant literature applying the weathering explanation to observed racial/ethnic difference in late-life functional change. We then empirically examine whether the age-based patterns of intraindividual variability over time in trajectories of functional limitations differ by race/ethnicity, using data from a long-term, national panel study of older adults. Finally, we discuss the implications of our findings for research on late-life health disparities and minority aging.
Theoretical Framework
Well-documented and robust racial/ethnic health disparities have certainly stimulated many theoretical considerations of their sociogenic origins. Several theories and conceptual models have been proposed to understand how health variability plays out over the life course through biological, behavioral, and sociostructural pathways (Dannefer, 2003; Ferraro & Shippee, 2009; Kuh & Ben-Shlomo, 1997; Wadsworth, 1997). In particular, Geronimus (1992) proposed the weathering hypothesis as one mechanism for social inequalities to “get under the skin” through the stress process as racial/ethnic minority adults age. Originally formulated to explain the Black/White difference in infant mortality, the weathering hypothesis has now evolved to a broader framework where the unique life course stress accumulation for minority adults is used to explain the distinct age patterns by race/ethnicity in a variety of late-life health and functional indicators (Geronimus, 2001).
Specifically, the weathering hypothesis posits that the adverse social conditions that racial/ethnic minorities experience can trigger stress-induced physiological dysregulation, which in turn results in onset of disease and more rapid health decline at older ages (Geronimus, Hickens, Keene, & Bound, 2006; Jackson, Knight, & Rafferty, 2010; Kaestner, Pearson, Keene, & Geronimus, 2009). Compared to Whites, racial/ethnic minorities are more likely to experience social environmental stressors such as discrimination and racism (Williams & Mohammed, 2009), unemployment (Wilson, Tienda, & Wu, 1995), and economic insecurity (Meschede, Shapiro, Sullivan, & Wheary, 2010). Higher rates of morbidity and disability incidents among minority older adults can then be attributed to sustained and frequent environmental press due to various social barriers.
While Geronimus and colleagues have focused on earlier and more rapid health deterioration of minority adults as the consequence of accumulated stress, prolonged and repeated activation of the body’s fight-or-flight response mechanisms can compromise its overall physiological capacity and make one’s health status more sensitive to social environmental influences (Cohen, Janicki-Deverts, & Miller, 2007), thereby generating instability in health measures (Campbell & Buchner, 1997). Thus, we may observe greater fluctuations in minority adults’ physical function as a second consequence of accumulated stress over the life course.
Despite the plausibility of such a process, instability in physical function has received little empirical attention. Extant literature has to date focused on capturing average differences in late-life health and functional decline by race/ethnicity. This is typically done by conducting cross-sectional comparisons of average differences in health indicators between groups within each age stratum (Geronimus, Bound, Keene, & Hicken, 2007; Geronimus et al., 2006; Nuru-Jeter, Thorpe, & Fuller-Thomson, 2011), or by comparing groups’ average rate of change in long-term health and functional trajectories facilitated by the recent expanding use of panel data and growth curve modeling (Brown et al., 2012; Haas & Rohlfsen, 2010; Johnson et al., 2012; Kelley-Moore & Ferraro, 2004; Kim & Durden, 2007; Kim & Miech, 2009; Shuey & Willson, 2008; Taylor, 2008; Warner & Brown, 2011; Wickrama et al., 2013; Yang & Lee, 2009). These comparisons often lead researchers to conclude that racial/ethnic minorities, especially Black older adults, have distinct health profiles characterized by early onset of disability (Haas & Rohlfsen, 2010; Taylor, 2008), “accelerated aging” (Geronomis et al., 2006), or “accelerated disablement” (Warner & Brown, 2011).
In this article, we extend this line of inquiry by shifting the lens of focus from average differences in health trajectories between subgroups to racial/ethnic patterning in intraindividual variability over time. Functional change during later life may not necessarily follow a continuous, gradually declining course (Campbell & Buchner, 1997; Gill, Allore, Hardy, & Guo, 2006; Hardy, Dubin, Holford, & Gill, 2005; Verbrugge, Reoma, & Gruber-Baldini, 1994; Wolf, Mendes de Leon, & Glass, 2007) and is, therefore, not best characterized by an average rate of change in a trajectory (Kelley-Moore & Lin, 2011). Moreover, some studies have shown that greater fluctuations in health are more commonly observed at upper ages (Callisaya et al., 2010; Gill et al., 2006), and among racial/ethnic minorities (Contoyannis et al., 2004) and those with non-English-speaking backgrounds (Christensen et al., 2005).
The empirical evidence of weathering may be most easily observed in average health differences between racial/ethnic groups, but potential patterns of intraindividual variability in physical function would raise a number of questions for studies of life course-health disparities and minority aging. Do the same social mechanisms that contribute to worse average health among minority adults also contribute to greater fluctuations in their health at upper ages? Do these patterns have implications for testing the weathering hypothesis and for comparing racial/ethnic groups in studies of late-life health disparities? Are the health dynamics of racial/ethnic minority adults best characterized by chronologically accelerated functional decline? Might it be beneficial to use intraindividual variability as the outcome when documenting and explaining racial/ethnic health disparities? Using eight waves of panel data from the Health and Retirement Study (HRS), we address these questions by empirically examining whether the age-based patterns of intraindividual variability over time in functional trajectories are different for White, Black, and Hispanic older adults.
