
Abstract
Objective:
We examined cumulative and differential experiences of aging in place.
Method:
Data came from the 2002 and 2010 wave of the Health Retirement Study. We modeled the trajectory of later-life depressive symptoms, and how senior-housing environments moderate the negative association between economic disadvantages and depressive symptoms.
Results:
At baseline, economically disadvantaged older adults were more likely to exhibit depressive symptoms. However, detrimental effects of income group (non-low income vs. moderate income; non-low income vs. low income) on depressive symptoms did not significantly change over time. The age-leveler hypothesis may account for nonsignificant effects of disadvantaged income groups over time.
Discussion:
Findings suggest that moderate-income seniors may experience positive differentials if they age in place in a supportive senior-housing environment. Moderate-income seniors may have broader opportunities in senior housing compared to private-home peers. Senior housing might partially counter risks such as low mental health, emerging from life-course disadvantage.
The concept of aging in place integrates age-related processes at individual, environmental, and societal levels; it is the preference of most older adults (Cutchin, 2003) and, some suggest, contributes to most positive aging outcomes (Pastalan, 1990). Aging in place literature equates place with home—a living environment ranging from specific residences to surrounding neighborhoods and broader communities (Black, 2008). It has been increasingly adopted in policies and programs designed to address rising long-term care costs.
This study addresses several gaps in the aging in place literature. Little extant research has examined the longitudinal effects of aging in place. From the life-course perspective, aging in place is a dynamic, heterogeneous process over the life course embedded in an individual’s institution, culture, and society (Elder & Shanahan, 2006). An aging individual’s health and behavior at any point partially reflects an accumulation of experiences over the life course; new factors, or constellations of new factors, may emerge in different phases of old age and influence how a person adapts (Baltes, 1987). Most existing aging in place studies are cross sectional and limited in their ability to make causal arguments about aging in place facilitators and inhibitors.
A second literature gap exists in knowledge of heterogeneous aging in place experiences. The person–environment (P-E) fit perspective posits that unique combinations of personal needs and resources, together with environmental characteristics, determine an individual’s adaptation (Wahl, Iwarsson, & Oswald, 2012). Previous P-E fit research has focused on health deterioration and increased frailty as old-age vulnerabilities. However, poor health is only one source of old-age vulnerability; others include race/ethnic minority status, low socioeconomic status (SES), and loss/absence of social support (Grundy, 2006). Low-SES older adults are particularly vulnerable, given limited postretirement financial resources and the cumulative disadvantages of lower income, education, and previous lower grade professions (Corna, 2013). Knowledge of patterns and associations regarding socioeconomic vulnerability and environmental risks/resources in old age would provide much-needed information for targeted, effective aging in place programs and interventions.
We focus on an understudied living environment in aging in place literature: senior housing. Once the initial move takes place, senior housing helps older adults age in place and often bridges conventional independent living and long-term institutional care residence (Stone, 2013). Senior housing for low-income elders is recognized as an underutilized resource for looming health-care issues affecting vulnerable subgroups (Handy, 2012). To date, however, limited research examines whether, and to what extent, senior housing supports aging in place for these subgroups.
Using the life-course and P-E fit perspectives, the present study examines aging in place as a process that is cumulative over time and differential across individuals with different personal and environmental conditions. We measure the person dimension by focusing on income status as one aspect of an older adults’ economic vulnerability and the environmental context by examining senior-housing residency in contrast to conventional, private-home dwelling. To gauge aging in place, we focus on depressive symptoms as one aspect of well-being. We examined depressive symptoms considering the significant implication for aging policy and program development. As a public health concern, the significance of depressive symptoms in the later years has been linked with a wide range of outcomes in old age such as impairment in daily functioning, quality of life, and life expectancy as well as higher risk of hospitalization (Abrams, Lachs, McAvay, Keohane, & Bruce, 2002; Blazer, 2003; Wada et al., 2005). A growing body of P-E fit research has shown that various aspects of the environment are related to well-being among low-income older adults (Lehning, Smith, & Dunkle, 2012; Park & Lee, 2016). Although depressive symptoms could be caused by various risk factors, based on the P-E fit model, this study focuses on economic vulnerability as a person dimension and senior housing as an environment dimension, which independently and jointly influence depressive symptoms in old age.
Specifically, this study asks the following: “What is the role of economic vulnerability and senior housing residence in the trajectory of depressive symptoms?” and further, “Is there evidence of P-E fit—measured by the interaction between income group status and senior housing residence—in the trajectory of depressive symptoms?”
Enhanced understanding of P-E fit dynamics between person and environment and how P-E fit affects well-being over time will inform aging in place policy and program development by identifying modifiable components of aging in place. We first describe the existing literature base concerning the longitudinal effects of economic vulnerability on mental health, particularly depressive symptoms, and the differential effects on aging in place with regard to senior housing grounded on the P-E perspective.