Research Design
Data and Sample
Data come from the HRS, which is a panel study initiated in 1992, with a nationally representative sample of noninstitutionalized adults aged 51 and over. Respondents have been interviewed every 2 years. The HRS utilizes a multistage area probability sampling design with oversamples of non-Hispanic Black and Hispanic adults, allowing us to adequately examine racial/ethnic differences. Although the study has evolved into a steady-state panel with new birth cohorts being added to the panel at regular intervals, our analysis focuses on the original HRS birth cohort (born 1931–1941), given evidence that racial disparities in functional limitations differ across cohorts (Yang & Lee, 2009).
We excluded the first two waves of data because the measures of functional limitations in 1992 and 1994 differ from those in subsequent waves. Only non-Hispanic White, non-Hispanic Black, and Hispanic respondents are included, as there are too few respondents in other racial/ethnic categories to permit meaningful contrasts. After excluding proxy interviews, we further limit the analysis to individuals who have at least two observation points for an examination of variability within individuals. The final analytic data set includes 7,715 individuals (5,763 Whites, 1,254 Blacks, and 698 Hispanics) aged 55–65 at baseline who contributed 43,680 observations over the 14-year period (1996/Wave 3 to 2010/Wave 10).
Measurement
The outcome under study is functional limitations, which is measured by a wave-specific summed score of 11 limitations related to mobility, strength, and upper and lower body tasks: (1) walking several blocks; 2) walking one block; (3) climbing several flights of stairs; (4) climbing a single flight of stairs; (5) sitting for 2 hr; (6) getting up from the seated position; (7) stooping, kneeling, or crouching; (8) pushing or pulling large objects; (9) lifting 10 pounds; (10) raising arms above the shoulder; and (11) picking a dime off of a table. Respondents indicate the level of difficulty in performing each functional task on the following scale: 0 = no difficulty, 1 = some difficulty, and 2 = a lot of difficulty/can’t do. The summed score ranges from 0 to 22. The validity of this measure has been documented (Wallace & Herzog, 1995).
Race/ethnicity is measured by three dichotomized variables: non-Hispanic White (= 1, else = 0; reference group), non-Hispanic Black (= 1, else = 0), and Hispanic (= 1, else = 0). The respondent’s age is measured in years and is calculated from his or her birth year. Gender is measured by a dichotomized variable—female (= 1, else = 0). We measure the respondents’ socioeconomic status (SES) using education (in years), individual earnings, and nonhousing assets. Nonhousing assets are the sum of all household assets excluding primary and secondary residence, minus any debts. We calculate an individual equivalent of household assets by dividing household-level assets by the square root of household size (Willson, 2003). Earnings and assets are both logarithmically transformed to correct for right skewness. We mean-center education, earnings, and assets to aid the interpretation of the intercept.
We include a number of covariates that are correlated with functional limitations: married (= 1, else = 0), currently working (= 1, else = 0), ever smoked (= 1, else = 0), obese (= 1, else = 0), and comorbidity (count of seven chronic conditions including heart disease, stroke, lung disease, cancer, diabetes, high blood pressure, and arthritis). Age, earnings, assets, married, working, obese, and comorbidity are time-varying covariates measured contemporaneously. Race, gender, education, and ever smoked are time-invariant covariates.
Trajectory Model of Functional Limitations
We estimate wave-based trajectory of functional limitations in a multilevel mixed-effects modeling framework:

The term yti is the functional limitation score for respondent i at time t, for i = 1: n and t = 1:T. β0 is the intercept and β1is the slope of the trajectory indexed by wave. The term Xpti represents time-varying covariates for p = 1:P, where P is the total number of such covariates and Zqi represents time-invariant covariates, for q = 1:Q, where Q is the total number of such covariates.
We note two analytic decisions in our specification of the trajectory model. First, we retain a more parsimonious linear specification of the trajectory because, consistent with prior studies (Brown et al., 2012; Warner & Brown, 2011), our preliminary analysis (not shown) specifying quadratic and cubic trajectories yields nonsignificant polynomial terms and do not significantly improve model fit when compared to the linear specification. Second, although functional limitations are measured in integers and exhibit a skewed distribution, we recognize a censored normal distribution for this type of measurement (Long, 1997) and use a Gaussian link for the trajectory model, which is most appropriate for handling a censored normal outcome variable in mixed-effects trajectory models (Skrondal & Rabe-Hesketh, 2004).
The random-effects equation accounts for between-individual (Level 2; random intercept ς oi , and random slope ς1Wave and within-individual variances (Level-1 residual ∊ ti ). We estimate the variance of Level-1 residual, θ, which describes the typical deviation of a response from model implied individual mean. For example, if the estimate variance of Level-1 residual is 2, it means that a typical distance between a response and the individual mean is 1.41. This estimate indicates unexplained intraindividual variability in the trajectory model, even after accounting for covariates in the fixed-effects equation (Rabe-Hesketh & Skrondal, 2012 ).
To investigate racial/ethnic differences in intraindividual variability in the trajectories, we relax the homoscedasticity assumption and allow Level-1 residual variance θ to differ by race/ethnicity. Specifically, we estimate a trajectory model with three Level-1 residual variance components: θ(W) for White adults, θ(B) for Black adults, and θ(H) for Hispanic adults. We compare this model to the base trajectory model to determine whether there is any significant racial/ethnic difference in Level-1 residual variance (i.e., intraindividual variability).