Longitudinal Aging in Place: A Life-Course Perspective
Socioeconomic disadvantage and later-life depressive symptoms
Disadvantaged SES is a major determinant of health and well-being in old age. The life-course perspective adds a longitudinal aspect asserting that early (dis)advantage tends to accumulate over time. SES levels have direct causal relationships with future SES levels, thereby increasing heterogeneity in rates of illness, disability and death, and worsening well-being (Dupre, 2007). Compelling longitudinal evidence indicates that SES inequalities in health widen across the life course. For example, prior work has shown patterns of persistent or increasing socioeconomic inequalities in old-age morbidity and mortality (Huisman, 2004; McMunn, Nazroo, & Breeze, 2009). Conceivably, such evidence from longitudinal studies suggests that low SES may not only affect the level of depressive symptoms in old age but also influences depressive symptoms over time, as earlier SES disadvantage associated with limited social resources and steady cognition decline may increase risk of subsequent health problems (Chen, Chiao, & Ksobiech, 2014).
Surprisingly few longitudinal studies explore changes in later-life depressive symptoms among socioeconomically vulnerable elders. A strong association between low SES and higher levels of depressive symptoms is well recognized (Back & Lee, 2011; Bjelland et al., 2008; ). Previous research has indicated a potential age dependency of socioeconomic effects on mental health (Miech & Shanahan, 2000) and that the effects of class differences in mental health may increase with age (Chandola, Ferrie, Sacker, & Marmot. 2007). These studies, however, have been primarily cross sectional in design and have found increases in depressive symptoms by comparing age-groups; they cannot make causal arguments about changes in late life depression.
Despite strong theoretical foundations on the longitudinal effects of SES on mental health, empirical evidence among existing studies seems equivocal. Chen, Chiao, and Ksobiech (2014) examined whether socioeconomic disadvantage and perceived midlife social support were associated with subsequent depressive symptoms among older Taiwanese women. During the 12-year observed period, they found older, socioeconomically disadvantaged women were more likely to have higher initial levels of depressive symptoms, but low SES did not exacerbate depressive symptoms over time. Green and Benzeval (2011) examined social class differences in anxiety and depression at five points over 20 years. Findings showed class differences increased over time: Low SES participants, compared to non-low SES participants, were likely to have more rapid rates of depression increase.
Differential Aging in Place: P-E Fit Perspective
Socioeconomic disadvantage as person dimension
Most existing environmental-perspective research examines health conditions (Wahl, Fange, Oswald, Gitlin, & Iwarsson, 2009). Although deterioration of health is one of the primary developmental risk factors that accompany aging, it is only one of many sources of vulnerability in old age. Three factors place low-income elders at higher risk of challenges to successful aging in place: relatively worse health conditions (chronic conditions, physical, and cognitive impairment), poorer housing conditions (physical deficiencies, outdated equipment), and insufficient financial resources to modify housing features or access supportive services (Bates & Fasenfest, 2005). Increasingly, low-income elders face higher risk of premature or avoidable nursing-home placement due to inadequate residential environments (Spillman, Biess, & MacDonald, 2012). We must address the challenges low- and moderate-income elders face in finding and maintaining affordable, stable housing that adapts to changing needs (Stone, 2013).
Senior housing as an alternative environment
From a policy perspective, it is important to examine if and to what extent environmental contexts, as modifiable resources, are associated with low-income elders’ disadvantage. Low-income elders may enjoy better quality of life and more independent lifestyles when they can relocate to supportive housing arrangements, such as affordable senior rental housing (Golant, 2008). Much aging in place discourse has developed in the conventional, private-home context, examining risk, and protective factors affecting health and well-being. In this study, we examine senior housing broadly defined—noninstitutional settings that support independent living by providing or arranging for services to meet residents’ evolving needs.
The limited empirical knowledge on how senior housing supports aging in place tends to conflict. Relocation literature, for example, suggests moving into senior housing can be a stressful and even harmful event causing various negative outcomes for older individuals including poorer health, higher health-care costs, increased risk of institutionalization, and increased morbidity and mortality (Bekhet, Zauszniewski, & Nakhla., 2009; Bradley & Willigen, 2010). Others suggest that senior-housing residents generally adapt well, leading to a better quality of life as indicated by independence, friendships, services, and safety (Portacolone & Halpern, 2014: Rossen & Knafl, 2007).
P-E fit suggests an older adult is more likely to experience improved outcomes in an environment congruent with his or her physical and cognitive abilities and emotional needs (Lawton, & Nahemow, 1973). The central proposition of P-E fit, the environmental docility hypothesis, posits that individuals with less competence are more affected by the same environmental demands or resources than individuals with more competence. In this hypothesis, low-SES elders would be positively affected by senior-housing environments compared to their peers in conventional-home environments. They also might benefit more from supportive senior-housing environments than less-disadvantaged elders.