Prediction Model of Intraindividual Variability
From the trajectory models, we extract predicted Level-1 residuals for each racial/ethnic group as the outcome variables for further analysis. We estimate a random-effects Gaussian regression model with a maximum likelihood estimator, which is more appropriate for an incomplete panel data structure (Rabe-Hesketh & Skrondal, 2012):

The term
Analysis Plan
The analysis proceeds in three stages. First, we report descriptive statistics of study variables for the total sample and for each race/ethnicity. We test for statistically significant differences (α = .05) between racial/ethnic groups using χ2 tests or t tests as appropriate.
Second, we estimate a wave-based trajectory model of functional limitations with covariates, assuming homoscedastic Level-1 residuals. We then estimate the same trajectory model with separate Level-1 variances for each race/ethnicity. Using likelihood ratio (LR) test, we compare these two models to determine if specifying heteroscedastic Level-1 residuals significantly improves model fit. If so, it would indicate that the degree of intraindividual variability in trajectories indeed varies by race/ethnicity (Rabe-Hesketh & Skrondal, 2012).
Third, we estimate prediction models of intraindividual variability for each race/ethnicity and use an equality of coefficients test to detect significant differences in model coefficients where appropriate (Paternoster, Brame, Mazerolle, & Piquero, 1998). To better characterize age-based patterns in intraindividual variability, we test alternative functional forms of age for each race/ethnicity. Based on preliminary analyses (not shown), the age-based patterns of intraindividual variability are best characterized by a quadratic function of age for Whites and Blacks. For Hispanics, age is not a significant predictor of intraindividual variability. We then retain the most parsimonious linear age function for this group.
For both the trajectory and the prediction models, we use a two-stage Heckman selection bias model to correct parameter estimates for nonrandom selectivity caused by panel attrition (Heckman, 1979). In our analytic sample, about one fifth of the sample died (18%, n = 1,389) and one quarter (25%, n = 1,929) missed at least one interview for reasons other than death. Preliminary analyses (not shown) suggest that racial/ethnic minority respondents in the sample have significantly higher rates of panel attrition. To account for this, we calculate two hazard-rate selection instruments (λ) for mortal and nonmortal attrition and include them in the trajectory and prediction models as covariates (Stolzenberg & Relles, 1997). In addition, models were not weighted or adjusted for sample clustering, due to the need to maintain statistical power afforded by the racial/ethnic oversamples in the HRS.
Results
We begin by describing our sample. Table 1 presents means and standard deviations (SDs) of study variables for the total sample and for each race/ethnicity. For all respondents, the average score of functional limitations at Wave 3 is 2.19 (SD = 3.00). Over time, respondents become increasingly functionally limited. Black and Hispanic adults have significantly higher levels of functional limitations than do White adults at all waves. Black and Hispanic adults are not significantly different from each other with regard to functional limitations at each interview.
Means and Standard Deviations (in Parentheses) of Study Variables for White, Black, and Hispanic Adults Aged 55 and Over: HRS Cohort, Health and Retirement Study (1996–2010).
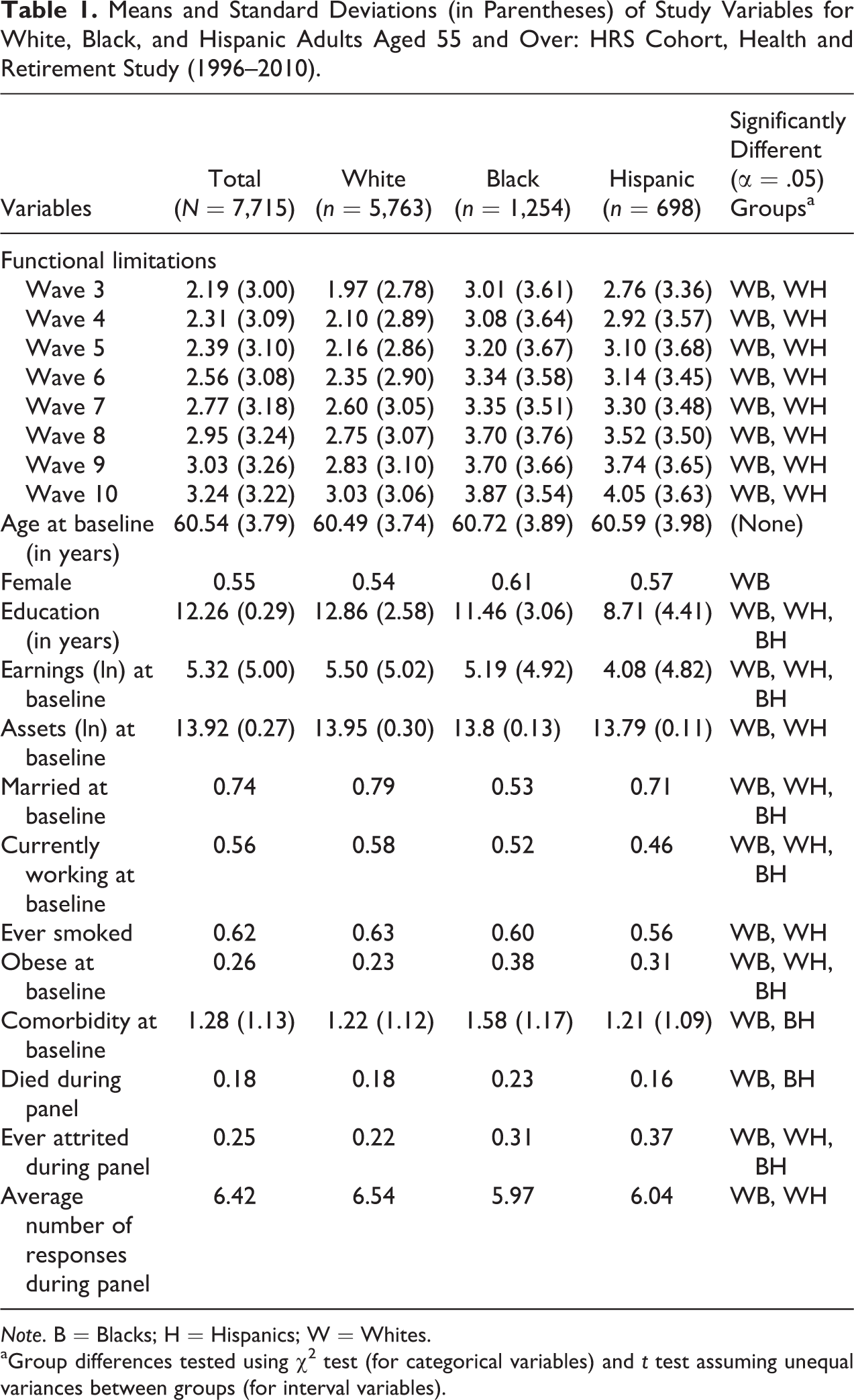
Note. B = Blacks; H = Hispanics; W = Whites.