Limited research has examined if and to what extent senior housing supports aging in place for vulnerable subgroups of elders, particularly low-income elderly. Focusing on vulnerable older people (limited income and limited mobility) aged 75 and older in age-segregated housing, Davidson, Brooke, and Kendig (2001) concluded that senior-housing residents had more friendship interaction than counterparts in age-integrated private housing, leading to higher self-esteem and life quality. Studies of subsidized housing programs that link housing and services for low-income elders found reduced anxiety and depression and improved personal control and psychological well-being (Levine & Johns 2008; Sheehan & Guzzardo 2008) and a greater sense of safety and security (Mollica & Morris, 2005). Rare empirical studies have compared aging in place among low-income elders in senior-living environments and conventional homes. One study compared change in functional health status among comparable groups of low-income older adults, comparing those living in conventional, private homes with those in an affordable assisted-living facility (Fonda, Clipp, & Maddox, 2002). Findings suggested that subsidized assisted-living environments enabled low-income residents to maintain function and/or cope well with functional decline (Fonda, Clipp, & Maddox, 2002).
Existing research focused on senior housing shares several important limitations: First, little work examines the extent to which senior housing affects changes in health and well-being (for a review, see Golant, Parsons, & Boling, 2010). Second, most extant studies are based on pilot programs or small sample surveys within particular geographic areas (Golant et al, 2010). More importantly, to the best of our knowledge, no known study examines the effects of senior-housing residence among a nationally representative sample from a longitudinal perspective.
Present Study
Drawing on life-course and the P-E fit perspectives, we explore aging in place conceptualized as an aging process at a site that involves varying degrees of “fit” between person and environment leading to differences in well-being over time. To measure the person dimension, we focus on poverty status, since many social policies and programs use the federal poverty level (FPL) as an eligibility criterion. To measure environmental context, we examine senior-housing residency in contrast to conventional, private-home dwelling. To gauge aging in place, we focus on depressive symptoms as an aspect of adaptation. Although environmental contexts such as neighborhood have received increased attention as related to mental health outcomes such as depressive symptoms (cf. Yen, Michael, & Perdue, 2009), no known study has examined the extent to which vulnerable elders’ depressive symptoms differ by senior-housing residence over time.
We first explore the extent to which income status and senior housing are independently associated with depressive symptoms. Based on the life-course perspective, we expect lower SES to predict a higher level of depressive symptoms both initially and over time. Second, to empirically examine the P-E fit or differential aging in place, we assess the extent to which senior-housing residence moderates the effects of low SES on older adults’ depressive symptoms. Guided by the environmental docility hypothesis, we hypothesize that lower income individuals, when residing in a senior-living environment, are likely to have better outcomes compared to their peers in conventional homes. As this is the first attempt to examine longitudinal P-E fit among economically vulnerable elders in senior housing, we set no specific hypothesis. Still, we expect that the possible compensating role of senior housing for vulnerable elders will hold over time.
Method
Data and Sample
Five waves of data (2002–2010) from the Health and Retirement Study (HRS), in combination with RAND Center for the Study of Aging (RAND HRS) data, were used in this study. The HRS is a prospective cohort study conducted by the University of Michigan with support from the National Institute of Aging. RAND HRS data include RAND’s collection of detailed health, behavioral, and demographic information and the use of bracketing methods to minimize nonresponse (RAND HRS, 2008). Details of multistage sample design, selection criteria, implementation, and response rates are available elsewhere (Sonnega, 2014). Study baseline is the 2002 wave. Since 2002, RAND HRS has included a poverty measure based on U.S. Census Bureau poverty threshold levels and family composition.
We used four criteria to draw our sample: First, we selected adults aged 75 and older at baseline to focus on very-old older adults (Neugarten, 1996; Nygren et al., 2007), eliminating young older adults who relocate to senior housing for amenities rather than adaptation for old-age losses and limitations (Lovegreen, Kahana, & Kahana, 2010) and accounted for low-income elders living in conventional private housing who are more likely to be under 75 (Golant, 2008). Second, respondents who were institutionalized or unable to independently answer survey questions were excluded. Third, the sample was restricted to respondents who provided housing-related information. Fourth, since we modeled the trajectory of outcomes over time, the sample was limited to those who participated in at least three time points during the study period. Since depressive symptoms among individuals in the same household may be interdependent, we included only one respondent from each household to ensure statistical independence among observations. This random selection procedure is particularly necessary because compared to those living in traditional private homes, senior-housing residents’ daily experiences such as social relations and social activities tend to be limited within their senior-housing community, resulting in stronger interdependence of mental health. Lastly, individuals with a depressive symptoms score of 4 or higher at the baseline were excluded to avoid reverse causality.