aGroup differences tested using χ2 test (for categorical variables) and t test assuming unequal variances between groups (for interval variables).
No racial/ethnic difference exists in baseline age. Proportion of women is higher among Black adults (0.61) than that among White adults (0.54), probably due to a disproportionately higher degree of premature mortality of Black men prior to the observation window. White adults have on average about 1.4 years more of education than Blacks and about 4 years more of education than Hispanics. Blacks and Hispanics also have lower levels of earnings and fewer assets than do Whites. A smaller proportion of racial/ethnic minority adults are married or working compared to their White counterparts. White adults have however the highest proportion of smokers (0.63). About one third of the racial/ethnic minority adults are obese (0.38 and 0.31 for Blacks and Hispanics, respectively), whereas only one fourth of the White adults are so. Black adults have an average of 1.58 (SD = 1.17) chronic conditions at baseline, compared to 1.22 (SD = 1.12) for White and to 1.21 (SD = 1.09) for Hispanic adults.
The next step of the analysis is to examine if intraindividual variability in trajectory of functional limitations varies by race/ethnicity. Table 2 presents findings from the trajectory models specifying homoscedastic (Model 1) and heteroscedastic Level-1 residuals by race/ethnicity (Model 2). We first discuss the results from Model 1. For all respondents, functional limitations increase by 0.104 (SE = .018, p < .001) every 2 years. Black adults, on average, have greater functional limitations than White adults (b = .240, SE = .073, p < .001). Hispanic adults, however, are not significantly different from their White counterparts with respect to functional limitations trajectory (b = .108, SE = .099, p > .05). Gender, SES, marital status, working status, smoking, obesity, and comorbidity are all significantly associated with functional limitations in expected directions.
Multilevel Mixed-Effects Models Predicting Wave-Based Trajectories Functional Limitations Among White, Black, and Hispanic Adults Aged 55 and Over: HRS Cohort, Health and Retirement Study (1996–2010).a
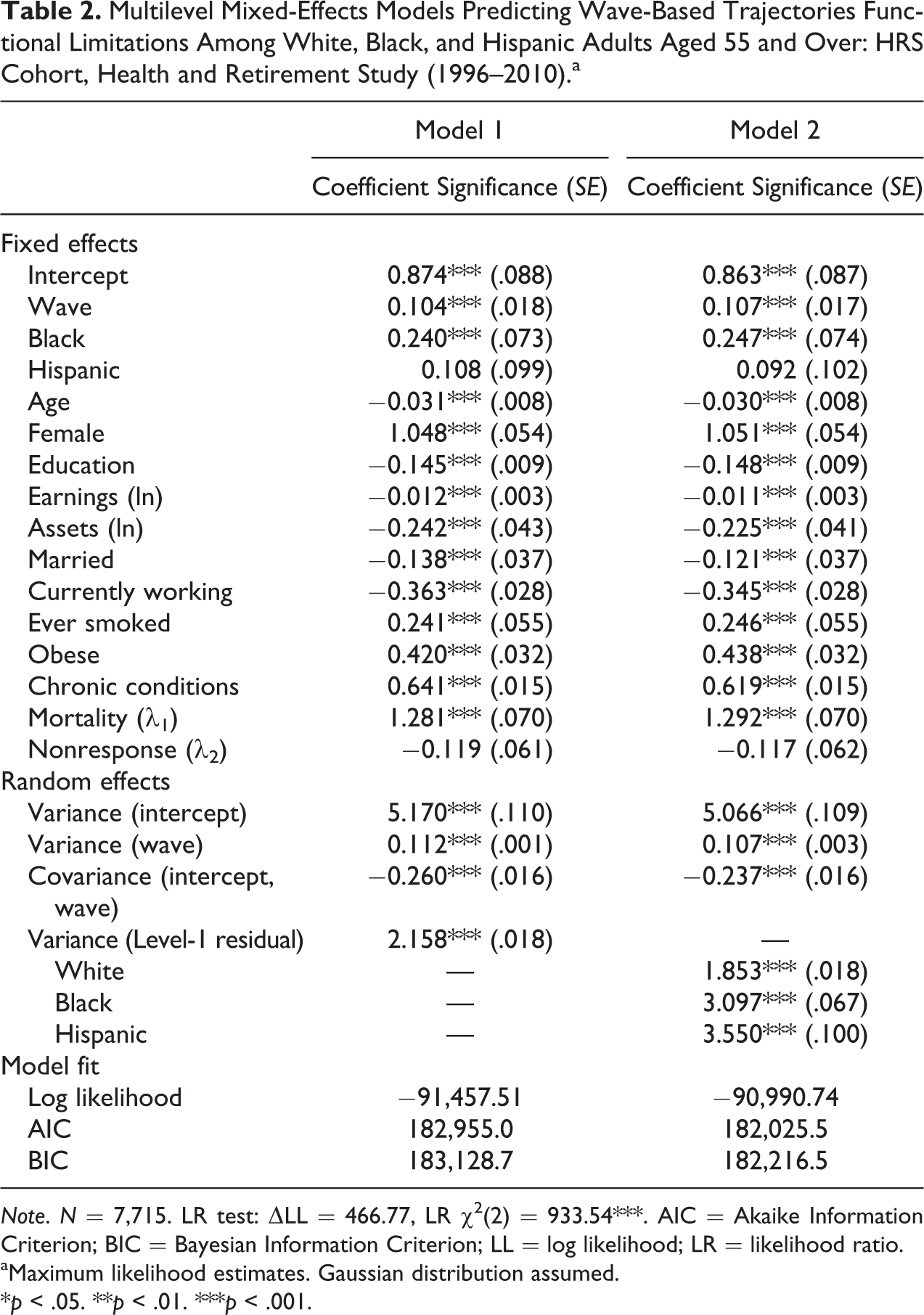