We used the HRS recommended cutoff point of 4 or higher that approximates the traditional cutoff point of 16 or higher for the original 20-item Center for Epidemiologic Studies–Depression (CES-D) Scale that indicates a high likelihood of clinical depression.
The above restrictions resulted in a sample of 9,638 observations, after removing 110 cases (1% of sample) missing information covariate information. In this study, we build a series of hierarchical models to examine the role of theoretical constructs in the P-E fit perspective. Since data with multiple imputations are not technically feasible for testing nested models in Stata, we dropped observations missing covariates. We ran identical hierarchical models with multiple imputed data without testing nested modeling; results were essentially the same. To control for bias introduced by missing data due to death, we include attrition and death information as covariates; retention of healthier respondents over time in longitudinal analyses can lead to biased results that favor more robust survivors and show narrowing health differences by SES.
Data were obtained from respondents between 2002 and 2010, with up to five repeated observations obtained over the 8 years. The sample contains 2,393 respondents and 9,523 observations. Of respondents, 21% participated in three waves, 27% in four, and 52% in all five waves. All descriptive analyses were weighted to adjust for differential probabilities of sample selection. We did not weight regression analyses because sampling was a function of independent variables included in the model, producing unbiased coefficients and standard errors (Winship & Radbill, 1994).
Measures
Low-income status
To focus on vulnerable SES groups, we used income status. Indicators of SES also include education and occupation. Prior work, however, suggested that for older adults in particular, education and occupation may not be suitable indicators of socioeconomic disadvantage as most people aged 65 and over are retired and education reflects early life achievements (Matthews, Smith, Hancock, Jagger, & Spiers, 2005). Research findings have suggested income is a more appropriate measure of deprivation, as older adults are often cash poor with fixed income (Rendall & Speare, 1995), and it is a reasonable indicator of poverty as measured by the gap between a person’s needs and income (O’Reilly, 2002). Following the low-income definition used in previous literature (Spillman et al., 2012), we categorized income status into three groups: Those with income levels higher than 300% of FPL were coded as non-low income (0); between 185% and 300% of FPL as moderate income (1); and below 185% of FPL as low income (2). At the national level, FPL corresponds to roughly 80% of area median income, the low-income threshold used by the U.S. Department of Housing and Urban Development.
Senior-housing residency
Senior-housing residency in HRS was measured with one question “Is your (house or apartment) part of a retirement community, senior citizens’ housing, or other type of housing that offers services for older adults or someone with a disability?” Senior-housing data were aggregated across earlier study waves and updated with information on new move-ins in 2008. The HRS uses extensive skip patterns for housing-related variables. In general, only new respondents or those who indicated moving were asked to provide new information about housing environment. Therefore, values for senior-housing information were hierarchically assigned for those entering the study prior to 2010. A binary indicator was used to measure senior-housing residency (0/1).
Outcomes
Depressive symptomology
We measured depressive symptoms using 8 items from the abbreviated CES-D. Six of the 8 indicators measured whether respondents experienced any of the following negative sentiments over the preceding week: depression, everything being an effort, restless sleep, feeling alone, feeling sad, and could not get going. Two items measured experiences of feeling happiness and enjoyment of life and were reverse coded (range = 0–8).
Covariates
We included a number of sociodemographic covariates: Age cohort groups (aged 75–84 = 0, 85 years and above = 1), current marital status (not married = 0, married = 1), wealth (1 = lowest, 3 = highest tertiles), gender (women = 1, men = 0), education (less than high school = 0, high school = 1, some college = 2, and college graduate = 3), and race (White = 1, non-White = 0). In addition, guided by the P-E fit perspective, we included additional covariates in the person and environment dimensions that have been identified as influential factors in older adults’ aging in place. For the person dimension, we included a range of health status indicators. Functional status measured activity of daily living (ADL) difficulties (bathing, eating, dressing, walking across rooms, and entering or leaving bed; no limitations = 0, less than two limitations = 1, three and more limitations = 2). Physical health was measured on a scale of 0–8, using presence of chronic health conditions prevalent in later life. Additionally, we included two environmental covariates: perceived neighborhood safety (excellent = 1, very good = 2, good = 3, fair = 4, poor = 5) and residential area (urban areas of more than 250,000 population = 0, rural areas of fewer than 250,000 population = 1) to control for the unequal availability of senior-housing facilities.