Note. N = 7,715. LR test: ΔLL = 466.77, LR χ2(2) = 933.54***. AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; LL = log likelihood; LR = likelihood ratio.
aMaximum likelihood estimates. Gaussian distribution assumed.
*p < .05. **p < .01. ***p < .001.
Almost all predictors in the fixed-effects equation exhibit significant, sizable effects on functional limitations, yet we note that there is a substantial amount of intraindividual variability left unspecified in this model. The estimated variance of Level-1 residual is 2.158, indicating that, even after accounting for covariates, the typical deviation of a response from the model implied individual mean is about 1.5. Substantively, this means some difficulty in performing up to two functional tasks or a lot of difficulty in performing one task.
Turning to Model 2, we estimate a trajectory model with the same set of predictors in the fixed-effects equation as in Model 1, allowing the variances of Level-1 residuals (i.e., intraindividual variability) to be racially/ethnically specific. The estimated variance of Level-1 residuals is remarkably different for each racial/ethnic group. White adults have the least amount of intraindividual variability in trajectories of functional limitations (
To test if the model implied racial/ethnic differences in intraindividual variability is statistically significant, we compare model fit statistics across Models 1 and 2. Model 2 yields smaller Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) as well as a larger log likelihood (LL). The LR test confirms that Model 2 is a better fit (ΔLL = 466.77, LR χ2 = 933.54, p < .001), providing evidence that the racial/ethnic difference in estimated variances of Level-1 residual is statistically significant. Collectively, these results suggest that intraindividual variability in functional limitations is present for all race/ethnicity and that the degree of intraindividual variability is greater for Black and Hispanic adults.
We now turn to substantive models examining the age and social patterns of intraindividual variability in functional limitations for each race/ethnicity. These models use extracted Level-1 residual estimates from Model 2 in Table 2 as the outcome variable. Table 3 presents findings for Whites, Blacks, and Hispanics, respectively, with baseline functional limitations, age, SES, and covariates predicting intraindividual variability in functional limitations over time. We use an equality of coefficients test to determine if the effect of any predictor on the outcome differs by race/ethnicity.
Age Patterns of Intraindividual Variability (ln) in Trajectories of Functional Limitations by Race/Ethnicity: HRS Cohort, Health and Retirement Study (1996–2010).a
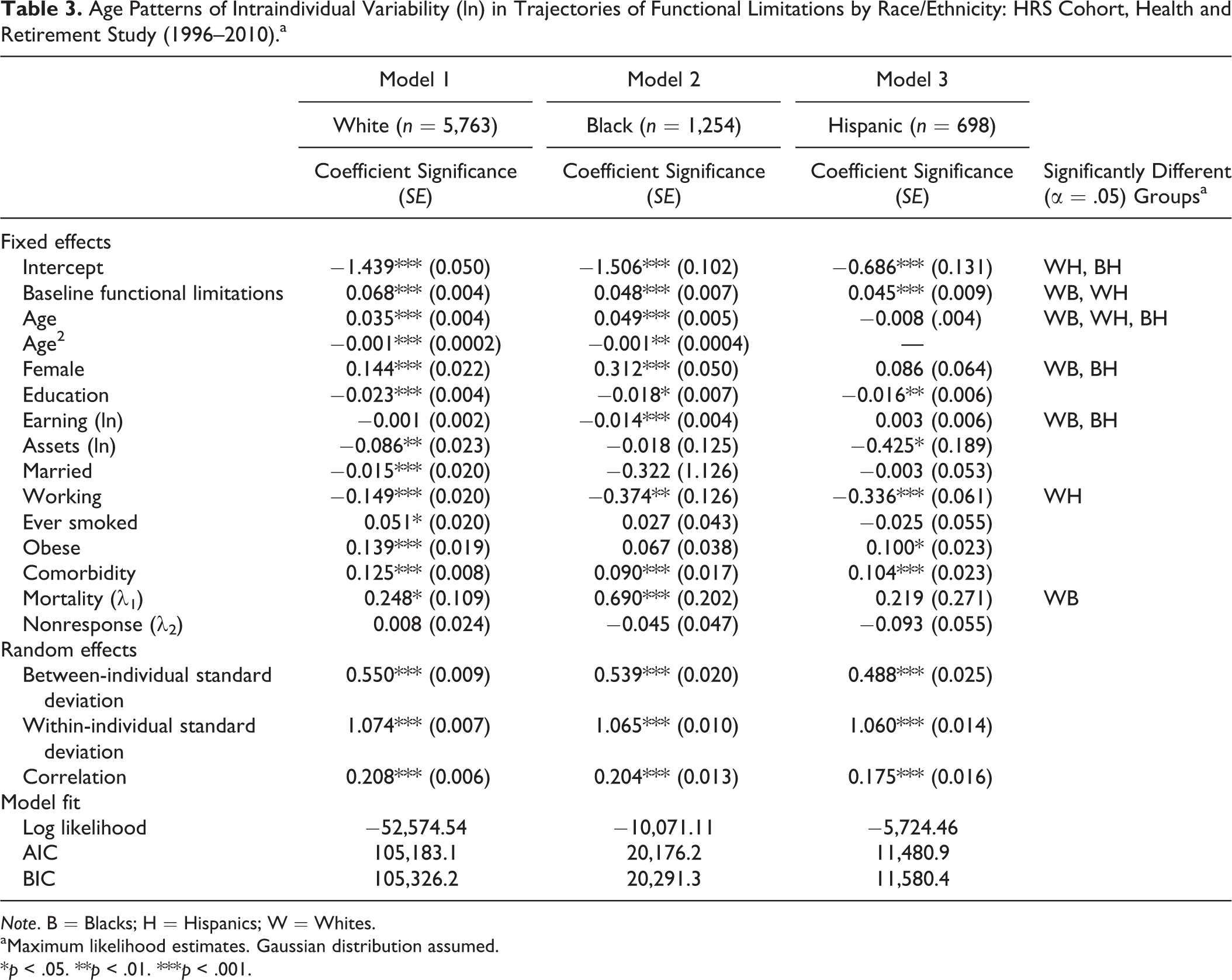
Note. B = Blacks; H = Hispanics; W = Whites.
aMaximum likelihood estimates. Gaussian distribution assumed.
*p < .05. **p < .01. ***p < .001.
For all race/ethnicity, individuals with higher levels of functional limitations at baseline show more fluctuations over time. The effect of baseline functional limitations on intraindividual variability is significantly greater for White (b = .068, SE = .004, p < .001) than for Black (b = .048, SE = .007, p < .001) and Hispanic adults (b = .045, SE = .009, p < .001).
Based on preliminary results (not shown), we specify a quadratic age function to characterize age-based patterns in intraindividual variability in functional limitations for White and Black older adults and a linear age function in the model for Hispanic adults. Intraindividual variability increases with age (b = .035, SE = .004, p < .001) at a decelerating rate (b = −.001, SE = .0002, p < .001) for Whites. Similarly, there is a systematic age-based increase in intraindividual variability for Black adults (linear slope b = .049, SE = .005, p < .001; quadratic slope b = −.001, SE = .0004, p < .01), and such increase is significantly greater among Blacks. Accounting for covariates in the model does not explain the significant age-based increase in intraindividual variability for White or Black adults. Hispanics on average have the greatest intraindividual variability in functional limitations than do White or Black adults, but there is no age-base pattern. Figure 1 illustrates the age-based patterns for each racial/ethnic group, based on results from Table 3.
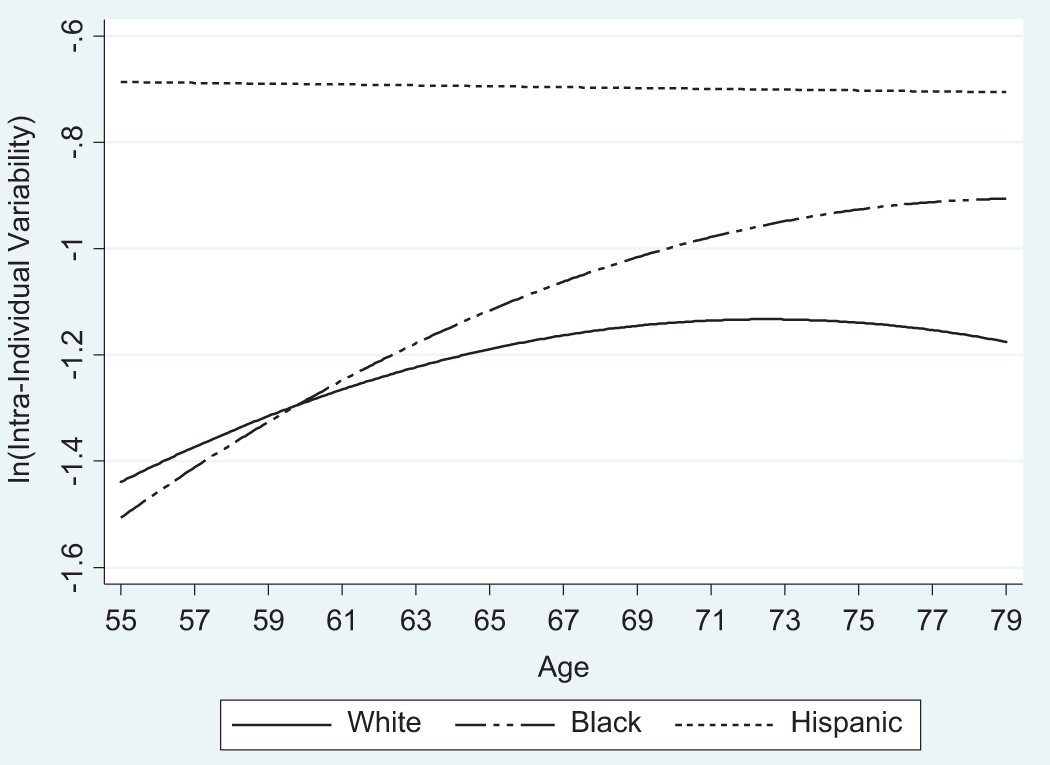
Fixed-effects estimates of age-based patterns of intraindividual variability (ln) in trajectories of functional limitations by race/ethnicity: HRS Cohort, Health and Retirement study (1996–2010).