Analytical Strategy
We used multilevel growth modeling to analyze depressive symptoms over time and to examine how socioeconomic disadvantage affects health depending on senior-housing residence. Multilevel growth models are specifically designed for analysis of trajectories in repeated measures of longitudinal or panel data (Bollen, Christ, & Hipp, 2004), and they estimate individual trajectories based on person-specific initial values of outcomes (intercepts) and rates of change (slope) that describe intraindividual change patterns in outcome as a function of time. Although distribution of depressive symptoms was slightly skewed, preliminary analyses with a logarithmically transformed outcome, producing comparable results, suggested the findings were not sensitive to the normality assumption. Accordingly, results are from the model using original scores of depressive symptoms. The time indicator was determined by the respondent’s wave participation represented as a continuous variable centered on the grand mean; the intercept represented outcome level at mean time of follow-up (3.82 years).
We conducted preliminary analyses to determine the specification of fixed and random effects for change in outcomes over time (results not shown). As the starting point for longitudinal analysis, we estimated total constant correlation across occasions and assessed the relative magnitude of each variation source via an intraclass correlation. Results show that 47% is due to constant mean differences between individuals, while 50% is due to remaining variation surrounding person means. Comparison of model fit between models of increasing complexity indicated that a random linear model provided the best fit for describing time-related outcome change.
Models were increasingly complicated and nested, one for each hierarchy level. Variables were entered sequentially in a model-building process. The first model added an attrition and death indicator to the unconditional model, containing only specification of fixed and random effects for time. The second model examined the effect of poverty status and senior-housing living on outcomes. Third, interaction terms between income status and senior housing were added to evaluate moderating effects of senior housing on outcomes. The final model included sociodemographic, health, and environmental covariates.
Results
Descriptive and Bivariate Analyses
Table 1 presents descriptive sample characteristics at baseline and bivariate associations with income status and senior-housing residency. Across all covariates, clear patterns of association indicate that low-income elders were most vulnerable, followed by moderate-income elders. Relative to their better-off peers, low-income elders were significantly more likely to be older, to be women, and to have lower levels of education; few were White and married. The income groups varied by health and environmental characteristics. A higher proportion of low-income elders had more than three ADLs (3%) and more chronic conditions (M = 1.99). The same pattern of association emerged on environmental context: Low-income elders were more likely to have lower neighborhood-safety levels (M = 2.23) and a higher proportion lived in rural areas (30%). Individuals living in senior housing were more likely to be the oldest-old (21%). A higher proportion was likely to be women (67%). Compared to elders not living in senior housing, a lower proportion of this group tended to be married (33%).
Background Characteristics and Components of Person–Environment Fit Among Older Adults at Baseline (Year = 2002).
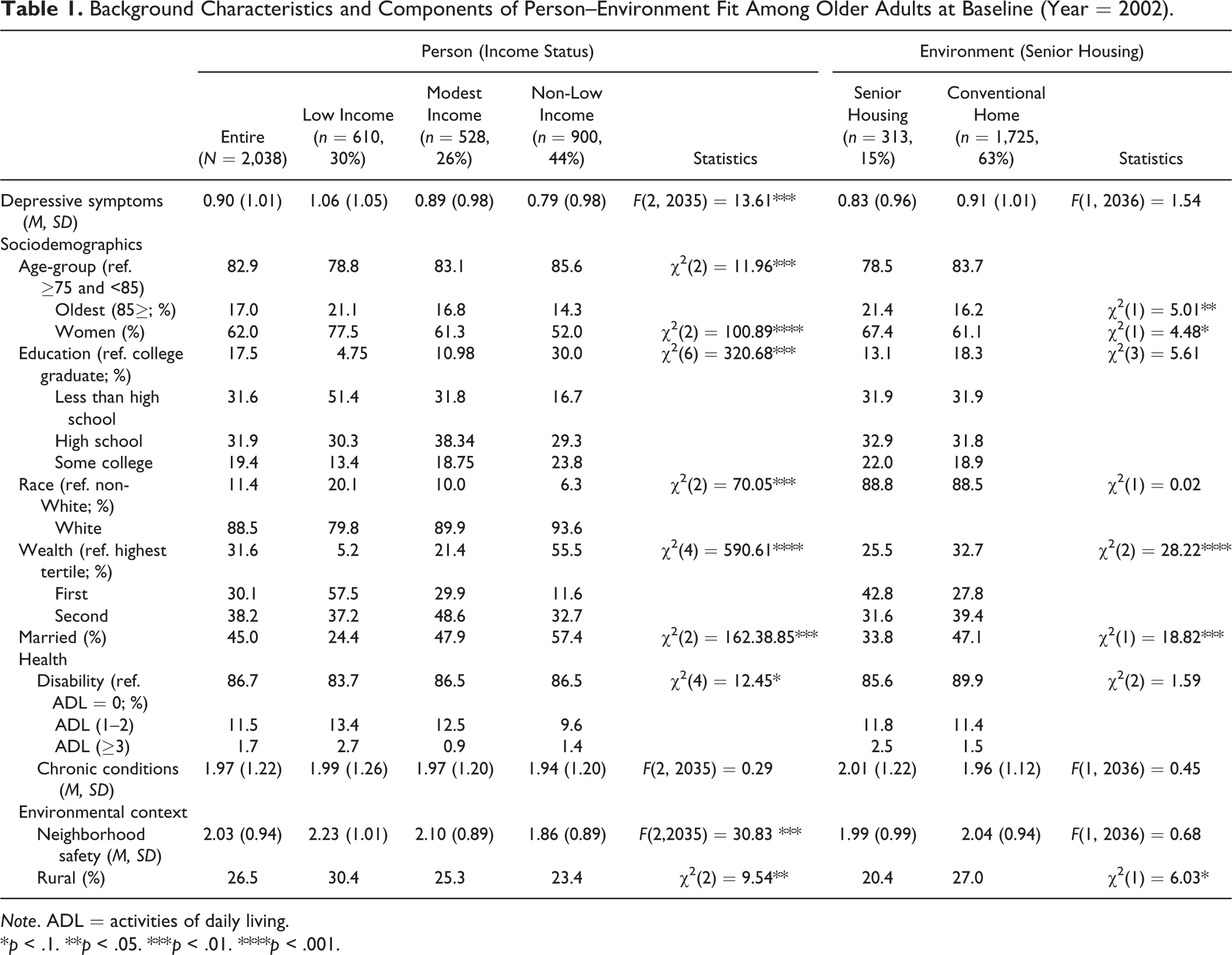
Note. ADL = activities of daily living.
*p < .1. **p < .05. ***p < .01. ****p < .001.
Trajectory of depressive symptoms
Table 2 shows the hierarchical models in this study using linear functions, including intercept and linear slope. Model 1 (Table 2) includes the fixed linear effect of time to examine whether, on average, there is change over time in depressive symptoms. It also includes a random linear effect of time to assess whether people differ in rates of change over time. Depressive symptoms at the mean time of follow-up were 1.22 of a total possible of 8, increasing over time (a linear slope of .39, p < .001 in Model 1). Time is strongly related to depressive symptoms across all models. Random effects are revealed to be significant in between- and within-person variations in depressive symptoms but is reduced or partially explained by each additional set of variables. The significant between- and within-person variance in depressive symptoms at a follow-up mean time of 3.82 years indicated that individuals have different levels of depressive symptoms and that depressive symptoms vary over time (Singer & Willett, 2003).
Economic Vulnerability, Senior Housing, Depressive Symptoms for Fixed and Random Effects.
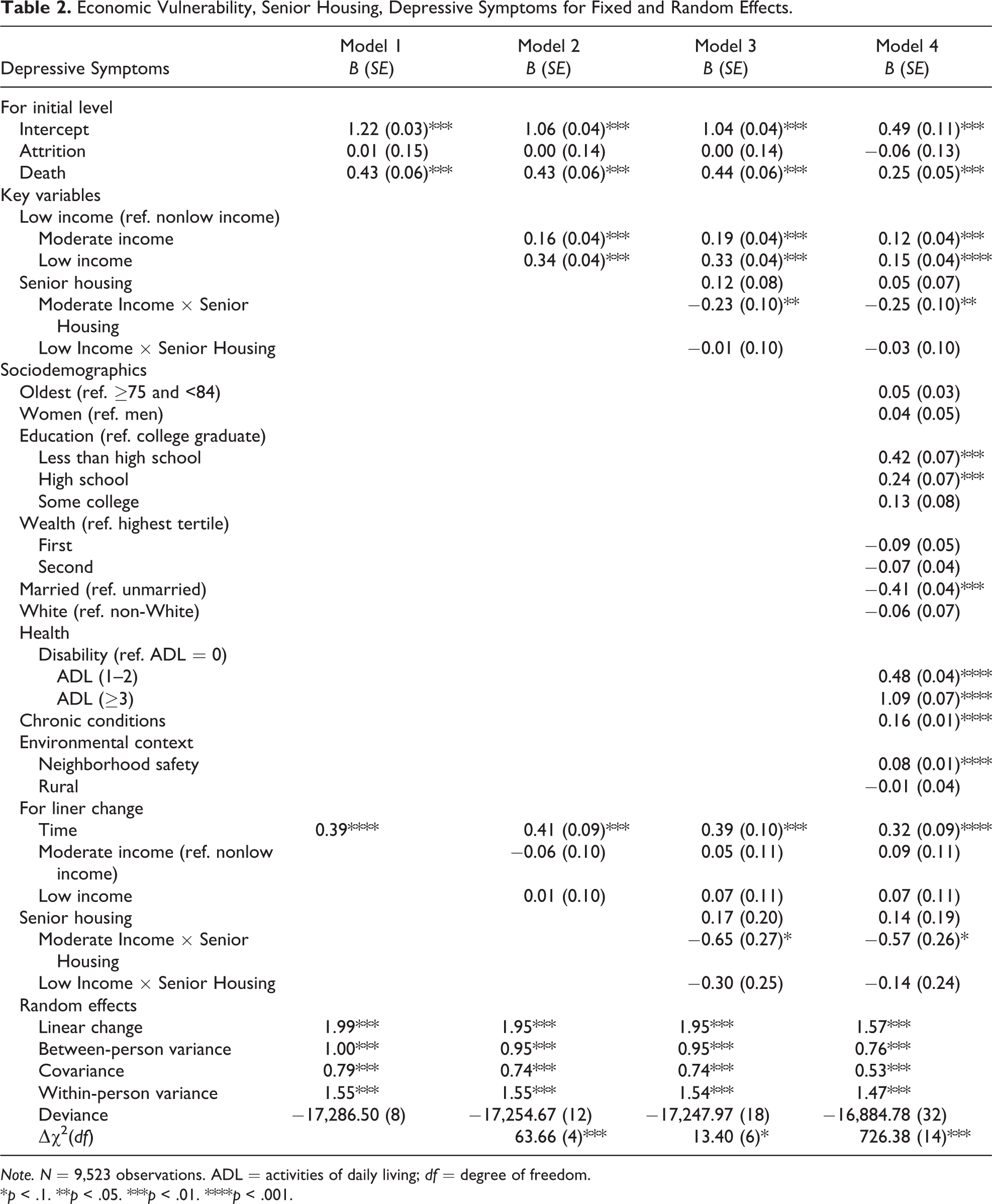
Note. N = 9,523 observations. ADL = activities of daily living; df = degree of freedom.
*p < .1. **p < .05. ***p < .01. ****p < .001.
Economic vulnerability and senior housing in trajectory of depressive symptoms
Main effects of economic vulnerability and senior-housing environment were examined starting at Model 2. As hypothesized, findings showed that, compared to the non low-income reference group, older adults in moderate- and low-income groups are significantly more likely to have higher levels of depressive symptoms across all models. After adjusting for sociodemographic and environmental covariates, moderate- and low-income elders were likely to have higher levels of depressive symptoms, respectively, at baseline (B = .12, p < .01; B = .15, p < .001 in Model 4). However, both moderate- and low-income status had no significant effect on change of depressive symptoms over time. Across all models examined, no main effect of senior-housing residency was found.
Trajectory of P-E fit: Economic vulnerability and senior housing interaction
In Model 3, interaction terms between income groups and senior housing were included to investigate the extent to which senior housing moderates the main effect of low income on depressive symptoms. Findings show that senior-housing environments positively moderate the main effect of economic vulnerability. Compared to the non-low-income reference group, older adults in the moderate-income group were less likely to have depressive symptoms when living in senior housing (B = −.23, p < .05). In Model 4, when all other covariates are controlled, the moderating effect of senior housing holds. This suggests that, for individuals in the moderate-income group, living in senior housing moderates the effect of their accumulated disadvantage on depressive symptoms (B = −.25, p < .05).