Turning to SES, we found patterns of intraindividual variability by SES as well as some racial/ethnic difference in these SES patterns. In general, higher levels of SES are associated with less intraindividual variability. More years of education are associated with less intraindividual variability for race/ethnicity. Specifically, for White adults, intraindividual variability (ln) decreases by 0.023 (SE = .004, p < .001) for each additional year of education. The amount of decrease in intraindividual variability (ln) per unit increase in education is 0.018 (SE = .007, p < .05) for Black adults and 0.016 (SE = .006, p < .01) for Hispanic adults. There is however no significant racial/ethnic difference in such education effect. Individual earning is a significant predictor of intraindividual variability for Blacks only (b = −.014, SE = .004, p < .001), whereas assets are associated with intraindividual variability only for Whites (b = −.086, SE = .023, p < .001) and Hispanics (b = −.425, SE = .189, p < .05).
White adults who are married tend to have less intraindividual variability over time in functional limitations (b = −.015, SE = .020, p < .001). Marital status however does not have an effect on intraindividual variability for Black or Hispanic adults. Individuals who are currently working have significantly less intraindividual variability regardless of race/ethnicity (White: b = −.149, SE = .020, p < .001; Black: b = −.374, SE = .126, p < .001; Hispanic: b = −.336, SE = .061, p < .001). With regard to health and health-related behaviors, ever smoked is associated with greater intraindividual variability only for Whites (b = .051, SE = .020, p < .05). Obesity is associated with greater intraindividual variability for Whites (b = .139, SE = .008, p < .001) and Hispanics (b = .100, SE = .023, p < .001), yet such effect is nonsignificant for Blacks. Higher levels of comorbidity are associated with greater intraindividual variability for all race/ethnicity (White: b = .125, SE = .008, p < .001; Black: b = .090, SE = .017, p < .001; Hispanic: b = .104, SE = .023, p < .001) and no racial/ethnic difference is found in this effect.
In addition, White and Black older adults with greater hazard of death during panel tend to have greater intraindividual variability in functional limitations and such an association is significantly stronger for Blacks (b = .690, SE = .020, p < .001) than for Whites (b = .248, SE = .109, p < .001). The hazard of nonresponse during panel is not significantly associated with intraindividual variability for any racial/ethnic group.
Discussion
In recent years, the weathering hypothesis has garnered considerable attention among social scientists studying late-life health disparities and minority aging (Geronimus, 2001; Thorpe & Kelley-Moore, 2013). Linking institutionalized racism and other structural barriers to accumulated stress, the weathering hypothesis provides a plausible framework for understanding the physiological consequence of social inequalities as minority adults age. However, few studies utilizing this explanatory framework have considered instability in health status as a second consequence of such accumulated stress for racial/ethnic minorities. To date, most empirical investigations in this line of inquiry have been concerned with average differences between racial/ethnic groups, as the primary—if not the only—empirical evidence for the influence of social disadvantage on health and aging outcomes (Brown et al., 2012; Haas & Rohlfsen, 2010; Johnson, et al., 2012; Kelley-Moore & Ferraro, 2004; Kim & Durden, 2007; Kim & Miech, 2009; Shuey & Willson, 2008; Taylor, 2008; Walsemann, et al., 2008; Warner & Brown, 2011; Wickrama et al., 2013; Yang & Lee, 2009). Our study moves the conversation forward regarding weathering and late-life racial/ethnic health disparities, by focusing on a source of health heterogeneity that has largely been overlooked in prior literature.
Based on an empirical examination of the racial/ethnic patterning in intraindividual variability in late-life functional limitations, our study suggests further nuances to the weathering hypothesis. The same mechanisms of social inequality that generate early onset of disease and faster health deterioration between groups’ average trajectories also contribute to greater fluctuations in physical function as minority adults age. White adults maintain relatively good and stable functional status over time, as evident in their lower levels of functional limitations on average and smaller intraindividual variability over time. Black and Hispanic older adults’ physical function, in contrast, is characterized by significantly greater fluctuations over time. This finding suggests that social disadvantage and related stress exposure can compromise one’s physiological capacity and make his or her physical functioning more sensitive to social environmental influences. For example, an individual who is already functionally limited is, at the same time, more likely to seek care or utilize compensatory mechanisms, which may result in temporary recoveries. However, limited resources, irregular access to health care, and the inconsistent quality of care can continue to trigger repeated onsets of functional limitations.