Sociodemographic and environmental covariates
Findings from Model 4 indicate that depressive symptoms are correlated with most sociodemographic characteristics, with the exception of age, gender, and race. Lower education level is significantly related to more depressive symptoms; and married individuals are less likely to be depressed (B = −.41, p < .001). Older adults with higher disability levels (B = .48, p < .001 and B = 1.09, p < .001) and those experiencing more chronic health conditions are more likely to have increased depressive symptoms (B = .016, p < .001).
Discussion
Based on the premise that aging in place is a longitudinal, differential process, this study extends the empirical examination of P-E fit from the life-course perspective. Specifically, focusing on low-income older adults and senior housing, we examined the trajectory of later-life depressive symptoms and how senior-housing environments moderate disadvantages of low-SES older people overtime. To the best of our knowledge, this is the first study that empirically examines differential aging in place over time using P-E fit perspective.
Depressive Symptoms Among the Economically Disadvantaged in Old Age Over Time
Our first research question investigates the extent to which lower income status and senior-housing environments are independently associated with depressive symptoms. Drawing from the life-course perspective, we examined low-income status among older adults as the downstream manifestation of a lifelong history of resource privation that was associated with later health and socioeconomic difficulties. As expected, economically disadvantaged older adults were more likely to exhibit depressive symptoms. The impact of low-income status on depression was stronger relative to moderate-income—unsurprising since descriptive and bivariate analysis showed low-income individuals were most vulnerable in all social stratification factors (i.e., age, gender, race, and education) and environmental contexts. Findings in our final model indicate that vulnerability in social stratification factors was a strong predictor of later-life depression. Together, these findings confirm the life-course perspective that old-age disadvantage level emerges from a life history of accumulated disadvantage.
The life-course perspective stipulates that current accumulation levels have direct causal relationships on future accumulation levels. We expected that older adults in lower income groups were likely to be more depressed over time. Interestingly, the detrimental effect of income group (non-low income vs. moderate income; non-low income vs. low income) on depressive symptoms (identified at baseline) did not significantly change over time. These results indicate that SES disadvantage among low- and moderate-income groups is weaker than hypothesized. Similar findings were reported in a longitudinal study of adults that applied latent-growth modeling to examine trajectory changes for depression (Kim & Durden, 2007). Caution is warranted, however, since few studies explicitly focus on longitudinal associations between SES disadvantage and depressive symptoms among old-old or very-old individuals. In accordance with prior findings, we suggest that the age-leveler hypothesis may account for the nonsignificant effects of disadvantaged income groups over time. In other words, the effect of poverty on depression over time may be suppressed by older adults’ adaptation mechanisms, thus maintaining a persistent rate of change in depression over time. In contrast to the life-course perspective, the age-leveler hypothesis holds that relationships between SES and health may weaken in old age. The diminished effects of perceived economic hardship or financial strain on depression may be stronger in the current study because of its focus on the oldest-old.
Differential Aging in Place
Given the environmental docility hypothesis, we expected economically vulnerable elders to be more affected by environmental resources and needs; therefore, we expected lower income individuals living in supportive senior housing—those that directly provide or arrange for health and social services—would be less likely to be depressed. Our findings showed that moderate-income individuals who live in senior-housing environments are less likely to be depressed; senior housing may also play a positive role for the most-vulnerable low-income elders, but the effect was not statistically significant.
Senior housing’s positive effect for disadvantaged groups may provide meaningful implications for both theoretical and empirical research and for aging in place policies and program interventions. Aging in place, some suggest, is the strong preference among older adults (Cutchin, 2003). For moderate- and low-income older adults with limited resources to modify their homes, aging in place become “stuck in place” because they lack a better option (Torres-Gil & Hofland, 2012). Our findings suggest that moderate-income seniors may experience positive differentials if they age in place in a supportive senior-housing environment. Specifically, moderate-income seniors may have broader opportunities for positive experiences such as social engagement within the senior housing environment compared to their private-home peers. As such, senior housing may help counter risks, such as higher depressive symptoms, emerging from life-course disadvantage (Ferraro, Shippee, & Schafer, 2009).
Among low-income groups in our sample, senior housing lacked the significantly positive effect it had among moderate-income elders. As most aging programs and services tended to be income-based entitlements, the low-income group may receive community-based social and health services when eligible for Medicaid or other state programs. This may suggest that despite the lifelong cumulative disadvantages of low-income elders, moderate-income elders may be more vulnerable, since they may have limited available and affordable community-based resources compared to low-income elders. Data limitations preclude us from identifying the role of community-based services. Future inquiry should confirm whether moderate-income elders benefit from senior housing when controlling for the possible cofounding effects of available supportive services in the community. From a policy-making and planning perspective, such future research will provide evidence regarding the need for affordable senior housing for moderate-income elders.
Limitations
We acknowledge this study’s limitations. We used a binary indicator for senior-housing environment, although a more refined senior-housing categorization using housing-industry definitions—independent living facility, assisted living facility, and continued-care residential complex—would be ideal (Coe & Boyle, 2012). To date, no nationally representative panel data enables in-depth examination of dynamic aging in place in diverse senior-housing environments. Lack of empirical senior-housing data is our foremost challenge, but senior-housing environments make it increasingly difficult to differentiate between independent- and assisted-living contexts. For example, in independent-living facilities, older adults receive community-based social and health services when eligible for Medicaid or other state programs. Also, many affordable senior-housing options, although designated independent-living facilities, offer service-coordination programs (Perl, 2010) that link community-health and social services. Individuals who live in senior housing may be considered relatively more risky in terms of health and SES, potentially causing selection problems. The use of methodological techniques that rigorously address this endogeneity issue, such as propensity score or instrumental variables, is warranted in future research.
Another concern is related to temporality of income status and senior-housing residence. We examined income as time varying but did not model temporal patterns over time to examine the relationship between income trajectories and later-life depressive symptoms. In more than 80% of the sample, no change in income status or senior housing occurred during the observed period. Separate analysis (results not shown) examined these variables as time fixed with baseline response; results were essentially identical. Explicit change modeling would be too complicated in the current analytic model, which tested three-way interactions. Still, previous SES health inequality research indicated the importance of examining dynamic temporal low-income patterns (i.e., change in poverty status, duration of poverty, and perceived economic strain; Adena & Myck, 2014).
Conclusion
Despite these limitations, our study is among the first to empirically demonstrate the positive effects of senior housing among economically vulnerable elders using nationally representative longitudinal data. Findings provide much-needed practical and theoretical information for policy-making efforts regarding vulnerable elders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.