We found an age-based increase in intraindividual variability in functional limitations for both White and Black older adults. Such increase with age is even faster for Blacks, evidence of accumulative mechanisms that exacerbate racial-health disparities over time. Some of these patterns may indeed be associated with SES and comorbidity, since these factors are all significant predictors of intraindividual variability in functional limitations. However, the age-based increases in intraindividual variability among Whites and Blacks remain significant, in spite of accounting for SES and comorbidity. This may suggest novel, unrecognized mechanisms of racial/ethnic inequality that operate over the life course or, alternatively, new empirical ways to theorize and characterize extant mechanisms and pathways. As researchers continue to disentangle these aspects of inequality, it is important to recognize that the empirical manifestations of social disadvantages, especially those that are more closely related to the lived experience of minority older adults are not necessarily limited to average differences between racial/ethnic groups. Future research should consider using intraindividual variability in health measures as the study outcome when examining factors and mechanisms that are hypothesized to result in disparities.
Our findings suggest no difference between White and Hispanic older adults in trajectories of functional limitations. We however found that Hispanics had the greatest intraindividual variability of all three racial/ethnic groups in the study, a finding that would have been masked if average differences were the only focus of the inquiry. Furthermore, the lack of age patterning in intraindividual variability for Hispanics may indicate unique functional dynamics for this group, or alternatively, the possibility that extant measures of functional limitations do not capture their physical functioning well, resulting in greater measurement errors and biases. Since our analysis does not identify subgroups of Hispanics due to the need to maintain sufficient statistical power, it is also possible that patterns of intraindividual variability differ across these subgroups. Future research should look into all three possibilities to further disentangle the dynamics of late-life functional changes for Hispanics.
Characterizing a race/ethnic group by their average health status obscures not only interindividual variability within groups but intraindividual variability within persons. Consistent with Verbrugge and colleagues (1994), we found that individuals’ functional status could be more variable over time than they are different from one another. Based on our estimates, the average difference in trajectories between Blacks and Whites is about a quarter of a unit yet at any given time point, their functional status could fluctuate by up to three units. As a result, empirical work relying solely on average differences between subgroups may have led to a biased interpretation toward independent race/ethnicity effects. The variability that is not adequately captured by averages indicates a missed opportunity for empirical research to characterize specific biological, behavioral, and sociostructural circumstances that contribute to such variability and identify compensatory mechanisms for intervention.
Similarly, with an exclusive focus on the average rate of change, researchers may conclude that for a given factor, mechanism or intervention decreases racial/ethnic inequality when it “slows down” the average rate of functional decline. If, however, the phenomenon of “slowing down” is accompanied by an increase in fluctuations over time, it would in fact caution against a conclusion of converging racial/ethnic inequality. For public health practice, it is then important to incorporate systematic measurement of intraindividual variability in health to complement average differences when evaluating the long-term stabilizing effect of an intervention targeted at health problems among racial/ethnic minorities.
Our study has two limitations. First, although the HRS has oversampled Hispanic adults, we cannot further identify subgroups of Hispanics without compromising the statistical power in current analysis. Functional dynamics and patterns of intraindividual variability may be different across these subgroups. In particular, the lack of age patterning in intraindividual variability for Hispanics in our results calls for research designs that can tease out possible subgroup variations within Hispanics, in order to provide a clearer documentation of functional changes for this group.
Second, our estimation of intraindividual variability over time is conservative, due to the spacing of measurement occasions in the HRS. The HRS is designed to only interview respondents every 2 years. We cannot capture fluctuations that happened inbetween these biannual assessments. This means that the actual degree of intraindividual variability may be even greater, especially for racial/ethnic minority adults. Future research should take into account how the spacing of panel interviews would bias estimates and explore alternative design and analytic options to capture intraindividual variability more adequately.
Despite the limitations, our findings highlight the conceptual and empirical gains by taking into account patterns of intraindividual variability in studies of racial/ethnic disparities in late-life physical function. Instead of being statistical noise in measurement, intraindividual variability represents an arena for further theorizing the influence of the social environment on individual aging and complementing the explanatory framework of the weathering hypothesis. Various mechanisms of social inequality that have been shown to account for racial/ethnic minority adults’ earlier onset of disease and faster health deterioration also contribute to their greater instability at older ages. Future research should explore mechanisms of social disadvantage that result in patterns of intraindividual variability in other health outcomes.
Conclusion
In this study, we begin by considering instability in physical function as, potentially, a second consequence of accumulated stress to complement current understanding of the weathering mechanism. Accordingly, we found that intraindividual variability in trajectories of functional limitations exhibited distinct age and racial/ethnic patterning—evidence of a new empirical manifestation of inequality-generating mechanisms underlying observed racial/ethnic health disparities. Our findings open a new vista of inquiry regarding racial/ethnic disparities in more broadly defined late-life health dynamics, which is crucial to testing the weathering hypothesis and other prevailing theories of aging.
Footnotes
Authors’ Note
This research was primarily conducted while the first author was at Case Western Reserve University. The opinions expressed in the article are the authors’ own and do not reflect the official views of the National Institutes of Health, the Department of Health and Human Services, or the U.S. Government.
Acknowledgments
We thank Dale Dannefer, Eva Kahana, Christopher Marcum, and the anonymous reviewers for their comments and suggestions on earlier drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by an Advanced Study Fellowship via Department of Sociology at Case Western Reserve University and a National Institutes of Health Intramural Research Training Fellowship (Z01HG200335).